Beat AML -sponsored by Leukemia & Lymphoma Society A new clinical trial for older patients ( 60) with previously untreated AML - prIME Oncology
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Beat AML
--sponsored by Leukemia & Lymphoma Society
A new clinical trial for older patients (>60) with
previously untreated AML
William Blum, MD
1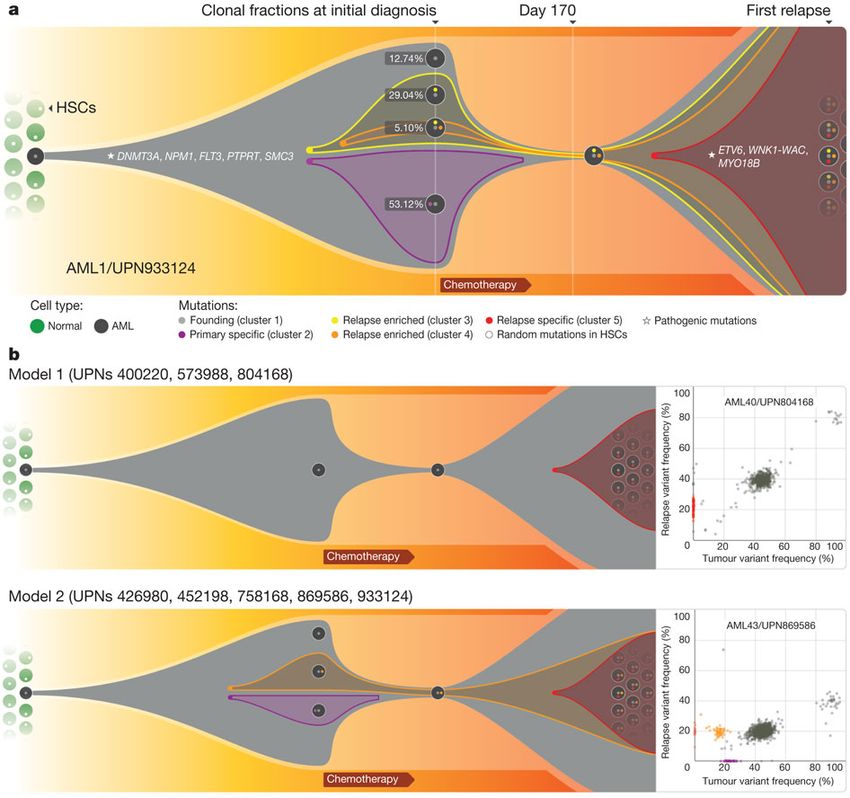
Case discussion
• 64 yo female with thrombocytopenia, circulating
blasts, obesity, diabetes, and longstanding
dysfunctional (mild) uterine bleeding (fibroids)
• WBC 10K, 12% blasts in blood
• Hgb 3.8g/dL, PLT 35K
• ECOG PS 2, morbid obesity
• DM II, remote history of “CHF” believed due to HTN
• BMBx, 30% blasts
Winship Cancer Institute | Emory University 2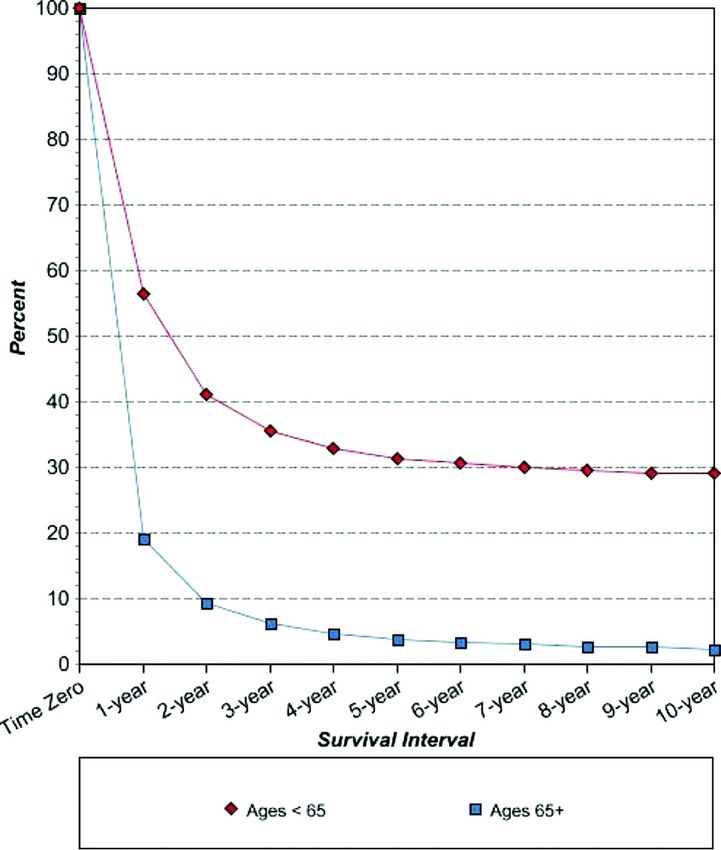
?
“This patient needs standard induction chemotherapy, to achieve CR
quickly and receive curative alloHCT as soon as possible.”
1. Why do we need a novel approach to AML for older patients?
2. What is Beat AML? Master trial: structure and logistics
3. Introduction to a couple of the ongoing Beat AML therapeutic trials
and brief trial updates (wait til ASH 2018)
Winship Cancer Institute | Emory University 3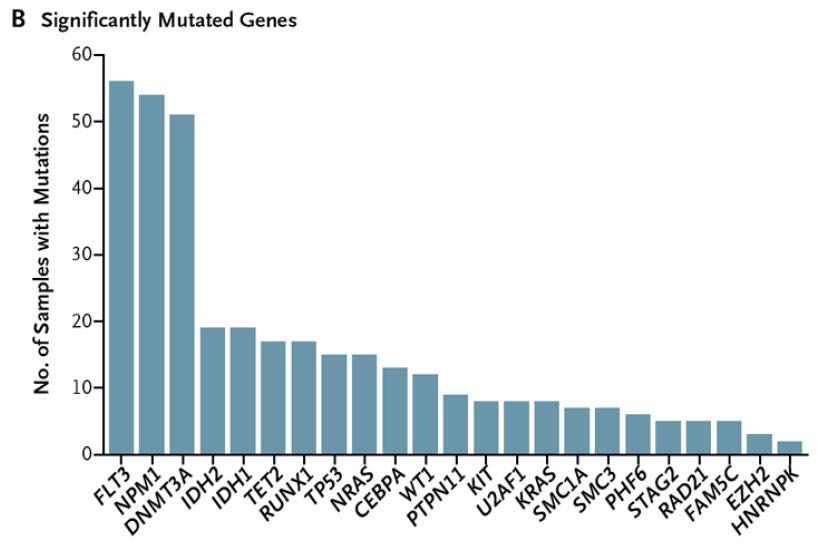
Outcomes in AML patients over
60 years of age
Age CR rate 5 yr OS
60-69 51% 8%
70-79 48% 8%
>80 24% 0
Farag, et al, Blood 2006 (CALGB) Winship Cancer Institute | Emory University 4
Risk CR 2yr DFS
G 82% 62%
I 60-65 32
U 56 39
VU 34 0
Only 10% of
patients received
alloHCT in CR1—
So we have to
figure out how to
get more patients to
International, randomized phase III study
Untreated AML>60, Median age 67yrsalloHCT
High dose daunorubicin vs. standard dose
Lowenberg B, et al. N Engl J Med. 2009;361(13):1235-1248.
Winship Cancer Institute | Emory University 5Studies based on intensive
induction may not
accurately reflect realities
for all older AML patients
National Cancer Institute.
Surveillance, Epidemiology,
and End Results.
SEER Cancer Statistics Review
1988-2004
The point being we have a Klepin HD, et al. Oncologist.
long way to go for “AML in 2009;14(3):222.232.
the older patient”
Although alloHCT is a
critical component of
increasing cures, that
doesn’t mean everyone
should receive 7+3 so they
can get transplanted…
Winship Cancer Institute | Emory University 6Outcomes for older (>60 yrs) AML patients who
received 7 + 3 chemotherapy in CALGB trials
(excludes patients with death < 30 days, excludes CBF) Best of the best….
Mutation Group CR Rate 3-year DFS 3-year OS
NPM1 mutated/FLT3 WT 82% 28% 35%
CEPBPA Double Mutant 50% 33% 17%
IDH1 mutated 60% 15% 19%
IDH2 mutated 58% 15% 26%
p53 mutated 33% 0% 0%
FLT3-ITD positive 63% 8% 14%
RAS or PTPN11 mutated 63% 9% 19%
TET2 or WT1 mutated 53% 10% 11%
EZH2 44% 14% 19%
No mutation 63% 18% 16%
All patients 57% 13% 15%
Winship Cancer Institute | Emory University 7Outcomes for older (>60 yrs) AML patients who
received 7 + 3 chemotherapy in CALGB trials
(excludes patients with death < 30 days, excludes CBF) Best of the best….
Mutation Group CR Rate 3-year DFS 3-year OS
NPM1 mutated/FLT3 WT 82% 28% 35%
CEPBPA Double Mutant 50% 33% 17%
IDH1 mutated 60% 15% 19%
IDH2 mutated 58% 15% 26%
p53 mutated 33% 0% 0%
FLT3-ITD positive 63% 8% 14%
RAS or PTPN11 mutated 63% 9% 19%
TET2 or WT1 mutated 53% 10% 11%
EZH2 44% 14% 19%
No mutation 63% 18% 16%
All patients 57% 13% 15%
Winship Cancer Institute | Emory University 8Outcomes for older (>60 yrs) AML patients who
received 7 + 3 chemotherapy in CALGB trials
(excludes patients with death < 30 days, excludes CBF) Best of the best….
Mutation Group CR Rate 3-year DFS 3-year OS
NPM1 mutated/FLT3 WT 82% 28% 35%
CEPBPA Double Mutant 50% 33% 17%
IDH1 mutated 60% 15% 19%
IDH2 mutated 58% 15% 26%
p53 mutated 33% 16% 0% 0%
FLT3-ITD positive 63% 8% 14%
RAS or PTPN11 mutated 63% 9% 19%
TET2 or WT1 mutated 53% 10% 11%
EZH2 44% 14% 19%
No mutation 63% 18% 16%
All patients 57% 13% 15%
Winship Cancer Institute | Emory University 9INNOVATIVE TRIAL
DESIGN
FOR AML
THE BEAT AML TRIAL
“ONE DOES NOT FIT ALL”
Pis: Byrd, Levine, Druker
Co-I: Blum, Mims, Walker, Borate, Stein, Pollyea, Collins, Stock, Odenike, Foran, othersBIOLOGY OF AML – COMPLEX AND
HETEROGENOUS
Growing number of gene mutations
- Relatively small number per case
- Significant differences between cases
including in co-mutational patterns
- However some groups of mutations
converge on common mechanisms of
transformation (TET/IDH/WT1)
Relapse represents more complex mixture of
disease
- Presence of pre-existence and/or evolution
of resistant subsets within single AML
cases
Targeting early, untreated disease –
potential therapeutic opportunity
11 BLOOD, 21 JANUARY 2010
N Engl J Med 2013; 368:2059-2074
Winship Cancer Institute | Emory University 11EXAMPLE CLINICAL TRIAL TIMELINE:
PATIENT IDENTIFICATION
Assign
Treatment Targeted Initiation
by Marker
Agent of Trial
Patient Bone
Genomic Screening
Registration Marrow
< 1 Week (7 days)
Consent Sample
Alternative therapy
Novel
Agent
Winship Cancer Institute | Emory University 12WHERE ARE WE NOW: ACTIVE CLINICAL
SITES
Clinical Sites
• Memorial Sloan Kettering
• Oregon Health Sciences
• Ohio State University
• UT Southwestern
• Colorado
• Mayo
• U Chicago
• Emory!!!
13
Winship Cancer Institute | Emory University 13Initial Prioritization
1. CBF alterations
2. NPM1 mutation (FLT3 wt)
3. KMT2A (formerly MLL) rearrangement
4. IDH2 mutation
5. IDH1 mutation
6. TP53 mutation
7. FLT3 mutation
8. TET2/WT1 mutation
9. None of the above (or no available trial)
Winship Cancer Institute | Emory University 14M1: Master screening study
S1: Core binding factor---Samalizumab (CD200) plus IC
S2: “HMA sensitive mutations”--AZA plus BI 836858 (glycoengineered CD33 mAb)
“Marker negative”—same therapy, different cohort
S3: AG-221 plus AZA
S4: KMT2A rearranged—Entospletinib (ENTO, Syk inhibitor) plus AZA
S5: TP53 mutated---ENTO plus decitabine
S6: NPM1 mutated (FLT3wt): ENTO plus IC or AZA
S9: TP53 mutated, Pevonedistat plus AZA
S16: IDH1 mutated, AG-120 plus AZA
In negotiations for FLT3 inhibitors, Cdk inhibitors, BRD4, many others
Winship Cancer Institute | Emory University 15M1: Master screening study
S1: Core binding factor---Samalizumab (CD200) plus IC
S2: “HMA sensitive”--AZA plus BI 836858 (glycoengineered CD33 mAb)
marker negative—same therapy, different cohort
S3: AG-221 plus AZA
S4: KMT2A rearranged—Entospletinib (ENTO, Syk inhibitor) plus AZA
S5: TP53 mutated---ENTO plus decitabine
S6: NPM1 mutated (FLT3wt): ENTO plus IC or AZA
S9: TP53 mutated, Pevonedistat plus AZA
S16: IDH1 mutated, AG-120 plus AZA
In negotiations for FLT3 inhibitors, Cdk inhibitors, BRD4, many others
Winship Cancer Institute | Emory University 16Results of a Phase 1b/2 Study of
Entospletinib (GS-9973) Monotherapy and
In Combination With Induction
Chemotherapy In Newly Diagnosed
Patients With Acute Myeloid Leukemia
Alison R. Walker1, John C Byrd1, Bhavana Bhatnagar1,Alice Mims1,Tara Lin2, Howland
E. Croswell3, Danjie Zhang4, Arati V. Rao4, Mark D Minden5, William Blum6
1The Ohio State University, Columbus, Ohio, USA; 2University of Kansas Medical Center, Kansas City, Kansas,
USA; 3Bon Secours St. Francis Health System, Greenville, South Carolina, USA, 4Gilead Sciences, Inc., Foster City,
California, USA; 5Princess Margaret Cancer Centre, Toronto, Ontario, Canada; 6Winship Cancer Institute of Emory
University, Atlanta, Georgia, USARole of SYK in AML
♦ Spleen tyrosine kinase (SYK) is a non-receptor tyrosine kinase primarily
expressed in hematopoietic cells
♦ Constitutive activation of SYK in acute myeloid leukemia (AML) has been
reported; targeted inhibition of SYK-induced differentiation in vitro
demonstrated anti-leukemia activity in AML mouse models1
♦ SYK promotes leukemogenesis by directly phosphorylating the FLT3
receptor, and inducing MEIS1 in conjunction with HOXA9 to form a
regulatory loop in KMT2A (mixed lineage leukemia [MLL]) rearranged
leukemia2,3
1. Boros et al. Oncotarget 2015;6:25575–87; 2. Puissant A. Cancer Cell 2014;25:226-42; 3. Mohr S. Cancer Cell 2017;31:549-62.e11.
18Investigating SYK as Critical Signaling Node in AML
BONE MARROW STROMAL CELL
Hypoxia
CD33 CSF-1R
β2 Integrin
or
FLT3-ITD
FcgRs
P P
P P ROS
SYK Entospletinib SYK
miR-146a
pSTAT3/5 pSTAT5
MEIS1
HOXA9
MLL
Survival and MYC
fusion
Proliferation
AML BLAST
19Study Schema
Allogeneic Stem
CR/CRi Post-Remission Cell Transplant
Lead-in Therapy
Cycle 1–2 ENTO + HiDAC*
Screen ENTO
ENTO +7+3 Treatment Failure
14 d (if completed 2 cycles CR MRD+
No CR of combination Rx)
Maintenance
ENTO x 1 y
Phase 1b n=12
No acute promyelocytic (M3) or
core binding factor leukemias
Phase 2 n=41
All AML patients except M3
*HiDAC: 3 gm/m2Results: Demographics and Baseline Characteristics
Total
N=53
Male, n (%) 31 (58)
Median age, y (range) 60 (18, 78)Conclusions
♦KMT2A
Monotherapy with
rearranged AL ENTO not
is sensitive active
to ENTO withoutside
CR of KMT2A rearrangement
observed
or NPM1on monotherapy
mutation in AML and high response
rates in AL patients treated with combination therapy.
♦3 CR
CRwith
rateENTO
70%single agentpatients
in AML [1 newly diagnosed
treated with ENTO+7+3
AML, 1 R/R AML, 1 ALL +vincristine in t(4;11)]
♦ Overall ENTO is well tolerated and 30-day induction mortality 0%
♦ Higher response rates with SYK inhibition in AML patients with high
HOXA9/MEIS1 expression
♦ Potential role in subsets of AML: KMT2A, NPM1; further development
with the Leukemia Lymphoma Society and the BEAT-AML program
22Conclusions
♦ Monotherapy with ENTO not active outside of KMT2A rearrangement
or NPM1 mutation
♦ CR rate 70% in AML patients treated with ENTO+7+3
♦ Overall ENTO is well tolerated and 30-day induction mortality 0%
♦ Higher response rates with SYK inhibition in AML patients with high
HOXA9/MEIS1 expression
♦ Potential role in subsets of AML: KMT2A, NPM1; further development
with the Leukemia Lymphoma Society and the BEAT-AML program
23Case discussion
• 64 yo female with thrombocytopenia, circulating
blasts, obesity, diabetes, and longstanding
dysfunctional (mild) uterine bleeding (fibroids)
• WBC 10K, 12% blasts in blood
• Hgb 3.8g/dL, PLT 35K
• ECOG PS 2, morbid obesity
• DM II, remote history of “CHF” believed due to HTN
• BMBx, 30% blasts
Winship Cancer Institute | Emory University 24Case discussion
• 64 yo female with thrombocytopenia, circulating
blasts, obesity, diabetes, and longstanding
dysfunctional (mild) uterine bleeding (fibroids)
• WBC 10K, 12% blasts in blood
• Hgb 3.8g/dL, PLT 35K
• ECOG PS 2, morbid obesity
• DM II, remote history of “CHF” believed due to HTN
• BMBx, 30% blasts
• AML with myelodysplasia related changes
• Complex karyotype
• TP53 mutation detected by Master Protocol Screen
Winship Cancer Institute | Emory University 25Winship Cancer Institute | Emory University 26
S5: Phase 2 study of Entospletinib (ENTO) plus decitabine in TP53 mutated AML
• Induction/Cycles 1-3
– All patients will receive ENTO 400mg orally twice daily d1-28 and
decitabine 20 mg/m2 daily by intravenous infusion over 1 hour for
d1-10/28 days.
– A bone marrow biopsy and aspirate will be performed between days 25-30 to determine disease
status after cycle 1 initiation.
– When bone marrow CR/CRi (< 5% blasts) has been confirmed, patients will go on to consolidation
therapy. If NR after 3 cycles, off study.
• Consolidation, decitabine reduced to 5 days for one year, plus ENTO
• Maintenance, ENTO alone
27A PHASE 2 STUDY OF
ENTOSPLETINIB IN
NPM1 MUTANT/FLT3
ITD WILD TYPE AML
PATIENTS AGE > 60
YEARS
BAML-16-001-S6
GILEAD
Protocol Training – Version 2.0 30JUL2017
Uma Borate MDBackground
• NPM1 mutated/FLT3 ITD wildtype group, extended 5 year event free and overall survival
approximates 0.3-0.40 in younger patients. Outcome for elderly NPM1 patients is considerably
worse, with a recent update of the CALGB data22 cited above who did not have an early death
from induction therapy with 7 + 3 chemotherapy using the treatment assignment strategy in
the umbrella study is shown below
NPM1 mutated CR* 1yr DFS 3yr DFS 5yr DFS 1 yr OS 3yr OS 5yr OS
pts with FLT3- WT
86 83% 55%% 27% 24% 71% 34% 27%
• Given single agent ENTO activity (not objective response) seen in prior Phase 1b/2…
29Study Objectives
• Primary Objectives
– To determine the overall survival rate at 3 year in NPM1+/FLT3 wt elderly AML
patients who are treated with ENTO in combination with induction and consolidation
therapy (Cohort A).
• Cohort A: The primary endpoint is 3-year overall survival (OS) rate. The null hypothesis is 3-year OS rate is 35% or
lower. Assuming a true 3-year OS rate of 55%, a total of 62 patients will have 90% power to rule out the null
hypothesis with a one-sided alpha of 0.025
– To determine the overall survival rate at 1 year in NPM1+/FLT3 wt elderly AML
patients of ENTO monotherapy or ENTO + azacitidine (Aza) regimen (Cohort B).
• Cohort B: The primary endpoint is OS rate at 1-year of ENTO monotherapy or ENTO + azacitidine (Aza) regimen. The
null hypothesis is a 1-year OS rate of 50% or lower. Assuming a true 1-year OS rate of 70%, a total of 62 patients will
have 90% power to rule out the null hypothesis with a one-sided alpha of 0.025
30Targeting CD200 with Samalizumab, in combo with intensive induction chemotherapy in CBF+ AML
Approach
Hypothesis
• Inhibition of CD200 may augment the cytotoxic T-lymphocyte (CTL)
mediated immune response against CD200-expressing tumor cells
Samalizumab is a CD200 binding humanized mAb,N=blocking
27 patients,interaction of2-
assuming a true
CD200 with CD200R on macrophages year PFS rate of 70%, this
• Samalizumab monotherapy well tolerated in B-cell malignancies
expansion will have 90% power to
rule out a PFS rate ofTargeting IDH1 and IDH2 mutations in older AML patients (monotherapy data courtesy E Stein)
Introduction Tumor cell
Mitochondrion
• Somatic IDH1 and IDH2 mutations result
in accumulation of oncometabolite 2-HG
2-HG Citrate
→epigenetic changes, impaired Citrate
cellular differentiation 2-HG 2-HG
Isocitrate
2-HG 2-HG Isocitrate
IDH2 IDH1
mIDH2 mIDH1
• mIDH identified in multiple solid and αKG αKG
hematologic tumors NADPH
NADPH
mIDH1 mIDH2
Epigenetic changes
% of AML cases ~6–10% ~9–13% Impaired cellular
differentiation
• AG-120, AG-221: first-in-class, oral, potent, reversible, selective
inhibitors of mIDH1/2 enzymes (respectively)
• under evaluation in multiple clinical trials as a single agent and in
combinations
2-HG = D-2-hydroxyglutarate; IDH = isocitrate dehydrogenase; mIDH = mutant IDH
Winship Cancer Institute | Emory University 34Patient below
achieved CR Clinical
by end of
Cycle 1-IDH1 activity
Dose escalation
Screening
44% blasts mIDH1 mIDH2
R/R AML R/R AML
n=63 n=109
CR, (%) 16 20.2
Cycle 1 CRi/CRp, (%) 13 6.8
Day 15
3% blasts PR, (%) 2 2.8
mCR/MLFS, (%) 3 9.2
SD, (%) 43 53.2
Cycle 1 ORR, (%) 33 38.5
Day 28
2% blasts
CR = complete response; CRi = CR with incomplete neutrophil recovery; CRp = CR with incomplete platelet recovery;
PR = partial response; mCR/MLFS (marrow CR/morphologic leukemia-free state) =Single agent activity in initial studies in AML
well tolerated…
…S3: AG-221 (Enasidenib) in Beat AML
• Window study of AG-221 monotherapy (CR/CRi by 5th cycle) followed
by combo with AZA in mIDH2 AML for patients ineligible (or unwilling) to
receive intensive chemo (following phase
Simon’s two-stage design1with
component)
N=27:
This modified minimax design has 89% power
for our alternative of a 50% CR/CRi rate (rule
outCan we improve response to HMA by selecting for “HMA-sensitizing” mutations? --Novel trials in combo with a glycoengineered CD33 antibody
HMA plus BI 836858
• We observed higher BI 836858–mediated ADCC at day 28 after start of
HMA treatment compared with pre-Rx in ex vivo studies
• this time point coincided with upregulation of NKG2D ligand(s) in primary
leukemia samples from HMA-treated patients
Simon’s 2-stage design N=44:
• LLS study includes separate arms for BI plus AZA
This design has 90% power to
• for “hypomethylating-sensitive” patients (TET2, WT1, IDH1)
correctly rule out a CR rateITS BEEN A YEAR, WHERE ARE WE NOW?? M1 Screening Status (as of 09JUL2018)
BAML-16-001-M1 Screening Status
Site
Grand
101 104 105 106 108 110 111 112 113 115
Total
Pending FM Report 2 0 0 0 0 0 1 0 0 0 3
Pending Sub-Protocol
Consent 2 0 1 0 0 0 0 0 0 1 4
S1-CBF 2 4 0 0 0 0 0 0 0 0 6
Genetic
S2-HMA/other 10 15 4 3 0 3 6 5 1 0 47
screening
results back S3-IDH2 13 5 2 2 0 0 1 2 0 0 25
within 8 days
S4-KMT2A 10 3 2 6 0 0 0 6 0 0 27
in 97%
S5-TP53 7 1 5 0 0 0 0 1 0 1 15
S6-NPM1 6 2 0 0 0 1 0 1 1 0 11
S9-TP53 4 0 0 0 0 1 1 0 0 0 6
Screen Fail 33 8 4 4 0 4 5 1 2 0 61
Treatment assigned
but did not enroll 47 24 11 12 1 10 1 5 2 0 113
Grand Total 136 62 29 27 1 19 15 21 6 2 318
39Beat AML abstracts for ASH 2018
• Update to Master protocol
• S2-AZA plus CD33 mAb
• S3-AZA plus IDH2 inhibitor
• NGS profiling thru treatment and at relapse
• More to come!
Winship Cancer Institute | Emory University 40Clonal evolution from
the primary AML to relapse
a, The founding clone in the primary
tumour with mutations
in DNMT3A, NPM1, PTPRT, SMC3 and
FLT3; one subclone within the founding
clone evolved to become the dominant
clone at relapse by acquiring additional
mutations
b. Model 1 shows the dominant clone in
the primary tumour evolving into the
relapse clone by gaining relapse-specific
mutations;
Model 2 shows a minor clone carrying
the vast majority of the primary tumour
mutations survived and expanded at
relapse.
L Ding et al. Nature 2012Winship Cancer Institute | Emory University 42
You can also read