Addiction vs. Pseudo-addiction or 50 Shades of Aberrant Opioid Use - Clifford Q Cabansag, MD, CTTS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Addiction vs. Pseudo-addiction
or
50 Shades of Aberrant Opioid Use
Clifford Q Cabansag, MD, CTTS
Addiction Medicine Physician
Tobacco Treatment Specialist
Adjunct Assistant Professor
Department of Psychiatry and Behavioral Neuroscience
September 26, 2014
Disclosures • NONE
Vocabulary • Opioid vs. opiate • Addiction • Substance use disorders • Tolerance • Withdrawal • Abuse • Pseudo-addiction • Misuse • Diversion
Age-adjusted drug-poisoning and opioid-analgesic poisoning death rates: United States, 1999–2011 SOURCE: CDC/NCHS, National Vital Statistics System, Mortality File.
Number of opioid-analgesic poisoning deaths, by opioid analgesic category: United States, 1999–2011 SOURCE: CDC/NCHS, National Vital Statistics System, Mortality File.

History
• CA 1872 – 1st anti-opium law
• Administration of opium a felony
• Private use not addressed
• Separate bureau to enforce narcotic laws
• Among 1st states to treat
• CT 1874
• Narcotic addict legally incompetent
• By law committed to state insane asylum
• For “medical care and treatment”
• NV 1877 – 1st state opium illegal without MD Rx
• OR 1887 – 1st comprehensive anti-substance lawHistory • USA 1914 – Harrison Narcotic Act • "An Act to provide for the registration of, with collectors of internal revenuer and to impose a special tax upon all persons who produce, import, manufacture, compound, deal in, dispense, sell, distribute, or give away opium or coca leaves, their salts, derivatives or preparations, and for other purposes.“ • Clause "in the course of his professional practice only" interpreted by law-enforcement to mean a doctor could not prescribe simply to maintain addiction
Other Factors • JCAHO – 2001 • Installs Quality Standard on pain identification • ↑ ID & treatment of pain strongly encouraged • Development of new and very effective opioids • Tremendous rise in Rx of opioids for NC pain
FSMB Model Policy Basic Tenets • Pain manage important & integral to practice of med • Use of opioids may be necessary for pain relief • Use of opioids for other than legitimate medical purpose poses threat to individual and society • Physicians have responsibility to minimize potential for abuse and diversion • Physicians may deviate from recommended treatment steps based on good cause • Not meant to constrain/dictate medical decision-making FSMB, Federation of State Medical Boards
Tomato Tomahto • OpiATES – • 20+ Natural derivatives of Papaver somniferum • Psychoactive: morphine / codeine / thebaine • OpiOIDS • Capable of binding opioid receptor • By default opiates included • ALL opiates are OPIOIDS • Only SOME opioids are OPIATES
Other Opioids • Heroin - diacetymorphine • Semi-synthetics • Buprenorphine / Subutex (+ naloxone = Suboxone) • Hydrocodone / Zohydro (+ APAP = Vicodin, Lortab) • Oxycodone / Oxycontin (+APAP = Percocet) • Oxymorphone / Opana • Hydromorphone / Dilaudid • Synthetics • Methadone / Dolophine • Fentanyl / Duragesic / Sublimaze • Propoxyphene / Darvon
Tis’ the Season
DSM-IV • Confusing • 2 categories • Substance ‘abuse’ vs. Substance ‘dependence’ • Assumption • ‘abuse’ = mild / early phase • ‘dependence’ = more severe • Problem – abuse criteria quite severe • Failure to fulfill work / home / school obligations • Use in physically hazardous situations • Associated legal problems • Cont’d use despite social / interpersonal problems
DSM-IV • Differentiating abuse vs. dependence unclear • Seemingly arbitrary • Differences did not reflect real life • Confusion RE: • Physical dependence vs. Substance dependence
DSM-5 vs. DSM-IV • Integrates two DSM–IV entities substance abuse and substance dependence • A single disorder – Substance Use Disorder • Sub classifications • mild / moderate / severe • dependent on number criteria met • Discards legal problems as criterion • Adds craving to criteria
DSM-5 SUD
A maladaptive pattern of substance use leading to clinically significant
impairment or distress, as manifested by 2 (or more) of the following,
occurring within a 12-month period:
1. recurrent substance use resulting in a failure to fulfill major role
obligations at work, school, or home (e.g., repeated absences or poor
work performance related to substance use; substance-related
absences, suspensions, or expulsions from school; neglect of children
or household)
2. recurrent substance use in situations in which it is physically
hazardous (e.g., driving an automobile or operating a machine when
impaired by substance use)DSM-5 SUD
3. continued substance use despite having persistent or recurrent
social or interpersonal problems caused or exacerbated by the effects
of the substance (e.g., arguments with spouse about consequences of
intoxication, physical fights)
4. tolerance, as defined by either of the following:
a. a need for markedly increased amounts of the substance to
achieve intoxication or desired effect
b. markedly diminished effect with continued use of the same
amount of the substance (Note: Tolerance is not counted for those
taking medications under medical supervision such as analgesics,
antidepressants, ant-anxiety medications or beta-blockers.)DSM-5 SUD
5. withdrawal, as manifested by either of the following:
a. the characteristic withdrawal syndrome for the substance
(refer to Criteria A and B of the criteria sets for Withdrawal from the
specific substances)
b. the same (or a closely related) substance is taken to relieve
or avoid withdrawal symptoms (Note: Withdrawal is not counted for
those taking medications under medical supervision such as
analgesics, antidepressants, anti-anxiety medications or beta-blockers.)
6. the substance is often taken in larger amounts or over a longer
period than was intended
7. there is a persistent desire or unsuccessful efforts to cut down or
control substance useDSM-5 SUD
8. a great deal of time is spent in activities necessary to obtain the
substance, use the substance, or recover from its effects
9. important social, occupational, or recreational activities are given
up or reduced because of substance use
10. the substance use is continued despite knowledge of having a
persistent or recurrent physical or psychological problem that is likely to
have been caused or exacerbated by the substance
11. Craving or a strong desire or urge to use a specific substancePerpetuation of Stigma
Power of language
• ‘Addicts’ vs. pt’s with substance use disorders
• Person vs. disease
• ‘Drug seekers’ vs. relief seeking
• All pt’s ‘seeking’ medication
• Testing terminology - Unique to SUD’s***
• Inherently confrontational
• ‘Choice’ / ‘weakness’ vs. chronic disease
• Other people …..
• ‘Just put it down / quit’
• Nancy Reagan “Just say No!”***Perpetuation of Stigma
Power of language
• Underlying fallacy
• People ‘like’ their circumstances and choose to remain
• Something inherently wrong / faulty / inferior / different
• Term ‘abuse’ - pejorative
• Child / Elder / Physical / Sexual / Verbal - ‘abuse’
• Discarded from DSM-5
• ‘Substance’ dependence
• Maladaptive compulsive use of a substance (behavior)
• (Not a particularly helpful term)
• Diversion – medication obtained other than by prescriptionPerpetuation of Stigma
Power of language
• ‘Misuse’
• Any use of prescription drug varying fr accepted medical practice
• Route – IDU / smoked / intranasal
• Dose - ↑ amount / ↑ frequency
• Implied value judgment - accidental vs. intentional
• ‘Problem use’ - ill defined
• Pejorative – substance problem vs. problem pt
• ‘Harmful’ more descript and useful
• ‘Inappropriate use’- ill defined
• Also pejorative
• According to who?
• By what criteria? (ASAM)Perpetuation of Stigma
Power of language
• Physical / Physiologic dependence (ASAM)
• “a state of adaptation that is manifested by a drug class specific
withdrawal syndrome that can be produced by abrupt cessation,
rapid dose reduction, decreasing blood level of the drug, and/or
administration of an antagonist.”
• Tolerance (ASAM)
• “ a state of adaptation in which exposure to a drug induces
changes that result in a diminution of one or more of the drug's
effects over time.”
• Withdrawal (DSM-5)
• “the characteristic withdrawal syndrome for the substance” OR
• “the same (or a closely related) substance is taken to relieve or
avoid withdrawal symptoms”Discussion
• Substance Use Disorders as chronic disease
• “Threshold” for treatment
• Comparable demands for other chronic conditions?
• e.g. Diabetes / Asthma / COPD
• Tobacco / nicotine – ironic
• e.g. Surgery / organ transplant / Hep C treatment
• How available is heroin?Coming Soon to a Highway Near You
The Role of Pain • Body’s way of alerting us about a problem • Hand on a hot stove • Pain from sprained ankle limp • Without it more injury • No impetus to withdraw from more injury / harm
Pain • Acute Pain • Trauma / injury / dental procedures / labor & delivery • Chronic Malignant Pain • Cancer • •Chronic Nonmalignant Pain • Arthritis / Disc Disease • “Withdrawal” related Pain
Types of Pain • Nociceptive noxious peripheral stimulation • Sprains / Fractures / Post-op • Inflammatory • OA / RA / Tendinitis • Neuropathic multiple mechanisms • DM peripheral / Post-herpetic / HIV polyneuropathy • Non inflamm / Non neuropath • Abnormal central processing • No obvious tissue / nerve damage • Fibromyalgia / Irritable bowel syndrome
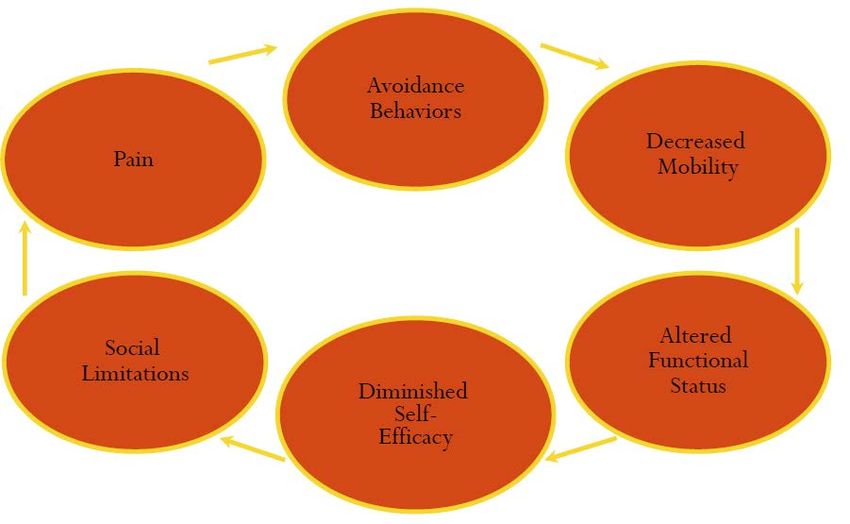
Uncontrolled Pain: A Vicious Cycle
Perception of Pain
• A 4-step model
• Transduction: Detection of acute noxious stimulation
– thermal / mechanical / chemical –
by nociceptive neurons
• Transmission: Nerve impulses via afferent neurons from
periphery to spinal cord - eventually to cerebral cortex
• Perception: Cortical and limbic structures involved in
awareness / interpretation of pain
• Modulation: Pain inhibited / facilitated by mechanisms
affecting ascending/descending pathwaysPain Pathway
Perception Modulation
Cerebral cortex Midbrain
Thalamus
Limbic systemModulation of Pain
Descending Pain Regulation:
• norepinephrine - alpha-2
stimulatory effects
• serotonin
• opiates relieve pain by
stimulating mu & delta receptors
at a host of sites.Adaptation to Pain
• Pain
• Identification of problem appropriate response
• Problem resolved
• Modulation of feedback
• Isolation / reduction
• Perception of pain
• Cognition / conditioningTreatment of Pain • Medications can augment or disrupt • Modulation / perception of pain • Problematic • Not an exact science • Not without risk
Multimodal Treatment
• Lifestyle modification – exercise / weight loss
• PM&R – assistive devices / electrotherapy
• CAM – acupuncture / message / supplements
• Psychological – psychotherapy / support groups
• Interventional – injections / neurostimulation
• Pharm – nonopioids/NSAIDS/adjuvant analgesia
Fine PG, et al. J Support Oncol. 2004;2(suppl 4):5-22
Portenoy RK, et al. In: Lowinson JH, et al, eds. Substance Abuse: A Comprehensive Textbook. 4th ed.
Philadelphia, PA: Lippincott, Williams & Wilkins; 2005:863-903.An Analogy • More to treating pain than Opioids • But opioids remain important • Opioids are like a spare tire • Used when other tire (modality) fails
An Analogy • More to treating pain than Opioids • But opioids remain important • Opioids are like a spare tire • Used when other tire (modality) fails • Opioid monotherapy is like going down the road – WITH ONLY A SPARE TIRE
Who is Misusing Opioids? Why? • Medical use • Pts in pain seeking more relief • Pts in pain escape from emotional pain • Non-medical use • ‘Recreational users’ • People with ‘addiction’ / substance use disorders
Considerations
• What is conventional practice for this type of pain or patient?
• Is there alternative therapy that likely to have an equivalent or better
therapeutic index for pain control, functional restoration, and
improvement in quality of life?
• Does the patient have medical problems or other risk factors that
may increase the risk of opioid-related adverse effects? (Genetics)
• Is the patient likely to manage the opioid therapy responsibly?
• Who can I treat independently?
• Who would I be able to treat with input from a specialist?
• Who should I refer rather than treat - if opioid therapy is a
consideration?
Fine PG, Portenoy RK. Clinical Guide to Opioid Analgesia. Vendome Group, New York, 2007.Other Considerations • Potential benefits • Analgesia • Increased function • Improved QOL • Potential risks • Toxicity • Decreased function / impairment • Addictive potential • Hyperalgesia
Pain and Mood Disorders
• Concurrent depression / anxiety common with persistent pain
• Dysphonia can decrease pain threshold / tolerance of pain
• Chronic pain often a factor in development of mood disorder
JAMA 1998; 280:147-151Risk Factors of Suffering • Past hx of SUD • Hx of emotional trauma • Dysfunctional family – a member has a SUD • Poor coping skills • Dependent traits • Deficit of stimulus augmenters – decreased hedonic tone
Flirting with Death
Treatment of Pain in Pt’s with SUD’s • Explicitly address addiction • Before considering opioid therapy - • Exhaust all available non-pharmacologic therapies • Exhaust all available non-opioid analgesics • If opioids indicated – provide adequate dose • Treat associated symptoms • Keep lines of communication open
Treatment of Pain in Pt’s with SUD’s • Avoid drug of choice • Consider longer acting opioids • Use medication with lower street value • If possible – avoid self administration • Case management
DDx of Aberrancy
• Addiction – i.e. out-of-control compulsive drug use
• Pseudoaddiction – disconcerting medication seeking behavior
• Due to inadequate analgesia
• Behavior normalizes with improved analgesia
• Other psychiatric diagnosis
• Organic mental syndrome – confused / stereotyped drug-taking
• Personality disorder – impulsive/ entitled/chemical-coping behavior
• Chemical coping - drug overly central to pt’s life
• Depression/anxiety/situational stressors
• Self-medication / mood regulation
• Criminal intent - diversion
Passik SD, Kirsh KL. Curr Pain Headache Rep. 2004;8:289-294.Identification and Management of Aberrancy • Assess risk of aberrant behavior • Obtain scheduled and random UDS’s • Intermittent call backs and pill counts • Utilizing state prescription monitoring • Develop good working relationship with PharmD’s / Pharmacies • Ongoing assessment • Adequacy of analgesia • Presence of other stressors • Acquiring collateral information • Family / friends / significant others / other pts
Aberrant Drug-related Behavior • Aggressive complaining of need for more drug • Hoarding medication during periods of decreased pain • Requesting specific drugs • Acquiring similar drugs from other medical sources when – • Original prescriber is unavailable • Pain undertreated • Unsanctioned dose escalations / other non-compliance x1-2 Are the above behaviors more or less predictive of SUD?
Aberrant Drug-related Behavior • Aggressive complaining of need for more drug • Hoarding medication during periods of decreased pain • Requesting specific drugs • Acquiring similar drugs from other medical sources when – • Original prescriber is unavailable • Pain undertreated • Unsanctioned dose escalations / other non-compliance x1-2 Are the above behaviors more or less predictive of SUD? LESS
Signs of Potential Misuse / Diversion
• Request appointments toward end-of-office hours
• Arrive without appointment
• Telephone/arrive after office hours (when staff are anxious to leave)
• Reluctance to have thorough PE / diagnostic tests / referrals
• Often fails to keep appointments
• Reluctance to identify previous providers
• Unwilling to release past medical records
• Unusual stories
• However emergencies happen
• Not every person in a hurry is misusing / diverting
Drug Enforcement Administration. Don't be Scammed by a Drug Abuser. 1999.
Cole BE. Fam Pract Manage. 2001;8:37-41.Aberrant Behavior More Indicative of SUD • Selling prescription drugs • Prescription forgery • Stealing or “borrowing” drugs • Obtaining prescription drugs form non-medical sources • Concurrent abuse of alcohol or illicit drugs • Multiple dose escalations / other non-compliance • Multiple episodes of prescription “loss” • Rx from other clinicians/EDs w/o seeking 1º prescriber • Decline in function that appears to be related to drug use • Resistance to change therapy despite significant SE’s
Edwin A. Salsitz, M.D., FASAM Beth Israel Medical Center, NYC Director Office-Based Opioid Therapy
Closing Thoughts
• Diversion & misuse indicate medication non-adherence
• Can decrease treatment effectiveness
• May harm patients or recipients of diverted medication
• IDU / clinical reputation
• We are not detectives
• We cannot control patient behavior
• We CAN influence and shape behavior
• Quality / Evidence-based practice / Compassion
• We CAN help patient’s re-focus behavior on their health
• Punishment is NOT effective
• Communicate to policy makers that cutting or decreasing treatment
access will NOT eliminate / guarantee less diversion / misuse
• May in fact adversely affect mortality rates
• Do our part to increase accessibility to treatment by using language that
decreases stigma of SUD’sOur Most Basic Role - To BELIEVE in our patients…..
on THEIR behalf!
René Magritte – La Clairvoyance (1936)References • PCSS-O Webinar Identifying and Intervening With Problematic Medication Use Behaviors, Stephen Wyatt, DO, Department of Psychiatry, Middlesex Hospital, Middletown CT, 6/1/2012 • PCSS-MAT Webinar Clinical Case Reviews: Managing Diversion and Misuse in Office-Based Treatment, Michelle Lofwal, MD, Associate Professor, Departments of Behavioral Science & Psychiatry, Center on Drug and Alcohol Research, University of Kentucky College of Medicine, 9/24/2014 • Contact info: clifford.cabansag@lindnercenter.org
You can also read