Aspirin and Tranexamic Acid for Coronary Artery Surgery (ATACAS) Trial: Rationale and design
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Aspirin and Tranexamic Acid for Coronary Artery
Surgery (ATACAS) Trial: Rationale and design
Paul S. Myles, MPH, MD, a,b,c,d Julian Smith, MS, e,f John Knight, MBBS,g D. James Cooper, MD,c,h
Brendan Silbert, MBBS,i,j John McNeil, PhD,c Donald S. Esmore, MBBS,f,l Brian Buxton, MD,k Henry Krum, PhD,c,d
Andrew Forbes, PhD, c,m Andrew Tonkin, PhD c,d and the ATACAS Trial Group Victoria, and Adelaide, Australia
Background Despite some concern that recent aspirin ingestion increases blood loss after coronary artery surgery,
there is some evidence that this may reduce thrombotic complications. In contrast, antifibrinolytic drugs can reduce blood loss
in this setting, but there is concern that they may increase thrombotic complications. Published guidelines are limited by a
lack of large randomized trials addressing the risks and benefits of each of these commonly used therapies in cardiac surgery.
The ATACAS Trial is a study comparing aspirin, tranexamic acid, or both, with placebo in patients undergoing on-pump or
off-pump coronary artery surgery.
Methods We discuss the rationale for conducting ATACAS, a 4600-patient, multicenter randomized trial in at-risk
coronary artery surgery, and the features of the ATACAS study design (objectives, end points, target population, allocation,
treatments, patient follow-up, and analysis).
Conclusions The ATACAS Trial will be the largest study yet conducted to ascertain the benefits and risks of aspirin and
antifibrinolytic therapy in coronary artery surgery. Results of the trial will guide the routine clinical care of patients in this setting.
(Am Heart J 2008;155:224-30.)
Coronary artery bypass graft (CABG) surgery is one of Coronary artery bypass graft surgery can be compli-
the primary treatment options for patients with coronary cated by excessive bleeding, a need for blood transfu-
artery disease, with N800 000 CABG operations done sion, and occasionally, surgical reexploration for
annually around the world.1 Although CABG surgery uncontrolled bleeding or cardiac tamponade.5-8 In
offers benefit to most patients, some die, and others contrast, there is a risk of thrombotic complications such
experience long-term disability.1-4 as myocardial infarction (MI) and stroke.1,3,5 Approxi-
mately 5% to 15% of cardiac surgical patients have ≥1
From the aDepartment of Anaesthesia and Perioperative Medicine, Alfred Hospital, major complication within 30 days of surgery, leading to
Melbourne, Victoria, Australia, bAcademic Board of Anaesthesia and Perioperative greatly increased health care costs.4 Antifibrinolytic
Medicine, Monash University, Melbourne, Victoria, Australia, cDepartment of Epidemiol-
ogy and Preventive Medicine, Monash University, Melbourne, Victoria, Australia,
drugs such as aprotinin and tranexamic acid (TxA)
d
Australian National Health and Medical Research Council Centre for Clinical Research reduce bleeding9-13 but could possibly increase throm-
Excellence in Therapeutics, Melbourne, Victoria, Australia, eCardiothoracic Surgery Unit, botic complications after cardiac surgery.14-19
Monash Medical Centre, Melbourne, Victoria, Australia, fDepartment of Surgery, Monash
Medical Centre, Monash University, Melbourne, Victoria, Australia, gDepartment of
Cardiac Services, Flinders Medical Centre, South Australia, Adelaide, Australia, hIntensive
Care Department, Alfred Hospital, Melbourne, Victoria, Australia, iDepartment of Antifibrinolytic therapy
Anaesthesia, St Vincent's Hospital, Melbourne, Victoria, Australia, jDepartment of Surgery, In a retrospective observational study on 4374 patients
University of Melbourne, Melbourne, Victoria, Australia, kDepartment of Cardiothoracic
undergoing CABG surgery, Mangano et al14 used pro-
Surgery, Austin Hospital, Heidelberg, Victoria, Australia, lDepartment of Cardiothoracic
Surgery, Alfred Hospital, Melbourne, Victoria, Australia, and mBiostatistics Unit,
pensity scores to investigate the potential adverse effects
Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, of aprotinin. They found that aprotinin was associated
Victoria, Australia. with an increased risk of renal impairment, MI or heart
Trial registration: www.actr.org.au: no. 12605000555651.
Conflict of interest statement: Bayer HealthCare (Leverkusen, Germany) has provided
failure, stroke, and encephalopathy. A follow-up study
aspirin and matched placebo tablets at no cost. Professor Julian Smith has received found an association between aprotinin and poor
honoraria as a clinical advisor to Bayer HealthCare, Pymble, New South Wales, Australia, survival.15 Another observational study published at
for advice on the use of aprotinin in cardiac surgery. None of the other authors has around the same time found no association between
declared any conflict of interest.
Submitted June 9, 2007; accepted October 1, 2007.
aprotinin and MI or stroke but did identify an association
Reprint requests: Paul S. Myles, Department of Anaesthesia and Perioperative Medicine, with renal dysfunction.16 These observational studies
Alfred Hospital, Commercial Road, Melbourne, Victoria 3004, Australia. have been criticized,20-22 largely because of their
E-mail: p.myles@alfred.org.au
susceptibility to bias and confounding.23-25
0002-8703/$ - see front matter
© 2008, Mosby, Inc. All rights reserved. Three meta-analyses of randomized trials have found
doi:10.1016/j.ahj.2007.10.003 that antifibrinolytic therapy reduces bleeding in cardiacAmerican Heart Journal
Volume 155, Number 2
Myles et al 225
surgery.9,10,13 These have had a major influence on highlight the lack of published data in the literature
consensus guidelines.12 Levi et al10 found that aprotinin (ie, no class I recommendations) and the need for a
decreased mortality almost 2-fold (odds ratio 0.55, 95% CI definitive large trial.37
0.34-0.90) compared with placebo. Treatment with
aprotinin and with lysine analogues decreased the
frequency of reoperation (0.37 [0.25-0.55] and 0.44 [0.22- Study objectives
0.90], respectively). Desmopressin, but not aprotinin and The overall study goal of ATACAS is to assess (i)
TxA, increased the risk of MI. whether aspirin should be continued up until the day of
Antifibrinolytic therapy may increase the risk of graft CABG surgery and (ii) whether should TxA be used
thrombosis.11 Although aprotinin is the antifibrinolytic routinely in CABG surgery. The study is funded by the
drug most frequently implicated, there is also some Australian National Health and Medical Research Council
concern with epsilon aminocaproic acid17,18 and des- (ID 334015).
mopressin.10 However, there is also evidence that
aprotinin inhibits various prothrombotic pathways, has Study design
antiplatelet activity,26 and may reduce stroke risk.27 In
The ATACAS Trial is a multicenter, randomized, blinded,
contrast, TxA increases thrombin generation.19
2 × 2 factorial trial testing whether aspirin, TxA, or both
Antifibrinolytics are recommended for reoperative and
can reduce mortality and/or major morbidity after
other complex cardiac surgery.12 However, it is not yet
elective CABG surgery. Eligible patients are randomly
clear whether these drugs provide any benefit beyond
allocated to 1 of the following 4 treatment groups:
limiting blood loss13 and (for aprotinin) reoperation for
aspirin, TxA, aspirin with TxA, or placebo.
bleeding.9,10 Both aprotinin and TxA have comparable
effects in reducing blood loss,9,12,13,28 and so, in view of
the marked cost advantages of TxA, it seems reasonable Primary end point
to evaluate its effectiveness in contemporary practice.13 It The primary end point is a composite including all-
remains unclear whether the reduced bleeding out- cause mortality or major ischemic morbidity (MI, stroke,
weighs an increased risk of thrombotic complications. pulmonary embolism, renal failure, bowel infarction) up
to 30 days after surgery.
Aspirin and cardiac surgery
Aspirin may 5,8 or may not 9,29-31 significantly increase Secondary end points
bleeding after cardiac surgery. Aspirin increases post- The secondary end points include the following: (i) all-
operative blood loss by b300 mL8; this should not cause mortality; (ii) ischemic complications (MI, stroke,
increase the need for blood transfusion.8,12 It is common renal failure, pulmonary embolism, bowel infarction);
practice to stop aspirin 5 to 7 days before elective cardiac and (iii) bleeding complications (major hemorrhage
surgery. Yet, aspirin-induced increased bleeding might be requiring reoperation for bleeding, cardiac tamponade)
outweighed by a beneficial effect on reduced graft and blood transfusion ≤30 days after surgery.
thrombosis, MI,32-35 and possibly stroke.30,35 Aspirin is
routinely recommenced 8 to 36 hours after surgery, but
the practice of stopping aspirin before surgery denies an Study methods
opportunity to avoid thrombosis in the days before and Patient population
during and crucial hours after surgery.36 Eligible patients consist of those undergoing elective
on-pump or off-pump coronary artery surgery identified
as being at an increased risk for major complications,2,3,5
Society of Thoracic Surgeons as detailed in Table I. We are enrolling 4600 patients in 15
practice guidelines to 20 participating sites in Australia, New Zealand, Asia,
The Society of Thoracic Surgeons has published and Europe. Institutional review board approval will be
guidelines on the use of aspirin and antifibrinolytic sought from each site, and all patients are asked to
therapy.37 They note that “there is only anecdotal provide informed consent.
information supporting the discontinuation of aspirin
before elective CABG surgery.” In brief, the recommen- Eligibility criteria
dations are to stop aspirin 3 to 5 days before elective After first obtaining agreement and support from
CABG surgery in low-risk patients but in high-risk CABG cardiac surgeons and anesthesiologists at each site, all
surgery, to continue or commence aspirin preopera- elective coronary artery surgical patients are screened for
tively (both class IIa recommendations). For aspirin- eligibility. The study allows individual surgeons to
treated high-risk CABG patients, they recommend exclude any of the patient or surgical risk factors if they
antifibrinolytics to limit bleeding. These guidelines have a strong preference to use or avoid aspirin orAmerican Heart Journal
226 Myles et al February 2008
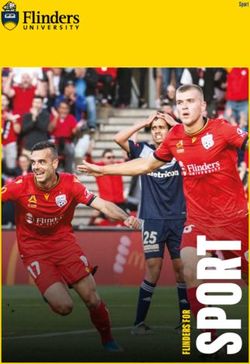
Table I. Specific inclusion and exclusion criteria
Death
This includes all deaths within 30 days of surgery from
Inclusion criteria any cause.
1. Men and women, aged ≥18 y, undergoing elective coronary
artery surgery (on-pump or off-pump)
2. Patient has any of the following risk factors: Myocardial infarction
• Age ≥70 y An MI is defined by the presence of either (i) a typical
• Left ventricular impairment (fractional area change b20%, rise and gradual fall (troponin) or more rapid rise and
ejection fraction b40%, or at least moderate impairment on
ventriculography)
fall (creatine kinase–MB [CKMB]) of biochemical markers
• Concomitant valvular or aortic surgery of myocardial necrosis after surgery with at least 1 of the
• Aneurysmectomy following: ischemic symptoms, development of
• Repeated cardiac surgery (“redo”) pathologic Q waves on 2 adjacent leads on the electro-
• Chronic obstructive pulmonary disease cardiogram (ECG), or ECG changes indicative of
• Renal impairment (serum creatinine N2.0 mg/dL or creatinine
clearance b45 mL/min)
ischemia (ST-segment elevation or depression); or (ii)
• Obesity (body mass index N25 kg/m2) pathologic findings of an acute MI. Also, in view of the
• Pulmonary hypertension (mean pulmonary artery pressure difficulty of detecting ischemic chest pain in the early
N25 mm Hg) postoperative period, in addition, a non–Q-wave MI is
• Peripheral vascular disease
defined by a cardiac enzyme elevation in isolated CABG
Exclusion criteria
1. Poor (English) language comprehension cases, using any of the following: troponin I N10 ng/mL
2. Clinician preference for antifibrinolytic therapy at any time N12 hours post-CABG,38-41 troponin T N4.0
3. Urgent surgery for unstable coronary syndromes at N12 hours post-CABG,38,41 or CKMB N3 times the
4. Active peptic ulceration upper limit of normal at N12 hours post-CABG surgery.41
5. Allergy or contraindication to aspirin or TxA
6. Aspirin therapy within 5 d of surgery
7. Warfarin or clopidogrel therapy within 7 d of surgery or glycoprotein Pulmonary embolism
IIb/IIIa antagonists within 24 h of surgery A pulmonary embolism will be diagnosed if confirmed
8. Thrombocytopenia or any other known history of bleeding disorder by high-probability VQ scan or documented on pulmon-
9. Severe renal impairment (serum creatinine N3.3 mg/dL or estimated
ary angiography.
creatinine clearance b25 mL/min)
10. Recent hematuria
11. Thromboembolic disease: history of postoperative or spontaneous Stroke
pulmonary embolism, spontaneous arterial thrombosis, or A stroke will be diagnosed if confirmed by
familial hypercoaguability (eg, lupus anticoagulant,
documented cerebral infarction or hemorrhage on
protein C deficiency)
12. Pregnancy computed tomographic or magnetic resonance imaging
scan or by new neurologic signs (paralysis, weakness,
or speech difficulties) lasting N24 hours or leading to
antifibrinolytic therapy in on-pump or off-pump cases. earlier death.
The number of patients eligible but not recruited into the
trial are detailed in a study log. This includes the reasons Acute renal failure
for the lack of participation. Acute renal failure will be diagnosed if confirmed by a
doubling of the serum creatinine in the postoperative
Allocation and randomization period when compared with the baseline (preoperative)
After patient consent has been obtained, a central value or by a rise N2.4 mg/dL from baseline.
24-hour interactive voice recognition system prompts
the researcher or study coordinator to identify their study Bowel infarction
site and whether the procedure is on-pump or off-pump, Bowel infarction will be diagnosed at laparotomy if
and then, patients are randomly allocated to treatment there is a need for bowel resection or if bowel infarction
group (1:1:1:1) from a computer-generated list. Rando- is diagnosed at autopsy.
mization is stratified by site and by on-pump/off-pump
surgery. This will equalize site-specific intergroup differ- Cardiac tamponade
ences in surgical and other perioperative care. In addition, Tamponade will be diagnosed by typical
the sample size is sufficiently large to ensure comparable hemodynamic and/or echocardiographic features
baseline and other perioperative characteristics. leading to and confirmed by surgical reexploration
or pericardiocentesis.
Study end point definitions
Data pertaining to study end points occurring up to 30 Major hemorrhage
days after surgery are sent to an adjudication committee Major hemorrhage is defined by any excessive bleeding
blinded to group identity. requiring reoperation. In addition, we will record theAmerican Heart Journal
Volume 155, Number 2
Myles et al 227
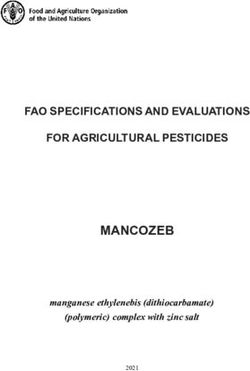
Table II. Steps to be taken if there is clinical evidence of excessive Table III. Red cell transfusion protocol
bleeding, as defined by bleeding N200 mL/h for N2 h or N400 mL
in any 1 h, after bypass or off-pump surgery 1. Before cardiopulmonary bypass, transfuse packed red cells if
hematocrit b28% or hemoglobin b90 g/L
1. Administer further protamine, 50-100 mg, whether ACT is elevated 2. During cardiopulmonary bypass, transfuse packed red cells if
or not hematocrit b20% or hemoglobin b70 g/L
2. Consider aprotinin therapy (bolus + infusion); use the Hammersmith 3. After cardiopulmonary bypass or at any time with off-pump surgery,
regimen: loading dose, 2 million U, followed by 500 000 U/h* transfuse packed red cells if hematocrit b25% or hemoglobin b80 g/L
3. Administer platelet transfusion, 5 U, if platelet count b100 000/L
4. Administer fresh frozen plasma, 5 U, if INR N1.4 or fibrinogen b150 g/L
5. Administer cryoprecipitate if fibrinogen b100 g/L unacceptable bleeding.34 The aspirin placebo group will
6. If bleeding remains problematic, N100 mL/h after protocol-directed receive inactive placebo tablets identical in appearance
therapies, consider recombinant VIIa (NovoSeven), 90 μg/kg* to active aspirin.
*In some countries, this constitutes off-label use, and so, local regulations should
Tranexamic acid will be prepared and administered by
apply. an anesthesiologist not responsible for the procedure—on
some occasions this may not be possible; this
number of units of blood products transfused within information is being recorded. Tranexamic acid is to be
30 days of surgery. administered within 20 minutes after induction of
anesthesia as an IV bolus, over 10 to 30 minutes. This
Surgical and anesthetic techniques regimen has been shown to provide and maintain
Preoperative demographic characteristics and details of effective TxA concentrations throughout and after sur-
patients' medical and surgical history are recorded. They gery.44 Placebo TxA solution will consist of normal saline.
will also undergo a 12-lead ECG, chest x-ray, pathology
testing, and other routine investigations. Clinical and Study procedures, blinding,
laboratory data will be used to generate ≥1 risk scores.2,42 and follow-up
On the day of surgery, patients are allocated to 1 of the The surgical team, including anesthesiologist and all
4 treatment groups. All other perioperative clinical care is other clinical staff, are blinded to aspirin allocation, with
according to standard practice at each site because this is study drug coding and delivery being managed by
an effectiveness trial designed to represent real-world research staff at the study coordinating center. However,
practice.43 All such relevant perioperative data are for TxA, an anesthesiologist is being asked to prepare the
recorded on the study case report form. IV study drug (TxA or placebo saline) at each site at the
Heparinization for bypass is based on a bolus dose of time of surgery. Ideally, this should not be the attending
300 U/kg and maintenance of an activated clotting time anesthesiologist responsible for the care of the patient
(ACT) N450 seconds during bypass, with additional during and after surgery. However, it is recognized that for
heparin as required. Heparin reversal at the completion of some sites, limited staffing may make this very difficult,
cardiopulmonary bypass (CPB) is achieved with prota- and so, the responsible anesthesiologist can prepare the
mine 4 mg/kg, monitored with ACT (b140 seconds). IV study drug provided that all other staff are kept blinded
Other antifibrinolytic therapy cannot be used before or to TxA/placebo group allocation. Patients, surgeons, and
during CPB but can be used if there is clinically significant research staff must be blinded to treatment allocation.
bleeding after protamine administration (Table II). The
study is guided by a transfusion protocol (Table III). Data collection
Blood is collected postoperatively at 12 to 24 hours for Data collection is done by local research staff and
cardiac enzyme (troponin and/or CKMB) levels, and a entered onto a paper case report form. All data are
12-lead ECG is performed on each of the 3 days after subsequently entered onto a database accessed via the
surgery to detect MI. Additional tests are ordered if study web site (www.atacas.org.au). This is managed by
clinically indicated (eg, chest pain, dyspnea, circulatory Monash University's Center for Clinical Research Excel-
instability). In addition, patients are contacted by phone lence in Therapeutics (Melbourne, Australia), and all data
at 30 days and their medical records reviewed to ascertain and processes are reviewed each day at the data
if they have experienced any adverse outcomes. management center: data fields are checked, and in
conjunction with the local site research staff, missing data
Study medications and duration or inconsistencies are corrected before being automati-
Two active study medications will be used: (i) oral cally downloaded onto the confirmed database.
enteric-coated aspirin, single dose of 100 mg given 1 to
2 hours preoperatively, and (ii) intravenous (IV) TxA
100 mg/kg administered postinduction but before CPB. Statistical considerations
The aspirin dose has been shown to be effective, with an Sample size and power
onset time of b1 hour and with a suitable side effect Our estimate of sample size is based on a ≥30%
profile 34; higher doses are more likely to cause reduction in the incidence of the primary end point, fromAmerican Heart Journal
228 Myles et al February 2008
Beneficial or harmful effects of aspirin and/or TxA may
Table IV. Planned subgroups of patients for secondary analysis of
the effects of aspirin and TxA exist in specific subsets of CABG surgery patients, and
so, we have identified subgroups for secondary analysis
1. Sex
(Table IV).
2. Patient age N65 y
3. Left ventricular function (grades 1-4)
Interim analysis will be performed after enrolment of
4. High bleeding risk, defined by any of the following: patient age 2300 and 3450 patients, that is, at 50% and 75% of the
N70 y, weight b55 kg, poor left ventricular function (grade 4), renal target recruitment number of 4600. Results will be made
impairment, emergency surgery, coagulopathy, or reoperation available to a data and safety monitoring committee
5. Surgical subtypes: isolated coronary artery surgery, combined
(DSMC). The interim analyses will be adjusted according
(coronary artery + other), or off-pump surgery
to an O'Brien and Fleming type I error spending function,
separately for the aspirin and TxA main effects, using an
10% to 7%. The baseline incidence is a conservative overall 5% significance level for each main effect. Should
estimate based on contemporary Australian data (ASCTS the result for a particular main effect (eg, aspirin vs no
Victorian Cardiac Surgery Database). The effect size is less aspirin) cross the designated boundary at an interim
than that of the best evidence from a systematic review of analysis, consideration will be given by the DSMC to
randomized trials of antifibrinolytics10 and a randomized termination of study of that intervention (eg, cease
trial45 and large observational study 30 of aspirin. The recruitment to the aspirin arms and randomize new
group distributions can be estimated, using the aspirin patients to TxA or placebo only).
comparison as an example, as aspirin alone + aspirin/TxA
versus TxA alone + neither: a difference of 5.95%
[0.5(7% + 4.9%)] versus 8.5% [0.5(7% + 10%)]. With a type Data safety and monitoring committee
I error of 0.05 and a type II error of 0.1 (power 90%), the The DSMC consists of a cardiologist (chair), cardiac
required number was calculated at 2242 patients per surgeon, independent statistician, cardiac anesthesiolo-
group. We will recruit 4600 patients in this study (ie, 1150 gist with an interest in medical ethics and law, and clinical
patients in each subgroup, with combinations of 2300 per pharmacologist. The DSMC will discuss the interim
group for the main comparisons), which accommodates results and vote for continuation or stopping the trial.
for the interim analyses. Most secondary end points have This will be communicated to the steering committee
a baseline incidence of about 3% to 6% in such a study according to the prespecified stopping rules and con-
cohort; our study will have 60% to 85% power for each of sideration of other evidence relevant to the DSMC.
these. The detectable risk ratios with 80% power are 0.67
for incidence of 6% and 0.57 for incidence of 3%. Conclusions
Debate on the likely benefits and risks of aspirin and
Statistical methods
antifibrinolytics in CABG surgery will continue until we
All patients who are randomly allocated to study drug
have the results from large randomized trials. The ATACAS
administration will be considered as comprising the
Trial will guide clinical decision making as to whether
intention-to-treat population for all primary, secondary,
patients should stop aspirin before elective CABG surgery
and safety analyses. Baseline characteristics of the
and whether TxA antifibrinolytic therapy should be used
4 treatment groups will be tabulated using appropriate
more widely or far more selectively. When considering
summary statistics.
the cost and extent of CABG surgery around the world,
Because no interaction between aspirin and TxA is
small improvements in outcome would have major
expected a priori, analysis of the principal outcome of
implications for health care delivery.
mortality/morbidity will be performed using χ2 tests for
the main effects of aspirin and TxA. The groups being
compared will be aspirin (n = 2300) versus no aspirin References
(n = 2300) and TxA (n = 2300) versus no TxA (n = 2300). 1. Nalysnyk L, Fahrbach K, Reynolds MW, et al. Adverse events in
Results will be expressed as risk ratios with 95% CIs. coronary artery bypass graft (CABG) trials: a systematic review and
Assessment of the assumption of no interaction between analysis. Heart 2003;89:767-72.
aspirin and TxA will be performed using log-binomial 2. Tu JV, Jaglal SB, Naylor CD. Multicenter validation of a risk index for
regression. This uses a generalized linear model with mortality, intensive care stay, and overall hospital length of stay after
binary outcome and logarithmic link function and cardiac surgery. Circulation 1995;91:677-84.
3. Shroyer AL, Coombs LP, Peterson ED, et al. The Society of Thoracic
preserves the natural association metric as the relative
Surgeons: 30-day operative mortality and morbidity risk models. Ann
risk rather than as the odds ratio as would be yielded Thorac Surg 2003;75:1856-64.
with logistic regression. Should baseline imbalances 4. Taylor GJ, Mikell FL, Moses HW, et al. Determinants of hospital
between arms in important prognostic factors occur, charges for coronary artery bypass surgery. The economic con-
sensitivity analyses will adjust the main effects of aspirin sequences of postoperative complications. Am J Cardiol 1990;65:
and TxA for these factors using log-binomial regression. 309-13.American Heart Journal
Volume 155, Number 2
Myles et al 229
5. Despotis GJ, Levine V, Filos KS, et al. Factors associated with 26. Day JR, Landis RC, Taylor KM. Aprotinin and the protease-activated
postoperative blood loss and hemostatic transfusion requirements: a receptor 1 thrombin receptor: antithrombosis, inflammation, and
multivariate analysis in cardiac surgical patients. Anesth Analg stroke reduction. Semin Cardiothorac Vasc Anesth
1996;82:13-23. 2006;10:132-42.
6. Grayson AD, Jackson M, Desmond MJ. Monitoring blood transfusion 27. Frumento RJ, O'Malley CM, Bennett-Guerrero E. Stroke after cardiac
in patients undergoing coronary artery bypass grafting: an audit surgery: a retrospective analysis of the effect of aprotinin dosing
methodology. Vox Sang 2003;85:96-101. regimens. Ann Thorac Surg 2003;75:479-83.
7. Chelemer S, Prato BS, Cox Jr PM, et al. Association of bacterial 28. Ferraris VA, Ferraris SP, Joseph O, et al. Aspirin and postoperative
infection and red blood cell transfusion after coronary artery bypass bleeding after coronary artery bypass grafting. Ann Surg
surgery. Ann Thorac Surg 2002;73:138-42. 2002;235:820-7.
8. Bélisle S, Hardy JF. Hemorrhage and the use of blood products after 29. Tuman KJ, McCarthy RJ, O'Connor CJ, et al. Aspirin does not
adult cardiac operations: myths and realities. Ann Thorac Surg increase allogeneic blood transfusion in reoperative coronary artery
1996;62:1908-17. surgery. Anesth Analg 1996;83:1178-84.
9. Brown JR, Birkmeyer NJ, O'Connor GT. Meta-analysis comparing the 30. Mangano DT, Multicenter Study of Perioperative Ischemia Research
effectiveness and adverse outcomes of antifibrinolytic agents in Group. Aspirin and mortality from coronary bypass surgery. N Engl J
cardiac surgery. Circulation 2007;115:2801-13. Med 2002;347:1309-17.
10. Levi M, Cromheecke ME, de Jonge E, et al. Pharmacological 31. Srinivasan AK, Grayson AD, Pullan DM, et al. Effect of preoperative
strategies to decrease excessive blood loss in cardiac surgery: a aspirin use in off-pump coronary artery bypass operations. Ann
meta-analysis of clinically relevant endpoints. Lancet Thorac Surg 2003;76:41-5.
1999;354:1940-7. 32. Goldman S, Copeland J, Moritz T, et al. Improvement in early
11. Alderman EL, Levy JH, Rich JB, et al. Analyses of coronary graft saphenous vein graft patency after coronary artery bypass surgery
patency after aprotinin use: results from the International Multicenter with antiplatelet therapy: results of a Veterans Administration
Aprotinin Graft Patency Experience (IMAGE) trial. J Thorac Cooperative Study. Circulation 1988;77:1324-32.
Cardiovasc Surg 1998;116:716-30. 33. Goldman S, Copeland J, Moritz T, et al. Starting aspirin therapy
12. Ferraris VA, Ferraris SP, Saha SP, et al. Peri-operative blood after operation: effects on early graft patency. Circulation
transfusion & blood conservation in cardiac surgery. www.sts.org/ 1991;84:520-6.
documents/pdf/BloodConservationGuidelines02.08.2007.pdf 34. Gavaghan T, Gebski V, Baron DW. Immediate postoperative aspirin
[accessed April 20, 2007]. improves vein graft patency early and late after coronary artery
13. Henry DA, Moxey AJ, Carless PA, et al. Anti-fibrinolytic use for bypass graft surgery. Circulation 1991;83:1526-33.
minimising perioperative allogeneic blood transfusion. Cochrane 35. Antiplatelet Trialists' Collaboration. Collaborative overview of
Database Syst Rev 2001;1:CD001886. randomised trials of antiplatelet therapy—II: maintenance of vascular
14. Mangano DT, Tudor IC, Dietzel C. The risk associated with aprotinin graft or arterial patency by antiplatelet therapy. BMJ
in cardiac surgery. N Engl J Med 2006;354:353-65. 1994;308:159-68.
15. Mangano DT, Miao Y, Vuylsteke A, et al. Mortality associated with 36. Burger W, Chemnitius JM, Kneissl GD, et al. Low-dose aspirin for
aprotinin during 5 years following coronary artery bypass graft secondary prevention—cardiovascular risks after its perioperative
surgery. JAMA 2007;297:471-9. withdrawal versus bleeding risks with its continuation—review and
16. Karkouti K, Beattie WS, Dattilo KM, et al. A propensity score case- meta-analysis. J Intern Med 2005;257:399-414.
control comparison of aprotinin and tranexamic acid in high- 37. Ferraris VA, Ferraris SP, Moliterno DJ, et al. The Society of Thoracic
transfusion-risk cardiac surgery. Transfusion 2006;46:327-38. Surgeons practice guideline series: aspirin and other antiplatelet
17. Dentz ME, Slaughter TF, Mark JB. Early thrombus formation on agents during operative coronary revascularization (executive
heparin-bonded pulmonary artery catheters in patients receiving summary). Ann Thorac Surg 2005;79:1454-61.
epsilon aminocaproic acid. Anesthesiology 1995;82:583-6. 38. Sadony V, Korber M, Albes G, et al. Cardiac troponin I plasma levels
18. Kluger R, Olive DJ, Stewart AB. Epsilon-aminocaproic acid in for diagnosis and quantitation of perioperative myocardial damage
coronary artery bypass graft surgery: preincision or postheparin? in patients undergoing coronary artery bypass surgery. Eur J
Anesthesiology 2003;99:1263-9. Cardiothorac Surg 1998;13:57-65.
19. Risch A, Dorscheid E, Stein G, et al. The effect of aprotinin and 39. Thielmann M, Massoudy P, Schmermund A, et al. Diagnostic
tranexamic acid on fibrinolysis and thrombin generation during discrimination between graft-related and non–graft-related perio-
cardiopulmonary bypass. Anaesthesist 2000;49:279-85. perative myocardial infarction with cardiac troponin I after coronary
20. Sedrakyan A, Atkins D, Treasure T. The risk of aprotinin: a conflict of artery bypass surgery. Eur Heart J 2005;26:2440-7.
evidence. Lancet 2006;367:1376-7. 40. Carrier M, Pellerin M, Perrault LP, et al. Troponin levels in patients
21. Body S, Mazer CD. Pro: aprotinin has a good efficacy and safety with myocardial infarction after coronary artery bypass grafting. Ann
profile relative to other alternatives for prevention of bleeding in Thorac Surg 2000;69:435-40.
cardiac surgery. Anesth Analg 2006;103:1354-9. 41. Nussmeier NA, Whelton AA, Brown MT, et al. Complications of the
22. Royston D, van Haaften N, De Vooght P. Aprotinin; friend or foe? COX-2 inhibitors parecoxib and valdecoxib after cardiac surgery.
A review of recent medical literature. Eur J Anaesthesiol N Engl J Med 2005;352:1081-91.
2007;24:6-14. 42. Roques F, Nashef SA, Michel P, et al. Risk factors and outcome in
23. Sackett DL. Bias in analytic research. J Chronic Dis 1979;32:51-63. European cardiac surgery: analysis of the EuroSCORE multinational
24. MacMahon S, Collins R. Reliable assessment of the effects of treatment database of 19030 patients. Eur J Cardiothorac Surg
on mortality and major morbidity. II: observational studies. Lancet 1999;15:816-22.
2001;357:455-62. 43. Tunis S, Stryer DB, Clancy CM. Practical clinical trials: increasing the
25. Datta M. You cannot exclude the explanation you have not value of clinical research for decision making in clinical and health
considered. Lancet 1993;342:345-7. policy. JAMA 2003;290:1624-32.American Heart Journal
230 Myles et al February 2008
44. Dowd NP, Karski JM, Cheng DC, et al. Pharmacokinetics of Steering committee: Paul Myles (chair and principal
tranexamic acid during cardiopulmonary bypass. Anesthesiology investigator), Julian Smith, D. James Cooper, John
2002;97:390-9. McNeil, Henry Krum, Stephanie Poustie (project man-
45. Klein M, Keith PR, Dauben HP, et al. Aprotinin counterbalances an
ager), and Sophia Wallace (research manager)
increased risk of perioperative hemorrhage in CABG patients pre-
End point adjudication committee: James W. Tomlin-
treated with aspirin. Eur J Cardiothorac Surg 1998;14:360-6.
son, David R. McIlroy, and D. James Cooper
Clinical pharmacologist: Henry Krum
Appendix A. Study organization Statistician: Andrew Forbes
and committees Data and safety monitoring committee: Andrew Tonkin
Sponsor: Alfred Hospital, Melbourne, Australia (chair), Brian Buxton, Alan Merry, Danny Liew, and
Funding sources: Australian National Health and Stephane Heretier (independent statistician)
Medical Research Council project grant ID 334015 and Data management and quality control: Stephanie
the Australian and New Zealand College of Anaesthetists, Poustie, John McNeil, and Adam Meehan
Melbourne, Victoria, Australia project grant ID 07/035 Web site design and maintenance: Adam Meehan
Receive tables of contents by e-mail
To receive the tables of contents by e-mail, sign up through our Web site at
http://www.ahjonline.com
Choose E-mail Notification
Simply type your e-mail address in the box and click on the Subscribe button
Alternatively, you may send on e-mail message to
majordomo@mosby.com
Leave the subject line blank, and type the following as the body of your message:
subscribe ahj_toc
You will receive an e-mail to confirm that you have been added to the mailing list.
Note that TOC e-mails will be sent when a new issue is posted to the Web site.You can also read