2021 Healthcare Coalition Preparedness Strategy Trauma Service Area D (TSA-D)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
2021 Healthcare Coalition Preparedness Strategy
Trauma Service Area D (TSA-D)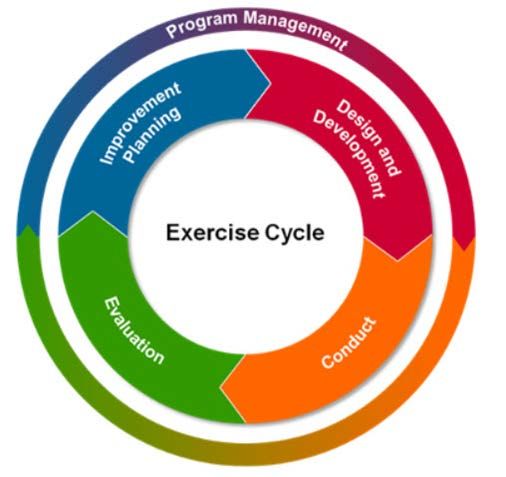
Record of Revision and Distribution
This document reflects the ongoing work and refinement of Trauma Service Area D Healthcare
Coalition’s regional strategies for emergency preparedness and disaster response. The
document will be revised annually to reflect the continuous process improvement.
Date Preparedness Strategy Approved:
Table 1. TSA-D’s Healthcare Coalition Record of Revision
Date Summary of Revision Reviser
10/20/2017 Template Built Shane Comer
12/21/2017 Draft Adapted and Angela Baker
Completed
3/5/2018 Draft submitted to HCC for
Comment
3/27/2018 Preparedness Strategy
Vote
Approve: 12
Reject: 0
Abstention: 10
12/5/18 Draft submitted to HCC for Toby Harbuck
comments
12/17/18 Comments and new Toby Harbuck
requirements added
1/24/19 Preparedness Strategy Toby Harbuck
Vote
Approved by Executive
Committee
Approve: 5
Reject: 0
Abstention: 0
3/12/20 Preparedness Strategy Toby Harbuck
Vote
Approved by Executive
Committee
Approve: 5
Reject: 0
Abstention: 0
Table 2. TSA-D Healthcare Coalition Preparedness Strategy Record of Distribution
To Whom: Person/Title/Agency Method of Delivery Date
Coalition Members Email 3-12-20
Coalition Executive Board Email, In-Person 3-12-20
Coalition Members Email, Web-Site 12-10-20
Coalition Executive Board Email, In-Person 12-17-20
2
Table of Contents
Introduction .............................................................................................................................. 4
Preparedness Strategy ............................................................................................................ 4
Healthcare Coalition Purpose............................................................................................................... 4
Mission Statement.................................................................................................................................. 4
Vision Statement .................................................................................................................................... 4
Scope ....................................................................................................................................................... 4
Funding..................................................................................................................................... 4
Operational Planning ............................................................................................................... 5
Operational Planning Process .............................................................................................................. 5
Hazard Vulnerability Analysis (HVA) ................................................................................................... 6
THIRA ...................................................................................................................................................... 6
HPP End of Year Survey....................................................................................................................... 6
Regional Partner Input via HSEEP ...................................................................................................... 7
Emergency Medical Task Force-2 ....................................................................................................... 7
Planning Assumptions ........................................................................................................................... 9
Health Care Coalition Members .............................................................................................10
Governance .............................................................................................................................10
Program Priorities ...................................................................................................................11
Gap Analysis ......................................................................................................................................... 12
TSA-D HCC Preparedness Objectives ............................................................................................. 13
Appendix A: HVA.................................................................................................................................. 16
Appendix B: HCC Member List .......................................................................................................... 19
Appendix C: TSA-D Healthcare Coalition Governance .................................................................. 20
Appendix D: ASPR Coalition Assessment Tool .............................................................................. 25
Appendix E: HPP Letter of Agreement ............................................................................................. 27
Appendix F: Acronyms ........................................................................................................................ 34
3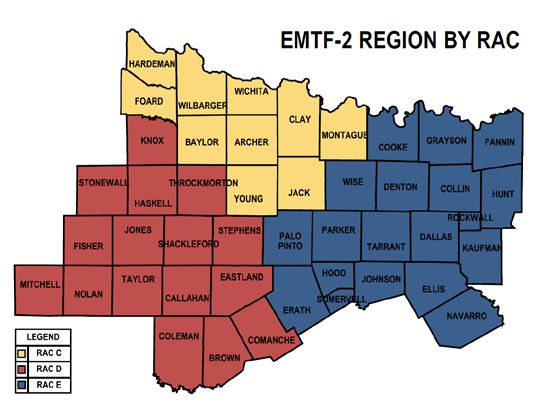
Introduction
This document provides the strategic framework that will guide the development of Trauma
Service Area D (TSA-D) Healthcare Coalition’s healthcare system preparedness, disaster
response and recovery activities. This plan was developed with input from leaders representing
hospitals, emergency medical services, public health, and emergency management agencies in
Trauma Service Area-D.
Preparedness Strategy
Healthcare Coalition Purpose
The TSA- D Healthcare Coalition (TSA-D HCC) is a network of healthcare providers that are
committed to coordinating and improving emergency preparedness and response activities in
alignment with the Health Care Preparedness and Response Capabilities established by Office
of the Assistant Secretary for Preparedness and Response (ASPR). The coalition is comprised
of representatives from the four core member types, Hospitals (public and private,) EMS,
Emergency Management offices, and Public Health Departments. It serves as a multi-agency
coordination group to assist Emergency Management with preparedness, response and
recovery activities related to health and medical disaster operations. The Coalition also
maintains the Regional Medical Communications Center for TSA-D.
The Coalition works to augment local operational readiness to meet the health and medical
challenges posed by a catastrophic incident or event. This is achieved by engaging and
empowering all parts of the healthcare community, and by strengthening the existing
relationships to understand and meet the actual health and medical needs of the whole
community.
Mission Statement
To support the development of cooperative partnerships in order to strengthen, promote and
enhance the well-being of the community’s healthcare system through coordinated disaster
preparedness training, education, public information, response/recovery activities, and the
sharing of resources.
Vision Statement
A Healthcare Coalition comprised of members who actively contribute to the HCC strategic
planning, identification of gaps and mitigation of strategies, operational planning and response,
information sharing and resource coordination to enable the healthcare delivery system in the
region is able to effectively provide a whole community based response that coordinates efforts,
before, during and after emergencies; continues operations; and appropriately surge as
necessary.
Scope
This plan does not replace regional or organizational emergency operations plans. It serves as
a guide for regional planning, and exercise and training development.
Funding
Funding for Healthcare Coalition development and sustainment is provided by the U.S.
Department of Health and Human Services, Office of the Assistant Secretary for Preparedness
and Response (ASPR), Healthcare Preparedness Program (HPP) Cooperative Agreement
4
and/or the Centers for Disease Control and Prevention (CDC) Public Health Emergency
Preparedness (PHEP) Cooperative Agreement (Agency Funding Opportunity Number CDC-
RFA-TP12-1201; Catalog of Federal Domestic Assistance Numbers 93.889 - National
Bioterrorism Hospital Preparedness Program; and, 93.069- Public Health Emergency
Preparedness; Texas Department Of State Health Services Contract No. 537-17-0307-00001
Under The Hospital Preparedness Program (HPP) Grant.
Current funding through 2022 is focused on the development and sustainment of Healthcare
Coalitions through:
1. Continued improvement of infrastructure- Help community-based healthcare providers
prepare for disasters with a public health impact.
2. Capability-based planning: Funding supports the National Health Security Strategy and
follows a capabilities-based approach. ASPR has identified the following four
capabilities that outline the high-level objectives that the Coalition should undertake to
prepare for, respond to, and recover from emergencies:
Capability 1: Foundation for Health Care and Medical Readiness
Capability 2: Health Care and Medical Response Coordination
Capability 3: Continuity of Health Care Service Delivery
Capability 4: Medical Surge
3. Community Risk Assessment- A central component of implementing a capability-based
approach to preparedness and response includes jurisdictional risk assessments that
identify potential hazards, vulnerabilities, and risk within the community that relate to the
public health, medical, and mental/behavioral systems inclusive of at-risk individuals.
4. Leveraging resources- Healthcare Coalition partners enhance a community’s response
capability through shared planning, organizing/equipping, training, exercise and
evaluation activities related to disaster operations.
5. Staged approach- Healthcare Coalitions function at the community level based on
existing partnerships in place and their relationship to their regional domestic security
structure. In the end, Healthcare Coalitions should be able to effectively and efficiently
demonstrate multi-agency coordination during response through exercises and real-life
incidents.
Operational Planning
Operational Planning Process
The Trauma Service Area D Healthcare Coalition planning group establishes its program
priorities based on the results from the Hazard Vulnerability Analysis (HVA), a locally developed
Threat & Hazard Identification and Risk Assessment (THIRA), the HPP End of Year Survey,
regional partner input, and After Action Reports.
Once regional priorities are established based on identified capability gaps, the Multi-Year
Exercise and Training Plan is developed to bring improvement to those areas.
A major component of TSA-D’s evaluation of the improvement process is derived from the After
Action Reports and Improvement Plans that follow the Homeland Security Exercise and
Evaluation Program (HSEEP.)
5Hazard Vulnerability Analysis (HVA)
The TSA-D Healthcare Coalition conducts a regional Hazard Vulnerability Analysis annually.
TSA-D HCC distributed a Hazard Vulnerability Analysis survey to hospitals for them to input
their hospital’s risk assessment data. The survey was comprised of four hazard categories
(Natural Hazards, Technological Hazards, Human Hazards, and Hazardous Materials). For
each category, the participants were asked to score each event type according to the probability
of the event occurring and the severity of the event based on six factors, (Human Impact,
Property Impact, Business Impact, Preparedness, Internal Response, and External Response).
From the facilities self‐reported scores, each event was assigned a corresponding risk
percentage. The assessment provided the top three hazards by type and top ten hazards as
seen below.
Table 3. Top Ten Hazard Vulnerability Analysis Regional Results
2020 Top Ten Hazard Vulnerability Analysis Regional Results
1) Tornado
2) Active Shooter
3) Inclement Weather
4) Seasonal Flu
5) Drought
6) Communication Failure
7) Mass Casualty Incident
8) Temperature Extremes
9) Chemical Exposure, External
10) Power Outage
The full HVA can be found in Appendix A.
THIRA
The 2019 Regional Threat and Hazard Identification Risk Assessment completed by the West
Central Texas Council of Governments for our region was utilized to assess hazards. The
WCTCOG THIRA identified the following as threats and hazards for the region:
Threats and Hazards
1. Wildfire
2. Hazardous Chemical Release
3. Active Shooter
4. Infectious Disease Outbreak
5. Water Main Break
HPP End of Year Survey
The HPP End of Year survey is an assessment presented to coalition members. The 2017
assessment served as the Baseline Assessment for the five-year program period and provide a
multi-year data trend of information. Based on the HPP YR 15 End of Year Survey, the
6following needs were identified by coalition members as training priorities and are listed in order
of priority:
1. HICS/Hospital EOC
2. WebEOC
3. NIMS
4. COOP and Recovery
5. Patient Tracking
Regional Partner Input via HSEEP
The Homeland Security Exercise and Evaluation Program (HSEEP) provides a set of guiding
principles for exercise programs, as well as a common approach to exercise program
management, design and development, conduct, evaluation, and improvement planning.
Exercises are a key component of national preparedness, as they provide elected and
appointed officials and stakeholders from across the whole community with the opportunity to
shape planning, assess and validate capabilities, and address areas for improvement. The
cyclic nature of HSEEP, as illustrated below, makes it a very useful tool in gauging effectiveness
of training and exercises in improving established capability gaps and regional priorities.
Emergency Medical Task Force-2
1. Overview
A. TX EMTF is a regional and statewide medical response capability. NCTTRAC serves as
the lead agency for administration of the EMTF-2 Program for North Central Texas
(TSA-E – DFW), North Texas (TSA-C – Wichita Falls), and West Central Texas (TSA-D
– Abilene). TX EMTF elements will stand ready to provide medical surge support
throughout the State of Texas, and regionally as requested for mutual aid. Designated
EMTF-2, the regional task force is capable of providing ambulance buses, mobile
medical units, nurse strike teams, ambulance strike teams, Ambulance Staging
Management, Medical Incident Support Teams (MIST), and Infectious Disease
Response Units (IDRU). When called upon by the State, teams and assets will deploy
7with costs reimbursed by the State. When called upon locally or regionally, costs must
reimbursed by the receiving jurisdiction, or be absorbed by the providing agency.
Figure 2: EMTF-2 Region by RAC
2. Mission
A. Emergency Medical Task Force Region 2 (EMTF-2) is designed to respond to disasters
or events to provide care and/or transportation. EMTF-2 resources may be requested by
contacting NCTTRAC or local Disaster District Chair (DDC).
B. The mission of EMTF-2 is to augment and support the needs of an impacted community
with temporary healthcare infrastructure configured to meet incident needs.
C. EMTF-2 will ensure that member agencies and deployment personnel are adequately
prepared to perform at their highest level under the dynamic and often adverse
circumstances faced in disaster medical operations. In order to facilitate this readiness,
EMTF-2 will utilize the EMTF Coordinator to assist in ensuring the highest level of
preparedness for the EMTF all-hazard response.
3. EMTF-2 Organizational Structure
A. The goal of the Texas EMTF program is to provide a well-coordinated response, offering
rapid professional medical assistance to emergency operation systems during large-
scale incidents. Eight Emergency Medical Task Forces can be rostered across Texas.
B. EMTF-2 consists of eight components:
1. Task Force Leadership
2. Ambulance Buses (AMBUS)
3. Ambulance Strike Teams (AST)
4. Ambulance Staging Management Teams (ASM)
85. Medical Incident Support Teams (M-IST)
6. Mobile Medical Units (MMU)
7. Registered Nurse Strike Teams (RNST)
8. Infectious Disease Response Unit (IDRU)
C. EMTF-2 TSA-D Members
1. Sweetwater Fire and EMS
2. Heart of Texas EMS
3. Mitchell County EMS
4. Stonewall County Ambulance Service
Planning Assumptions
The TSA-D Healthcare Coalition will use the National Incident Management System (NIMS) as
a basis for supporting, responding to, and managing activities and will have on-going training to
help keep healthcare providers up to date. In order for there to be a smooth transition between
local, regional and State operations, it is essential that all organizations are able to understand
the NIMS structure to managing incidents.
The following assumptions will be made for the TSA-D HCC:
1. Emergency and disaster incidents affecting TSA-D organizations will be managed on the
local level until the need exceeds local resources, at which time the Regional
Emergency Operations Plan will be implemented to access regional resources.
2. If the need exceeds available regional resources, then State resources will be accessed
through the Texas Department of Emergency Management Disaster District Coordinator
(Greg Goettsch) for TSA-D.
3. HCC members will take advantage of training opportunities to prepare for disaster and
medical surge events
4. HCC members will participate in the CST and other exercises to prepare for disaster and
medical surge events
5. HCC members will keep HPP inventory updated and serviceable in preparation for any
disasters or medical surge events
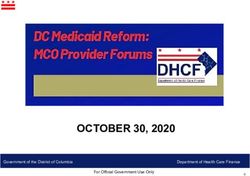
TSA-D HCC Regional Boundaries
The geographical area served by TSA-D HCC includes sixteen counties (Brown, Callahan,
Coleman, Comanche, Eastland, Fisher, Haskell, Jones, Knox, Mitchell, Nolan, Shackelford,
Stephens, Stonewall, Taylor and Throckmorton) and all municipalities within. The TSA-D HCC
strives to improve an all-hazard medical response in West Central Texas through effective
communication, planning, coordinated exercises, and collaboration between regional health
care organizations, emergency responders, local/regional emergency management directors,
public health and other emergency response planners.
9Health Care Coalition Members
Membership in the HCC is typically composed of (but not limited to) the following
groups:
1. Hospitals
2. EMS Agencies
3. Emergency Management Organizations
4. Public Health Agencies
5. Jurisdictional Emergency Management Partners
6. Outpatient Health Care Delivery Facilities
A full list of current HCC members can be found in Appendix C.
Governance
The TSA- D coalition is a network of healthcare organizations and providers that are committed
to coordinating emergency preparedness and response activities through the following roles and
responsibilities. The HCC comprises representatives from hospitals, EMS, public health,
emergency management, and other key partnering agencies, which serves as the governance
10body. The HCC meets monthly, with any ad hoc meetings occurring as needed. The HCC
governance can be found in Appendix B.
Program Priorities
The Trauma Service Area D Healthcare Coalition MYTEP planning group will focus its program
on the priority capabilities that need to be in place to meet the top threats facing the
organization as identified in the locally developed Threat & Hazard Identification and Risk
Assessment (THIRA), ASPR Coalition Assessment Tool High Priority Recommendations,
comply with any related grant-based requirements and improve the overall preparedness and
response capabilities of the organization.
The TSA-D Healthcare Coalition’s overall healthcare system preparedness will be achieved
through a continuous cycle of planning, organizing and equipping, training, exercises,
evaluations and corrective actions.
Based on the preceding planning principles, the TSA-D Healthcare Coalition has established the
following to be regional priorities for this year:
1. Pandemic/HCID Response
2. CBRNE Response
3. Health Care and Medical Response Coordination
4. Continuity of Operations and Recovery
11Gap Analysis
Gaps have been identified from the CST AAR/ IP, ASPR Coalition Assessment Tool, and
lessons learned from the HCC.
Table 4. TSA-D HCC Gap Analysis
HPP Capability Gap Corrective Action Capability Element
Capability 1: 1) Identifying Risks Complete Coalition Planning
Foundation for Health and Needs Supply Chain
Care and Medical Integrity Survey.
Readiness
1) Notification to the Create a Regional Planning
Healthcare Response Plan.
Coalition of an
Evacuation.
2) Incorrect contact Ensure Correct Planning
information within Information is shared
the HCC. with regional
Capability 2: Health healthcare facilities
Care and Medical and in the Regional
Response Response Plan.
Coordination
Conduct Drills and
Exercises to maintain Training
functionality.
Conduct
3) EMResource EMResource training. Training
operations.
Capability 3: 1) CBRNE Complete RRS Training
Continuity of Health Response. Decontamination
Care Service Training.
Delivery
1) Delayed EMS Create a resource Planning
Communication. document with all
EMS contact
numbers.
Capability 4: Medical
Surge Review previous Planning
2) Pandemic/HCID
Response HCID plan to ensure
capability continues
without an
assessment center in
the region.
The Capability Planning Report can be found in, Appendix D
12TSA-D HCC has adopted an all-hazards approach that focuses on the development of
capabilities necessary to respond and recover from any hazard. In 2017 the Office of the
Assistant Secretary for Preparedness and Response (ASPR) identified four capabilities as the
basis for health care system, Healthcare Coalition, and health care organization preparedness:
1. Foundation for Health Care and Medical Readiness
Goal of Capability 1: The community’s health care organizations and other
stakeholders—coordinated through a sustainable HCC—have strong relationships,
identify hazards and risks, and prioritize and address gaps through planning, training,
exercising, and managing resources.
2. Health Care and Medical Response Coordination
Goal of Capability 2: Health care organizations, the HCC, their jurisdiction(s), and the
ESF-8 lead agency plan and collaborate to share and analyze information, manage
and share resources, and coordinate strategies to deliver medical care to all
populations during emergencies and planned events.
3. Continuity of Health Care Service Delivery
Goal of Capability 3: Health care organizations, with support from the HCC and the
ESF-8 lead agency, provide uninterrupted, optimal medical care to all populations in
the face of damaged or disabled health care infrastructure. Health care workers are
well-trained, well-educated, and well-equipped to care for patients during
emergencies. Simultaneous response and recovery operations result in a return to
normal or, ideally, improved operations.
4. Medical Surge
Goal of Capability 4: Health care organizations—including hospitals, EMS, and out-
of-hospital providers—deliver timely and efficient care to their patients even when the
demand for health care services exceeds available supply. The HCC, in
collaboration with the ESF-8 lead agency, coordinates information and available
resources for its members to maintain conventional surge response. When an
emergency overwhelms the HCC’s collective resources, the HCC supports the health
care delivery system’s transition to contingency and crisis surge response and
promotes a timely return to conventional standards of care as soon as possible.
TSA-D HCC Preparedness Objectives
The Healthcare Coalition has both long-term goals and short-term objectives. Long-term goals
are expected to be met within a five-year period and short-term objectives are expected to be
met within a year. The goals and objectives for TSA-D HCC include the following:
1. Long-Term Goal:
Strengthen regional preparedness and response to CBRNE incidents through improved
plans and increased exercises
Short-Term Objectives:
13A. Provide regional decontamination training, PER-211 Medical Management of
Chemical, Biological, Nuclear, and Explosive (CBRNE) Events
B. Ensure all coalition hospitals have standardized PPE in their inventories
C. Help facilitate Table Top Exercises for CBRNE events in each hospital upon
request.
D. Provide decontamination training / exercise opportunities through RRS
Decontamination Training vendor for the region.
2. Long-Term Goal:
Strengthen regional preparedness and response to mass casualty medical/infection
incident through improved understanding and plans, and increased community-based
exercises
Short-Term Objectives:
A. Provide regional medical countermeasures training, MGT-319: Medical
Countermeasures: Points of Dispensing (POD), Planning and Response
B. In conjunction with the local council of governments and public health
departments to provide opportunities to regional communities to hold a
community-based medical countermeasures table top exercise.
C. Invite DSHS Regions 2/3 Coordinator to share information about the Strategic
National Stockpile at a coalition meeting.
3. Long-Term Goal:
Improve regional redundant communications response
Short-Term Objectives:
A. Provide training at every hospital in crisis communications programs WebEOC
and EMResource
B. Hold coalition wide Redundant Communications Drills quarterly
C. Provide instruction on all operations of satellite phone systems.
D. Distribute a call down list to all coalition members.
4. Long-Term Goal:
Improve coalition member healthcare organizations’ understanding and implementation of
NIMS
Short-Term Objectives:
A. Provide resources for NIMs training online
B. Provide NIMS course training for ICS 300 and ICS 400
5. Long-Term Goal:
Improve coalition member hospitals’ understanding and implementation of Hospital Incident
Command System
Short-Term Objective:
14A. Provide HICS training
6. Long-Term Goal:
Improve regional Hospital recovery
Short-Term Objectives:
A. Provide COOP training to each coalition member
B. Provide COOP templates to each coalition member
7. Long-Term Goal:
Improve medical surge response
Short-Term Objective:
A. Conduct one coalition surge test annually
8. The Preparedness Strategy will be reviewed and updated annually.
9. A HCC Response Strategy will be developed in BP2 and will be reviewed and updated
annually thereafter. The Response Strategy will describe HCC operations.
10. An assessment will be conducted in BP2 to identify health care resources and services at
the jurisdictional and HCC levels.
11. The HCC activities will be tracked and monitored through multiple resources to include
monthly meeting agenda and minutes, regional project updates, and program performance
updates. HCC leadership will ensure accountability and completion by reviewing these
products monthly.
12. A HCC Continuity of Operations Plan (COOP) will be developed in BP3 and reviewed and
updated annually.
15Appendix A: HVA
9/10/2020
HCC-D REGIONAL
HAZARD VULNERABILITY
ANALYSIS REPORT
16HCC-D Regional
Hazard Vulnerability Analysis Report
The Regional Hazard Vulnerability Analysis Report is a product of the Healthcare
Coalition D (HCC-D) including the North Central Texas Trauma Regional Advisory
Council, HCC-D regional hospital and pre hospital partners, and EMS.
HVA Top Survey Results – September 2020
Our region is exposed to many hazards, all of which have the potential to impact
the community, causing casualties and damaging or destroying public / private property.
With this in mind, it is critical that the Healthcare Coalition be aware of the potential
impact. The tables displayed below have been generated from survey results provided
by healthcare delivery partners in the region.
Throughout each program year, hospital representatives are encouraged to
consider and remain aware of their top individual hazard and vulnerability levels. The
responsible hospital staff members prioritize and assign their hazards and ultimately
calculate risk, in collaboration with surrounding healthcare organizations and community
partners as needed. This report captures the potential threats/hazards of concern from
the 2017 Threat and Hazard Identification Risk Assessment (THIRA). All HVA results
are consolidated into separate tables (also provided below) to show areas of concern
based on the overall highest rated hazards, hazard vulnerabilities based on location
within the region, and also separated by hazard classification.
2020 Regional Threat and Hazard Identification Risk Assessment
Threats and Hazards of Concern
1) Wildfire
2) Hazardous Materials Release
3) Active Shooter
4) Pandemic/HCID
5) Radiological Attack
The Regional Hazard Vulnerability Analysis Report is a product created in Year
17 of the Hospital Preparedness Program and is a vital tool for the advancement of the
Healthcare Coalition. This report details the cumulative hazard results surveyed from
hospital members as well as the qualitative analysis of the hazards that are a threat to
the region. These findings will be used to drive future training, exercise, and planning
initiatives in HCC-D.
17Top Ten Hazard Vulnerability Analysis Regional Results
1) Inclement Weather
2) Tornado
3) Active Shooter
4) Trauma
5) Drought
6) Bomb Threat
7) Mass Casualty Incident
8) Temperature Extremes
9) Chemical Exposure, External
10) Power Outage
18Appendix B: HCC Member List
Hospital Name Administrator Representative Type
Anson General Hospital Dave Clark Glenda Fuston Hospital
Coleman County Medical Center Clay Vogel Harvey Ramirez Hospital
Comanche County Medical Center David Freshour Michael Moore Hospital
Eastland Memorial Hospital Ted Matthew Laura Kay Pfeifer Hospital
Fisher County Hospital Leanne Martinez Randy Martin Hospital
Haskell Memorial Hospital Fran McCown Mary Belle Olson Hospital
Hendrick Medical Center Brad Holland Mike Miller Hospital
Hendrick Medical Center South Brad Holland Sarah Alvarez Hospital
Hendrick Medical Center Brownwood Brad Holland William Loyd Hospital
Knox County Hospital District Stephen Kuehler Stephen Kuehler Hospital
Mitchell County Hospital Robbie Dewberry Murray Hall Hospital
Rolling Plains Memorial Hospital Donna Boatright Stephanie Leibowitz Hospital
Stephens Memorial Hospital Matt Kempton Marty Dover Hospital
Stonewall Memorial Hospital Andy Kolb Cody Hicks Hospital
Throckmorton County Memorial Hospital Kirby Gober Billy Boyd Hospital
Abilene Behavioral Health Stacey Sanford Tracy Noland Hospital
Encompass Rehabilitation Hospital Joe Roberson Robert Krackenfels Hospital
Comanche County EMS N/A Bryan Welch EMS
Sweetwater Fire and EMS Grant Madden Grant Madden EMS
Eastland EMS N/A Gene Wright EMS
Mitchell County EMS Jason Gruben Bambi Redwine EMS
West Texas COG Keith Collom Toby Virden EM
DDC-7 Greg Goettsch Greg Goettsch EM
DSHS Region 2/3 Community Preparedness N/A Clint Taylor Public
Health
Abilene-Taylor County Public Health Annette Lerma Nathaniel Lester Public
Health
Brownwood- Brown County Public Health Cliffton Karnes Donna Burleson Public
Health
Sweetwater-Nolan County Public Health Richard Acuna Tod Donham Public
Health
19Appendix C: TSA-D Healthcare Coalition Governance
I. TSA-D Healthcare Coalition
The TSA- D coalition is a network of healthcare organizations and providers that
are committed to coordinating emergency preparedness and response activities
through the following roles and responsibilities.
II. TSA-D Healthcare Coalition Preparedness Roles
A. Provide a regional structure and process for members and partners to
improve organizational and regional emergency preparedness through
joint-planning and problem-solving
B. Coordinate medical assets and communications for the healthcare system
C. Provide a healthcare training and exercise program based on healthcare
sector and regional plans to improve preparedness
III. TSA-D Healthcare Coalition Response Roles
A. Participate in local and regional EOC’s to support ESF #8 response and to
meet the health and medical needs of the community
B. Provide a structure for the healthcare system to address priorities that
arise during a response
C. Maximize the healthcare system's emergency response capacity by
sharing information and resources
IV. Chair Responsibilities
A. The TSA-D HCC Chair presides over meetings of the Executive Council
and general Coalition membership meetings, and represents the Coalition
as needed. The TSA-D HCC Chair serves for a term of two years.
B. The TSA-D HCC Chair has the authority to call or postpone the TSA-D
Healthcare Coalition meetings.
C. The TSA-D HCC Chair position will be assumed by the Vice Chair upon
the resignation or end of the presiding Chair’s term for a period of two
years or their resignation from the position
D. An individual cannot hold the TSA-D HCC Chair position for two
consecutive terms, but there is no limit to the total number of terms an
individual can hold the Chair position
20E. Appoint a TSA-D HCC representative to the NCTTRAC Regional
Emergency Preparedness Committee for HPP contract oversight purposes
F. Facilitate the appointment of a Big Country RAC representative to the
NCTTRAC Regional Emergency Preparedness Committee for HPP EMTF-
2 oversight purposes
V. Vice Chair Responsibilities
A. The Vice Chair assists the Chair with committee functions and assumes
the Chair responsibilities for TSA-D Healthcare Coalition activity and
meeting management in the temporary absence of the Chair.
B. Upon resignation or the end of the presiding Chair’s term, the Vice Chair
ascends to the Chair position.
C. The Vice Chair must be an employee of an HCC Core Group in good
standing.
D. The TSA-D HCC Vice Chair position will be nominated & elected by the
TSA-D Core Membership and will hold office for a two-year term.
E. An individual cannot hold the TSA-D HCC Vice Chair position for two
consecutive terms, but there is no limit to the total number of terms an
individual can hold the Vice Chair position.
VI. Meetings, Agenda, and Minutes
A. The HCC will convene at least six times per year.
B. All general coalition meetings will be held as open meetings.
C. The TSA-D Healthcare Coalition will follow a NCTTRAC approved format
for the meeting agenda and minutes.
D. The TSA-D Healthcare Coalition will normally be provided with staff
support to draft minutes and capture attendance information following
each meeting as a record of committee activities.
VII. TSA-D Healthcare Coalition Core Group members
The Coalition is an inclusive body that is open to all organizations that provide
health services in TSA- D, but the TSA-D Healthcare Coalition Core Group
members shall be comprised of representatives from hospitals, emergency
medical services (EMS), public health departments, and emergency
management offices.
A. Participation: All Core Group members are expected to do the following
to maintain a good standing within the Coalition:
211. Participate in a minimum of 50% of scheduled HCC meetings
through attendance by their primary or alternate appointee.
2. Share information that is relevant for emergency planning and
response, including information about available capacity and
resources.
3. Participate in coordinating and sharing resources
4. Participate in Coalition preparedness activities, including training
and drills
5. Maintain current emergency preparedness plans and designate a
person who is responsible for emergency preparedness and
response
VIII. Voting: The Chair shall manage voting issues in accordance with existing
TSA-D bylaws and procedures. All Coalition Core Members have voting rights
if they are members in good standing. Either the TSA-D Healthcare Coalition
Core Group member representative or a designated alternate shall exercise
the right to vote on TSA-D HCC matters as necessary. A simple majority vote
of those Core Group members who are present at the call for a vote is
required to take action.
IX. How constituted: The TSA-D HCC Chair shall preside over TSA-D HCC
and the Executive Council. The Chair is determined in accordance with TSA-
D bylaws. The TSA-D HCC Core Group members will also vote to identify a
Vice Chair as defined in paragraphs IV and V above. The Executive Council
will serve as the governing body of the Healthcare Coalition and consists of
the Chair, Vice Chair, a Secretary and a minimum of one member from each
of the Coalition Core Member Groups (Hospitals, EMS, Public Health and
Emergency Management.) All Executive Council members will be will be
nominated and elected by the HCC Core Membership with the exception of
the Chair, which is determined in accordance with sections IV and V of TSA-
D’s Governance. Executive Committee Members will be need to attend 75%
of schedules Executive Committee Meetings and General Membership
Meetings in order to maintain their position on the committee.
Committees, workgroups and project managers will be formed to address
topic specific planning areas.
The current TSA-D Executive Council Members are as follows:
Miranda Clemmons (Chair) – Brownwood Regional Medical Center
22Stephanie Lebowitz (Vice Chair) – Rolling Plains Memorial Hospital
Murray Hall (Member) – Mitchell County Hospital
Randy Martin (Member) – Fisher County Hospital
Pixie Clark (Secretary) – Brownwood- Brown County Public Health
X. Meetings: General Membership Meetings shall be managed in accordance
with TSA-D’s Bylaws. Meetings will be held at least 6 times per calendar year.
The Executive Council will plan to convene every month but will ensure that a
minimum of six (6) meetings occur during each fiscal year.
XI. Funds: The right to execute legal contracts or obligations is reserved for
NCTTRAC staff under the direction from the TSA-D HCC and NCTTRAC
Board of Directors.
XII. Amendments: This Governance may be altered, amended or repealed in
accordance with TSA-D’s bylaws and with approval of the Executive Council.
XIII. TSA-D NON CORE MEMBERSHIP ROLES
A. Coalition members that are not from the core group organizations
(Hospitals, EMS, Public Health and Emergency Management) will receive
a letter of participation from the coalition if they comply with the following:
1. Participate in a minimum of 25% of scheduled HCC meetings through
attendance by their primary or alternate appointee.
2. Share information that is relevant for emergency planning and
response, including information about available capacity and
resources.
3. Participate in coordinating and sharing resources
4. Participate in Coalition preparedness activities, including training and
drills
5. Maintain current emergency preparedness plans and designate a
person who is responsible for emergency preparedness and response
XV. Product Responsibilities (SOPs, SOGs, Protocols, Guidelines, and
Plans)
A. Regional Hazard Vulnerability Analysis
B. MYTEP
23C. HCC Preparedness Strategy
D. HCC Response Plan
XVI. PROCUREMENT
A. NCTTRAC as the HPP grantee and contractor for TSA-D has the
responsibility to provide administrative support and oversight of
procurement of HPP funded supplies, expendable property, equipment,
and services in TSA-D.
B. NCTTRAC procurement procedures will be conducted in accordance with
the NCTTRAC Financial Policies and Procedures Manual.
C. NCTTRAC will address Historically Underutilized Business (HUB)
requirements in accordance with all individual contract specifications.
Hospital Preparedness Program HUB Procurement Thresholds are listed
below:
DOLLAR BID REQUIREMENT
Up to No bids required from eligible HUB vendors
$2,500.01 - At least one bid from eligible vendors on the
$100,000.00 Centralized Masters Bidders List (CMBL) with 1
being a CPA/TPASS- certified HUB
$100,000.01 At least two bids from eligible vendors on the
and up Centralized Masters Bidders List (CMBL) with 2
being CPA/TPASS- certified HUBS
D. Procurement Flow / Process
1. HCC Asset Request Tracking Form Submitted to HCC
2. HCC Chair signs the Asset Request Tracking Form signifying the
request has been approved by HCC
3. The HCC Chair will submit the Asset Request Tracking Form to
NCTTRAC via email
4. NCTTRAC will approve or deny the request:
a. Approval: Work with NCTTRAC logistics to retrieve Purchase
Request and Purchase Orders to procure the request
b. Denial: If request is denied, it will be returned with reason for
denial and will be open for re-submission
24Appendix D: ASPR Coalition Assessment Tool
The ASPR Coalition Assessment Tool (CAT) is used by coalitions to prioritize Coalition
Capabilities and track Capability progress electronically. The CAT provides a single
location to assess and track HCC progress toward achieving the 2017–2022 Health Care
Preparedness and Response Capabilities, meeting the requirements of the 2017-2022 HPP
Cooperative Agreement and completing the 2017–2022 HPP Performance Measures. The
CAT is a nationwide tool that also provides a more effective avenue for HCCs to request
targeted technical assistance. The CAT provides a variety of reports for HCC planning and
analysis, including a Capability Planning Report. This report provides an objective score
and recommendation for future progress. The application generates a recommendation for
capability progress based on responses to capability activities and suggested level of
importance. The scale used to measure objective ability is provided below.
Ability Level Objective Score
No Ability 0-20
Limited Ability 21-40
Some Ability 41-60
Significant Ability 61-80
Full Ability 81-100
See full chart on the next page.
25The CAT Capability Planning Report Results from November 6, 2018 are presented below.
Objective Objective Level of Recommendation
Score (%) Importance
Capability 1: Foundation for Health
Care and Medical Readiness
Objective1 - Establish and 100 Important Sustain
Operationalize a Health Care Coalition
Objective3 - Develop a Health Care 78 Important Build - low priority
Coalition Preparedness Plan
Objective4 - Train and Prepare the 100 Important Sustain
Health Care Coalition Preparedness
Plan
Objective5 - Ensure Preparedness is 83 Important Sustain
Sustainable
Objective2 - Identify Risk and Needs 25 Important Build - high priority
Capability 2: Health Care and Medical
Response Coordination
Objective1 - Develop and Coordinate 13 Important Build - high priority
Health Care Organization and Health
Care Coalition Response Plans
Objective2 - Utilize Information Sharing 71 Important Build - low priority
Procedures and Platforms
Objective3 - Coordinate Response 30 Important Build - high priority
Strategy, Resources, and
Communications
Capability 3: Continuity of Health Care
Service Delivery
Objective1 - Identify Essential 0 Important Build - high priority
Functions for Health Care Delivery
Objective2 - Plan for Continuity of 25 Important Build - high priority
Operations
Objective3 - Maintain Access to Non- 20 Important Build - high priority
Personnel Resources during an
Emergency
Objective4 - Develop Strategies to 0 Important Build - high priority
Protect Health Care Information
Systems and Networks
Objective5 - Protect Responders' 60 Important Build - medium
Safety and Health priority
Objective6 - Plan for and Coordinate 50 Important Build - medium
Health Care Evaluation and Relocation priority
Objective7 - Coordinate Health Care 63 Important Build - low priority
Delivery System Recovery
Capability 4: Medical Surge
Objective1 - Plan for a Medical Surge 38 Important Build - high priority
Objective2 - Respond to a Medical 36 Highly Build - very high
Surge important priority
26Appendix E: HPP Letter of Agreement
2728
29
30
31
32
33
Appendix F: Acronyms
AAR /IP– After Action Report / Improvement Plan
ASPR – Assistant Secretary for Preparedness and Response
CAT – Coalition Assessment Tool
CDC – Center for Disease Control and Prevention
CONOPS – Concept of Operations
DSHS – Department of state Health Services
EMS – Emergency Medical Services
EMTF – Emergency Medical Task Force
EOC – Emergency Operations Center
ESF-8 – Emergency Support Function-#8
HCID – Highly Contagious Infectious Disease
HICS – Hospital Incident Command System
HSEEP – Homeland Security Exercise and Evaluation Program
ICS – Incident Command System
LOA – Letter of Agreement
MAC – Multi-agency Coordination
MAP – Mutual Aid Plan
MCI – Mass Casualty Incident
MOS – Memorandum of Sharing
MYTEP – Multi-Year Training and Exercise Plan
NIMS – National Incident Management System
THIRA - Threat Hazard and Identification Risk Assessment
34You can also read