BASE HOSPITAL PHYSICIAN ORIENTATION HANDBOOK - www.hsnsudbury.caportalen/basehospital
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
`
BASE HOSPITAL PHYSICIAN
ORIENTATION HANDBOOK
www.hsnsudbury.ca/portalen/basehospital
BHP ORIENTATION HANDBOOK BASE HOSPITAL PHYSICIAN’S ROLES AND RESPONSIBILITIES BASE HOSPITAL PHYSICIAN (BHP) DEFINITION A physician that works in the Emergency Department of the Base Hospital who has been trained by the Medical Director of the Base Hospital Program or delegate to provide advice and orders to Paramedics within the Base Hospital catchment area BASE HOSPITAL PROGRAM REQUIREMENTS FOR BHPS The Base Hospital Program is responsible for ensuring that: Emergency physicians engaged as a base hospital physician shall hold the appropriate emergency medicine qualifications prescribed by the Royal College of Physicians and Surgeons, The College of Family Physicians or the American College of Emergency Physicians unless otherwise specified by the Director. The Base Hospital Program is responsible for ensuring that emergency physicians providing Base Hospital Physician responsibilities: a) abide by the provisions of the Ambulance Act and its associated Regulations, other relevant legislation, the MoHLTC Emergency Health Services Branch Patient Care Standards, the Provincial Base Hospital Medical Directives and the Base Hospital Performance Agreement, and b) has the judgement and skills to be capable of providing service in accordance with the Ambulance Act and its associated Regulations, other relevant legislation, the Provincial Base Hospital Medical Directives and this Agreement, and in accordance with the Patient Care Standards issued by the Director of the MoHLTC Emergency Health Services Branch. ROLE The role of the Base Hospital Physician is supportive to the Base Hospital Program and its Medical Director(s). The Base Hospital Physician acts within the parameters provided in their orientation to assist Paramedics with telephone patient care related advice and orders. Their role may also include assisting with clinical training, certifications, field assessments and other educational activities as may be mutually agreed to. RESPONSIBILITIES Base Hospital Physicians shall: a) be familiar with the most recent Medical Directives, standing orders, and policies and procedures of the Base Hospital as supplied; b) be familiar with the procedure for answering the telephone in the ED for Paramedics patching for advice or orders; c) answer the telephone for a Paramedic patch promptly, when required; d) give advice or orders to a Paramedic when requested. This would include land based paramedics, either Primary Care Paramedics from anywhere in Northeastern Ontario or Advanced Care Paramedics located in the Sudbury and North Bay areas; Revised – August 2015 2|Page
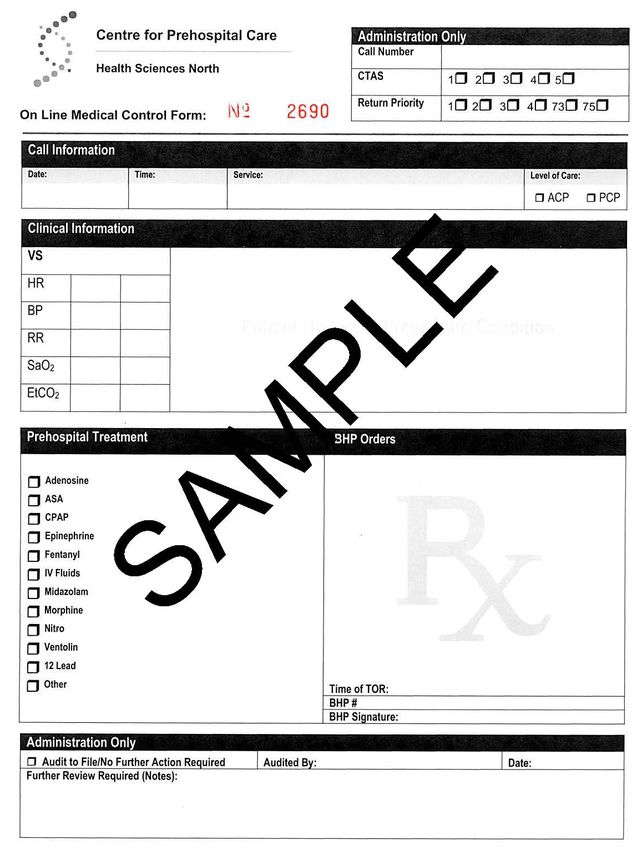
BHP ORIENTATION HANDBOOK e) complete a Base Hospital Physician Patch Form located in the binder next to the patch phone for every patch taken; f) provide feedback to the Base Hospital Program on individual paramedics when appropriate; g) provide feedback to the Base Hospital Program on its policies, procedures and protocols as appropriate; BASE HOSPITAL PHYSICIAN PATCH FORM Revised – August 2015 3|Page
BHP ORIENTATION HANDBOOK
BASE HOSPITAL PHYSICIAN PATCH FORM COMPLETION
1. When on any shift in the Emergency Department and the Base Hospital Communications
Phone line rings, the Base Hospital Physician on duty is responsible for responding to
Paramedic patches.
2. For each patient, one Base Hospital Physician Patch Form must be completed.
3. Complete the Patch form as thoroughly as possible. Each Patch form is pre-numbered. Ask
the Paramedic for their name and the call number. Provide the paramedic with the Patch
number on your BHP Patch Form. This allows the Base Hospital Program to match your
orders with the Paramedic’s treatment for quality assurance measures.
4. The Patch Form must clearly specify any physician orders provided to the paramedic. If
medications are ordered the physician must document the medication, dosage and route of
administration and any other information that they believe is vital to the proper care of the
patient.
5. If an order for Termination of Resuscitation is provided, please document the time of the order
and provide that time to the Paramedic.
6. If orders are provided by a BHP and no Patch Form is completed you will be sent a reminder
letter and a Patch Form to complete via the Base Hospital Medical Director.
7. If a Paramedic patches to a BHP and only advice but no orders are provided we ask that a
Patch Form still be completed.
BASE HOSPITAL PHYSICIAN RADIO COMMUNICATION ORIENTATION
Radio Phone Communication:
When the BHP (Base Hospital Physician) telephone rings, it is CACC (Central Ambulance
Communication Centre) that is linking a phone call from a Paramedic to your phone. The link up
could be from a cellular phone, regular phone or a radio. All forms of communication link-up are
tape recorded at CACC. The tapes are kept by CACC for a 3-month period unless a call is under
review. If you are linked up to a cell phone or regular phone line, you can talk normally in regular
phone communication.
In radio communication, it is different, as only ONE-WAY communication is possible. If you are
talking, the Paramedic will be cut-off and vice-versa. The other important item is that your voice
has to initialize for the “voice recognition” pickup system. It only takes about 2 seconds for your
voice to be recognized electronically and transmission to begin. Therefore, do not just give short
one or two word voice bursts or much of what you say will be cut-off when the paramedic is
listening to you.
A typical radio communication conversation might go something like this:
DOCTOR: 5243, this is Dr. Prpic, how do you read?
PARAMEDIC: Dr. Prpic, this is Paul Myre, Advanced Care Paramedic, I read you loud and
clear. I have a 55-year-old male in CHF. Medical history: Diabetes, CHF and MI 2 years
ago. MEDS: Nitro, Lasix, ASA, Monopril. Allergies: NIL – how do you read?
DOCTOR: You are coming through loud and clear, go ahead with vitals.
Revised – August 2015 4|PageBHP ORIENTATION HANDBOOK
PARAMEDIC: HR 59, BP 210/120, RR 32 full and regular, GCS 10, SpO2 77%, cyanotic,
clammy and cool. I started an IV, and am looking for a nitro order.
DOCTOR: Administer Nitro as per protocol and proceed to ED.
PARAMEDIC: 10-4 Dr. Prpic, Nitro prn. I am 15 minutes from ER over
DOCTOR: 10-4 over and out
Note that the Paramedic and Doctor always stated over when they have completed conversation.
They do not go on for long before they stop to confirm that the other party is hearing them
satisfactorily. You are talking on the ambulance provincial common line, but you still have to
assume citizens may be listening to your conversation. Therefore, no patient names can be
communicated over the radio. Also, note that no specific patient address was communicated
over the radio. It is better to talk in terms of ETA (Estimated Time of Arrival) at your ED. This way,
the Paramedic takes into account extrication time plus travel time to the ED. Although these
conversations do become intense at times, remain calm, and do not use profanity during
conversation. (Radio Communication’s Act forbids use of profanity.)
Finally, ensure you complete the Base Hospital Physician Patch Form each time you complete a
patch with a paramedic. Each patch form is matched up with the Paramedic’s ACR (Ambulance
Call Report). The BHP Patch Form protects you legally as does the taped conversations you have
with Paramedics. BHP Patch forms are audited and your orders given are matched up to
Paramedic controlled acts completed. Occasionally, radio conversations are audited for accuracy
if handwriting is questionable. All taped conversations can be transcribed and may become part of
legal proceedings in a court of law. This legal protection is for all concerned, but is very rarely
utilized in court. It is more frequently used for day to day clarification of conversation and orders
relayed. We cannot stress enough the importance of completing your BHP Patch Form.
SKILLS AND DRUG LIST
PARAMEDIC LEVEL DESIGNATION
The two levels of paramedics within the HSN Centre for Prehospital Care Ontario Land EMS
system are as follows: Primary Care Paramedic and Advanced Care Paramedic. Each is defined
by a scope of practice, which can be implemented based on medical directives or direct order from
a Base Hospital Physician.
STANDARD FOR BASE HOSPITAL PHYSICIAN CONTACT
Physician contact may be required when:
• A patient does not stabilize after protocol treatment and further advanced intervention is
indicated
• Drugs and skills are required which are not covered by Medical Directives
• The Paramedic wishes Base Hospital Physician advice
• A Base Hospital Medical Directive indicates a Paramedic must contact Base Hospital Physician
Revised – August 2015 5|PageBHP ORIENTATION HANDBOOK
SCOPE OF PRACTICE FOR PARAMEDICS (Y=YES * = SELECT AREAS OF THE REGION)
Primary Advanced
Airway/Ventilatory Compromise Skills
Care Care
CPAP Y Y
Endotracheal Intubation (oral/nasal) Y
Endotracheal Suctioning Y
King LT Insertion Y Y
Magill Forceps Utilization Y
Needle Thoracostomy Y
Oral/Nasal Airway Y Y
Oximetry Y Y
Positive Pressure Ventilation with BVM Y Y
Suctioning Mouth and Nose Y Y
Primary Advanced
Cardiovascular Compromise
Care Care
12 Lead Acquisition Y
12 Lead Interpretation Y
ECG Interpretation (PCP-five basic rhythms only) * Y
Pacing Y
Fluid Bolus Initiation Y
Intravenous Cannulation
* Y
Intraosseous Access
* Y
Manual Defibrillation Y Y
Synchronized Cardioversion Y
Primary Advanced
Obstetrical/Neonatal Transfer
Care Care
Assess and Recognize Obstetrical Emergencies Y Y
Delivery of the Neonate Y Y
Primary Advanced
Drug Administration
Care Care
Administer Drugs via SL; SC; PO; IM, MDI and Nebulized Routes Y Y
Administer Drugs via ETT; IO Y
Administer Drugs via IV * Y
PICC Line Access Y
Revised – August 2015 6|PageBHP ORIENTATION HANDBOOK
SCOPE OF PRACTICE FOR PARAMEDICS (Y= YES * = SELECT AREAS OF THE REGION)
Primary Advanced
MEDICATIONS CARRIED
Care Care
Adenosine Y
Amiodorone (North Bay ACP) Y
Atropine Y
ASA Y Y
50% Dextrose in water * Y
Calcium Gluconate Y
Dimenhydrinate Y Y
Diphenhydramine Y Y
Dopamine Y
Epinephrine 1:1,000 Y Y
Epinephrine 1:10,000 Y
Glucagon Y Y
Lidocaine (Sudbury ACP) Y
Midazolam Y
Morphine Y
Naloxone Y Y
Nitroglycerin Y Y
Oxygen Y Y
Salbutamol (MDI and Nebulization) Y Y
Sodium Bicarbonate Y
Xylometaxoline HCI (Otrivin®) Y
CONTACT INFORMATION
Any questions or concerns can be addressed to:
Dr. Jason Prpic, Regional Medical Director
Health Sciences North Centre for Prehospital Care / Trauma Services
705 675 4783 x 6
jprpic@hsnsudbury.ca
ALS Patient Care Standards
http://www.hsnsudbury.ca/portalen/basehospital/Documents/MedicalDirectives/tabid/1206/Default.aspx
Ontario Base Hospital Group (OBHG) link: http://www.ontariobasehospitalgroup.ca/
Revised – August 2015 7|PageYou can also read