2021/22 Priorities and Operational Planning: Narrative Submission Template - 29 March 2021 v1.0 - Mid Essex CCG
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2021/22 Priorities and Operational Planning: Narrative Submission Template 29 March 2021 v1.0
1. Introduction and overview
This narrative submission is intended to provide additional information against numerical plans and further detail to support national and
regional assurance. Systems should be developing their own local delivery plans to address each area.
ICSs should set out;
• Where appropriate, the actions and assumptions that underpin the trajectories within the activity and workforce numerical submissions;
• other critical actions that systems will take over the next 6 or 12 months to address the priorities set out in 2021/22 priorities and
operational planning guidance and in section 3 (elective recovery), section 4 (health inequalities) and section 5 (maternity) of 2021/22
implementation guidance.
Further instructions to support completion are set out within each section of the template.
2. Submission process
Draft and final plans should be submitted at ICS level, using this template to the appropriate regional planning mailbox (see contacts at
section 4) by;
• Draft submission: 12noon Thursday 6th May
• Final submission: 12noon Thursday 3rd June3. Summary of sections
Response Required
Against
Ref Section of 2021/22 priorities and operational planning guidance Numerical Priorities
Plan A-F
A Supporting the health and wellbeing of staff and taking action on recruitment and retention Yes Yes
B Continuing to meet the needs of patients with Covid-19 No Yes
C1 Maximise elective activity, taking full advantage of the opportunities to transform the delivery of service Yes No
C2 Restore full operation of all cancer services Yes No
C3a Expand and improve mental health services [incorporated in section A.] No No
C3b Expand and improve services for people with a learning disability and/or autism Yes Yes
C4 Deliver improvements in maternity care, including responding to the recommendations of the Ockenden review No Yes
D1 Restoring and increasing access to primary care services No Yes
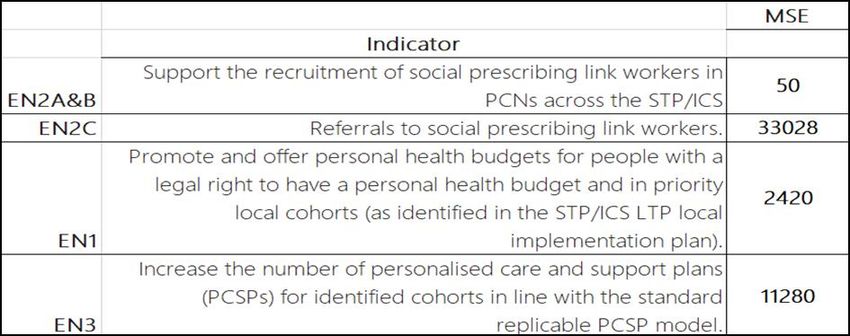
D2 Implementing population health management and personalised care approaches to improve health outcomes and Yes Yes
address health inequalities
E1 Transforming community services and improve discharge Yes Yes
E2 Ensuring the use of NHS111 as the primary route to access urgent care and the timely admission of patients to Yes Yes
hospital who require it from emergency departments
F Working collaboratively across systems to deliver on these priorities [no requirement for narrative submission] No No
Other areas outlined within implementation guidance
Elective Recovery Framework: Gateway Criteria
Health Inequalities: 5 priority areas
4. Contacts/queries
Any queries relating to this submission and template should be directed to your regional planning leads. Contact details below;
Location Contact information
East of England england.eoe2021operplan@nhs.netSystem name: Mid and South Essex Health and Care Partnership
A. Supporting the health and wellbeing of staff and taking action on recruitment and retention – Ruth Jackson
Please set out the specific actions that, as a system, you will prioritise over the next 6 months to address the objectives below
A1 Looking after our people and helping The Mid and South Essex (MSE) system is in the early stages of recovering from an intense period of activity
them to recover related to COVID-19. Both qualitative and quantitative indicators show there is much to be done in terms of
improved results in terms of our workforce. Our workforce must therefore become a central focus of everything
we do. For example:
• Morale, staff numbers and corporate capabilities are all lacking in a number of service areas.
• Performance, professional standards and quality/safety remain at risk in some key areas of provision
(e.g. maternity, elements of primary care).
• The nature and scale of the management and organisational reforms required to stand up our
Integrated Care System (ICS) are considerable.
People and partnerships are key to tackling these things. We must therefore shift resources and skills from
other areas in order to fulfil not only the tasks listed here (in the workforce section of the plan) but to ensure
that other aspects of our overall system work programme can be implemented successfully against tight
deadlines.
The data in the workforce template highlights the challenges we face in terms of recruitment across a broad
range of areas. In this section we have included additional metrics related to sickness and absence which are
one quantitative measure of the efficacy in our plans to look after staff to date.
The Mid & South Essex People Board agreed the following metrics (as part of the five year plan) which will be
used as a benchmark for our system absence rates. The recent appointment of a system workforce analyst will
enable us to develop a broader range of metrics at a system level to enable us track and measure the impact of
any interventions over time. This will enable us to provide assurance as an ICS on the wider workforce
transformation agenda:
Metric 2020/21 2021/22 2022/23 2023/24
Absence Rate NHS 4% 3.5% 3% 2.5%
Absence Rate Direct Care 5% 4.5% 4% 3.5%AGGREGATED AT SYSTEM LEVEL
East of England (EoE) figures have been released up until November 2020 (which do not include COVID-19
sickness) showing that the ICS (Mid and South Essex Health & Care Partnership (MSEH&CP)) was in a
marginally better position with respect to the regional benchmark:
2020/21 STP Moving
Staff Group Aug Sep Oct Nov Dec Jan Feb Mar Average
Add Prof Scientific APS 2.9% 4.2% 2.0% 2.3% 7.4% 8.1% 7.6% 2.0% 2.9%
Additional Clinical Services ACS 5.0% 5.0% 5.2% 5.8% 7.4% 9.1% 6.6% 5.6% 5.3%
Administrative and Clerical A&C 3.2% 3.7% 4.1% 4.1% 4.2% 5.0% 3.3% 2.6% 3.8%
Allied Health Professionals AHP 1.8% 2.7% 1.6% 1.9% 3.8% 4.6% 2.6% 1.8% 2.0%
Estates and Ancillary E&A 7.2% 6.4% 4.0% 4.7% 9.5% 9.6% 5.8% 5.5% 5.6%
Healthcare Scientists HCS 0.2% 0.5% 0.9% 1.5% 0.9% 1.1% 0.8% 0.8% 0.8%
Medical and Dental M&D 1.7% 3.0% 2.9% 3.0% 0.9% 1.4% 4.8% 2.0% 2.6%
Nursing and Midwifery N&M 3.8% 4.0% 4.4% 5.2% 6.4% 8.7% 5.7% 4.0% 4.4%
Total 3.2% 3.7% 3.2% 3.6% 5.1% 6.0% 4.7% 3.0% 3.4%
The underlying data however indicates an increase in sickness related to stress/anxiety and musculoskeletal
conditions which has informed our plans as outlined below.As our system transitions to an ICS we will enact our responsibilities as stipulated in the People Plan and in
accordance with the emerging ICS People & Organisational Development Operating framework. Our current
MSEH&CP workforce strategy will be modified and finessed following the recent System Workforce
Improvement Model (SWIM) review, resulting in the direct responsibility for the planning and organisation of our
workforce initiatives being devolved to modified subgroups of our People Board.
We will:
• Ensure our system Health & Wellbeing Leads network is supported to continue sharing best practice
initiatives developed in NHS providers and extend the membership of this group to primary and social
care colleagues. Utilise the feedback from health and wellbeing guardians in our organisations via the
health and wellbeing leads network to design, plan and implement a system wide initiative which will
complement the existing provider functions utilising a recently received NHSE/I grant.
• Publicise & encourage uptake of our wellbeing offer via our wellbeing leads network and the system
COVID-19 wellbeing webpages. These initiatives include wobble rooms, mindfulness sessions,
Schwartz rounds, Board wellbeing guardians, buddy networks, wellbeing hubs, team time reflective
practice sessions, wellness action plans, embedding wellness conversations within appraisals.
• Co-ordinate system approach to the carry forward and buy back of annual leave.
• With one of our partner organisations, Essex Partnership University Trust (EPUT), evaluate the uptake
and impact of the “Here for You” a 24/7 psychological support helpline offered across our system to all
staff in health& social care https://eput.nhs.uk/our-services/here-for-you.
• Launch “Live life Connected”: a personal development platform open to all staff in our system that
challenges, supports and provides resources to support staff in 6 key areas: sleep, movement, nutrition,
connection, quiet time and clear thinking. The programme will create a common community from across
our partners and space where people can be supported to recover, grow personal resilience and
flourish. The outcomes of this programme specifically address the increasing levels of stress, anxiety
and Musculoskeletal (MSK) issues experienced by our workforce.
• Launch the System Carers Passport: an initiative which facilitates conversations between carers and
their line managers to support staff with caring responsibilities.
• Via the wellbeing leads network promote the occupational health and wellbeing support available to all
staff – which includes fast track access to psychological support and MSK physiotherapy.
• Develop a system wide support network for staff members affected by Post COVID-19 syndrome
(otherwise known as Long COVID-19) and those caring for people with COVID-19 or Post COVID-19
syndrome.
• Working with Human Resource Directors develop a system wide action plan in response to the recent
staff survey results including a network of anti-bullying ambassadors.
• Continued support for staff who fall into the categories of extremely clinically vulnerable and clinically
vulnerable using both individual COVID-19 and workplace risk assessment to ensure the necessary
support is in place for staff to feel confident they are working in safe environments.• Equality, Diversity and Inclusion: support line in place and promoted for all to access and assurance
around individual COVID-19 risk assessments.
• Flexible working in place to support staff with personal, homeworking and operational service
commitments. Develop a system wide approach to returning to the office arrangements.
A2 Belonging in the NHS and addressing Following the publication of the Workforce Race Equality Standard (WRES) data and staff survey we are taking
inequalities urgent actions to tackle racism and address systemic inequality which is experienced by some of our staff,
including ethnic minority staff. We have identified a Senior Responsible Officer (SRO) for the system who will
lead the Equality, Diversity and Inclusion agenda and a new working group will be established to provide
assurance to the Health and Care Partnership Board that actions are being taken. It is proposed that the
People Board will oversee progress on tackling racism and ensuring all system partners have a nominated
Board level SRO to ensure Equality Diversity Inclusion (EDI) is considered as an integral component of Board
agendas. In addition, the System Workforce Improvement Model (SWIM) analysis reinforces we have further
work to establish a robust and effective programme of activity at a system level.
To continue to grow EDI networks and facilitate them to implement changes to improve the support and
resources available from staff and patients in these protected groups. The network is to be responsible for
utilising such guidance as anti-racism strategies (EoE) and prompting action within organisation.
Undertake a system wide analysis of EDI activity with our partners to share and disseminate best practice
initiatives develop the ‘model employer’ plan.
Establish a new subgroup of the People Board to develop and deliver the EDI workforce initiatives for the next
12 months utilising WRES, Staff Survey and focus group data to inform the workforce plans.
Appoint a system EDI lead to work and develop a system plan that has Board sign off in our partner
organisations and through our own governance arrangements via our People Board and MSEH&CP Board.
In September 2020 our People Board agreed a workplan to include the following actions which will be
developed into a system plan by the end of Quarter 1 2021/22:
• Establish a direct link between organisational and system leaders and Black, Asian and other ethnic
minority voices.
• Agree a consistent standard for investment in EDI across all organisations and systems.
• Appoint a senior leader responsible for EDI in each organisation to report to both Executive and Board
meetings as a standing item.
• Equality and Inclusion objectives to be set for all CEOs/AOs/Executives.
• All line managers to undertake cultural competence, compassionate leadership and unconscious bias
training.• All organisations to have Freedom to Speak Up guardians who are reflective of the workforce and part
of Board conversations.
• Develop a consistent message and ensure actions are in place in every organisation for patients and
the public who are abusive towards staff.
• Set up supported Black, Asian and other ethnic minorities network with Executive or NED as Chair.
• Appoint a board level champion for Black, Asian and other ethnic minorities.
• Encourage applicants external to the NHS into roles through the language we use on job adverts and
were we advertise, and tailor our sometimes unwieldy and unfriendly application process to support
candidates.
• Put in place transparent recruitment for stretch opportunities and secondments and encourage our
Black, Asian and other ethnic minority colleagues to apply and support them through the application
process.
• Very Senior Managers (VSMs) and Board members to act as mentor/reverse mentor and sponsor at
least one talented ethnic minority staff at band 8d or below.
• Support a recruitment drive on Black, Asian and other ethnic minority non-executive directors and
associate non-executive directors.
• Existing NEDs will be encouraged to play an active role in mentoring and sponsoring Black, Asian and
other ethnic minority staff that have the potential to move into an executive role within three years.
• Occupational risk assessments of all COVID-19 vulnerable groups will be conducted in a timely manner
and data reviewed at every board meeting, alongside reporting on mitigations in place. Enable staff
voices and concerns to be heard and acted upon at board meetings.
• Invite Black, Asian and other ethnic minority colleagues to join bronze, silver and gold command
groups, to be active participants at senior leadership meetings, to be part of providing staff briefings and
part of shadow board development programmes.
• Agree a dataset to measure progress on equality for all organisations and each MSEH&CP/ICS.
• Capture additional equality data for indicators such as turnover, exit interviews and absences and share
with MSEH&CP/ICS and Region.
• Review the occupational health contracts to improve the offer to primary care.
• Deliver the SWAP and Stepping Up programme.
• Launch the system coaching & mentoring programme on the staff development hub of the Health &
Care Academy.
• Commence the NHS leadership academy transformational mentoring programme with 20 ICS staff.
• Develop a diversity workforce fellowship programme.
• Deliver 3 inequalities summits May-July 2021: Leadership, Collaboration, Strengthening belonging.
A3 Embed new ways of working and We are working with system partners to design a new model of care driven by a Population Health
delivering care Management (PHM) model and based around a ‘stewardship” model; initially we will work in respiratory,
cardiology, stroke, cancer, frailty/ageing well & urgent care. This will require us to develop integrated care
teams and cross sector working. To support this initiative, we will:• Launch a system employment passport which includes all health, primary care and local authority
partners and will enable us to stand up new multi-professional teams to run the projects.
• Develop our system leadership capacity appointing a new lead and launching a new programme with
Exeter University in addition to bidding for the leadership academy offer for system development.
• Launch a train the trainer population health management initiative from the University of Oxford to
embed PHM skills across our workforce.
• Utilising a web based virtual learning environment in our Health & Care Academy we will develop an
initial suite of CPD programmes e.g. personalisation/health coaching, FRAIL+ thus developing our
digital delivery capacity.
• Launch our Band 5 nurse rotation and preceptorship portal programme across acute, community and
mental health providers.
• Commence second cohort of our Quality Improvement leadership development programme.
• Develop an Advanced Clinical Practitioners (ACP) and Allied Health Professionals (AHP) strategy
across primary, secondary and community care.
• Work with Anglia Ruskin University (ARU) develop a career framework for Medical Associate
Professionals (MAPs) with the first phase focusing on psychiatry.
• Work with Essex Welfare Services to expand the ‘positive pathways & progressions” programme for 18-
25 years olds volunteering in Health and Social Care.
• Recommence the work on the System Volunteer Lead Network including training, passport and
Memorandum of Understanding (MOU).
• All service providers have e-rostering in place and majority of staff have access to the system. Policies
are in place to ensure six weekly rostering is in place and unfilled shifts are identified, meaning the
system is currently meeting the ‘level 2 of the attainment and meaningful use standards. We will
support service leads and develop a plan through our recruitment and retention sub-group to meet the
maximum expectations stated within level four criteria, measured through E-rostering key performance
indicators and metrics. We anticipate this will give our teams clearer visibility of their working patterns
and facilitate planning particularly as we promote the commitment to staff taking carried forward leave.
• Promote the flexible working opportunities described in section A1.
A4 Grow for the future The overall vacancy rate for the STP/ICS last year (2020/21) was circa 11%, which is in line with the national
benchmark of 12%. However, whilst this headline figure lower than the national average there are a number of
staff groups with significant vacancy rates in particular nursing, midwifery and some branches of medicine. The
commentary below reflects the high trending (Nursing and Midwifery) vacancy position for each provider which
ranges from 10% for organisations like MESFT to 19% for organisations like NELFT.
The 50K nursing project will produce a clear plan to address these vacancy figures, which includes a focus on
both domestic and international supply, and the development of a plan and target for retention. Turnover data
for Nursing within the system is relatively low at approximately 3.4% but there are issues in specific areas ofthe system like MSEFT and pockets in EPUT attributed to their proximity to London. In contrast to this figure
there seems to be an ongoing retention concerns for Nursing and Midwifery posts within the system with a
higher figure at: 4.4%. Furthermore, these areas do not qualify for initiatives such as high fringe payments, so
the action points below and within the 50K project are designed to support a positive change.
In Autumn 2020 we undertook a recruitment and retention deep dive and this, taken together with our SWIM
phase 1 analysis, has underpinned our thinking and helped us develop the following system objectives:
• Building on the work we have done with Healthcare Support Workers (HCSW) develop with partners a
system wide centre of excellence for recruitment.
• Work with our School of Medicine to design a ‘clinical academic system’ which supports the recruitment
of consultants and GPs and the retention of our undergraduate medical graduates.
• Partner with an oversea hospital group to develop a ‘train, earn and return’ initiative for shortage
medical specialities.
• Develop employment brand including digital assets.
• Develop a system placement dashboard to facilitate forward planning and expansion.
• Develop a system recruitment and retention dashboard to support the 50K nursing initiative using QLIK
sense platform.
• Develop and implement a 50k nursing strategy including increases in the nursing associate role;
embedding international recruitment expertise in all key partners, employer led Real Time Payments
initiatives, maximising undergraduate retention initiative via our Health & Careers Academy, working
with systems estates staff and LAs to develop plans for key worker housing.
• Building on our anchor institution work Deliver Sector-based Work Academy programmes (SWAP)
working with LAs and DWP to promote local opportunities in Health and Social Care. Planned sessions
in the next 6 months include entry level caring roles, administrative roles and estate and facilities.
• Explore and promote talent pipelines - recruit directly into entry level clinical roles, apprenticeships and
non-clinical roles, whilst identifying training recovery plans that integrate local training needs.
• Increase student retention into permanent positions within our system working with partners to expand
our current guaranteed job scheme to nursing and midwifery to psychology and AHP– monitor through
recruitment and retention subgroup.
• Develop a legacy plan for staff approaching retirement to retain their skills and in particular their support
for students with the system.
• Develop a retention action plan with ARU to maximise the number of students remaining in our system
for foundation training in 2023.
• Working with Directors of Medical Education and our local post graduate Dean, we will support medical
trainees whose education and experience may have been disrupted through the surge activity in our
system. The plans focus on three main areas as per the HEE guidance: rotations & educational time;
recruitment and ARCPs exams, and progression. In addition, we are working closely with our School ofMedicine to ensure undergraduate students are now placed and supervised to facilitate their
achievement of the Outcome for Graduates.
Please summarise the key assumptions that underpin the numerical workforce plan submissions listed below, highlighting any key risks and issues. Please
also set out any system actions that are critical to the delivery of the planned workforce levels where these are not set out above, including recruitment and
retention, use of bank and agency, redesign of teams and roles, deployment across sectors and/or organisations and sickness absence.
Primary Care – William Guy
Assumptions GPs:
Increase in FTE for substantive GPs from 2020/21 to end of year 2021/22, based on the following assumptions:
• Inflow of qualifying registrars entering the GP workforce, based on the percentage of trainees likely to be
retained across the system post-qualification (39.80 FTE).
• Inflow of GPs returning to the workforce via retention schemes, the International GP Recruitment Programme
(IGPR) and other retention schemes (3.56 FTE).
• Outflows include assumptions made for GP retirement and a general attrition rate of 15%.
• No change in the volume of locums frequently working across the system.
Nursing:
Marginal increase in FTE of Nursing staff from 2020/21 to end of year 2021/22, based on the following assumptions:
• Inflow assumption made for qualifying nursing students joining general practice via the GPN Fellowship
Programme.
• Inflow of Nurses via the introduction of a GP International Recruitment Scheme planned for 2021/22.
• Inflow based on the historic growth over the past three years of Advanced Nurse Practitioner (ANPs)
headcount and FTE.
• Outflows include assumptions made for Nursing retirement and a general attrition rate of 15%.
Direct Patient Care Roles (Additional Roles Reimbursement Scheme (ARRS) Funded):
• Significant increase in staff employed via the ARRS from 2020/21 to EOY 2021/22 based on the following
assumptions:o Inflow of planned recruitment for all PCNs across the system, including a margin for roles not recruited
to in 2020/21.
o 5% attrition applied to each ARRS role based on the 2020/21 FTE totals.
Direct Patient Care Roles (non-ARRS funded):
• No change in DPC staff employed outside of the ARRS.
• 5% attrition applied in tandem with ARRS roles.
Admin and Non-Clinical:
• No change in Administrative and Non-Clinical, based on historic data trends since 2015.
Actions Recruitment, retention and integration of new roles in primary care is a critical focus for MSEH&CP. The approach is
being driven through "place" based transformation across the four places in MSEH&CP, working closely with our
central workforce team.
ARRS Roles
• Place-based planning and ownership – the four 'places' in MSEH&CP have identified ARRS recruitment as
a critical priority for 2021/22. As a result, increased capacity will support the PCNs plan, recruit and embed
new roles. The Alliance Directors and Chairs will provide leadership within place to deliver our stated
ambitions. In Q1, Place-Based Plans will be approved.
• PCN Clinical Director Accelerator Programme – Clinical leadership is paramount to the long-term success
of the ARRS recruitment. To enable PCN Clinical Directors to provide the required level of leadership, we
have established an "Accelerator Programme" that aims to provide facilitated support to the PCN CDs that will
both deliver a specific outcome (identified by the PCN CD) and offer leadership development. The first wave
of this programme will be undertaken in Q1 2021/22.
• Infrastructure to support the ARRS development – PCNs have identified physical space as a limiting
factor when recruiting roles via the ARRS. MSEH&CP is committed to working as a system to address this
issue (utilising wider estate where this makes sense). An initial workshop was held on 08/04/21. This work will
be continued throughout 2021/22.
• Support functions – the Clinical Commissioning Groups (CCGs) have established a number of support
functions to assist recruitment via the ARRS. This includes a workforce hub, a recruitment facilitator function,
external legal and accountancy advice. This comprehensive offer will be reconfirmed to PCNs in April 2021
and throughout 21/22 to address concerns raised.
• Workforce Planning – a requirement in the 2021/22 Direct Enhanced Service (DES) is for PCNs to submit
complete workforce plans to their respective commissioner, providing details of updated recruitment intentionsfor 2021/22. The workforce hub and commissioners will undertake this process to ensure PCNs are fully
supported to embed and recruit roles that support improved health outcomes and collaborative working.
Nursing Staff
• International Nurse Recruitment Programme – Implementing an integrated recruitment programme,
working in collaboration with secondary care, to support international nurses entering primary care across the
system.
• GPN Fellowships – continuation of NHSE/I's GPN Fellowship Programme, locally adapted to support newly
qualified nurse inflow into primary care.
• CPD - an array of continued professional development is available to support nurses in upskilling and
developing their core competencies, supporting retention and development.
GPs
• GP Fellowships – expansion of the current GP Fellowship Programme, working at scale with other ICS'
across the East of England, to deliver a programme which provides GPs with the skills to take leading roles in
PCNs and increase the retention of new to practice GPs.
• International GP Recruitment – recommencement of the IGPR Programme following limited activity during
the pandemic.
• Portfolio Working – support the retention of GPs in general practice by providing opportunities and training to
undertake portfolio opportunities.
• Peer Support and Networking – The First 5 Clinical Leads will continue to build their networks of GPs (within
5 years post qualification) delivering educational support, training and networking opportunities.
• Supporting Mentors Scheme – providing GPs with the opportunity to undergo a programme of mentoring.
Experienced GPs across the system have the opportunity to apply for training to become a mentor and work in
a portfolio way.
All Staff
• Expanding clinical placement capacity – the approval of training environments for all staff members (GPs,
AHPs and Nurses), allowing more trainees and students to undertake placements in accredited learning
environments across the system.
• Wellbeing and support – peer to peer coaching opportunities for all staff, networking and forums.
Risks and issues ARRS recruitment across MSEH&CP has not delivered forecast levels of recruitment in 2019/20 nor 2020/21 plans.
In 2020/21 our actual vs planned rate of recruitment was at 52% (133 WTE roles unrecruited). Support offers were
put in place to enable recruitment (e.g. work force hub, service planning, recruitment support, legal and accountancyadvice) however, these were under-utilised. By making this programme a key priority for ‘place’, the CCGs will
continuously work with primary care and wider stakeholders to ensure earlier recruitment to roles.
There is a risk associated with the type of roles being recruited as professions which already have recruitment and
retention concerns. Two key examples of this are paramedics (29 FTEs planned in 2021/22) and mental health
practitioners (21 FTEs planned in 2021/22). To mitigate this, we will work closely with other providers to look at
rotational roles and collaboration to secure the workforce for the system. This includes EEAST, EPUT and other
mental health providers.
Acute, Community and Ambulance – Charlotte Williams (acute), Stephanie Dawe/James Wilson (community), EEAST is a separate submission and not part
of this – as advised by Region
Assumptions Acute:
• Staffing of Critical Care and key services in preparation for further COVID-19 waves.
• Staffing of theatres to support and compliment temporary theatre (Vanguard) to maximise theatre capacity
and decrease waiting lists.
• Review of other vacancy hotspots and put plans in place to close the vacancy gap.
• Reduce reliance on bank and agency workforce by recruiting to vacancy gaps.
Community
• Staffing prioritised on RTT backlogs working across the three community providers as part of the collaborative
arrangements.
• Staffing of Long COVID-19 to continue
• A shift in focus of resource to recovery at home models away from bed-based settings.
Actions Acute:
Recruitment and training
• International recruitment (Nurse) – 41 critical care nurses resourced from India, with another ten to arrive
before the end of May 2021. Budget and project for 260 general nurses underway. Part of the funding
includes pastoral care for this group of staff.
• HCSW – 250 recruitment up to the 1st April 2021. Plan in place to close the 100 WTE gap.
• Medical staffing –Consultant led project to review MSEH&CP approach to resourcing of medical staff. Project
scope includes the review of job role and skills mix within medical workforce.
• Review of the retention offering for all staff within the Trust. This will be overseen by the Trust recruitment and
retention group.• Considering Artificial Intelligence (AI) to scope potential for shortening of recruitment process.
• Student/In training offer – build on how the Trust treats students in order to retain those who have trained with
us.
Creating flexibility to respond to a future wave (e.g. training of enhanced care specialists on ward who could support
CCU in escalation):
• Trained and upskilled circa 300 staff to work in specialist areas.
• Moving all staff onto e-roster to provide greater visibility and coverage.
• Review of all consultant job plans and implementation of e-job planning.
• Use of AI technology to free up working hours for better use in other areas (patient booking hub).
Plans for seven day working
• All essential/clinically critical services operating on a 7-day working basis.
• Scope to review clinics to be offered at weekends.
Community:
• Under MSEH&CP community collaborative, People stream led by single executive across three community
provider organisations to drive joined up recruitment and people response.
• Joint recruitment models across Community collaborative being developed.
• Passport arrangements to enable movement of staff.
• Joint campaigns with system wider partners to support vacancy gaps.
• Community Nursing review exploring longer term model and staffing requirements.
Risks and issues Acute:
Ability to recruit into speciality roles and departments.
Further COVID-19 restrictions on travel may risk international supply or delay plans already in place.
Community:
Ability to recruit into speciality roles and departments.
Further COVID-19 restrictions impacting on previously shielding staff.Mental Health- Mark Tebbs and Alex Green
Assumptions; Approach to recruitment
Our plan is to continue to adopt a multi-faceted approach to recruitment, including newly qualified staff, international
recruitment, retire and return and role specific recruitment drives as well as a continued focus on retention of existing
staff. Where there are hard to recruit areas, either geographic areas or specific staff groups, we have a range of
strategies to help find a solution, including skill mixing, CPD opportunities and accelerated development.
Recruitment strategy
• Newly qualified staff – MSE H&CP continues to develop the excellent support packages in place for both
students and newly qualified staff, and for university students and apprentices. Numbers of university students
taking roles within MSEH&CP has increased with 86 new nurses coming through last September. We are also
now seeing newly qualified staff coming through from our apprenticeship pathways, with 21 taking up qualified
roles within MSE H&CP last September. Future supply of staff from both pathways in more professions (e.g.
nursing, OT, psychology) looks set to increase over the coming years.
• Bank staff – MSEH&CP has focused on recruitment from bank to substantive roles, for example within the
HCSW role.
• International recruitment – MSEH&CP is looking to recruit overseas nurses this year to supplement existing
workforce and supply routes.
• Recruitment drives – MSEH&CP has had success with geographic specific recruitment drives as well as role
specific recruitment drives. Currently we are in the final stages of a recruitment drive for HCSWs with the aim
to fill all vacancies, and over recruit where possible.
Actions Below are some other headline initiatives:
• More placements to increase student recruitment along with a guaranteed job not only for nurses but also
psychology.
• Retention of staff approaching 55 years of age.
• Career conversations now form part of appraisal and supervision.
• Talent management hub being developed.
• Medical Clinical Fellowship offered by EPUT and working closely with ARU Medical School to encourage
psychiatry placements for future junior doctors in the region.
• Development of Advanced Clinical Practitioners (ACP) and Physician Associate (PA) roles within clinical
teams/services.
• Momentum of volunteer workforce - training, routes into employment.• Promoting opportunities for system working and support - rotational posts, shared learning opportunities and
programmes, system placements, joint posts, joint initiatives on talent pipeline.
Risks and issues Risks to recruitment and our approach to deal with the hard to recruit to posts
As with many NHS Trusts, the risk to recruitment is the lack of supply of qualified staff with many Trusts looking and
offering similar roles to the same small group of people. This is made more difficult due to the location of Essex,
bordering on the English Channel and the River Thames to the east and south respectively, and proximity to London
to the west offering more financially attractive employment.
Our apprenticeship offering is one key element for MSEFT in tackling this. We now have a range of clinical and non-
clinical apprenticeships, an example being a pathway from a healthcare assistant to a fully qualified nurse, available
within MSEFT.System name: Mid and South Essex Health and Care Partnership
A. B. Continuing to meet the needs of patients with Covid-19 – Stephanie Dawe and James Wilson
Please set out the specific actions that, as a system, you will prioritise over the next 6 months to address the objectives below
Preparations for any future potential surge • The Mid and South Essex System has well-rehearsed plans to increase and expand the use of its
requirements for Covid patients community bed base including enhancing the acuity of patients that can be supported on the
wards at short notice. Although as a system the focus of our reset and recovery is testing more
home first ‘virtual ward’ approaches rather than traditional community ward settings for the majority
of our patients, we are still agile enough across the system to increase capacity as required.
• Specifically, for COVID-19 patients, in early 2021, COVID-19 Virtual Wards and Clinical Oximetry
at Home (with onboarding via 111, primary care and community) models were mobilised across
the Mid and South Essex system. A system strategy is being developed to translate the COVID-19
response capacity into ‘business as usual’ capacity to support individuals with non-COVID-19
breathlessness symptoms and wider applications, with the flexibility to re-focus back to support
COVID-19 needs and demand as a priority.
• It is recognised that PCNs have an important ongoing role in response to the pandemic which will
involve the continued use of home oximetry, alongside hospital-led ‘virtual wards’, proactive care
pathways delivered virtually in people’s homes. This will be considered as they continue to prepare
for any future potential surge requirements for COVID-19 patients. A working group to support this
endeavour is being established April 2021, in collaboration with a sub-group of the MSE Digital
Programme dedicated to remote monitoring digital solutions.
• Data reporting and regular monitoring is being established across system for the Virtual Ward and
Oximetry at Home models to allow early identification of rising activity and allow timely escalation
and flexibility of services back to COVID-19 priorities. This reporting will go live in April 2021.
Operational monitoring groups will continue to meet and agree criteria for escalation of services in
response to COVID-19; further actions will be agreed as and when required.
This is supported by movement of management of all COVID-19 care response services under the remit
of the MSE Respiratory Transformation Programme, the structure of which is in line with the East of
England Regional Clinical Network. The MSEH&CP have named contacts for support in national and
regional forums.
Pathway in place for admission avoidance and early facilitated discharge utilising remote monitored home
pulse oximetry for COVID-19 positive patients. Wave 2 utilisation demonstrated clinical safety of the
approach and mitigated against four to five beds per day of respiratory surge occupancy at Level One.
Investment cases in development for the expansion of core Critical Care and Acute Respiratory Care Unit
(ARCU) capacity to ensure adequate baseline teams and to enable better supported surge expansion withmuch reduced impact to elective programme activities. Gateway One Target to expand by five Level
Three beds and 14 Level Two beds within Critical Care and ARCU across the MSE.
In-Hospital streaming pathways in place for segregation of patients and reduction of cross-infection,
reviewed by Care Quality Commission (CQC) during Infection Prevention and Control inspection at the
Basildon Hospital site.
Provision of timely and equitable access to Mid and South Essex implemented a Long COVID-19 Clinic on 14th December 2020 but had to pause the
Post Covid Syndrome (‘Long Covid’) service two weeks later due to the system-wide OPEL-4 status in response to the COVID-19 pandemic.
assessment services. Paul Taylor Once the OPEL status was de-escalated the clinics recommenced on Monday 22nd February 2021. The
clinic operates video call assessments in usual office hours, five days a week, using the Airedale Holistic
Assessment tool. Following assessment, cases are either signposted to an appropriate specialist service
or reviewed by the multidisciplinary team in a virtual clinic.
• At present the referral rates into the clinic are outstripping capacity and there is a waiting list of 114
people. This surge in numbers is likely to be the result of the large numbers of cases seen in Mid &
South Essex approximately 12 weeks ago. The curve in Long COVID-19 incidence numbers will
echo the number of positive COVID-19 cases seen 12 weeks ago, so it is anticipated that referrals
will begin to slow in the next few weeks. In response to the current Long COVID-19 surge, clinic
capacity has been doubled from 12th April 2021 for three weeks. Referral rates and waiting times
will be closely monitored so action to redress long waiting times can be taken swiftly if needed.
• The Mid and South Essex financial allocation for Long COVID-19 clinics for 2021/22 has been
confirmed at £474k. Financial modelling and service specification development is underway to
ensure the service will meet the volume of cases and develop unacceptable waiting times for first
appointments.System name: Mid and South Essex Health and Care Partnership
B. C1. Maximise elective activity, taking full advantage of the opportunities to transform the delivery of service – Andrew Pike and Karen Wesson
Please summarise the key assumptions that underpin the activity plan submission, highlighting any key risks and issues. Please also set out any
system actions that are critical to the delivery of the planned activity levels. – Please ensure response includes collaboration between primary care
and secondary care, effective prioritisation, patient communication
Elective Spells
Assumptions
The pandemic has had a significant impact on the delivery of elective care and, as a result, on the lives of many
patients who are waiting for treatment. The system is aiming to recover towards previous levels of elective
activity and beyond where possible, and is planning for the highest possible level of activity across the system
(including via the Independent Sector) on the basis that additional funding above core envelopes with be
available from the additional £1bn Elective Recovery Fund for 2021/22.
CCG Activity assumptions:
The CCGs have been working jointly with MSEFT in their plans to address the significant elective recovery
programme. In addition to maximising the use of existing capacity within the MSEFT as set out above, a
considerable effort has been placed on securing as much Independent Sector capacity as possible for the
system to be utilised, for both eRS patient Inter Provider Transfers from MSEFT, against a backdrop of their
own private patient waiting lists being at an all-time high.
The CCG model which has informed the functional template has taken the following assumptions:
• The model has been built using the MSEFT activity assumptions as set out above, the agreed
indicative activity plans agreed with the Independent Sector Providers under the Increasing Capacity
Framework, and modelled assumptions regarding the activity at other NHS and in-scope Non-NHS
providers.
• The model assumes that Independent Sector Providers can deliver 139% of 2019 baseline elective
activity in H1.
• The output of the model is that the CCG total activity undertaken will meet 106% of 2019 baseline
elective activity for H1.• Current model assumes capacity remains stable (i.e. no COVID-19 or other incident impacts on this).
MSEFT Activity assumptions:
For 2021/22 the system has built the MSEFT elective model so that any change can be added allowing for the
future forecasting of impact e.g. if activity reduces due to fourth wave of COVID-19. The model used
demonstrates the sensitivity to capacity changing in year and shows that with current productivity post COVID-
19 MSEFT can only reduce the 52 week number if the current planned capacity remains.
The model which has informed the functional template has taken the following assumptions:
• That the activity undertaken must meet at least 90% of 2019 baseline activity.
• Current model assumes 100% capacity remains (i.e. no COVID-19 or other incident impacts on this) so
as to enable the following approach to modelling 52 week recovery (performance at 14 April 2021 for
52 week wait patients exceeds 8000).
• Waiting list has been calculated using projected activity based on capacity available remaining and
forecast clock stops. This modelling results in a 2021/22 year end position of circa 5500 patients
waiting over 52 weeks.
• Following agreement of a backstop position with Region, the system is working to deliver a H1
backstop position of zero long waiting patients over 98 weeks. The ambition for the system is to
achieve that no patients wait longer that 90 weeks by July 2021.
• The model shows that if the clock stops after 6 months, or activity is lost due to a further COVID-19
surge, or there is a marked change in referrals there is a risk that those waiting over 52 weeks could
rise over 8000.
• The model is built up from each specialty i.e. the overall MSEFT position is a summation of each
specialty.
• Demand in the model is based on the cumulative average weekly number of patients whose RTT
wait ‘tip in’ to the backlog 52+ week wait cohort, seen since week ending 15th November 2020.
• Clock stops: for patients waiting 52+ weeks, based on either:
o Cumulative average percentage of total planned clock stops from week ending 15th
November 2020 or a specific percentage has been used, based on efficiencies thought to
increase the proportion from the baseline for example extra work undertaken in
orthopaedics.
o Additional recovery capacity through either: Inter Provider Transfer to Independent Sector
Providers (ISP); Insourcing; and additional Vanguard Mobile Theatres with assumptions
around the proportion of this additional capacity used for patients with an RTT wait of 52+
weeks.Collaboration between primary care and secondary care Across the planned care programme and pathway development work, we have been working collaboratively both with our primary care, MSEFT colleagues and Tier 2 providers to resolve pathway challenges. This collaborative working has been successful in developing plans and agreeing approaches to primary care practice communications, developing pathways and understanding “tricky” issues, for example when work was in progress to address the ASI issue and redirection to primary care/Tier 2 a working group was established to support understanding and communication with primary care colleagues. We have primary care leads aligned to each of the pathways who are working with acute and Tier 2 colleagues. Effective prioritisation MSEFT on average treat/clock stop circa 4,000 patients per week. If MSEFT only treated patients chronologically instead of applying the Royal College of Surgeons (RCS) clinical prioritisation criteria both the 104+ and 78+ week backlogs could be cleared relatively quickly within a couple of weeks however this would be at the detriment of those who were identified as having greater clinical priority. The complexity of recovery lies in triaging patients based on clinical need as well as chronologically. Patient communication Through the MSEFT work programme patient communication materials are being developed to ensure we update patients and keep them informed about changes, use of virtual technology for outpatients, waiting times etc. Work with Healthwatch has been undertaken to ensure that themes are picked up and managed via patient communications. Through the clinical prioritisation work and validation against the Service Restriction Policy, patient letters will be tailored to the patient specific pathways to ensure that they inform the patients as to the rationale for any decision or change in their pathway. Cancer – please see cancer section. Further impact from COVID-19 on Elective Activity
Assumptions
We have explored the findings from Imperial College and Warwick modelling so far. This modelling considers a
range of factors, those most influential to hospitalisations are the R value and the relaxation of lockdown.
Vaccine efficacy and hesitancy are key factors which play a larger role in modelling this time.
Imperial have suggested that the East of England may be likely to experience fewer hospitalisations and
deaths in wave 4 as a result of experiencing higher levels in waves 1, 2 and 3.
“Regions which were worst hit by the epidemic so far (for example the East of England and London)
are projected to experience much fewer cases, hospitalisations and deaths than other regions”.
(Imperial College COVID-19 response team)
Our initial modelling uses both the Imperial and Warwick models to understand what the expectation will be for
the size of wave 4 relative to the size of our wave 3. This is the very first step in modelling the wave 4 size.
Our very initial modelling explores the impact if we experience a similar wave to wave 1 again, if we were to
experience 55% of wave 3 and a more pessimistic model if we experience 70% of wave 3. This helps illustrate
what we think the model could look like once all assumptions are built.
Further work is currently in progress to develop some robust local assumptions to help us model wave 4 based
on factors such as local transmission, vaccine uptake and efficacy. This will be completed for the final
submission.
Actions System actions that are critical to the delivery of the planned activity levels are outlined below:
• Ensure capacity secured within the Independent Sector is fully maximised through eRS and Inter
Provider Transfer, through active monitoring and communication with the ISP providers, and weekly
review of any potential issues that may impact on throughput.
• Operational leads and service managers are reviewing their theatre capacity to understand how
quickly the patients waiting can be slotted in. This review will include efficiencies to increase the
proportion/number of treatments for patients waiting over 78 weeks through:
o Optimise capacity for chronological booking after prioritisation.
o Ensure Inter-provider transfers to identified additional capacity at Independent Sector
Providers are strictly transferred in chronological order for priority 3 and 4 procedures.
o Identify any opportunities for Tier II provider capacity where activity can be outsourced to
release acute capacity (determined by treatment required). This has been beneficial to date
for cystoscopy, dermatology procedures, hysteroscopy, some MSK activity, ophthalmology.• Use part of the weekly PTL meeting to individually track those waiting over 78 weeks, enabling
specific actions, plans to be developed to support recovery.
• Priority patients (whose intended procedure is categorised as priority 1 and priority 2) to be
identified and scheduled first.
• Service leads to validate all patients (whose procedure are categorised as priority 3 or 4 by
specialty) waiting 78+ weeks against the Service Restriction Policy.
• Service Restriction Policy adherence:
o Patients listed not meeting the clinically evidenced criteria for the procedure, or with no
funding approval will be followed up to identify a more appropriate pathway to be sought or
removal of patient from the list (with appropriate communication to the patient and primary
care) this in turn will release capacity for patients meeting clinical need.
• Mobilise additional capacity within the system:
o Braintree – this community hospital was released to support COVID-19 response providing
community intermediate care beds. The plan is for this to return to becoming an acute
facility to support up to an additional 50 patients to be treated per week (based on Phase 3
planning).
• Vanguard theatres – MSEFT on behalf of the system have been successful in securing mobile
theatre space for Half 1 (H1) of 2021/22. This will enable mobilisation and commencement date of
early June 2021.
• Critical care capacity – increase capacity based on numbers required as part of the COVID-19
surge, business case being developed for MSEFT governing body approval June 2021. Planning
is still being progressed to inform the Business Case.
Transforming Services – Stewardship
We want to change how we care for people in Mid and South Essex Health and Care Partnership and have
developed an innovative approach we are calling ‘stewardship’. Instead of each organisation or sector
determining their offering and then co-ordinating with others, a stewardship team for each service area will
start by considering MSE’s population health needs overall. Stewardship teams will strive to deliver truly
integrated care, benefiting in their decision-making from data and perspectives from clinical and non-clinical
professions, localities (i.e. Local Authority and Alliance Board representatives), health and care sectors and
patient voices.
We have brought together six stewardship groups in:• Care of the elderly
• Respiratory
• Stroke
• Emergency Medicine
• Cancer
• Cardiology
Each group has engaged in two initial facilitated discussion events, exploring the conceptual and practical
aspects of adopting a stewardship approach within their service area.
To deliver change at scale and the pace required we must first wrap a leadership support package with access
to Subject Matter Experts around the group as below:
• The support package will cover leadership and coaching from the Staff College including master-
classes with Subject Matter Experts e.g. Population Analytics, Business Intelligence Lead and
Analysts provided by the MSE Strategy Unit and ICS Data & Intelligence Hub including insights and
modelling; research Fellow/contract with UCL Partners or similar, for rapid appraisal of applied
health research; finance and forecasting via the Chief Finance Officers.
We have developed a four month plan with a view to service line plans for April 2022 expecting that during this
time the cohorts will develop quick wins and programmes of work.
This work is approved by the Executives across the system and will be supported by the Mid and South Essex
Partners Support Team.
Elective System Programme
We are in the process of pulling all elective projects into one programme with our system partners.
Pre assessment digital platform group
Braintree model for elective Orthopaedics as described in our activity modelling.
Our pre assessment team now have access to the acute care portal and SystmOne which joins up system
working.
GynaecologyReinforcements of pathways and referral acceptances to ensure all steps in the pathway are completed before
referrals are accepted into the acute. We are reviewing all activity that could be done in a community setting;
the long-term vision is for a community women’s clinic in conjunction with primary care to undertake
procedures which could be done in primary care e.g. coil fitting and removal.
Orthopaedics
Reviewing referral criteria and pathways, including the use of best practice models of referral management e.g.
physio led initial assessment, first line pain management and appropriate onward referral to surgeon led
services. The service aim is to establish a single MSK triage hub for all GP referrals.
We are benchmarking against best in class length of stay for elective procedures and developing
transformation initiatives to for the four sites (Basildon, Southend, Broomfield and Braintree).
We are using the environment of an elective orthopaedic unit (Braintree) to deliver high standards of pre, peri
and post-operative care and rolling out best practice across all sites.
Reviewing and standardising post-operative care pathways across the system ensuring seamless transition of
care from acute to community:
• Maximising opportunities for converting in-patients to day cases thereby releasing bed capacity for
additional throughput.
• Standardisation of virtual fracture clinic pathways.
• Standardisation of prosthesis and equipment across MSEFT.
High Volume Low Complexity Model
Within this programme we will review High Volume Low Complexity (HVLC) Models. Learning from the London
Elective Surgery Recovery and Transformation Programme we will develop our HVLC work.
We will draw on our Get It Right First Time (GIRFT) recommendations using Model Hospital and other
methods to benchmark.
Our strategic partners, PWC, are working on system financial efficiency; the data will be used with robust
activity monitoring tools to rapidly identify core procedures to focus on, standardise and use best practice to
deliver better outcomes for patients. We will, as with our ophthalmology transformation work, set up system
pathway groups to deliver change.
TheatresYou can also read

















































