A more practical guide to incorporating health equity domains in implementation determinant frameworks
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Woodward et al. Implementation Science Communications
https://doi.org/10.1186/s43058-021-00146-5
(2021) 2:61
Implementation Science
Communications
METHODOLOGY Open Access
A more practical guide to incorporating
health equity domains in implementation
determinant frameworks
Eva N. Woodward1,2* , Rajinder Sonia Singh2,3, Phiwinhlanhla Ndebele-Ngwenya4, Andrea Melgar Castillo5,
Kelsey S. Dickson6 and JoAnn E. Kirchner2,7
Abstract
Background: Due to striking disparities in the implementation of healthcare innovations, it is imperative that
researchers and practitioners can meaningfully use implementation determinant frameworks to understand why
disparities exist in access, receipt, use, quality, or outcomes of healthcare. Our prior work documented and piloted
the first published adaptation of an existing implementation determinant framework with health equity domains to
create the Health Equity Implementation Framework. We recommended integrating these three health equity
domains to existing implementation determinant frameworks: (1) culturally relevant factors of recipients, (2) clinical
encounter or patient-provider interaction, and (3) societal context (including but not limited to social determinants
of health). This framework was developed for healthcare and clinical practice settings. Some implementation teams
have begun using the Health Equity Implementation Framework in their evaluations and asked for more guidance.
Methods: We completed a consensus process with our authorship team to clarify steps to incorporate a health
equity lens into an implementation determinant framework.
Results: We describe steps to integrate health equity domains into implementation determinant frameworks for
implementation research and practice. For each step, we compiled examples or practical tools to assist
implementation researchers and practitioners in applying those steps. For each domain, we compiled definitions
with supporting literature, showcased an illustrative example, and suggested sample quantitative and qualitative
measures.
Conclusion: Incorporating health equity domains within implementation determinant frameworks may optimize
the scientific yield and equity of implementation efforts by assessing and ideally addressing implementation and
equity barriers simultaneously. These practical guidance and tools provided can assist implementation researchers
and practitioners to concretely capture and understand barriers and facilitators to implementation disparities.
Keywords: Health equity, Implementation, Health disparities, Framework, Theory, Implementation science,
Determinant
* Correspondence: Eva.woodward2@va.gov
1
Center for Mental Healthcare and Outcomes Research, U.S. Department of
Veterans Affairs, North Little Rock, AR, USA
2
Department of Psychiatry, University of Arkansas for Medical Sciences, Little
Rock, AR, USA
Full list of author information is available at the end of the article
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.Woodward et al. Implementation Science Communications (2021) 2:61 Page 2 of 16
communities in developing implementation science and
Contributions to the literature
practice [8], lack of consistent methods and data ele-
Applications of how the Health Equity Implementation ments related to equity across implementation studies
Framework guided other implementation efforts [9], and exclusivity and social injustice within the imple-
mentation science workforce perpetuated by structures
Practical tools, including a table of sample measures for
making it harder for institutions to recruit and retain
health equity determinants, a qualitative interview guide,
marginalized people (e.g., school-to-prison pipeline).
and a qualitative codebook Also, disparities exist for innovations being implemented
Clarified broad steps for integrating a health equity lens into and, if not adapted for marginalized populations, imple-
an implementation determinant framework mentation may perpetuate the exclusion of marginalized
communities and widen health inequities [6]. Similar to
Background implementation studies, marginalized populations have
Health equity occurs when all people have socially just historically been excluded from clinical trials and effi-
opportunities for optimal well-being. Disparities in cacy studies [10]. Further, innovations are often not de-
healthcare implementation exist when a healthcare signed nor as efficacious for marginalized populations
innovation, such as a program or treatment, is delivered [11–13]. Thus, the limitations of disparities in
with significantly worse access, receipt, use, quality, or innovation development can be inherited by implemen-
outcomes for certain populations compared to others tation science and likely perpetuated if the implementa-
[1]. Structural factors and systems greatly contribute to tion does not systematically consider disparity
different as well as unjust or unfair treatment of certain determinants, cultural adaptations, and other ways to
populations. Populations that experience worse health or ensure health equity.
healthcare might be defined by race, ethnicity, sexual Outside the U.S., health equity and implementation re-
orientation, gender identity, socioeconomic status, func- search predominantly focus on a specific marginalized
tional limitation, or other characteristics [2]; we refer to population, which is an important and valid path toward
these groups as marginalized populations based on so- equity [9, 14–16]. Examples in low- and middle-income
cial, economic, and/or environmental disadvantage that countries include measurement tools normed with par-
accompanies health inequities [3]. One example of an ticipants from those countries [17], adapting innovations
implementation disparity in United States (U.S.) or delivery methods specifically to those populations
pediatric healthcare is screening and diagnosis of autism [18] and reviewing or developing frameworks specific to
spectrum disorder. Although there are valid and reliable those countries [14, 19, 20]. Although adaptations to
autism screenings and clear criteria for diagnosis, racial local contexts are important, there remain gaps in apply-
and ethnic minority children who meet the criteria are ing principles of health equity to implementation re-
less likely to be diagnosed than non-Hispanic white chil- search broadly, partly because locally adapted
dren [4]. Thus, effective screenings and diagnoses are frameworks are not easily generalizable to other coun-
implemented inequitably for racial and ethnic minority tries or contexts. The current charges to implementation
children, resulting in delayed treatment for children of researchers to ensure health equity in their efforts [6,
color. This implementation disparity is exacerbated 21] are not possible without adapting implementation
when children are finally diagnosed properly with aut- determinant frameworks to first capture and under-
ism, as children of color are less likely to receive quality standing barriers to equitable implementation.
treatment [5]. Unfortunately, several implementation
disparities may be undetected. As Braveman wrote, Implementation determinant frameworks with an equity
“Health disparities are the metric we use to measure focus are needed
progress toward achieving health equity” [3]. Implementation science frameworks have been catego-
Overall, implementation science has yet to actively and rized into three types: determinant (establishing what
systematically assess, address, and evaluate unique fac- factors determine or predict implementation success),
tors contributing to healthcare inequities, including in- process (clarifying how to address determinants to
stitutional and structural problems, such as racism, that achieve implementation success), and evaluation (deter-
are economic, regulatory, social, historical, and political mining metrics and assessment to know when imple-
determinants of implementation for marginalized groups mentation success is achieved) [22]. Implementation
[6]. There are many reasons why implementation re- determinant frameworks are key to inform study design
searchers have yet to showcase solutions to healthcare and selection of strategies to match contextual needs;
inequities including underrepresentation of marginalized yet, we have only recently considered determinants
and resource-poor communities in implementation stud- unique to health inequities, starting with the Health
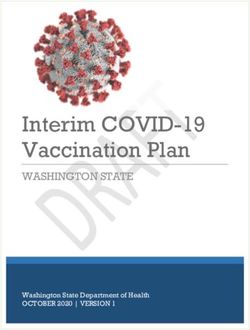
ies [6, 7], lack of true engagement with marginalized Equity Implementation Framework [23]. We first pilotedWoodward et al. Implementation Science Communications (2021) 2:61 Page 3 of 16 health equity domains within the context of a determinant more depth than in prior work, showcase two applica- framework as this type of framework represents the key tions of this determinant framework from the literature, first step to detecting (and eventually addressing) imple- and delineate steps to incorporate health equity do- mentation disparities. If implementation researchers and mains in an implementation determinant framework, practitioners could meaningfully and practically assess and with sample measures and data collection tools for each understand the determinants of implementation dispar- domain. ities, this would allow them to adapt the innovation and implementation strategies for marginalized populations and detect health equity determinants as potential moder- Health Equity Implementation Framework ators for implementation success/failure [21]. Unfortu- In the Health Equity Implementation Framework, we nately, most implementation determinant frameworks proposed determinants believed to predict successful have yet to be explicitly adapted for or tested within health and equitable implementation, seen in Fig. 1 [23]. These equity efforts and any that do appear too vague to be used determinants are grouped under domains. We define do- meaningfully [24]. mains as broad constructs relevant to implementation Our prior work documented and piloted adaptations and health equity success. Within each domain are sev- of one existing implementation determinant framework eral determinants or specific factors that are measurable with three health equity domains to create the Health and, together in constellation with other determinants, Equity Implementation Framework [23]. One may also clarify barriers, facilitators, moderators, or mediators to use the Health Equity Implementation Framework in its implementation and health equity success. This frame- entirety as an implementation determinant framework work was developed for healthcare and clinical practice or use the three health equity domains as additions to settings [25]. In the Health Equity Implementation another implementation determinant framework. Many Framework, we added three health equity domains to researchers and practitioners have requested clarification the Integrated Promoting Action on Research in Imple- of the Health Equity Implementation Framework do- mentation in Health Services (i-PARIHS) framework mains for practical use. Damschroder argued that imple- [26], which also proposes a process—facilitation—by mentation frameworks must describe how domains are which change in each domain would occur [25, 26]. The well-grounded in existing literature, provide clear defini- focus of this manuscript is on the three health equity do- tions, and offer suggested validated implementation mains, rather than facilitation, as science is still emer- strategies [22]. Therefore, we review definitions of the do- ging on how implementation processes should be main of the Health Equity Implementation Framework in tailored or adapted to promote equity. Fig. 1 Health Equity Implementation Framework
Woodward et al. Implementation Science Communications (2021) 2:61 Page 4 of 16
Domains typical in implementation determinant Domains known to affect health equity
frameworks The Health Equity Implementation Framework incorpo-
Broad domains typical in implementation determinant rates these domains known to affect health disparities
frameworks focus on factors spanning multiple levels, and thus, equity: (1) culturally relevant factors, such as
including the individual (e.g., personal characteristics, medical mistrust, demographics, or biases of recipients
actors of implementation, individuals receiving an [34–37]; (2) clinical encounter or patient-provider inter-
innovation), organization (e.g., clinical service, school, action [38–40]; and (3) societal context including phys-
department, factory), community (e.g., local government, ical structures, economies, and social and political forces
neighborhood), system (e.g., school district, hospital sys- [41–43]. We added these three health equity domains,
tem), and policy (e.g., state government, broader laws) described below, from existing research that have clear,
[27]. These domains can be further specified, such as strong associations with disparities in health status, ac-
inner setting or outer setting within an organization cess to, quality of, or outcomes of healthcare, [44] or
[28]. Domains from i-PARIHS are the basis of the there is enough evidence to suggest determinants within
Health Equity Implementation Framework and include these domains should be considered (e.g., [45]).
those typical in most implementation determinant
frameworks [27]. Determinants within each domain act 1. Culturally relevant factors of recipients. Recipients
to enable or constrain implementation and each domain in the implementation process are individuals who
is briefly defined below. will be asked to offer or receive an innovation (e.g.,
patients, providers) [26]. Culturally relevant factors
Innovation of recipients are characteristics unique to a group
Innovation refers to the treatment, intervention, practice, of people in the implementation effort (e.g.,
or new “thing” to be implemented, adopted by providers patients, staff, providers) based on their lived
and staff, and delivered to patients [29]. The innovation experience. Some examples of recipient factors that
may be a program, practice, principle, procedure, prod- may be culturally relevant are implicit bias,
uct, pill, or policy [30]. socioeconomic status, race and/or ethnicity,
immigrant acculturation, language, health literacy,
Recipients health beliefs, or trust in the clinical staff or patient
Recipients are individuals who influence implementation group [36, 37]. Demographic characteristics, such
and those who are affected by its outcomes, both at the as socioeconomic status or race, are not inherently
individual and collective team levels [26]. In healthcare, descriptive of one’s culture. Rather, the important
recipients are typically grouped into providers and other takeaway is how living in the world with these
staff, and patients and caregivers. factors shapes one’s culture and experience (e.g.,
living in impoverished neighborhoods, experiencing
Context racism). We do not feel strongly that any
Context includes different micro, meso, or macro levels demographic factor be categorized as a culturally
that correspond to inner and outer contexts [26]. Con- relevant factor—the most important thing, from our
text can include factors such as resources, culture, lead- view, is that implementation practitioners and
ership, and orientation to evaluation and learning. In scientists acknowledge these demographics among
this framework, the micro-level includes the local inner their recipient groups and consider how
context (e.g., specific ward or clinic), whereas the meso implementation may need to be adapted based on the
includes the organization (e.g., hospital or medical cen- lived experience of recipient groups. For instance,
ter). The macro-level of outer context includes the wider implementation practitioners and scientists should
healthcare system and effect this has on the other do- consider how implementation would need to change
mains (e.g., United Kingdom National Health Service) for those who have little formal education, are people
[28]. of color, or are underinsured. Factors from patients
and providers might attend to differences between,
Facilitation or process for example, age, pre-existing stereotypes, or lack of
There are processes by which barriers in implementation trust that could hinder the interaction [40]. Culturally
domains are solved or overcome, and strengths are har- relevant factors will vary by group, local context, and
nessed to promote the use of an innovation in routine individuals. It is crucial that culturally relevant factors
practice [28]. In i-PARIHS, facilitation is the “active in- of recipients are considered as determinants or
gredient” or process [31]. Facilitation involves imple- potential moderators in implementation success/failure
mentation strategies that result in implementation when patients belong to a group experiencing a health
coming to fruition [32, 33]. or healthcare disparity.Woodward et al. Implementation Science Communications (2021) 2:61 Page 5 of 16
2. Clinical encounter (patient-provider interaction). factor is exclusively an economy, physical structure, so-
This domain describes the transaction that occurs cial norm, or all three; rather, it is important these soci-
between patients and providers in healthcare etal determinants are detected and addressed to ensure
appointments, where decisions concerning strategies address key drivers of societal inequities. Soci-
diagnoses and treatment are made, and providers etal context may not be assessed comprehensively in one
administer care [46]. The clinical encounter is study or initiative, due to feasibility constraints, but they
important to assess because there is a myriad of should be documented in formative evaluations/initial
behaviors and perceptions during the clinical diagnostic assessments of the implementation problem.
encounter that affect whether an innovation is
offered by a provider and whether it is accepted by Economies
a patient. Behaviors will vary by innovation, There are four typical structures of economies including a
context, and recipients and may be especially traditional economy (i.e., mostly agricultural), market
important for patients who experience health or economy (i.e., firms and private interests control capital),
healthcare disparities due to unequal power command economy (i.e., government controls capital),
between them and providers. Factors to measure and a mixed economy (combination of command and
might be how recipients maneuver the conversation market) [53]. It is helpful to consider how economic struc-
accordingly to achieve their individual and shared ture affects access to resources for implementation. Mar-
goals [40, 47]. It would also be important to capture ket forces can be used to change demand for products
unconscious or implicit bias from either recipient deemed healthy or unhealthy, therefore driving policy im-
about the other recipient’s characteristics, such as plementation. Examples of market forces include taxes on
race, weight, or perceived sexual orientation [48– tobacco, unhealthy food, and soft drinks, or food subsidy
50]. These unconscious biases may manifest in programs for women with low incomes [41].
unhelpful behaviors during the encounter, such as
dismissing someone’s concerns, interrupting the Physical structures
other person, or not smiling, touching, or making Equity can be affected by how physical spaces, or “built
eye contact. Clinical encounters predict patient environments,” are arranged and how transition between
satisfaction, trust, and health outcomes; thus, it is those spaces occurs for healthcare [41]. Physical struc-
crucial to assess and address what occurs during tures include any factors where people have to physically
the clinical encounter, especially with regard to go to get healthcare and what environmental elements
implementation disparities [47, 50–52]. people may be exposed to (e.g., privacy or lack thereof,
3. Societal context: economies, physical structures, what they see, what is emitted in the air and into their
and sociopolitical forces. This domain is similar to bodies). One example in healthcare settings is the type
social determinants of health, yet also incorporates and quality of language translations of information dis-
more upstream determinants (e.g., governance) that played (e.g., flyers, waiting rooms)—whether it matches
have been investigated less relative to mid- or the language of patients served [54]. The location of the
downstream determinants (e.g., neighborhoods) healthcare setting in a town or city is important in rela-
[44]. Societal context includes three specific tion to where patients reside [54, 55], e.g., is it difficult
determinants: (1) economics, (2) physical structures, for patients to get to the point of care? Another example
and (3) sociopolitical forces. In piloting the Health is the implementation of one U.S. state’s naloxone stand-
Equity Implementation Framework, societal context ing order in which pharmacies could distribute naloxone
affected receipt of antiviral hepatitis C virus without a prescription: 61.7% of retail pharmacies had
medicine for Black patients in the U.S. Veterans naloxone available without a prescription [56]. However,
Health Administration [23]. naloxone availability was lower in neighborhoods with
higher percentages of residents with public health insur-
Societal context may include historical or current dis- ance—a physical structure problem (lower availability of
crimination against marginalized groups, such as racism, naloxone in some neighborhoods) interacting with an
classism, or transphobia that may be formally or infor- economic factor (public health insurance). This finding
mally institutionalized within any organizational or local was particularly problematic due to an increased cost of
context. These factors usually occur in the broadest naloxone for people on public health insurance as a re-
levels of the environment (e.g., province, nation), affect- sult of the statewide mandate.
ing the healthcare system, clinics, and recipients down-
stream. Many societal context determinants are Sociopolitical forces
interrelated, such as a policy affecting a physical struc- The third societal context describes social norms or pol-
ture. It is not as important to distinguish whether a itical forces, which can include but are not limited toWoodward et al. Implementation Science Communications (2021) 2:61 Page 6 of 16
political support, laws, and social structures in which framework guided subsequent integration of qualitative
linkages between institutions perpetuate oppression, and quantitative data, including the use of qualitative
such as racism, misogyny, classism, or heterosexism [43, themes to complement and expand quantitative findings.
57]. For instance, public health policies (e.g., fiscal, regu- Preliminary findings indicate a significant impact of
lation, education, preventative treatment, and screening) outer and inner context on inequities, including fit be-
demonstrate positive and negative effects on health dis- tween patient recipient characteristics, culturally relevant
parities that occur across health domains (e.g., tobacco, factors, and characteristics of available innovations. Add-
food and nutrition, reproductive health services) [41]. As itional outer context factors, including sociopolitical fac-
another example, a study examined U.S. state legislators’ tors and physical structures such as location (urban
behavioral health research-seeking practices and dissem- versus rural) also impact service utilization, including in-
ination preferences and found significant variation be- teractions with provider factors and innovation
tween Democrats and Republicans, suggesting characteristics.
dissemination materials be tailored to different social
norms for different groups [58].
Next, we showcase two examples of how implementa- Conducting a process evaluation to categorize ongoing
tion teams have used culturally relevant factors of recipi- barriers/facilitators
ents, patient-provider clinical encounter, and societal In Toronto, Canada, legally sanctioned supervised con-
context as health equity domains in formative and sumption services (the innovation) are integrated within
process evaluations. Each example comes from different health centers; implementation has occurred and is on-
health service sectors and describes efforts focused on going. Supervised consumption services are for people
implementation disparities. who inject drugs to receive sterile injection equipment
and inject under staff supervision. Staff educate on safer
Conducting a formative needs assessment prior to injecting, provide referrals to services, and can respond
implementation to overdoses, reducing transmission of infectious dis-
The Health Equity Implementation Framework has been eases (e.g., HIV) and overdose deaths. Researchers used
applied to guide a needs assessment for an implementa- ethnographic observation and individual semi-structured
tion project aiming to reduce inequities in the provision interviews with 24 patients who injected drugs in super-
and receipt of publicly funded services for individuals vised consumption services at two community health
with developmental disabilities in the U.S. (Rieth SR, centers, half of who were people of color or Indigenous
Dickson KS, Plotkin R, Corsello C, Ko J, Cook-Clark T, to Canada [59]. After coding, researchers interpreted
et al: An in-depth analysis of expenditures for Latinx in- findings within domains of the Health Equity Implemen-
dividuals with developmental disabilities: Following the tation Framework.
money and perspectives from the front line, in prepar- Integrating legally sanctioned supervised consumption
ation). In 2016, the State of California Department of services within health centers (sociopolitical force) pro-
Developmental Services made funds available to address vided clients access to other health services, including
significant inequities in service expenditures for Latinx dentistry and medical assistance that eliminated the need
clients. In response, the San Diego Regional Center, the for a provider visit (characteristics of the innovation,
local agency coordinating and funding publicly-funded organizational context). Patients appreciated having
developmental disability services, initiated a partnership everything in one physical place (physical structure).
with local services and implementation researchers to One participant said the services allowed them to avoid
identify inequity reduction targets and develop and im- meeting providers who were prejudice against drug use
plement an inequity reduction model. A mixed methods (sociopolitical force, provider culturally relevant factor).
needs assessment was conducted to inform model devel- Yet, there were barriers to implementation. Patients
opment and implementation activities. Quantitative data were uncomfortable being seen by peers using the center
included administrative data from the previous year. due to stigma about drug use (sociopolitical force).
Qualitative data were gathered from focus groups with Spatial limitations at the center made it difficult to have
regional center case managers to identify key determi- privacy while injecting (physical structure). Patients pre-
nants of inequities from their perspectives. ferred the center to be open all the time (organizational
The Health Equity Implementation Framework guided context), but there were not enough staff for that flexi-
the identification of implementation determinants and bility (healthcare system context). Ethnographic observa-
the selection of data coding and analyses. Specifically, tion suggested standalone supervised consumption
the framework informed the development of the qualita- services were consistently busier than integrated ser-
tive codebook, including coding domains and definitions vices, potentially because some people felt uncomfort-
that were iteratively refined for this project. The able in a healthcare setting (patient factor).Woodward et al. Implementation Science Communications (2021) 2:61 Page 7 of 16
Methods Determine implementation determinants
We completed a consensus process to clarify steps for Assess which determinants are present in an implemen-
incorporating a health equity lens into an implementa- tation disparity and whether each determinant is a bar-
tion determinant framework, situated within the existing rier (challenge) to improving equitable implementation
literature. We reviewed Moullin and colleagues’ ten sug- or a facilitator (strength). Through formative evaluation
gested steps for incorporating frameworks into an imple- to assess barriers and facilitators in each domain [62, 63]
mentation effort [60] and selected the five steps align qualitative interview guides, quantitative measures,
applicable to an implementation determinant framework and other assessment methods (e.g., participant observa-
(vs. evaluation or process frameworks). The first author tion, policy review) to the framework’s determinants. For
(ENW) expanded those five steps from Moullin and col- qualitative and quantitative assessments of determinants,
leagues [60] with steps on how to incorporate health we present in Table 1 a variety of assessment methods
equity domains and determinants. These steps were vet- and measures one might use to assess determinants
ted with the authorship team through a process of oral within the Health Equity Implementation Framework.
discussions, reviewing written documents, and refining An illustrative example is given to showcase how others
steps until all agreed. Next, our team created or aligned have assessed various determinants incorporated in the
a table, tool, or example for more practical guidance on framework. Although Table 1 is not exhaustive, it is a
how each step could be executed. robust reference and guide to consider certain measures,
tools, or data sources for formative evaluation.
Results If one is using qualitative methods to determine some
Applying health equity domains across an or all of the equitable implementation determinants, we
implementation effort provide examples of questions from qualitative interview
Below are suggested steps on how to use frameworks in guides we piloted that are aligned to domains of the
an implementation effort [60] with a focus from our Health Equity Implementation Framework (see Add-
authorship team specifically on health equity in an im- itional file 1). If this approach is used, the framework do-
plementation determinant framework. mains are then helpful for designing qualitative
codebooks or templates for analysis. We provide a code-
Select a suitable framework or domains for an book for analysis we piloted that is aligned to the three
implementation disparity problem health equity domains (see Additional file 2). The code-
If an implementation effort will focus on a health condi- book for the health equity domains can be combined
tion or marginalized population with documented health with codebooks of other determinant frameworks, such
or healthcare disparities, we strongly suggest incorporat- as Consolidated Framework for Implementation Re-
ing determinants from the three health equity domains search [126].
into one’s preferred implementation framework or use
the Health Equity Implementation Framework. If we do Use domains to develop an implementation mechanistic
not assess or consider domains that promote or inhibit process model or logic model
disparities, then we cannot expect to address them in a Determinants in the Health Equity Implementation
meaningful way, and we cannot build our scientific inte- Framework may directly influence the success and equity
gration of health equity and implementation science to of an implementation effort or they may indirectly affect
generalize across implementation efforts. To find an im- outcomes as mechanisms through which success or
plementation determinant framework other than the equity are enhanced. Using the three health equity do-
Health Equity Implementation Framework that can be mains added to an implementation determinant frame-
adapted for implementation disparities, pick a frame- work, one may develop theoretically driven hypotheses
work using an online webtool showcasing many imple- about which domains, or determinants within them,
mentation determinant frameworks (https:// must change to lead to improved equity and implemen-
dissemination-implementation.org/) [61]. tation success [127]. These determinants are mecha-
The Health Equity Implementation Framework can be nisms. When working on an implementation disparity
adapted to any population or country where implemen- problem, this will ensure some mechanisms related to
tation disparities occur. The framework proposes deter- equity and implementation are investigated.
minants of inequitable implementation and a process To understand the concept of mechanisms of imple-
(facilitation) by which to address determinants. The mentation disparities, we consider a hypothetical ex-
framework has not been used as a process or evaluation ample of an implementation disparity at one hospital
framework; thus, we cannot speak to the value of focus- where an evidence-based innovation is received mostly
ing on these domains in implementation processes or to by White people with moderate or high incomes. In this
these domains as evaluation outcomes. example, the implementation disparity between patientsWoodward et al. Implementation Science Communications (2021) 2:61 Page 8 of 16
Table 1 Definitions, illustrative examples, and sample measures of the Health Equity Implementation Framework
Domain and Definition Illustrative example(s) Sample measuresa
determinants
Characteristics of the An innovation is a treatment, A study examined the uptake of the Quantitative:
innovation [31]: intervention, or practice with unique Healthy Heart Kit (innovation), a risk • Decision-Maker Information Needs
• Underlying knowledge characteristics that determine how management and patient education and Preferences Survey
sources such innovations will be applied in a resource for the prevention of • Electronic Health Record Nurse
• Clarity particular setting. Innovations fall into cardiovascular disease, in a primary Satisfaction Survey [67]
• Degree of fit with one of the “7 Ps”: programs, practices, care setting. They found that relative • Reports assessing the current status
existing practice/values principles, procedures, products, pills, advantage (innovation was the most of implementing the innovation,
• Usability or policies [30]. comprehensive tool for cardiovascular completed by one clinic point of
• Relative advantage The innovation should be tailored health) and observable results contact or champion [68]
• Trialability with minor changes or adapted with (evidence-based practice supports Qualitative:
• Observable results major changes to the setting’s needs innovation) were more influential to • Barriers and facilitators assessment
• Evidence for the and practices for successful the uptake of Healthy Heart Kit than instrument
innovation [64] implementation [31, 65]. other characteristics [66]. • General practitioners’ perceptions of
• Research the route of evidence-based
• Clinical experiences medicine
• Patient experiences • Knowledge, attitudes, and
expectations of web-assisted tobacco
interventions [67]
*Clinical encounter This is the nature of the interaction In studying recordings of HIV patient- Quantitative:
(patient-provider between patient and provider. This provider encounters, there was less • Patient and provider questionnaires
interaction) domain is centered on how the psychosocial talk in patient-provider about relevant demographics to
patient and provider choose, adapt, encounters with Hispanic compared to assess concordance/match between
and coordinate the conversation to non-Hispanic white patients [39]. patient and provider
achieve their shared and personal In a study on predictors and • Patient rating about the encounter:
goals concerning health-related mat- consequences of negative patient- Interpersonal Processes of Care
ters [40]. provider interactions among a sample Survey [39]
The interaction could be influenced of African American sexual minority • Experiences of Discrimination Scale
by: women, authors found racial discrimin- [69]
• Predisposition features which are ation was most frequently mentioned, Qualitative:
individual differences that influence and gender and sexual orientation dis- • Patient qualitative interviews about
communication that may be crimination were also related to nega- their experience of care [70, 71]
objective (e.g., age) and subjective tive patient experiences [50]. Clinical encounters coded using
(e.g., self-concept). audiotapes, analyzed using the Roter
• Cognitive/affective influences that Interaction Analysis System [39]
show how communication is related
to strategy (e.g., goals), attributions
(e.g., stereotypical), and trust.
• Communication influences refer to
how the patient and the provider
tailor their responses to create a
coherent and effective exchange
[40].
Recipients [31]: Recipients are individuals who See below See below
• Motivations influence implementation processes
• Values and beliefs and those who are affected by
• Goals implementation outcomes, both at
• Skills the individual and collective team
• Knowledge levels. Recipients can facilitate uptake
• Time, resources, support of an innovation or resist its
• Local opinion leaders implementation [31].
• Collaboration/ teamwork
• Existing networks
• Learning environment
• Power and authority
• Presence of boundaries
*Recipients: providers In a healthcare setting, providers and Physicians who consider themselves Quantitative:
and staff: staff are the people who administer “liberal” spent more time giving more • Implicit Association Test to assess
Culturally relevant factors the innovation. information to patients than those implicit bias [48]
include [35]: A providers’ objectives and beliefs who consider themselves • Surveys of relevant practice,
• Demographics (e.g., about a patient affect how they “conservative” [40]. knowledge, attitudes, or skills [74, 75]
neighborhood immigrant behave during the patient-provider Providers may engage in more • Colorblind Racism Scale [76]
status) interaction [72]. detailed conversations about the Qualitative:
• Unconscious/implicit bias Providers, especially in busy healthcare health status of educated patients, yet • Analysis of taped conversation
• Knowledge and attitudes settings, may be vulnerable to provide basic explanations for less- between provider and patient [39,
• Skillsets subconscious bias and stereotypes educated patients [40]. 48]
[73]. During a post-angiogram encounter, • Participant observation [77]Woodward et al. Implementation Science Communications (2021) 2:61 Page 9 of 16
Table 1 Definitions, illustrative examples, and sample measures of the Health Equity Implementation Framework (Continued)
Domain and Definition Illustrative example(s) Sample measuresa
determinants
physicians perceived patients of lower • One-on-one interviews [78]
socioeconomic status as having more
negative personality characteristics
that include lack of self-control and
more negative behavioral tendencies
[38].
*Recipients: patients: In a healthcare setting, patients are Asian American patients in Hawaii Quantitative [34]:
Culturally relevant factors the people (individuals, families, participated less in their medical visits • Telephone survey of a random
include [34, 35, 45, 79–81]: caregivers) who will actually receive than mainland Americans [82]. sample of residents
• Medical mistrust the innovation. Culturally relevant Patients with more formal educations • Medical Mistrust Index [84]
• Health literacy and factors are associated with health and are more expressive and tend to want • Measures of underutilization of
numeracy healthcare disparities and can include to play a role in the decision-making health services
• Demographics (e.g., demographic factors, beliefs, process than less educated patients • Health literacy question [85]
neighborhood, immigrant information, and biological or genetic [40]. • Health numeracy question [86]
status) conditions related to equitable Many patients are unsure about their • Appropriated Racial Oppression Scale
• Socioeconomic status, implementation. role in the encounter and the [87]
including household appropriateness of their participation Qualitative:
income, net wealth, health [83]. • Interview about expectations for
insurance status, education treatment or the patient-provider-
level interaction [39, 88]
• Expectations about • Interviews about experience seeking
therapeutic relationships care [89]
• Beliefs and preferences
Inner context (local) [26]: The immediate local setting of Among 303 providers working in 49 Quantitative:
• Formal and informal implementation. Examples include: publicly funded health programs for • Perceptions of Supervisory Support
leadership support • Ward youths, providers’ perception of Scale [92]
• Culture • Unit certain leadership styles was • Organizational commitment [93]
• Previous experience of • Clinic associated with stronger provider • Readiness for Organizational Change
innovation or change • Hospital department willingness to adopt evidence-based measure [94]
• Change mechanisms for treatments [90]. • Validated inner setting measures [95]
embedding innovation Pisando Fuerte is a fall prevention Qualitative [96]:
• Evaluation and feedback program linguistically and culturally • Site visit
processes tailored for Latino individuals at risk for • Key informant interviews about
falls. It is adapted from “Stepping On,” inclusivity
an evidence-based fall prevention pro- • Stakeholder meetings or focus
gram. Fidelity to Pisando Fuerte was groups with providers about their
subpar; when comparing fidelity be- understanding of equitable care
tween the two sites, fidelity was lower • Public forums and listening sessions
in the site that did not give additional • Provider and staff interviews to
time to implement the program (poor determine actual practice and
leadership support) and had no ex- processes [97]
perience in organizing programs like
Pisando Fuerte (no previous experi-
ence of innovation) [91].
Inner context The organizational atmosphere in Hospitals’ adoption of the Culturally Quantitative:
(organizational) [26]: which the unit or team is embedded. and Linguistically Appropriate Services • Measures of organizational readiness
• Organizational priorities standards focused on retaining for change [100]
• Senior leadership and translators and adapting culturally and • Cultural Competency Assessment
management support linguistically appropriate materials. Tool for Hospitals [98]
• Culture However, this adoption did not often Qualitative [101]:
• Structure and systems include engagement in broader • Key informant interviews assessing
• History of innovation and organizational change [98]. knowledge/action of policies about
change Researchers studied a disparity- equity
• Absorptive capacity reduction program in Israel across 26 • Key informant interviews assessing
• Learning networks clinics and 109 clinical teams. After 3 beliefs organization holds about
years, they found different inner con- marginalized people
text configurations of factors predict- • Stakeholder meetings about the
ing disparity reduction. One example importance of equitable care
of a successful configuration was • Public forums and listening sessions
clinics with a large disparity gap to [102]
minimize, high clinic density, high per- • Focus groups
ceived team effectiveness, and focused
efforts on tailoring services to their en-
rollee patients [99].
Outer context This is the broader context defined in Researchers examined predisposing, Qualitative:Woodward et al. Implementation Science Communications (2021) 2:61 Page 10 of 16
Table 1 Definitions, illustrative examples, and sample measures of the Health Equity Implementation Framework (Continued)
Domain and Definition Illustrative example(s) Sample measuresa
determinants
(healthcare system) [26]: terms of resources, culture, leadership, enabling, and need factors as • Archival analysis, reading and
• Policy drivers and and orientation to evaluation and predictors of changes in healthcare documenting policies, program
priorities learning. utilization and found that patients’ manuals, or procedural protocols
• Incentives and mandates There is an increasing amount of experiences differed by group within [103, 104]
• Regulatory frameworks research that shows that inequities in the healthcare system and impacted • Interviews with leadership [99]
or external accreditation obtaining preventative care among their beliefs and attitudes about Quantitative:
systems racial and ethnic minorities compared receiving healthcare, ultimately • 15 core measures of healthcare
• Inter-organizational net- with non-Hispanic whites are due to affecting the extent to which qualit y[105]
works and relationships “organizational characteristics, includ- healthcare services were utilized [50]. • Population surveys
ing location, resources, and complexity • Social network analysis of
of a clinic or practice” [35]. relationships between relevant
leadership and/or teams [99]
• Existing reports hospital-wide scores
on assessments of care and equity,
e.g., National Quality Forum or
Healthcare Equality Index [106]
*Societal context [41, 42]: Forces outside the healthcare system See below See below
• Economies that influence all other domains and
• Physical structures determinants of implementation may
• Sociopolitical forces include but be broader than social
• Up-, mid-, or determinants of health, may focus on
downstream social the presence of stigma and
determinants of health [44] discrimination such as racism, classism,
or transphobia (as examples) and the
institutionalization of such
discrimination in every determinant of
implementation.b,c
*Economies [53]: The structure of the city, state, or In a study assessing longitudinal Quantitative:
• Traditional country related to the wealth and effects of health insurance and • Insurance claims data
• Command resources of people and what is poverty, researchers reported low- • Gross domestic product [108]
• Market exchanged for healthcare delivery income, middle-aged adults in the U.S. • Gross national product [109]
• Mixed (e.g., insurance). This can be divided with no insurance, unstable coverage, • Minimum wage [110]
into human resources (i.e., labor, or changes in insurance have higher • Population and total employment
management) and non-human re- out-of-pocket expenditures and finan- [111]
sources (i.e., land, capital goods, finan- cial burdens than public insurance • Annual average wage level of the
cial resources, and technology) [55]. holders [107]. primary, secondary, and tertiary
In a case study, the presence of industries [112]
chronic kidney disease indicators in • Tax revenue as a percentage of total
the pay-for-performance system in pri- revenue [113]
mary care created an incentive for im- • Interest rate on saving deposits and
provement [26]. inflation rate [114]
Qualitative [115]:
• Key informant interviews about
goods and services exchanged [116]
• Analysis of comparative economic
structure [115]
*Physical structures: The physical environment, structure, One study compared Black and White Quantitative:
• Location location of services, and recipients, Americans who were exposed to the • Indices of segregation [119]b
• Availability of public also known as the built environment same set of socioeconomic, social, and • Public data such as hospitals per
transportation as it relates to equitable environmental conditions in an area of capita, public transportation trips per
• Actual environment of implementation [55]. one U.S. city. Although there is robust capita, car ownership, revenue
the point-to-care research documenting disparities in dedicated to parks and recreation,
• Language spoken and/or hypertension, diabetes, obesity, and transportation, other infrastructure
signage use of health services by race among needs, and grocery stores per capita
• Available structures in national samples, within the racially • Center on Budget and Policy
one’s neighborhood to use integrated city in the study, disparities Priorities data
innovation in these health conditions were either • State Departments of Finance and
• Grocery stores absent or significantly smaller. Thus, Administration [55]
• Healthcare facilities the place where people lived had an Qualitative:
• Local businesses impact on their health conditions, • Windshield and walking surveys
• Physical infrastructure beyond race [117]. include assessing infrastructure;
In a qualitative study of transgender surveyors are on foot and take note
individuals’ experiences in residential of the neighborhood related to the
addiction treatment, researchers physical or built environment [120].
observed that residential facilities that
split the milieu and housing based onWoodward et al. Implementation Science Communications (2021) 2:61 Page 11 of 16
Table 1 Definitions, illustrative examples, and sample measures of the Health Equity Implementation Framework (Continued)
Domain and Definition Illustrative example(s) Sample measuresa
determinants
the gender binary may be
stigmatizing people who identify as
transgender or gender non-
conforming [118].
*Sociopolitical forces [41, Policies and procedures, formal or In a U.S. study on the adoption of Quantitative:
43, 57]: informal, in national and local behavioral health evidence-based • Select measures of determinants of
• Policy climate governments that systemically inhibit treatment by states, the following policy implementation, such as
• Political support or promote equitable health. were some factors that played a role: visibility of policy actors or policy
• Laws state characteristics, state fiscal sup- implementation climate [121]
• Local culture ports to promote innovation adoption, • The State-Level Racism Index [122]b
• Social movements or and state policy that supports to pro- Qualitative:
structures such as racism, mote evidence-based treatment adop- • INCLENS equity lens: examines
classism, heterosexism, tion [57]. whether clinical guidelines address
transphobiac health needs and inequities
experienced by marginalized groups
[123]
• Interview questions with recipients
about laws, policies, or social
movements relevant to the
innovation
• Archival analysis of policy documents
[103, 104]
*Health equity domains adapted to i-PARIHS
a
Measures or data collection methods are examples from literature; for a repository of implementation science measures, see the Society for Implementation
Research Collaboration’s Instrument Review Project [124]
b
For a repository of measures specific to racism, see Appendix B of Racism: Science & Tools for the Public Health Professional [125]
c
Implementation scientists should review existing measurement tools specific to health disparities in your area of interest or study to further integrate health
equity into implementation
of different races and incomes may be due to (1) the and equitable delivery of healthcare. Consider these
innovation was developed and tested in samples of health equity determinants in developing a logic
mostly White people such that it is not acceptable to or model to explain the implementation process, includ-
effective for Black people (characteristic of the ing its mechanisms of change.
innovation), (2) providers do not offer the innovation as
often to Black patients as they do to White patients Use framework determinants to conduct and tailor
(clinical encounter), (3) there may not be many Black or implementation
lower-income people served at the hospital (outer con- After formative evaluation or initial diagnosis of the im-
text), or (4) the hospital is not readily accessible via pub- plementation disparity is complete, the areas for change
lic transportation to people with lower incomes who do will become clear and implementation strategies will
not have motor vehicles (physical structure). There may need to be selected and tailored to local context and re-
be some known or unknown determinant within any do- cipients with careful attention to equity and justice.
main of the Health Equity Implementation Framework There are many existing ways to use information from
contributing to implementation disparities; perhaps pro- formative evaluation to select and tailor implementation
viders have unconscious biases toward Black people (a strategies [128–130]. To address implementation dispar-
factor within the cultural recipients domain) that lead to ities, explicitly include determinants of inequity in
them offering the innovation less frequently to Black pa- selecting and tailoring strategies, as well as unique bar-
tients than to White (clinical encounter). The key factor riers that may prevent organizations from addressing
to change would be unconscious bias to affect provider these inequities. For example, there may be a need to
behavior and alter the clinical encounter. To the extent use community- or patient-informed strategies to repair
possible, one can hypothesize which factor is the lever harm and build trust among patient recipients who have
for more equitable implementation—which of these been and are marginalized in healthcare systems, im-
factors, if changed, would result in the innovation be- prove cultural and structural competence at all levels of
ing received by more people with lower incomes and an organization, or continuously monitor reach between
more Black people at that hospital? These levers are patient subgroups to detect change in disparities. Al-
mechanisms of implementation disparities (areas to though some are focusing on equity more in using im-
change with implementation strategies) for more just plementation strategies [33, 91, 99, 131], there isWoodward et al. Implementation Science Communications (2021) 2:61 Page 12 of 16
considerably more work to be done on this, and careful levels in implementation science and practice will eluci-
attention to equity elements is needed to tailor date drivers of health inequities such as structural ra-
implementation. cism, heterosexism, and patriarchy. Thus, the discovery
As implementation progresses, an implementation of these drivers of health inequities should necessitate
plan will need to be adapted as determinants change. implementation strategies to overcome or resolve such
The Health Equity Implementation Framework can be complex and oppressive structures. Future research
useful for determining areas to assess repeatedly and should focus on implementation strategies (or other pro-
thus, intervene on, throughout implementation. Doing cesses) used to address health equity determinants of
so ensures an equity lens is applied throughout imple- unjust health inequities in our healthcare systems and
mentation and that implementation processes, such as societies.
planning, strategy use, and goal setting, are thoughtfully We have only piloted the three health equity domains
executed according to dynamic needs. Repeated assess- within the context of a determinant framework; however,
ments can be done informally through observations, they may be suitable as process or evaluation variables. As
consultations with recipients and leadership, or more this framework evolves through implementation research
formally through mixed methods, including ones men- and we have more data to inform its application, future
tioned in Table 1 and used previously in formative considerations could include that some of these domains
evaluation [63]. for determinants should also be outcomes of implementa-
tion disparity reduction efforts. For an implementation
Writing implementation reports or findings process framework that incorporates an equity lens, see
For documenting the results of an implementation ef- frameworks proposed by Nápoles and Stewart [132] and
fort, clarify how the Health Equity Implementation Eslava-Schmalbach and colleagues [133]. For an imple-
Framework or its three health equity domains were in- mentation evaluation framework that incorporates an
corporated. For example, barriers and facilitators from equity lens, see preliminary equity-focused implementa-
formative evaluation may be presented by framework tion outcomes [133] and the proposed extension of the
domains. As implementation progresses, a team may RE-AIM framework [134].
want to document key changes within domains from the There are limitations to our framework and practical
Health Equity Implementation Framework, similar to guidance presented here. We have piloted test many, but
how ongoing implementation barriers and facilitators not all, the feasibility and acceptability of the steps we
were recorded for the study that examined the imple- described using three health equity domains and mea-
mentation of legally sanctioned supervised consumption sures in Table 1. However, we suggest these as starting
services in Canada [59]. The mixed method approaches places, and with confidence, as they all have entire bod-
suggested earlier will provide key information to be re- ies of science showcasing their relevance to health
ported, making clear why implementation was successful equity. We limited the application of this framework to
or not, and how certain strategies affected whether dis- healthcare settings, although it could be adapted to com-
parities in receipt, use, access to, or quality of an munity or school settings. Although health equity can be
innovation were reduced [6]. incorporated across several determinant frameworks, we
provided a detailed application of health equity domains
Discussion tied to i-PARIHS. They have the potential for broader
Disparities in healthcare occur in implementation out- applications to other implementation science frame-
comes and patient health outcomes. Implementation dis- works. This has not been piloted yet to our knowledge.
parities are rooted in social injustice, exacerbated by
multiple inputs, such as societal context, patient mis- Conclusion
trust, provider bias, and poor patient-provider interac- Implementation researchers and practitioners must
tions. The three health equity domains presented in adopt a health equity lens as foundational to any
more depth here are key adaptations for implementation research-practice gap where inequity exists. Researchers
researchers and suggested to adapt one’s preferred im- might collect data on the feasibility, acceptability, and
plementation framework (e.g., EPIS) to incorporate an predictive utility of health equity determinants in this
equity lens and account for inputs contributing to imple- burgeoning area of implementation science. The Health
mentation disparities. Three health equity domains from Equity Implementation Framework is an implementation
the Health Equity Implementation Framework can be determinant frameworks to capture and understand bar-
studied as determinants of implementation, as show- riers and facilitators to health inequities [23, 135]. The
cased in the application to services for developmental applications, steps, and tools in the manuscript are one
disabilities in California. We propose that an increased step toward systematic integration of health equity and
focus on health equity explicitly at multiple ecological implementation science in frameworks.You can also read