Abdominal Pain in the Roux-en-Y Gastric Bypass Patient - USA Health System
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
THE RED SECTION 161
see related editorial on page x
Abdominal Pain in the Roux-en-Y Gastric Bypass
HOW I APPROACH IT
Patient
Allison R. Schulman, MD, MPH1, 2 and Christopher C. Thompson, MD, MSc, FASGE, FACG AGAF1, 2
Am J Gastroenterol 2018; 113:161–166; doi:10.1038/ajg.2017.361; published online 10 October 2017
INTRODUCTION following RYGB (Figure 3). Marginal ulceration occurs in up to
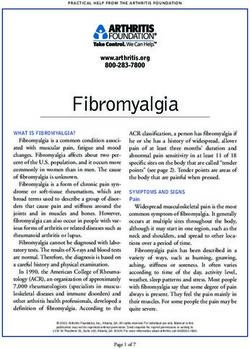
Roux-en-Y gastric bypass (RYGB) is a common bariatric surgical 16% of patients, and can develop from weeks to years following
procedure resulting in weight loss and resolution of comorbidi- surgery (1,2). The pain is often described as constant, gnawing,
ties. It involves partitioning of the upper portion of the stomach sometimes incapacitating, and may or may not be affected by
to create a small gastric pouch, along with diversion of oral intake meals. Additional symptoms, such as nausea, vomiting, lack of
and biliopancreatic digestive enzymes to the distal small bowel, appetite, or gastrointestinal bleeding may also be present. Con-
via creation of a Roux limb (Figure 1). comitant mid-epigastric pain and anemia strongly suggests the
Abdominal pain is common in patients who have undergone presence of a marginal ulceration, as chronic occult bleeding may
RYGB, although existent literature is variably sparse. Numerous cause anemia in as many as 10.2% of patients after RYGB (4).
studies focus on conditions such as marginal ulceration, and fewer Physical exam often demonstrates tenderness to palpation in the
studies describe other causes (1,2). In a large retrospective study of epigastric region.
1,429 RYGB patients, over one-third presented with abdominal pain Marginal ulcerations can be due to several factors. Acid produc-
(3). This is likely an underestimate as this study was not performed tion is important in the formation of marginal ulcerations. The gas-
in a closed setting, and oftentimes patients will be admitted to other tric pouch produces a small amount of acid, with larger pouches
hospitals or change health-care providers. A standard abdominal producing more acid. The jejunum, unlike the duodenum, is sus-
pain work-up evaluating potential etiologies unrelated to bariatric ceptible to even small amounts of acid production, as the mucosa
surgery should be pursued as appropriate, including but not lim- does not secrete bicarbonate, and it is not in proximity to bicar-
ited to cardiovascular disease, pancreatitis, appendicitis, functional bonate-rich pancreatic secretions. Gastrogastric fistula (Figure 4)
pain, splenic infarcts or abscesses, pulmonary processes, or vascular allow larger amounts of acid to enter the pouch and jejunum from
evaluation for what would be considered an atypical presentation. the gastric remnant, amplifying this effect. Another element in the
These and other rare causes of abdominal pain that are not unique pathophysiology of marginal ulcerations is tissue ischemia. This
to gastric bypass will not be addressed in this review. typically involves small vessel ischemia, such as seen with diabetes
A surgery specific work-up should also be pursued, with atten- and tobacco use. Other contributory factors include inciting medi-
tion to unique diagnostic strategies and treatment plans. With this cation such as nonsteroidal anti-inflammatory drugs, Helicobacter
in mind, patient history and physical examination are often essen- pylori, and foreign material such as surgical suture.
tial in making a diagnosis, with prioritization of diagnostic stud- Upper endoscopy is important to diagnose, assess the severity
ies depending on initial presenting symptoms. Symptoms may be of, and monitor healing of ulceration. Additionally, the diagnos-
suggestive of a particular diagnosis, but they are seldom pathogno- tic strategy for H. pylori is different from that in the non-bypass
monic. Below, we discuss the most common diagnoses tied to type population. The preferred diagnostic studies include fecal antigen,
and location of abdominal pain; however, there is no doubt that off proton pump inhibitor (PPI) therapy for 2 weeks, and serology,
there is overlap between symptoms and other diagnoses. We also if there is no history of exposure. In our experience, pouch biop-
propose a suggested treatment algorithm (Figure 2) and manage- sies (rapid urease or histology) and breath tests are less reliable in
ment strategy (Table 1), although additional studies are underway this patient population, as the majority of the stomach where H.
to solidify the approach. pylori resides is inaccessible, and therefore can yield false-negative
results.
Epigastric pain There are also some unique treatment considerations. PPIs are
Ulceration at the gastrojejunal anastomosis, also known as mar- typically effective in the management of marginal ulcerations, and
ginal ulceration, is the most common cause of epigastric pain should be opened or prescribed in soluble form. Owing to rapid
1
Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women’s Hospital, Boston, Massachusetts, USA; 2Harvard Medical School, Boston,
Massachusetts, USA. Correspondence: Christopher C. Thompson, MD, MSc, FACG, FASGE, AGAF, Division of Gastroenterology, Hepatology and Endoscopy,
Brigham and Women’s Hospital, 75 Francis Street, ASB II, Boston, Massachusetts 02115, USA. E-mail: cthompson@hms.harvard.edu
© 2018 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY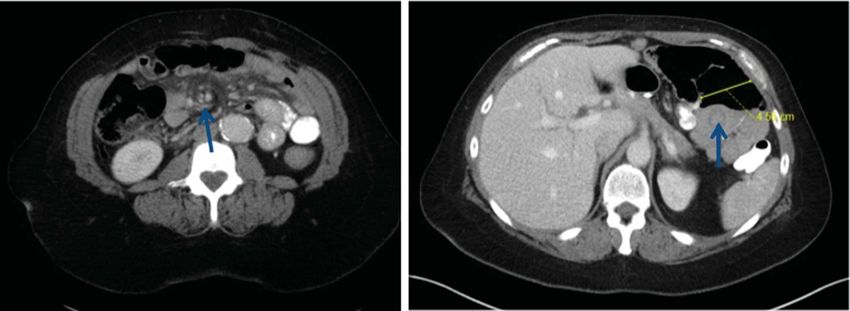
162 THE RED SECTION
Right upper quadrant pain
Right upper quadrant pain, particularly within the first 24 months
following bariatric surgery, warrants investigation of gallstone
disease. The highest risk period for development of this disorder
HOW I APPROACH IT
is during the rapid weight loss phase, and decreases to a minimum
once the weight has stabilized (8). Aside from rapid weight loss,
postoperative anatomic changes and compromised gallbladder
emptying may also play a role in its development. Pain that pro-
longs beyond 6h may favor choledocholithiasis over biliary colic,
and fevers or leukocytosis raise concern for cholangitis. Physical
exam demonstrates pain in the right upper quadrant or epigastric
region. Elevated bilirubin, alkaline phosphatase, and GGT are all
independent predictors of choledocholithiasis. Abdominal ultra-
sound or magnetic resonance cholangiopancreatography should
be performed as a first-line test to evaluate for these conditions.
Endoscopic retrograde cholangiopancreatography is particu-
larly challenging in RYGB anatomy, and oftentimes requires a
pediatric colonoscope, spiral overtube, balloon-assisted entero-
scope, or a duodenoscope back-loaded onto a guidewire. Addi-
tionally, endoscopic ultrasound (EUS)-guided access (Figure 5)
Roux-en-Y and laparoscopic-assisted procedures may have advantages over
gastric bypass these techniques (9,10). Choice of procedure is dependent on local
(RYGB)
expertise and severity of illness, with acutely ill patients likely ben-
efitting from a percutaneous approach. Patients who are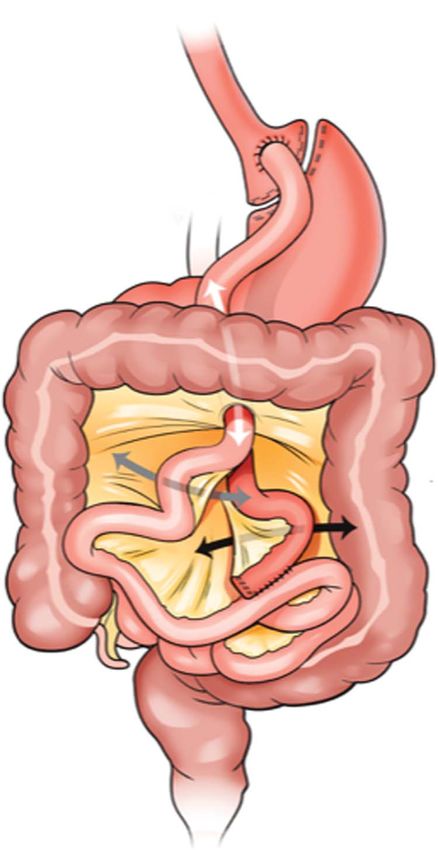
THE RED SECTION 163
Abdominal pain in RYGB*
Site-specific
–
work-up
Physical exam Carnett’s sign
+
HOW I APPROACH IT
Pain referral
If unresponsive
to therapy
Epigastric pain RUQ pain LUQ pain Diffuse pain
EGD
Mild to Severe, Mild to severe
EGD RUQ u/s moderate, intermittent moderate
or MRCP constant
+ – + –
Treat Cross- Treat Cross- Breath test Cross-
EGD EGD
condition sectional condition – sectional with transit sectional
imaging imaging time imaging
+ – + –
– –
–
Treat EGD Treat EGD
condition condition
Evaluate remnant vs. – –
empiric ursodiol
*Exclude non-GI causes as appropriate
Figure 2. Proposed treatment algorithm for abdominal pain in Roux-en-Y gastric bypass.
be considered. This is critical in patients who also have unex- lution of gastropathy on repeat histologic examination have been
plained anemia, as adenocarcinoma, mucosa-associated lymphoid demonstrated in small series (14).
tissue, and peptic ulceration have been described in the remnant
stomach. Diffuse discomfort
A more common condition that presents with this type Small intestinal bacterial overgrowth is a condition in which bac-
of pain is remnant gastropathy, which is likely due to mucosal teria proliferate in the intestine resulting in excessive inflamma-
atrophy owing to the lack of nutrient contact with the gas- tion, or malabsorption, and may cause diffuse or lower abdominal
tric mucosa and a chemical irritation due to pooling of bile. discomfort. Abdominal bloating and change in bowel habits often
Additionally, acid production continues in the remnant stomach accompany these symptoms, and should raise suspicion for this
without the buffering effects of food. Finally, the pooling condition. In fact, change in bowel habits and abdominal disten-
of bile due to the proximity of the papilla to the remnant, in tion may be the only symptoms. Hydrogen or methane breath
addition to a lack of antegrade flow, all contribute to mucosal tests are the diagnostic standard. These studies may be fraught
damage and resultant abdominal pain. Device-assisted enteros- with false positives, as there is also faster transit time in RYGB
copy with biopsy can be used to make the diagnosis; however, patients. As such, transit time to the colon should be estimated
this procedure is technically demanding, invasive, and only by small bowel follow through, and duration of breath test should
performed in a limited number of centers. Cholescintigraphy be adjusted to this transit time (15). The mainstay of treatment
(99mTc-heapto-iminodiacetic acid scanning), for patients with- includes antibiotic therapy, in addition to dietary changes and
out anemia, may be a less invasive means of identifying patients management of underlying causes.
at risk for remnant gastropathy. 99mTc-heapto-iminodiacetic
acid scans allow for a radiolabeled substance to be taken up Other presentations
selectively by hepatocytes and excreted into bile, thereby yield- It is important to keep in mind that the pain location is not with-
ing information about bile flow. Pooling of bile in the remnant out variation for the above conditions, and quality of pain must
stomach yields a positive test and may suggest increase risk for be taken into consideration. For instance, severe intermittent
bile acid gastropathy (13). abdominal pain typical of small bowel obstruction occurring in
If this condition is suspected, treatment with ursodeoxycholic a location other than the left upper quadrant still warrants urgent
acid, a secondary bile acid, should be considered. This medica- evaluation for obstructive processes. Additionally, pain referred
tion alters the composition of bile, halting the caustic damage and from other locations such as back and kidneys must also be con-
allowing the mucosa to heal. Elimination of symptoms and reso- sidered.
© 2018 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY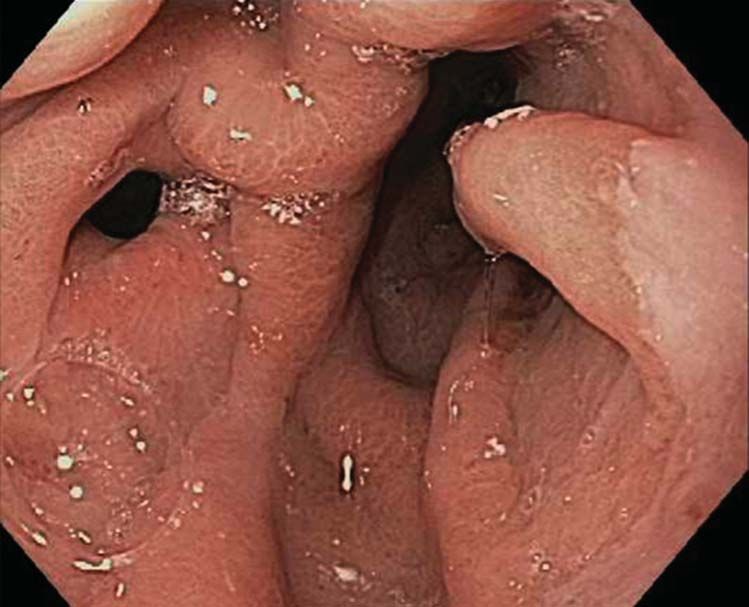
164 THE RED SECTION
Table 1. Common diagnoses and proposed management strategy
for abdominal pain in Roux-en-Y gastric bypass
Diagnosis Treatment
HOW I APPROACH IT
Marginal ulceration High dose PPI (soluble form)±sucralfate
Stop smoking
No NSAIDs
H. pylori stool antigen or serology
Foreign body removal using endoscopic scissors
Foreign body Endoscopic scissors to facilitate removal
Gastrogastric fistula If asymptomatic: PPI+dietary counseling
If symptomatic: closure (endoscopic (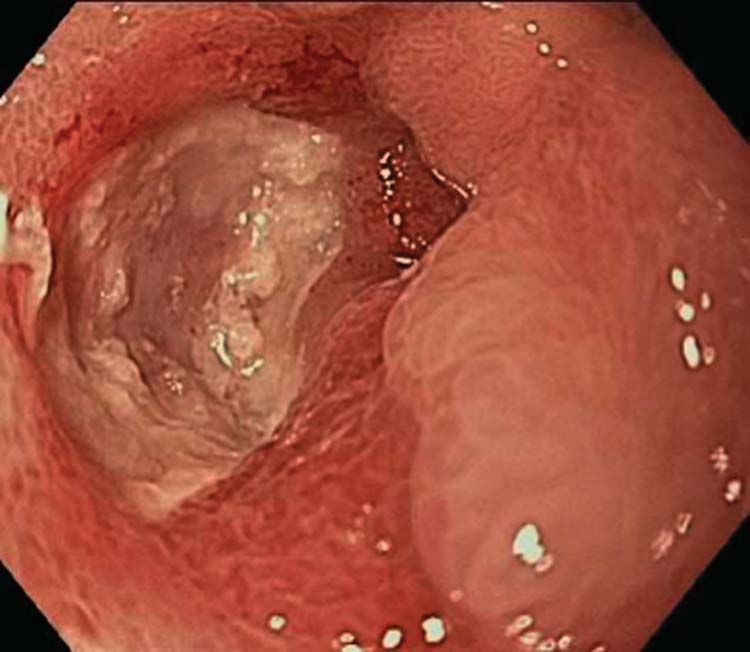
THE RED SECTION 165
a b
HOW I APPROACH IT
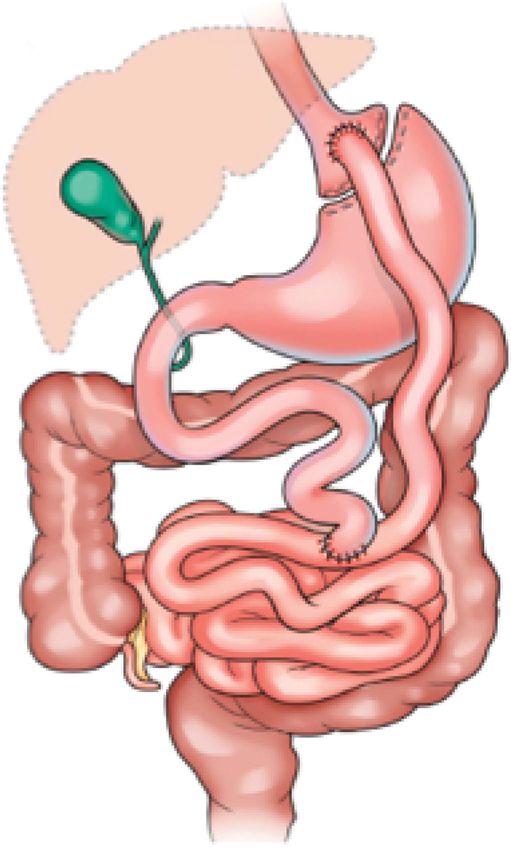
Figure 6. Examples of radiographic findings in patients with intestinal obstruction. Computed tomography demonstrating swirled appearance of mesenteric
vessels due to internal hernia (a) and “target sign” due to intussusception (b).
Table 2. Small bowel obstruction in Roux-en-Y gastric bypass
Etiology of Common locations Overall inci- Imaging findings Other features
obstruction dence (%)
Adhesions Can occur anywhere, 0.5–1.8 Abrupt change in bowel caliber without evidence of Open>laparoscopic
often near jejunojejunal other causes of obstruction Retrocolic>antecolic
anastomosis Acute angulation of small bowel loops Bimodal distribution (1 year)
Internal hernia Defect in transverse 3–16 “Swirl sign”: swirled appearance and twisting of Laparoscopic>open
(Figure 7) mesocolon (67%) bowel and mesenteric vessels (Sn: 79–100%; Sp: Retrocolic>antecolic
Defect at the jejunojejunos- 80–90%) Increased in pregnancy
tomy (21%) “Clustered loops”: abnormally clustered otherwise 2–3 years following RYGB
Space between transverse normal appearing loops of small bowel (Sn: 22–33%;
mesocolon and Roux limb Sp: 70–90%)
(Peterson’s hernia) (7.5%) Small-bowel obstruction (Sn: 11–22%; Sp: 11–80%)
Other (4.5%) “Mushroom sign”: A mushroom shape to the herni-
ated mesenteric root with associated crowding and/
or stretching of the mesenteric vessels (Sn: 0–56%;
Sp:100%)
“Hurricane eye”: tubular distal mesenteric fat sur-
rounded by bowel
“SMA sign”: bowel other than duodenum posterior to
the superior mesenteric artery
Right-sided location of the distal jejunojejunal anas-
tomosis (i.e., right-sided anastomosis)
Ventral inci- Laparotomy site 0.5–24 Defect in the abdominal wall Open>laparoscopic
sional hernia Trochar site External protrusion of bowel loops through defect Incision length/trochar size
Dilation of the bowel loops within the hernia Morbid obesity-->increased intra-
Normal/collapsed bowel distal to obstruction abdominal pressure-->increased
risk
Volvulus Mesenteric root
166 THE RED SECTION
the work-up strategy, and a thorough understanding of the diag-
nostic modalities is requisite to optimal care.
HOW I APPROACH IT
CONFLICT OF INTEREST
Guarantor of the article: Christopher C. Thompson, MD, MSc,
FASGE, FACG AGAF.
Specific author contributions: Allison R. Schulman—drafting of
the manuscript; this author has approved the final draft submitted.
Christopher C. Thompson—editing of the manuscript; this author
has approved the final draft submitted.
Financial support: None.
Potential competing interests: A. Schulman—has no personal or
financial conflicts of interest to disclose. C.C. Thompson—Apollo
Endosurgery (Consultant/Research Support); Olympus (Consultant/
Research Support); Boston Scientific (Consultant); Covidien (Con-
sultant, Royalty, Stock).
REFERENCES
1. Coblijn UK, Lagarde SM, de Castro SMM et al. Symptomatic marginal
ulcer disease after Roux-en-Y gastric bypass: incidence, risk factors and
management. Obes Surg 2015;25:805–11.
2. Azagury DE, Abu Dayyeh BK, Greenwalt IT et al. Marginal ulceration after
Roux-en-Y gastric bypass surgery: characteristics, risk factors, treatment,
and outcomes. Endoscopy 2011;43:950–4.
3. Høgestøl IK, Chahal-Kummen M, Eribe I et al. Chronic abdominal pain
and symptoms 5 years after gastric bypass for morbid obesity. Obes Surg
2016;27:1438–45.
4. Avgerinos DV, Llaguna OH, Seigerman M et al. Incidence and risk factors
for the development of anemia following gastric bypass surgery. World J
Gastroenterol 2010;16:1867–70.
5. Schulman AR, Chan WW, Devery A et al. Opened proton pump inhibitor
capsules reduce time to healing compared with intact capsules for marginal
ulceration following Roux-en-Y gastric bypass. Clin Gastroenterol Hepatol
Figure 7. Three potential sites for internal hernia location following Roux-en- 2016;15:494–500.e1.
Y gastric bypass including the defect in the transverse mesocolon through 6. Ryou M, Mogabgab O, Lautz DB et al. Endoscopic foreign body removal
which the Roux limb passes (white arrow), through the mesenteric defect at for treatment of chronic abdominal pain in patients after Roux-en-Y gastric
bypass. Surg Obes Relat Dis 2010;6:526–31.
the jejunojejunostomy (black arrow) and the space between the transverse
7. Pauli EM, Beshir H, Mathew A. Gastrogastric fistulae following gastric
mesocolon and the Roux limb known as Peterson’s hernia (gray arrow). bypass surgery—clinical recognition and treatment. Curr Gastroenterol
Rep 2014;16:405.
8. Karadeniz M, Gorgun M, Kara C. The evaluation of gallstone formation in
anesthetic is injected directly into the site of pain, or neuroma patients undergoing Roux-en-Y gastric bypass due to morbid obesity. Turk-
resection. ish J Surg 2014;30:76–9.
9. Thompson CC, Ryou MK, Kumar N et al. Single-session EUS-guided
A growing number of studies have provided information
transgastric ERCP in the gastric bypass patient. Gastrointest Endosc
regarding the frequency of addiction and alcohol consumption, 2014;80:517.
and possible changes in the effects of consuming alcohol fol- 10. Kedia P, Kumta N, Widmer J et al. Endoscopic ultrasound-directed
transgastric ERCP (EDGE) for Roux-en-Y anatomy: a novel technique.
lowing bariatric surgery. Narcotic bowel, withdrawal, and drug-
Endoscopy 2015;47:159–63.
seeking behavior can all mimic the above symptomatology. These 11. Tsai J-H, Ferrell LD, Tan V et al. Aggressive non-alcoholic steatohepatitis fol-
issues should be included in a detailed patient history. lowing rapid weight loss and/or malnutrition. Mod Pathol 2017;30:834–42.
12. Elms L, Moon RC, Varnadore S et al. Causes of small bowel obstruction af-
ter Roux-en-Y gastric bypass: a review of 2,395 cases at a single institution.
Surg Endosc 2014;28:1624–8.
CONCLUSION 13. Schulman AR, Thompson CC. Utility of bile acid scintigraphy in the
diagnosis of remnant gastritis in patients with Roux-en-Y gastric bypass.
Abdominal pain is extremely common in patients who have
Gastrointest Endosc 2016;83:AB327–8.
undergone RYGB, and the evaluation has several unique features 14. Kumar N, Thompson CC. Ursodiol is effective for treatment of abdominal
that should not be overlooked. As gastroenterologists encoun- pain associated with gastritis of the remnant stomach in Roux-en-Y gastric
bypass patients. Gastroenterology 2013;144:S-270.
ter these patients with ever increasing frequency, it is important
15. Abidi W, Chan WW, Thompson CC. Breath testing for small intestinal
that we familiarize ourselves with the surgical anatomy and likely bacterial overgrowth in Roux-en-Y gastric bypass patients: the impor-
complications. Pain quality and location are helpful in directing tance of orocecal transit time. Gastroenterology 2016;150:S688–9.
The American Journal of GASTROENTEROLOGY VOLUME 113 | FEBRUARY 2018 www.nature.com/ajgGASTROENTEROLOGY ARTICLE OF THE WEEK
April 26, 2018
Schulman AR, Thompson CC. Abdominal pain in the Roux-en-Y gastric bypass patient.
Am J Gastroenterol 2018;113:161-166
1. True statements regarding marginal ulcerations include
a. Do not respond to PPI
b. Tissue ischemia may be a contributing factor
c. Bile salt injury plays an important role
d. Gastrogastric fistula may be a possible cause
True or False
2. Bypass surgery reduces risk of cholelithiasis as patients lose weight.
3. Remnant gastropathy can be a cause of LUQ pain, treatment with ursodeoxycholic acid may
help
4. The most common cause of epigastric pain after bypass surgery is marginal ulceration
5. Left upper quadrant pain should raise suspicion for an internal hernia, endoscopy is the
diagnostic test of choice
6. Visible suture material at the anastomotic site is normal and does not contribute to pain.
7. H. pylori infection of the gastric pouch is best diagnosed by stool antigen tests and not only
gastric pouch biopsies
8. PPI therapy for marginal ulceration should be given as soluble forms or sprinkled on foodsYou can also read