2020 Collector Update - Lyndsey Diehl, RHIA, CHDA, CSTR Director of Trauma Data Quality Stephanie Radzevick, CPC Trauma Data Analyst
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2020 Collector Update
Lyndsey Diehl, RHIA, CHDA, CSTR
Director of Trauma Data Quality
Stephanie Radzevick, CPC
Trauma Data Analyst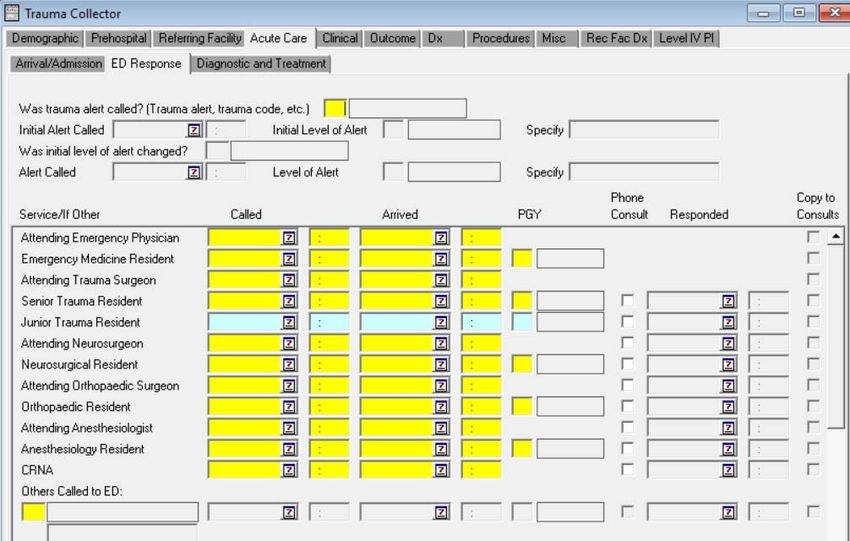
Proprietary Rights Notice The Digital Innovation, Inc. Trauma Registry Software and related materials, including but not limited to this document, and other written material provided by Digital Innovation, Inc. (collectively “Software Products”) constitute confidential and proprietary information of Digital Innovation, Inc. It is the responsibility of the user to comply with all applicable copyright laws. The Software Products are to be maintained in confidence and not to be disclosed, duplicated, or otherwise reproduced, directly or indirectly, whole or in part, or any materials relating thereto, except as specifically authorized by Digital Innovation, Inc. No portions of this presentation may be reproduced, duplicated, or disclosed without the expressed written approval of Digital Innovation, Inc. Reasonable steps are to be taken to ensure that no unauthorized persons have access to the Software Products and that all authorized persons having access to the Software Products refrain from any such disclosure, duplication, or reproduction except as authorized by Digital Innovation, Inc.
Proprietary Rights Notice Copyright © 1998‐2017. Digital Innovation, Inc. All Rights Reserved The referenced Trauma Registry Software is developed and maintained by Digital Innovation, Inc., PTSF’s Technology Partner. The Trauma Registry Software screenshots included in this presentation are from Digital Innovation, Inc.’s product suite.

Change Cycle
Request received
(by August 1)
Trauma Registry
Committee
(March, June,
August, December)
PTSF Board of
Directors (March,
July, September,
December)
PTOS Manual
(December)
Collector Software
(January)
Breakdown This Photo by Unknown Author is licensed under CC BY‐ND
Stephanie Radzevick, CPC Trauma Data Analyst

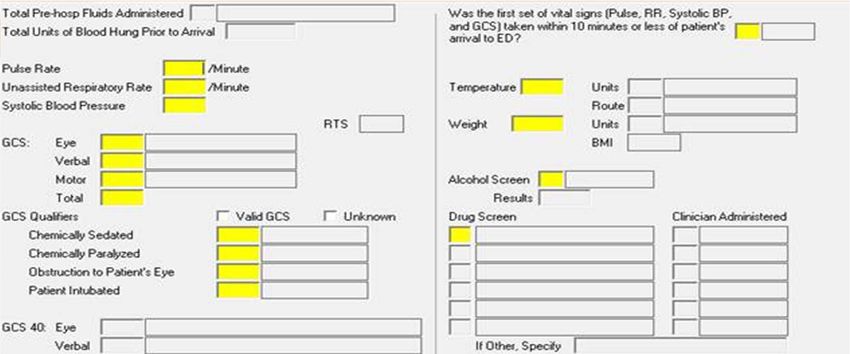
Initial ED/Hospital Height • Has been an NTDB element, but in 2020 will be added as required PTOS element and match NTDB ‘Initial Height’ element • Definition ‐ First recorded height within 24 hours or less of ED/hospital arrival. • Move from NTDB tab to PTOS Clinical Data section, Admission Vitals tab under Weight element • Allows for auto calculation of BMI • Only for On Admission vitals, not added to Referring Facility vitals
Initial ED/Hospital Oxygen Saturation, Supplemental
Oxygen
• The following NTDB elements will also become
required PTOS elements in 2020
– Initial ED/Hospital Oxygen Saturation
• 1st recorded oxygen sat within 30 mins or less of
ED/hospital arrival, expressed as %
and
– Initial ED/Hospital Supplemental Oxygen
• Presence of supplemental oxygen during assessment of
initial ED/Hospital oxygen sat level within 30 mins or less of
arrival
• Will be moved to the Clinical tab under Admission
Vitals
Audit Filters 16 and 20 ‐ Signs of Life • Add Signs of Life = 2 (Arrived with signs of life) to the queries for Audit Filters 16 and 20 • Audit Filter 16 = Nonfixation of femoral shaft fx in adult trauma patient • Audit Filter 20 = Diagnosis at discharge of c spine fx, subluxation, or neuro deficit not addressed on admission • Eliminate DOA’s from triggering for these two filters
Audit Filters 16 and 20 ‐ Signs of Life
• Audit Filter 16 = Nonfixation of femoral shaft fx in adult trauma
patient
– Trauma Patient; AND
– Derived Age (AGE) ≥ 15; AND
– Any ICD‐10‐CM diagnosis code (ICD10_01, ICD10_02, ... ICD10_27)
that starts with S72.3;
– AND
– NO Procedure that starts with (PR_01_I10...PR_84_I10 OQS
[6,7,8,9,B,C] [0,3,4][4,5,6,B,C,D]OR starts with OQH [6,7,8,9,B,C]
– Signs of Life = 2 (Arrived with signs of life)Audit Filters 16 and 20 ‐ Signs of Life • Audit Filter 20 = Diagnosis at discharge of c spine fx, subluxation, or neuro deficit not addressed on admission • Trauma Patient; AND • "Did patient have discharge diagnosis of cervical spine fracture, subluxation, or neuro deficit not addressed on admission?" (MISSED_CS) = 1 (Yes) • Signs of Life = 2 (Arrived with signs of life)
Audit Filter #3a • In 2019 it was discovered that AF 3a was not applying the 2 hour criteria • Change made to title of Audit filter in manual for 2019 – Patient with admission Glasgow Coma Scale score
Audit Filter #11a
• AF #11a ‐ Patient transferred in after 3 hours at initial hospital
– "Is this a transfer patient?" (TRANSF_PT) = 1 (Yes);
– AND Time from Arrival at Referring Hospital (DATE_REF_AR,
TIME_REF_AR) to Departure from Referring Hospital > 3 hours
(DATE_REF_DP, TIME_REF_DP)
• For 2020 – Add to Filter 11a query to exclude patients with
injury time greater than 24 hours prior to arrival at referring
hospital
• Applies to patients transferred in to your facilityAudit Filter #11b • Filter 11b ‐ Patient transferred out after 3 hours from ED arrival • Should filter #11b also exclude patients who are transferred out > 24 hours after injury time? • There is a standards requirement to review pts transferred out > 3 hours (regardless of injury date/time) • No changes will be made to filter #11b
TRISS EOE Functionality • TRISS EOE is designed to provide scoring for intubated patients but uses ICD‐9 codes. This is not seen in Collector, as it requires automapping to report out. We are working with DI to update this measure to utilize ICD‐10 codes
Administrative Time in ED (LOS) (Auto‐Calculation)
• For 2020 ‐ Add an Auto Calculation for administrative ED
length of stay
• ED Admission Date/Time to Administratively Discharged from
ED Date/Time
– Administratively Discharged = Time order was written for pt to be
d/c’d from ED
• Will be located on Acute Care/Arrival/Admission tab of
collector
• HH:MMOthers Called to ED ‐ PGY option • Currently ‐ PGY field enabled only if a resident specialty is selected
Others Called to ED ‐ PGY field • Request to make PGY available for all menu choices in ‘Others Called to ED’ list – A Not Applicable (N/A) option will be added – There is currently no check on the PGY fields – No plans to add a check
Consult Tab ‐ PGY field • Request to make PGY available for all specialty choices on the Consult tab – A Not Applicable (N/A) option will be added – There is currently no check on the PGY fields – No plans to add a check
Admit Unit
• Admit Unit ‐ New optional element for 2020
– Will allow PA Trauma Centers to record a specific floor or location
within their facility for Post ED Destination
• For 2019 admissions, an “other” and specify option was added
to the “Post ED Destination” menu
– This new “other” option should NOT be used to enter specific floors
or ICU’s within your facility, only to capture a Post ED Destination
that is not listed as a menu option
• Negatively affects reporting on Post ED DestinationDeath/Discharge/Transfer Date and Time
• Currently ‐
• Date of Death/Discharge/Transfer
– Record the date (month/day/year) the patient expired, was
discharged alive, or was transferred
• Time of Death/Transfer
– Record the time patient expired or was transferred to another acute
care facility (trauma center, burn center, other)
• For 2020, record Date and Time for ALL hospital deaths,
discharges, and transfers
– Death/Discharge/Transfer Date
– Death/Discharge/Transfer TimeMidline Shift • Located on the Procedures 2 tab • Update element to read ‘Midline Shift >5mm imaged within 24 hours?’ in 2020
Date/Time Entered ED • Currently ‐ • Date Entered ED – record date pt entered the emergency department (ED) • Time Entered ED – record military time pt entered the emergency department (ED)
Date/Time Entered ED/Hospital
• Request to add ‘Hospital’ to title and definition
• Date Entered ED/Hospital – Record the date the pt arrived to
the Emergency Department (ED)/hospital
• Time Entered ED/Hospital – Record the military time pt
entered the Emergency Department (ED)/hospital
– Additional Information
• If the patient was brought to the ED, enter time patient arrived at ED. If
patient was directly admitted to the hospital, enter time patient was
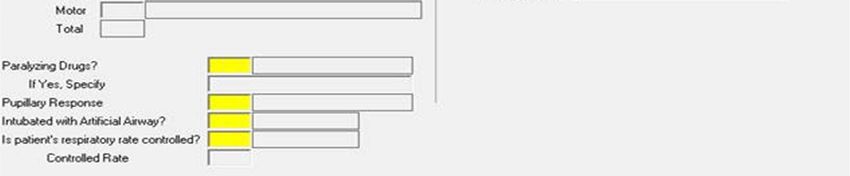
admitted to the hospital.GCS Qualifiers – Paralyzing Drug Specify
• GCS Qualifiers do not apply when GCS 40 is used
– GCS 40 does not have qualifier elements
– GCS 40 contains ‘Not Testable’ options for each component,
eliminating the need for Qualifiers
• The Paralyzing Drugs element is triggered by GCS Qualifiers
• Paralyzing Drugs will be separated from GCS Qualifier
elements for 2020
– This is the way it had been setup prior to 2018
• This will apply to Pre‐hospital (Scene and transport), Referring
Facility, Inter‐Hospital Transport and On Admission sectionsCurrent Screen
Lyndsey Diehl, RHIA, CHDA, CSTR Director of Trauma Data Quality
ABUSE – WAS PATIENT DISCHARGED TO A
DIFFERENT CAREGIVER THAN WHEN THEY
WERE ADMITTED? & IF YES…
Patient discharged to a different caregiver than when they were
admitted to your facility
Made optional for 2020!2019 ‐ S.08 – Pre‐hospital Cardiac Arrest with CPR
A patient who experienced a sudden cessation of cardiac
activity. The patient was unresponsive with no normal
breathing and no signs of circulation. The event must have
occurred outside of the reporting hospital, prior to
admission at the center in which the registry is maintained.
Pre‐hospital cardiac arrest could occur at a transferring
institution. Any component of basic and/or advanced cardiac
life support must have been initiated by a health care
provider.
Revised for 2020!2020 ‐ S.08 – Pre‐hospital Cardiac Arrest with CPR Indication of whether patient experienced cardiac arrest prior to ED/Hospital arrival. Additional Information • A patient who experienced a sudden cessation of cardiac activity. The patient was unresponsive with no normal breathing and no signs of circulation. • The event must have occurred outside of the index hospital. Pre‐hospital cardiac arrest could occur at a transferring institution. • Any component of basic and/or advanced cardiac life support must have been initiated.
2019 ‐ Post ED Destination
Record the patient’s final destination from the ED
Additional Information
• If patient was a direct admission, record patient
destination.
• The ‘Other’ option should not be used to capture specific
floors at a facility. If the location is a step down, ICU, or
floor unit, the appropriate menu option should be used
– A custom element can be used to capture specific units within
your facility
Definition revised and clarification added for 2020!2020 ‐ Post ED Destination
The disposition unit the order was written for the patient to be
discharged from the ED.
Additional Information
• If patient was a direct admission, record patient destination.
• The ‘Other’ option should not be used to capture specific floors at a
facility. If the location is a step down, ICU, or floor unit, the appropriate
menu option should be used
– A custom element can be used to capture specific units within your
facility
• If multiple orders were written, report the final disposition order.
• If the patient was discharged from the ED to the OR, Interventional
Angiography or Morgue, record the destination even if there is no formal
order documented.2019 ‐ N.02 – Chronic Ongoing Alcohol Abuse Utilize the NTDB definition for Alcohol Use Disorder, (Consistent with American Psychiatric Association (APA) DSM 5, 2013.) which is defined Diagnosis of alcohol use disorder documented in the patient medical record, present prior to injury, consistent with APA DSM 5. Note: Social work, drug and alcohol counselor consults may be used to document this pre‐ existing condition. Do not also code N.01 Substance Abuse Disorder. Revised for 2020!
2020 ‐ N.02 – Chronic Ongoing Alcohol Abuse Descriptors documented in the medical record consistent with the diagnostic criteria of alcohol use disorder OR a diagnosis of alcohol use disorder documented in the patient’s medical record. Additional Information • Present prior to injury. • Consistent with American Psychiatric Association (APA) DSM 5, 2013. • The null value “Not Known/Not Recorded” is only reported if no past medical history is available.
2019 ‐ E.00 – Mental/Personality Disorder
Utilize the NTDB definition for Mental/Personality
Disorder which is defined as ‐ (Consistent with
American Psychiatric Association (APA) DSM 5, 2013
Documentation of the presence of pre‐injury
depressive disorder, bipolar disorder, schizophrenia,
borderline or antisocial personality disorder, and/or
adjustment disorder/post‐traumatic stress disorder.
A diagnosis of Mental/Personality Disorder must be
documented in the patient's medical record.
Revised for 2020!2020 ‐ E.00 – Mental/Personality Disorder
History of a diagnosis and/or treatment for the following disorder(s)
documented in the patient’s medical
record:
• Schizophrenia
• Bipolar Disorder
• Major Depressive Disorder
• Social Anxiety Disorder
• Posttraumatic Stress Disorder
• Antisocial Personality Disorder
Additional Information
• Present prior to injury.
• Consistent with American Psychiatric Association (APA) DSM 5, 2013.
• The null value “Not Known/Not Recorded” is only reported if no past
medical history is available.2019 – P.00 – Pregnancy
Patient presenting with current (gravid)
pregnancy with obvious physical findings of
pregnancy, confirmed by lab work, ultrasound,
or as reported by patient and/or family
members.
Revised for 2020!2020 – P.00 ‐ Pregnancy Pregnancy confirmed by lab, ultrasound, or other diagnostic tool OR diagnosis of pregnancy documented in the patient’s medical record. Additional Information • Present prior to arrival at your center.
2019 – N.01 – Substance Abuse Disorder
Utilize the NTDB definition for Substance Abuse
Disorder (Consistent with American Psychiatric
Association (APA) DSM 5, 2013. Documentation of
Substance Abuse Disorder in the patient medical
record, present prior to injury. A diagnosis of Substance
Abuse Disorder must be documented in the patient's
medical record. EXCLUDE: Tobacco Use Disorder and
Alcohol Use Disorder
Revised for 2020!2020 – N.01 – Substance Abuse Disorder
Descriptors documented in the patient’s medical record consistent with the diagnostic criteria of
substance use disorders specifically cannabis, hallucinogens, inhalants, opioids, sedative/hypnotics, and
stimulants (e.g. patient has a history of drug use; patient has a history of opioid use) OR diagnosis of any
of the following documented in the patient’s medical record:
• Cannabis Use Disorder; Other Cannabis‐Induced Disorder; Unspecified Cannabis‐Related
• Disorder
• Phencyclidine Use Disorder; Other Hallucinogen Use Disorder; Hallucinogen Persisting Perception
Disorder; Other Phencyclidine‐Induced Disorder; Other Hallucinogen‐Induced Disorder; Unspecified
Phencyclidine‐Related Disorder; Unspecified Hallucinogen‐Related Disorder
• Inhalant Use Disorder; Other Inhalant‐Induced Disorder; Unspecified Inhalant‐Related Disorder
• Opioid Use Disorder; Other Opioid‐Induced Disorder; Unspecified Opioid‐Related Disorder
• Sedative, Hypnotic, or Anxiolytic Use Disorder; Other Sedative, Hypnotic, or Anxiolytic‐Induced
• Disorder; Unspecified Sedative, Hypnotic, or Anxiolytic‐Related Disorder
• Stimulant Use Disorder; Other Stimulant‐Induced Disorder; Unspecified Stimulant‐Related Disorder
Additional Information
• Present prior to arrival at your center.
• Consistent with the American Psychiatric Association (APA) DSM 5, 2013.
Note: Now referred to as “Substance Use Disorder” in NTDB!2019 – 206 = Cardiac Arrest with CPR
Utilize the NTDB Complication definition for Cardiac Arrest
with CPR, which states: Cardiac arrest is the sudden cessation
of cardiac activity after hospital arrival. The patient becomes
unresponsive with no normal breathing and no signs of
circulation. If corrective measures are not taken rapidly, this
condition progresses to sudden death.
INCLUDE patients who have had an episode of cardiac arrest
evaluated by hospital personnel and received compressions or
defibrillation or cardioversion or cardiac pacing to restore
circulation.
EXCLUDE patients who are receiving CPR on arrival to your
hospital
Revised for 2020!2020 – 206 = Cardiac Arrest with CPR Cardiac arrest is the sudden cessation of cardiac activity after hospital arrival. The patient becomes unresponsive with no normal breathing and no signs of circulation. If corrective measures are not taken rapidly, this condition progresses to sudden death. Additional Information • Must have occurred during the patient's initial stay at your hospital. • Cardiac arrest must be documented in the patient's medical record. • EXCLUDE patients whose ONLY episode of cardiac arrest with CPR was on arrival to your hospital. • INCLUDE patients who, after arrival at your hospital, have had an episode of cardiac arrest evaluated by hospital personnel, and received compressions or defibrillation or cardioversion or cardiac pacing to restore circulation.
2020 ‐ Delirium
Added for 2020 (# TBD)!
Acute onset of behaviors characterized by restlessness, illusions, and incoherence of
thought and speech. Delirium can often be traced to one or more contributing factors,
such as a severe or chronic medical illness, changes in your metabolic balance (such as
low sodium), medication, infection, surgery, or alcohol or drug withdrawal.
OR
Patient tests positive after using an objective screening tool like the Confusion
Assessment Method (CAM or the Intensive Care Delirium Screening Checklist (ICDSC).
OR
A diagnosis of delirium documented in the patient’s medical record.
Additional Information
• Must have occurred during the patient's initial stay at your hospital.
• EXCLUDE: Patient’s whose delirium is due to alcohol withdrawal.2019 – 35 = Myocardial Infarction
Utilize the NTDB Complication definition for Myocardial Infarction, which states:
An acute myocardial infarction must be noted with documentation of any of the
following:
Documentation of ECG changes indicative of acute MI (one or more of the
following three):
1. ST elevation >1 mm in two or more contiguous leads
2. New left bundle branch block
3. New q‐wave in two or more contiguous leads
OR
New elevation in troponin greater than three times upper level of the reference
range in the setting of suspected myocardial ischemia
OR
Physician diagnosis of myocardial infarction
Must have occurred during the patient’s initial stay at your hospital.
Revised for 2020!2020 – 35 = Myocardial Infarction An acute myocardial infarction must be noted with documentation of ECG changes indicative of an acute MI AND New elevation in troponin greater than three times upper level of the reference range in the setting of suspected myocardial ischemia AND Physician diagnosis of an acute myocardial infarction that occurred subsequent to arrival at your center
2019 – 203 = Unplanned Return to the OR
203 = Unplanned return to the OR: Unplanned
return to the operating room after initial
operation management for a similar or related
previous procedure.
Revised for 2020!2020 – 203 = Unplanned Visit to the
Operating Room
Patients with an unplanned operative procedure OR patients
returned to the operating room after initial operation
management of a related previous procedure.
Additional Information
• Must have occurred during the patient's initial stay at your
hospital.
• EXCLUDE: Pre‐planned, staged and/or procedures for
incidental findings.
• EXCLUDE: Operative management related to a procedure that
was initially performed prior to arrival at your center.2019 – Discharge Destination
The destination of the patient on formal discharge.
Additional Information
• See Appendix 8 for more information on Discharge Destination choices
• This element will be skipped if the patient died
• If a burn patient is discharged or transferred to a burn center that is also a trauma center the
“Discharge Destination” should be “6” for burn center
• “If the patient is discharged from the acute care unit to a facility rehab
• If the patient is discharged to an in‐patient rehabilitation facility or in‐patient psychiatric facility within
an acute care hospital, record ‘Discharge Destination’ as 4, Rehabilitation Center or 7, Psychiatric
Facility. Use the facility number for the acute care hospital to record ‘Discharge to Facility Number.’
• If the patient is discharged from the acute care facility to a Skilled Nursing Facility, record the discharge
destination as “5” Skilled Nursing Facility. Comment field may be used to note “Home” if the SNF is
patient residence.
• If patient discharge home on hospice services, record discharge destination as ’17 Hospice’. Comment
field may be used to note “Home” for patient location.
• If patient instructed to go to another hospital via private vehicle, record ’14 PA Trauma Center’.
Comment field may be used to indicate ‘Private Vehicle’.
Clarification added for 2020!2020 – Discharge Destination
The destination of the patient on formal discharge.
Additional Information
• See Appendix 8 for more information on Discharge Destination choices
• This element will be skipped if the patient died
• If a burn patient is discharged or transferred to a burn center that is also a trauma center the “Discharge
Destination” should be “6” for burn center
• “If the patient is discharged from the acute care unit to a facility rehab
• If the patient is discharged to an in‐patient rehabilitation facility or in‐patient psychiatric facility within an
acute care hospital, record ‘Discharge Destination’ as 4, Rehabilitation Center or 7, Psychiatric Facility. Use
the facility number for the acute care hospital to record ‘Discharge to Facility Number.’
• If the patient is discharged from the acute care facility to a Skilled Nursing Facility, record the discharge
destination as “5” Skilled Nursing Facility. Comment field may be used to note “Home” if the SNF is patient
residence.
• If patient discharge home on hospice services, record discharge destination as ’17 Hospice’. Comment field
may be used to note “Home” for patient location.
• If patient instructed to go to another hospital via private vehicle, record ’14 PA Trauma Center’. Comment
field may be used to indicate ‘Private Vehicle’.
• If multiple orders were written, report the final disposition order.2019 ‐ Blood Products Retired for 2020! (New Additions for 2020!)
2020 – Blood Products • Packed Red Blood Cells • Whole Blood • Plasma Added for 2020! • Platelets • Cryoprecipitate Additional Definition Changes: • Enter only in CC/mLs within 4 hours • Exclude transfusing product upon patient arrival Note: PTOS will continue to capture Total Prehospital Units of Blood Hung which will capture the number of units of packed cells or whole blood hung during the pre‐hospital treatment.
2020 – Antibiotic Therapy • Was Intravenous Antibiotic Therapy Administered Within 24 Hours After the First Hospital Encounter? • Antibiotic Therapy Date • Antibiotic Therapy Time Additional Information: Open fractures as defined by the Association for the Advancement of Automotive Medicine AIS Coding Rules and Guidelines.
Tourniquet Use (Draft Only!)
New Additions for 2020!
• Tourniquet Use
• Tourniquet Placed
• Tourniquet Placed By
• Date Tourniquet Placed
• Time Tourniquet Placed
• Date Tourniquet Removed
• Time Tourniquet Removed
Note: These elements will be located under “Demographics” on
the Injury Tab within Collector.Tourniquet Use Definition: Did the patient have a tourniquet placed? Field Values: 1 – Yes 2 – No U – Unknown
Tourniquet Placed Definition: In what setting was the tourniquet placed? Field Values: 1 – Prehospital 2 – Outside Hospital 3 – Interhospital Transport 4 – In house U – Unknown Additional Information: Will skip if Tourniquet Use is answered as 2 – No or U – Unknown
Tourniquet Placed By Definition: Who placed the tourniquet? Field Values: 1 – EMS 2 – Police 3 – Fire 4 – Bystander 5 – Hospital Staff U – Unknown Additional Information: Will skip if Tourniquet Use is answered as 2 – No or U – Unknown
Others Called to ED & Consults Interventional Radiology to be added to both Others Called to ED and Consults dropdown menus for 2020.
34 = Major Dysrhythmia
REMOVED for 2020!
This Photo by Unknown Author is licensed
under CC BYProvider ID New addition for 2020!
Burn Patients at Burn Centers Only!
• 10 = Burn Graft Loss (of any percentage)
– 2020 – 10 = Burn Graft Loss (of any percentage)
requiring repeat procedure
• 15 = Hypovolemia
– REMOVED for 2020!PTOS Patient
Appendix 7: Prehospital Examples Additions, changes and clarification in 2020 PTOS Manual!
Some Potential Last Minute Changes • Is there sequential neurological documentation on ED record of trauma patient with diagnosis of skull fx, intracranial injury, or spinal cord injury? – Required for 2020! • Is there hourly documentation beginning with ED arrival? – Required for 2020! • Drug Screen ‐ Clinician Administered – Clarification regarding the use of medical marijuana • E‐cigarette and Vaping Use – Added as a pre‐existing condition for 2020
For Your Information!!!
NTDB Inclusion Criteria Changes • “…within 14 days of initial hospital encounter…” • “Patient transfer from one acute care hospital* to another acute care hospital” • “Patients directly admitted to your hospital (exclude patients with isolated injuries admitted for elective and/or planned surgical intervention)” • “Patients who were an in‐patient admission and/or observed” • Patients who were a trauma consult or any level of trauma activation” • REMOVED: “Hospital admission as defined by your trauma registry inclusion criteria;”
Continued…
The PTSF Board of Directors discussed the new NTDB inclusion criteria that was
recently communicated by the American College of Surgeons as being effective
January 1, 2020. Our PTSF Board Chairman Dr. Patrick Reilly reached out to ACS
leadership to communicate the impact this change will have on Pennsylvania
trauma centers. At this time, the PTSF Board asks that you make no changes until
further notice related to the patients your hospital is submitting to the NTDB. The
ACS communicated that they are going to further discuss these changes among
their leadership and offer further advice in the future.
Meanwhile, we will be asking various Pennsylvania Professional Trauma groups to
formally convey the impact of this change with ACS leadership. Those groups
include the PaCOT, PATNAC, and PTSF. Formal letters from hospitals would also be
helpful. Letters should be sent to:
American of Surgeons Committee on Trauma
Attention: NTDB Staff
633 N. Saint Clair Street
Chicago, Illinois
60611‐4111DI Projects
• Collector Transition to PA V5 Trauma Registry
– Minimal to no changes will be made to PTOS for
2021 admissions!
• PTOS Driller
• Registry Educational SoftwareTrauma Registry Tab
• Resources
• Education
• FAQ’s
This Photo by Unknown Author is licensed under CC BY‐NDFYI http://www.memegen.com/meme/en82sg
KnowledgeConnex
https://www.elearningconnex.com/ptsf/
This Photo by Unknown Author is licensed under CC BYAIS 2015 https://goo.gl/images/7vLn8F
PTOS Manual Updates
Look for the 2020 PTOS Manual to be released
Mid‐December 2019!
Throughout 2020 be on the look for…
• Minor corrections
• Clarification
• Possible changesAdditional Resources • Change Document • PTOS vs NTDB Comparison • Element History • RW Dictionary • Facility Lists • PA EMS Affiliates
Baby Diehl Coming January 2020 (hopefully)!
https://goo.gl/images/2TW1Ap
Lyndsey Diehl, RHIA, CHDA, CSTR
Trauma Data Quality Specialist
AHIMA Approved ICD‐10‐CM/PCS Trainer
717‐697‐5512 ext. 105
ldiehl@ptsf.org
www.ptsf.org
Stephanie Radzevick, CPC
Trauma Data Analyst
AHIMA Approved ICD‐10‐CM/PCS Trainer
717‐697‐5512 ext. 109
sradzevick@ptsf.org
www.ptsf.org
Gabrielle Wenger, RHIT, CPC, CAISS
Trauma Registry Auditor
717‐697‐5512 ext. 110
gwenger@ptsf.org
www.ptsf.orgYou can also read