CAUSES AND CONSEQUENCES: WHAT DETERMINES - OUR SEXUAL AND REPRODUCTIVE HEALTH? - THE EUROPEAN MAGAZINE FOR SEXUAL AND REPRODUCTIVE HEALTH
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

CAUSES AND CoNSEqUENCES: WHAT DETERMINES
oUR SExUAL AND REPRoDUCTIvE HEALTH?
THE EUROPEAN MAGAZINE FOR SEXUAL AND REPRODUCTIVE HEALTH
No.73 - 2011
Contents
The European Magazine for Sexual and
Reproductive Health Editorial
By José Maria Martin-Moreno 3
Entre Nous is published by:
Division of Noncommunicable Diseases Social determinants of sexual and reproductive health:
and Health Promotion A Global Overview
Sexual and Reproductive Health By Jewel Gausman and Shawn Malarcher 4
(incl. Making Pregnancy Safer)
Social determinants of health and Millennium Development Goal
WHO Regional Office for Europe
(MDG) 5: improving maternal health
Scherfigsvej 8
An excerpt from “Progress towards Millennium Development Goals 4, 5, and 6
DK-2100 Copenhagen Ø
in the WHO European Region: 2011 Update.” 8
Denmark
Tel: (+45) 3917 17 17 The Millennium Development Goals, social determinants and sexual
Fax: (+45) 3917 1818 and reproductive health: an overview in Europe
www.euro.who.int/entrenous By Sandra Elisabeth Roelofs and Tamar Khomasuridze 12
Chief editor
Dr Gunta Lazdane UNFPA Regional technical meeting on reducing health inequalities
Editor in eastern Europe and central Asia
Dr Lisa Avery By Rita Columbia 14
Editorial assistant
Jane Persson Sexual and reproductive health in eastern Europe and central Asia:
Layout exploring vulnerable groups’ needs and access to services
Kailow Creative, Denmark. By Manuela Colombini, Susannah H. Mayhew and Bernd Rechel 16
www.kailow.dk
Sexual and reproductive health inequities among Roma
Print in the European Region: lessons learned from the
Kailow Graphic
former Yugoslav Republic of Macedonia
By Sebihana Skenderovska 18
Entre Nous is funded by the United Nations
Population Fund (UNFPA), New York, with the Decreasing inequality in health – moving towards Health 2020
assistance of the World Health Organization Interview with Dr Agis D. Tsourus 20
Regional Office for Europe, Copenhagen,
Denmark. Domestic violence in Romania:
Present distribution figures stand at: 3000 The relationship between social determinants of health and abuse
English, 2000 Spanish, 2000 Portuguese, By Cornelia Rada, Suzana Turcu and Carmen A. Bucinschi 22
1000 Bulgarian and 1500 Russian.
Migrants’ health needs and public health aspects associated with
Entre Nous is produced in: the north Africa crisis
Bulgarian by the Ministry of Health in Bul- By Santino Severoni 24
garia as a part of a UNFPA-funded project;
Portuguese by the General Directorate for Contraceptive behaviour change: beyond contraceptive prescription
Health, Alameda Afonso Henriques 45, By Lisa Ferreira Vicente 26
P-1056 Lisbon, Portugal;
Displaced populations in Georgia:
Russian by the WHO Regional Office for
UNFPA supported sexual and reproductive health programmes
Europe Rigas, Komercfirma S & G;
By Tamar Khomasuridze, Lela Bakradze and Natalia Zakareishvili 28
Spanish by the Instituto de la Mujer, Minis-
terio de Trabajo y Asuntos Sociales, Almagro Resources
36, ES-28010 Madrid, Spain. By Lisa Avery 30
The Portuguese and Spanish issues are
distributed directly through UNFPA repre
sentatives and WHO regional offices to
Portuguese and Spanish speaking countries
in Africa and South America.
Material from Entre Nous may be freely trans-
lated into any national language and reprint-
ed in journals, magazines and newspapers or
2 placed on the web provided due acknowl- The Entre Nous Editorial Advisory Board
edgement is made to Entre Nous, UNFPA and
the WHO Regional Office for Europe. Dr Assia Brandrup- Dr Evert Ketting Prof Ruta Nadisauskiene
Lukanow Senior Research Fellow, Head, Department of Obstetrics
Articles appearing in Entre Nous do not Senior Adviser, Radboud University and Gynaecology
necessarily reflect the views of UNFPA Danish Center for Health Nijmegen Department Lithuanian University of Health
or WHO. Please address enquiries to Research and Development of Public Health, Sciences,
the authors of the signed articles. Faculty of Life Sciences Netherlands Kaunas, Lithuania
For information on WHO-supported activi-
ties and WHO documents, please contact Ms Vicky Claeys Dr Manjula Lusti- Dr Rita Columbia
Dr Gunta Lazdane, Division of Noncom Regional Director, Narasimhan Reproductive Health Advisor
municable Diseases and Health Promotion, International Planned Scientist, Director’s Office UNFPA Regional Office for
Sexual and Reproductive Health at the Parenthood Federation HIV and Sexual and Eastern Europe and Central Asia
address above. European Network Reproductive Health
Please order WHO publications directly from Department of
the WHO sales agent in each country or from Dr Mihai Horga Reproductive Health
Marketing and Dissemination, WHO, Senior Advisor, and Research
CH-1211, Geneva 27, Switzerland East European Institute for WHO headquarters,
Reproductive Health, Geneva, Switzerland
ISSN: 1014-8485 Romania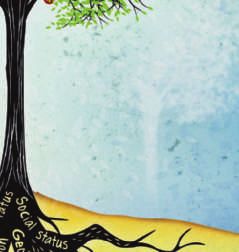
,,
Editorial José
Maria
Martin-
Moreno
As the countdown to the formal deadline to attend antenatal care or to obtain the However, with political will, consider-
for the Millennium Development Goals appropriate information about pregnancy able progress can be made. This issue
in 2015 grows nearer, it is apparent that services. If she happens to reside in a of Entre Nous highlights what progress
gross inequalities in health, including country where public policies penalize and challenges have been made in the
sexual and reproductive health (SRH), are adolescent pregnancy or prevent youth European Region in tackling this very
present both across and within regions friendly health services, she becomes even important issue. It is our hope that long
and countries, globally and in Europe. more marginalized, with limited ability to after you have completed reading the
While it is true that the majority of Mem- access SRH services. All of these aspects articles you will continue to ask yourself
ber States in the WHO European Region combine to greatly reduce both her and “What determines our SRH?” It is only in
have much to celebrate when it comes to her unborn child’s opportunity for posi- continually asking this question that we
progress in improving SRH and increas- tive health outcomes. will be able to address the root causes and
ing access to SRH services, it is also true However, SRH and other health decrease SRH inequities. From our side,
that even in the most affluent countries inequities are not inevitable – quite the the WHO Regional Office for Europe will
of the Region, social injustice exists, with contrary. Health inequities are a problem continue defining goals and targets of
select groups at greater risk of poor SRH for all countries and require actions that the New European Health Policy, Health
outcomes and limited access to SRH move beyond treating adverse health and 2020, gathering best practices and assist-
services. This social gradient holds true SRH outcomes to tackle the underlying ing countries in promoting equity and
across all health fields and in all socie- causes that contribute to them. Across championing the principles of human
ties; the most disadvantaged experience Europe, more and more countries are in- rights.
poorer health and shorter life expectancy. troducing policies that address the social
In order to address this social injustice, determinants of health, but translating
there is an urgent need to move beyond these policies into action remains a chal- Dr José Maria Martin-Moreno,
examining the different statistics that lenge. Doing this successfully requires Director,
highlight these disparities (e.g. maternal that action across all five of the key build- Programme Management,
mortality, neonatal mortality, contracep- ing blocks of the “social determinants
WHO Regional Office for Europe
tive prevalence rate, abortion rate, adoles- approach” recommended by the WHO
cent pregnancy rate, number of antenatal Commission on Social Determinants of
care visits, HIV and sexually transmitted Health is taken. This entails involvement
infections incidence and prevalence) and of multiple sectors at all levels (inter-
ask, “What determines our SRH?” national bodies, governments and civil
In fact, the answer is quite complex. society), with concerted action across the
While genetic susceptibility plays a small following five themes:
role, it is our environment and the condi-
tions in which we live and work that have 1. Governance to tackle the root causes
the greatest impact and effect on our of health inequities: implementing
health. Increasingly, social factors such as action on social determinants of
geographic location, education, employ- health;
ment, economic status, religion, culture, 2. Promoting participation: community
social exclusion, gender and ethnicity are leadership for action on social deter- 3
being identified as the underlying causes minants;
of these health disparities. Individually 3. The role of the health sector, includ-
or in combination, these factors under- ing public health programmes, in
mine more than just SRH health, but reducing health inequities;
also development, sustainability and 4. Global action on social determinants:
overall community wellbeing. Public aligning priorites and stakeholders;
policies that fail to act on these adverse and
social conditions help contribute to 5. Monitoring progress: measurement
unfair and avoidable inequities in SRH and analysis to inform policies and
between groups. For example, a pregnant, build accountability on social deter-
unmarried adolescent girl will likely face minants.
social stigma because of her pregnancy.
Although she attends school, she may Addressing the social determinants
not have the financial means to be able of health can appear overwhelming.
No.73 - 2011
Social Determinants of Sexual
and Reproductive Health:
A Global Overview
T
he World Health Assembly and largest cancer-related cause of life human papillomavirus can lead to the
the World Health Organization years lost in these countries (5). development of genital cancers, while
(WHO) affirm that “sexual and STIs are the main preventable cause
reproductive health is fundamental to Observed imbalances in access to re- of infertility (8). Infertility is often
individuals, couples and families, and sources result in a cycle of disadvantage blamed on the woman, and women
the social and economic development of at the individual level. Evidence demon- may suffer similar negative conse-
communities and nations” (1). strates that less advantaged population quences including humiliation and
In many countries, however, improve- groups are more vulnerable to exposure, physical abuse.
ments in sexual and reproductive health less likely to access health care, and have • Women in developing countries are
(SRH) related outcomes have often been worse health outcomes. Migrant popula- more likely to suffer from chronic dis-
slow despite significant investment. tion, adolescents, and ethnic minorities ability resulting from unsafe abortion
Social and economic inequalities have are often difficult to reach through the or complicated pregnancies. When a
come to the attention of the interna- existing health infrastructure, and face a woman develops an obstetric fistula,
tional community as an important factor variety of legal, social and cultural barri- she not only faces the physical suffer-
driving many health inequalities. Social, ers to accessing SRH services. For many ing associated with the condition, but
demographic, economic and geographic vulnerable groups, issues surrounding may also face divorce, social exclu-
differences within a population are im- language, cultural attitudes, perceptions sion, malnutrition, and increased
portant underlying factors that influence of health service availability, and provider poverty.
access to high quality health care and thus attitudes make accessing services, if they • Environmental factors play an im-
health status. are available, a challenge (6). portant role in women’s susceptibility
At the global level, the world’s poorest Women in many developing countries to rape and gender based violence
countries often struggle with resource also face increased economic vulnerability (GBV). For example, women are often
constraints that limit investment in the which combines with low levels of educa- placed in vulnerable situations while
health infrastructure. As a result, develop- tion and a reduced social status – thereby waiting for transportation at night,
ing countries bear the highest burden of resulting in them having little autonomy collecting water, or using latrines.
disease, including maternal mortality, to make decisions on how or when to seek • Where early marriage and/or
reproductive cancers, and sexually trans- medical care or family planning services. childbearing is prevalent, girls who
mitted infections (STIs) while also facing Underutilization of health services are exposed have less education and
high population growth. by women has been well documented schooling opportunities, less house-
Globally, the magnitude of poverty’s with factors related to underutilization hold and economic power than older
impact on SRH is astounding: of health services grouped into three married women, less exposure to
• Of the 20 million unsafe abortions categories (7). The first includes service modern media and social networks,
that occur each year, 19 million are factors such as affordability, accessibil- are at great risk of GBV, and face
estimated to take place in developing ity, and adequacy of the health system to greater health risks, such as exposure
countries. The consequences of un- meet women’s needs. The second group to HIV and/or having their first birth
safe abortion are also highly variable. addresses user constraints, such as social at a young age (9).
Women living in Sub-Saharan Africa mobility, lack of financial resources, • GBV is rooted in gender inequality. A
are 75 times more likely to die than a and greater demand’s on women’s time, WHO multi-country study on GBV
4 woman living in a developed country and information asymmetries of health found that the prevalence of women
(2). information between women and men. who have suffered physical violence
• The annual incidence of STIs ranged The third group identifies institutional from a male partner ranged from
from 109.7 million new cases in the factors, including men’s decision-making 13% in Japan to 61% in provincial
Africa region to 25.6 in the Eastern power and control over health budgets Peru. In terms of sexual violence,
Mediterranean region. As a com- and facilities, local perceptions of illness, Japan also had the lowest level at 6%,
parison, incidence in the European and stigmatization and discrimination in and Ethiopia had the highest at 59%
Region was estimated at 44.6 (3). health settings. (10).
• Approximately 80% of cervical cancer The following examples illustrate the
cases occur in low-income countries breadth of gender’s influence on SRH, Education is an important mediating
and this is expected to increase to but also highlight how multiple social factor with regard to women’s SRH
90% by 2020 (4). Cervical cancer is determinants often compound to have an outcomes. Increased women’s education
the second most common cancer even greater impact. is not only linked to fertility decline, but
among women living in the devel- • STIs are often more easily transmitted also facilitates the diffusion of ideas re-
oping world, and is also the single to women from men. Infection with garding childbearing, contraception, and
Jewel Shawn
Gausman Malarcher
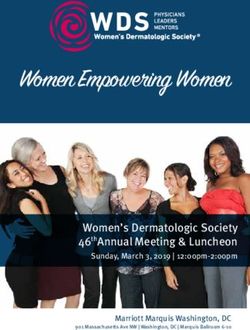
Figure 1. Total Fertility Rate by Highest Educational Level, Selected Countries. include armed conflict and legal systems
Background Characteristics that fail to prosecute sexual violence or
Total fertility rate and proportion of women pregnant Highest educational level
Fertility rates: Total fertility rate No education
protect women’s civil rights (13). A recent
8
Primary analysis in 20 countries with the highest
Secondary or higher
prevalence of child marriage found four
7 factors were strongly associated: educa-
6
tion of girls, age gap between partners,
geographical region and household
5 wealth (13).
For women who are sexually active,
4
modern contraception is the best protec-
3 tion from an unintended pregnancy.
In most developing countries, wealthy
2
individuals are more likely to adopt
1
modern contraception than the poor.
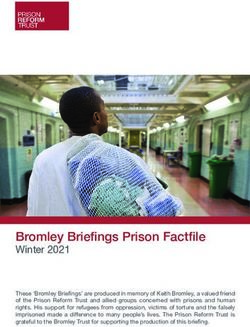
This relationship is illustrated in Figure 2
0 with data from selected developing coun-
Armenia Bangladesh Haiti India Kenya Mali Nigeria Ukraine
DHS 2005 DHS 2007 DHS 2005-06 DHS 2005-06 DHS 2008-09 DHS 2006 DHS 2008 DHS 2007 tries. In all the countries shown, modern
ICF Macro, 2011. MEASURE DHS STATcompiler - http://www.statcompiler.com - October 13 2011. contraceptive use is significantly higher
among women in the highest wealth
quintile versus those in the lowest.
the social status and value placed upon without full and informed consent. Be- Health services are responsible for
women. As shown in Figure 1, fertility yond the potential consequences of STIs providing women with essential informa-
tends to decrease as household educa- and unwanted pregnancy, evidence sug- tion to make an informed choice and suf-
tional level increases. For example, girls gests that sexual coercion negatively af- ficient instruction for correct method use.
with secondary education in Bangladesh, fects victims’ general mental and physical Yet women often receive differential treat-
were nine times less likely to be married well-being. Sexual violence is also asso ment from providers. Studies from Ghana
by their 18th birthday (11). While wealth ciated with risky behaviours such as early and Nepal using “simulated patients”
and educational status are closely related, sexual debut and multiple partners (11, indicate that lower-class, uneducated and
some analysis indicates that education 13). Key factors associated with higher younger clients receive poorer treatment
may moderate the effect of wealth on levels of sexual violence and coercion (14,15). Clients of lower socioeconomic
contraceptive use (7).
A Closer Look at the Social Figure 2. Use of a Modern Method of Family Planning Comparing the Lowest
Determinants of Unintended and Highest Wealth Quintiles, Selected Countries.
Pregnancy Current use of contraception among currently married women
Background Characteristics
Household wealth index
Worldwide, 40% of all pregnancies are Contraceptive method: Any modern method Lowest
Highest
60
unintended (12). The burden of unin-
tended pregnancy disproportionately 5
affects the poor, in almost all countries. 50
Higher rates of unintended pregnancy
have also been observed among young 40
people, the uneducated, ethnic minorities
and migrants compared to more advan- 30
taged groups. Vulnerability to unintended
pregnancy is strongly influenced by access 20
to and use of effective contraception and
by exposure to unwanted sex through 10
child marriage and sexual violence.
Women are particularly susceptible to 0
unwanted sexual activity. Sexual violence Armenia Bangladesh Haiti India Kenya Mali Nigeria Ukraine
DHS 2005 DHS 2007 DHS 2005-06 DHS 2005-06 DHS 2008-09 DHS 2006 DHS 2008 DHS 2007
and child marriage are two common ways
ICF Macro, 2011. MEASURE DHS STATcompiler - http://www.statcompiler.com - October 13 2011.
women are exposed to sexual activity
No.73 - 2011
Social Determinants of Sexual
and Reproductive Health:
A Global Overview (continued)
status and adolescents are especially sus- A number of studies have documented determinants of health include factors
ceptible to restrictive provider practices, higher complication rates and mortality that may directly influence biological
as they have fewer options for where to resulting from unsafe abortion among exposure or susceptibility, such as living
access services (16). women of low socioeconomic status (22). conditions and working conditions, as
The low status of women in many Women from more affluent households well as behavioral, biological, and psycho-
countries restricts their ability to make are more likely to obtain an induced social factors. Health inequities observed
decisions within the household. One way abortion from a physician or nurse, while in a population are driven by a complex
Demographic and Health Surveys capture poor women living in rural areas are relationship between social determinants,
this dynamic is by asking women if they more likely to use a traditional practi- and are mutually reinforced through
are able to decide for themselves to seek tioner or self-induce an abortion. multiple feedback channels.
health care. In the 30 countries where Unintended childbearing detrimentally While the challenge is significant,
data were available, an average of only affects women and children. Women who progress can be made in SRH with
37% of women report they are able to have an unintended pregnancy are more increased attention to the social deter-
seek their own care. In 26 of 30 countries, likely to delay antenatal care or have fewer minants. There are a growing number of
a smaller proportion of women in the visits and experience maternal anxiety, programmes that have been successful
poorest households were able to seek care. depression and abuse (23). Unintended at designing interventions that address
The rich–poor gap ranges from less than children are more likely to experience social determinants and contribute to
1 percentage point in Bangladesh (2004) symptoms of illness, less likely to receive improved SRH. Programmes that have
to 32 percentage points in Peru (2000) treatment or preventive care such as vac- been successful have taken a targeted
(17). cinations, less likely to be breastfed and approach such as fostering community
Women with an unintended pregnancy more likely to have lower nutritional sta- participation, encouraging governments
are faced with a difficult decision, one tus, have fewer educational and develop- to support more equitable policies, and
of which may be abortion. Deciding ment opportunities and are at increased improving data collection to better
whether to terminate an unintended risk of infant mortality (23-25). understand health disparities. In order
pregnancy is influenced by many factors, Improving pregnancy outcomes will to meet the objectives set forth in the
including the availability and accessibility require interventions specifically designed Millennium Development Goals, greater
of induced abortion services, the social to achieve equity in the availability of all attention must be paid to inequities and
acceptability of childbearing and induced related health services, especially targeting the social and economic structures that
abortion, and support from social struc- the poor and disadvantaged for access to contribute to them.
tures. The decision made will have social, contraceptive and skilled birth attendant
financial and health consequences that are services. Such efforts will be most effec
not equally experienced among women. tive when combined with addressing Jewel Gausman, MHS, CPH,
“Unsafe abortion” is defined as a pro upstream determinants, such as improv- Technical Advisor
cedure for terminating pregnancy carried ing education for women and the effective Research, Technology and
out by attendants without appropriate functioning of the health sector and of Utilization Division
skills, or in an environment that does government services in general.
Office of Population and
Reproductive Health
not meet minimum standards for the
USAID
procedure, or both (18). Unsafe abortion What can be done?
jgausman@usaid.gov
6 is a major cause of maternal mortal- The varying levels of inequality present
ity, accounting for an estimated 13% of in a population have an important Shawn Malarcher, MPH,
maternal deaths worldwide (2). In 2005, impact on SRH outcomes. Differences Senior Technical Advisor,
an estimated 5 million women were hos- in control over and access to resources Research, Technology and
pitalized for treatment of complications determine both physical and financial Utilization Division,
from unsafe abortion (19). The highest access to health services. Power dyna Office of Population and
estimated rate of unsafe abortion is in mics also influence quality of clinical Reproductive Health,
Latin America and the Caribbean, where care received by a client. Additionally, USAID,
there are 33 unsafe abortions per 100 live individual health-related behavior is often
smalarcher@usaid.gov
births, followed by Africa (17 per 100 live influenced by norms surrounding social
births) and Asia (13 per 100 live births) position, ethnicity, and gender. At the
(20). Rates of unsafe abortion are highest structural level, the socioeconomic and
among young women, with almost 60% political environments interact with an
of unsafe abortions in Africa occur- individual’s position - social class, gender,
ring among women under age 25 (21). ethnicity, and income. The intermediary
References Medicine National Academies Press, matter? International Bank for Re-
2005. construction and Development and
1. Reproductive Health Strategy to acce 12. Blas, E, Kurup AS. Equity, social World Bank (Washington, DC), 2005.
lerate progress towards the attainment determinants and public health pro 24. Jensen ER, Ahlburg A. Impact of un-
of international development goals and grammes. Geneva: WHO, 2008. wantedness and family size on child
targets. Geneva: WHO, 2004. 13. Bott S. Sexual violence and coercion: health and preventive and curative
2. Unsafe Abortion: global and regional implications for sexual and reproduc- care in developing countries. Policy
estimates of the incidence of unsafe tive health. In: Malarcher S, editor. Matters No. 4. Policy Project, 2000.
abortion and associated mortality in Social determinants of sexual and 25. Wellings K et al. Sexual and repro-
2003. Geneva: WHO, 2007. reproductive health: informing pro ductive health – sexual behaviour in
3. Prevalence and incidence of s elected grammes and future research. Geneva: context: a global perspective. Lancet,
sexually transmitted infections, WHO, 2010. 2006, 368(9548):1706–1728.
Chlamydia trachomatis, Neisseria 14. Huntington D, Lettenmaier C,
gonorrhoeae, syphilis and Trichomonas Obeng-Quaidoo I. User’s perspective
vaginalis: methods and results used of counselling training in Ghana: the
by WHO to generate 2005 estimates. “mystery client” trial. Stud Fam Plann,
Geneva: WHO, 2011. 1990, 21(3):171–177.
4.. Parkin DM, Bray F, Chapter 2: The 15. Schuler SR et al. Barriers to effective
burden of HPV-related cancers. family planning in Nepal. Stud Fam
Vaccine. 2002 Aug; 24 (Supplement Plann, 1985, 16(5):260–270.
3): S11-S25. 16. Tavrow P. How do provider atti-
5. Cancer of the Cervix. WHO. http:// tudes and practices affect sexual and
www.who.int/reproductivehealth/ reproductive health? In: Malarcher S,
topics/cancers/en/. Accessed: October, ed. Social determinants of sexual and
6, 2011. reproductive health: informing pro
6. Female Migrants: Bridging the Gaps grammes and future research. Geneva:
through the Life Cycle. New York: WHO, 2010.
2006. 17. Gwatkins DK et al. Socio-economic
7. Buvini´c M, Médici A, Fernández E et differences in health, nutrition, and
al. Chapter 10: Gender Differentials population within developing coun
in health. In: Jamison DT, Breman JG, tries. Washington, DC: World Bank,
Measham AR et al, editors. Disease 2007.
control priorities in developing 18. Grimes DA et al. Sexual and repro-
countries, 2nd edn. Oxford University ductive health – unsafe abortion: the
Press (New York), 2006. preventable pandemic. Lancet, 2006,
8. Fact Sheet Number 110: Sexually 368(9550):1908–1919.
Transmitted Infections. WHO. 19. Singh S. Hospital admissions resulting
http://www.who.int/mediacentre/ from unsafe abortion: estimates from
factsheets/fs110/en/index.html 13 developing countries. Lancet, 2006, 7
9. Williams LB. Determinants of un 368(9550):1887–1892.
intended childbearing among ever- 20. Sedgh G et al. Induced abortion:
married women in the United States estimated rates and trends worldwide.
1973–1988. Fam Plann Perspect. 1991; Lancet, 2007, 370(9595):1338–1345.
23(5):212–218. 21. Shah I, Ahman E. Age patterns of un-
10. Garcia-Moreno C, Jansen HA, safe abortion in developing country
Ellsberg M et al. WHO Multi-country regions. RHM, 2004, 12(Suppl. 24):
study on women’s health and dome 9–17.
stic violence against women. Geneva: 22. Korejo R, Noorani KJ, Bhutta S.
WHO, 2005. Sociocultural determinants of in-
11. Growing up global: the changing duced abortion. J Coll Physicians Surg
transitions to adulthood in developing Pak, 2003, 13(5): 260–262.
countries. Washington, DC: National 23. Greene ME, Merrick T. Poverty
Research Council and Institute of reduction: does reproductive health
No.73 - 2011Social determinants of health and
Millennium Development Goal (MDG) 5:
improving maternal health
The following is an excerpt • Delay in receiving adequate care when the Region, the percentage of births as-
a facility is reached, for reasons such sisted by skilled health personnel between
from the report “Progress as, but not limited to, shortages of 2000 and 2010 was 98%, compared to
towards Millennium Devel- qualified staff or because electricity, 66% globally (5).
water or medical supplies are not Despite most countries in the Region
opment Goals 4, 5, and 6 in available (2). having almost all births attended by
the WHO European Region: skilled health personnel, there is evi-
Delays will be characterized differently dence of inequities within countries and
2011 Update.” depending on the country context and concerns about quality of the services
where a woman or adolescent girl finds provided. Available data indicate that
MDG 5 aims to improve maternal and herself within that context (i.e. her socio- socially disadvantaged groups (including
reproductive health. Its targets are: economic position, geographic location, populations with lower socioeconomic
A) to reduce by 75%, between 1990 and being of an ethnic minority group or status, ethnic minority groups and
2015, the maternal mortality ratio; irregular migrant experiencing social socially excluded migrants) and rural
B) to achieve, by 2015, universal access to exclusion). populations have poorer access (5-7).
reproductive health. Due to these social determinants, These inequities in the proportion of
inequities in MM between countries are births attended by skilled health person-
Globally, progress towards MDG 5 is stark in the European Region. Accord- nel reflect global trends. For instance,
insufficient. In 2008, there were approxi- ing to estimates from 2008 the country according to the report Progress for
mately 358 000 maternal deaths world- with the highest estimated MMR was children: Achieving the MDGs with Equity,
wide, representing only a 34% decline Kyrgyzstan (with an estimated ratio of in all regions worldwide women from
compared to 1990 (1). Maternal mortality 81) and the lowest estimated ratio was in the richest 20% of households are more
diminished by 2.3 % per year globally Greece (with an estimated ratio of 2) (1). likely than those from the poorest 20%
between 1990 and 2008, which is far short Romania had the fastest rate of decline, of households to deliver their babies with
of the 5.5% annual reduction necessary to with an 84% change in MMR between the assistance of skilled health personnel
achieve target A (1). 1990 and 2008 (1). (8).
In the European Region, the estimated Inequities in MM also persist within
average maternal mortality ratio (MMR) countries. Rural populations tend to have Contraceptive prevalence rate (CPR)
decreased from 44 deaths per 100 000 live higher MM than their urban counter- and the unmet need for family
births to 21 between 1990 and 2008 (1). parts. Ratios and risk vary widely by planning
This represents only a 52% decline when ethnicity, education and wealth status, An estimated one in three maternal
compared to 1990. The annual reduction and remote areas bear a disproportionate deaths globally could be prevented if
of 4.1% is also below the 5.5% needed to burden of deaths. Within urban areas, the women who desired contraception could
reach the target (1). risk of MM and morbidity can also differ have access to it (9). Hence, CPR and
Maternal mortality (MM) is influenced significantly between women living in the unmet need for family planning are
by interlinked social determinants that wealthy and deprived neighborhoods (3). two of the indicators used to monitor
prevent pregnant women from accessing In western Europe, where MM is gener- progress towards MDG 5 target B, which
the health services they need and are ally low, there is evidence of significantly is to achieve by 2015 “universal access to
8 entitled to as a basic human right. These higher risks for migrant and refugee reproductive health”.
determinants, of which the health system populations (4). Gender inequities, ad- Contraceptive prevalence is the per-
is one, collude to result in the “three de- dressed by MDG 3, undermine progress centage of women who are currently us-
lays”, which—when considering maternal to address MM and morbidity. ing, or whose sexual partner is currently
mortality globally—are understood to using, at least one method of contracep-
encompass: Proportion of births attended by tion, regardless of the method used. It is
• Delay in seeking appropriate medical skilled health professionals usually reported for married or in-union
help for an obstetric emergency for One of the indicators for monitoring women aged 15 to 49. The CPR for the
reasons of cost, lack of recognition of progress towards MDG 5 target A is the European Region was 70.7% for the
an emergency, poor education, lack of proportion of births attended by skilled 2000-2010 period (5). Evidence suggests
access to information, administrative health personnel. In the European Region that contraceptive prevalence (using any
barriers and gender inequality; as a whole, overall percentages of births modern method) has generally increased
• Delay in reaching an appropriate attended by skilled health personnel are across the European Region since 1990
facility for reasons of distance, infra- generally high when compared to coun- (10).
structure and transport; and tries in other regions of the world (5). In Women with unmet need for familyTable 1. ANC coverage (%) in select European Member States, by place of cations due to unsafe abortion and 50%
residence, wealth quintile and education level of mother (20). less likely to receive medical treatment,
compared to women in an urban area
ANC coverage
with a high income (16). Lack of quality
Place of Wealth Educational equipment, facilities and care may en-
Country Year
residence uintile
q level of mother
hance the risk of post-abortion complica-
Rural Urban Lowest Highest Lowest Highest tions. Stigma and psychosocial considera-
tions (including those influenced by age
Albania 2008-2009 96.2 99.1 93.3 99.3 96.9 99.4
and cultural beliefs), as well as irregular
Azerbaijan 2006 63.3 89.7 53.2 95.3 63.8 93.5 migrant status, can also be risk factors for
Turkey 2008 84.2 94.7 76.1 98.6 78.3 99.3 unsafe abortion.
Ukraine 2007 98.1 98.7 96.7 98.9 97.8 99.1 Adolescent birth rate
The adolescent birth rate, defined as the
annual number of births given by women
planning are those who are fecund and this is largely due to poor family planning aged 15–19 years per 1000 women in
sexually active but are not using any information in migrants’ home countries the age group, is an indicator for MDG
method of contraception, and report not and inadequate outreach services within 5 target B. Pregnant women under 20
wanting any more children or wanting the health services of the destination years of age face a considerable burden
to delay the birth of their next child. An country (4, 13). of pregnancy-related death and com-
average of 9.7% of women (of reproduc- Low CPR and the unmet need for plications. When compared to women
tive age who were married or in a union) family planning can contribute to higher aged 20–29 years, the risk of dying from
had an unmet need for family planning rates of abortion. Although records in pregnancy-related complications is twice
in the European Region during the 2000- many countries are not comprehensive, as high for girls/women aged 15–19 years
2009 period (5). evidence suggests that eastern Europe and and five times higher for girls aged 10–14
As with other MDG 5 indicators, central Asia has one of the highest abor- (17). Many health problems are particu-
differences can be seen across the social tion rates in the world (14). Cultural con- larly associated with negative outcomes
gradient and by location; that is, women siderations in some population groups, of pregnancy during adolescence. These
with higher incomes, education levels, including reliance on traditional methods include anaemia, sexually transmitted
and urban rather than rural residence of birth control such as withdrawal, can infections, postpartum haemorrhage and
tend to have higher use of contraceptives contribute to higher rates of abortion. mental disorders such as depression (15).
and lower unmet need for family plan- The average induced abortion rate in Taken as a whole, the European Region
ning. An example of urban versus rural countries of western Europe is low, but had an average adolescent birth rate of 24
differences comes from Turkey, where in there is evidence that requests for abor- for the 2000-2008 period (5). According
urban areas the percentage of women us- tion are higher among women with low to the latest data available, San Marino
ing a method of family planning is higher socioeconomic status, particularly if they has the lowest adolescent birth rate (1 per
(74%) than that of women residing in also have migrant status (13). 1000) and Turkey (56 per 1000) has the
rural areas (69%) (11). In some countries of the European highest. Adolescent birth rates have de-
Multidimensional social exclusion Region, abortion still causes more than creased in countries across the European 9
processes—such as those affecting ethnic 20% of all cases of maternal mortality Region (5). In the Caucuses and central
minorities and migrants—can also con- (15). In most of the Member States of the Asia, the adolescent birth rate declined
tribute to lower CPR. There is evidence European Region law permits abortion from 45 in 1990 to 29 in 2008 (18).
that the more pronounced the social to save a women’s life and in more than Adolescent fertility is influenced by a
exclusion (i.e. crossing social, political, half of the countries abortions on request range of social and cultural factors. These
economic and cultural domains), the are permitted. Despite this, it is estimated include but are not limited to gender
lower the prevalence. For instance, in Bul- that half a million unsafe abortions were inequities, low education levels, house-
garia, 65% of richer and more educated performed in 2008 in the European Re- hold poverty and lack of job prospects,
Roma women use any family planning gion, causing 7% of maternal deaths (15). stigmatization about seeking services, and
method, compared to 31% among all Exposure to unsafe abortion is socially early marriage (13). These factors com-
interviewed Roma women (12). Several determined and linked to weak health pound, resulting in more socially disad-
studies suggest that migrants tend to un- systems. Globally, a woman with low vantaged adolescents having less access to
deruse contraceptive methods compared income residing in a rural area is three needed services and less awareness about
to non-migrant populations in Europe; times more likely to suffer from compli- sexual and reproductive health (SRH)
No.73 - 2011Social determinants of health and
Millennium Development Goal (MDG) 5:
improving maternal health (continued)
and rights. Adolescents living in poverty among those in the highest education and perinatal components of basic
are particularly vulnerable. Evidence from level to only 63.8% among women in the benefit packages. Secure sufficient in-
developing countries globally suggests lowest education level. Almost all women vestments for SRH through increased
that an adolescent from a household in (95.3%) of women in the highest wealth awareness among decision-makers of
the poorest quintile is 1.7 to 4 times more quintile receive ANC, compared to only the contribution of health, includ-
likely to give birth than an adolescent 53.2% of women in households in the ing SRH, to the social and economic
from the wealthiest quintile (13). lowest wealth quintile (20). prosperity of countries.
Social and cultural factors play an Other aspects of social exclusion also • Ameliorate data collection and moni-
important role in shaping young people’s influence ANC coverage rates. Inadequate toring and evaluation systems, with
sexual behaviour. Factors such as gender social protection, at times linked to lack mechanisms in place to ensure the ef-
stereotypes, social expectation with re- of necessary documentation, is one of fective use of data on maternal health,
gards to reputations, and the existence of these. Lack of financial coverage for basic FP, SRH behaviour and the needs of
penalties and rewards for sex from society health services contributes to higher vulnerable populations. National in-
are strong determinants of behaviour. maternal mortality ratios among Roma formation systems should account for
Stereotypes can lead to refraining from women, especially when family planning the health status and needs of ado-
planned or rational behaviours in sex and antenatal care services are not cov- lescents and young people (including
practice (i.e. using a condom) and can ered. Reports from the former Yugoslav pregnant adolescents and, linked to
give limited space for young girls to adopt Republic of Macedonia show that Roma MDG 6, the numbers of adolescents
a proactive attitude in negotiating sex mothers often lack health insurance and and young people living with HIV).
practices within a societal paradigm of cannot afford the co-payment and infor- • Ensure quality of SRH services for
femininity and masculinity (19). mal costs linked to regular ANC, delivery all populations. Control for quality
and postnatal care (21). in the RMNCH continuum of care,
Antenatal care coverage Migrant women can also face chal- including for referrals and follow-
Antenatal care (ANC) is an indicator for lenges in access to ANC (13). Even when up allowing for effective coverage.
MDG 5 target B. A minimum of four socioeconomic and educational back- Increase attention to the production
ANC visits is recommended for opti- ground is taken into account, migrant and continuous capacity-building of
mal benefits. Globally, although 80% of women seem to be less likely to seek and/ professionals with the right skills mix
pregnant women received ANC at least or receive adequate ANC and have good and ensure their equitable availability
once during the 2000–2010 period, only pregnancy outcomes. This is especially for all population groups.
53% received the minimum of four ANC the case when the legal status of a migrant • Ensure access to and availability of
visits (5). in a country is unclear, and when women essential medicines and commodities
For the European Region as a whole, perceive local policies and social attitudes for SRH. Provide adequate well-
an average of 97% of women received towards them as negative. maintained equipment at all levels of
ANC from skilled health personnel at maternal/perinatal and SRH care.
least once during pregnancy during the Policy considerations • Create a demand for services through
2000-2010 period (5). In only Azerbai- In the European Region, actions where appropriate communication for
jan and Tajikistan did fewer than 90% particular attention will be required behavioural change. Communication
of women have at least one visit during to accelerate progress towards MDG 5 should be gender-, age-, literacy-level,
10 pregnancy, with coverage being 77% and include: culturally and contextually appropri-
89% respectively (5). Many countries • Increase government political and ate (reflecting thorough knowledge
do not have comprehensive data on the financial commitment for SRH and of the target population’s evolving
minimum of 4 visits. However, available rights. Ensure an enabling legal needs), and address men and tradi-
records points to inequities. and policy framework to overcome tional leaders. Due attention is also
In many countries globally, women access barriers, ensure quality, required to providers’ practices and
from the poorest households are less and strengthenthe Reproductive, attitudes, including towards adoles-
likely to receive ANC than women from maternal, neonatal and child health cents and socially excluded popula-
the wealthiest households (5). While (RMNCH) continuum of care. Facili- tions, that may obstruct patients’
varying considerably by country, in the tate that health reforms are designed access to services.
European Region differences in ANC to expand delivery of SRH services, • Establish multi-sectoral linkages and
coverage can be seen by place of resi- including through strengthened fam- integrate actions to address gen-
dence, wealth quintile and education level ily planning (FP) and service integra- der inequalities and other social
of mother (see Table 1). For instance, in tion in primary health care. determinants of SRH into policies,
Azerbaijan, ANC decreases from 93.8% • Improve financing of the maternal programmes, and laws within andbeyond the health sector. Strengthen NCDs be provided as part of an inte- stry of Health General Directorate of
partnership and coordination grated approach to promote women’s Mother and Child Health and Family
between various stakeholders and and children’s health. Planning, TR Prime Ministry Under-
donors working in SRH areas, child secretary of State Planning Organiza-
health, gender equality and the em- tion and TÜBiTAK, 2009.
powerment of women. 12. Krumova T, Ilieva M. The health
• Increase government support for the status of Romani women in Bulgaria.
active involvement of civil society and Veliko Turnovo, Center for Intereth-
References
communities in the design, provision nic Dialogue and Tolerance “Amalipe”,
and evaluation of SRH policies and 1. Trends in maternal mortality: 1990- 2008.
programmes. In keeping with this, 2008. Geneva: WHO, 2010. 13. Social determinants of sexual and
efforts can also be scaled up to move 2. Report of the Office of the United Na reproductive health: Informing future
beyond the historical approach to tions High Commissioner for Human research and programme implementa
promoting SRH that focuses on the Rights on preventable maternal mor tion. Geneva: WHO, 2010.
deficit model towards one that also tality and morbidity and human rights. 14. A review of progress in maternal health
embraces the assets model and hence Geneva: Human Rights Council, in eastern Europe and central Asia.
accentuates resources of individuals 2010. Doc. A/HRC/14/39 New York: UNFPA, 2009.
and communities. A participatory 3. Shakarishvili G. Poverty and equity 15. Making pregnancy safer: adolescent
approach is a key part of this change. in health care finance: analyzing post- pregnancy [web site]. Geneva: WHO,
• Ensure the rights of adolescents to Soviet healthcare form. Budapest: 2011. http://www.who.int/mak-
age-appropriate information, confi- Local government and Public Service ing_pregnancy_safer/topics/adoles-
dentiality and privacy, and access to Reform Initiative and Open Society cent_pregnancy/en/
services and commodities. Reinforce Institute, 2006. 16. Singh S et al. Abortion worldwide: a
the Convention on the Rights of the 4. Machado MC et al. Maternal and decade of uneven progress. New York:
Child principle of evolving capacities child healthcare for immigrant popula Guttmacher Institute, 2009.
of the child for autonomous decision- tions. Brussels: International Organi- 17. Issues in adolescent health and devel
making and informed consent. zation for Migration, 2009. opment. Adolescent pregnancy – unmet
Indentify and reduce the barriers for 5. World Health Statistics 2011. Geneva: needs and undone deeds. A review of
(pregnant) adolescents to access HIV/ World Health Organization, 2011. the literature and programmes. Ge-
SRH services, including safe abortion 6. Conference document: The Millen neva,: WHO, 2007.
and post-abortion care services where nium Development Goals in the WHO 18. The Millennium Development Goals
abortion is legal. Enforce laws and European Region: health systems Report 2011. New York: UN, 2011.
policies that directly protect most- and health of mothers and children – 19. Marston C, King E. Factors that shape
at-risk adolescents, decriminalize the lessons learned. Copenhagen: WHO young people’s sexual behaviour:
behaviours that place them most at Regional Office for Europe (EUR/ a systematic review. Lancet, 2006;
risk, and ensure that they have access RC57/8), 2007. 368:1581-1586.
to the services they need and are 7. Lloyd CB. Growing up global: the 20. Azerbaijan Demographic and Health
protected from stigma. changing transitions to adulthood in survey 2006. Calverton, Maryland:
• Address the links between non- developing countries. Washington, DC, State Statistical Committee [Azerbai- 11
communicable diseases (NCDs) and National Research Council, 2005. jan] and Macro International Inc,
MDG 5. NCDs increasingly affect 8. Progress for children: Achieving 2008.
women and children across the the MDGs with equity. New York: (http://www.measuredhs.com/pubs/
RMNCH continuum of care. For UNICEF, 2010. pdf/FR195/FR195.pdf, accessed 1July
instance, obesity in women increases 9. Gender Justice and the M illennium 2011).
the risk of gestational diabetes, Development Goals. New York: 21. Report on the Progress towards the
pre-eclampsia, pregnancy-related hy- UNIFEM, 2010. Millennium Development Goals. Sko-
pertension, induced labour, caesarian 10. World Contraceptive Use 2010. (POP/ pje: Government of the Republic of
sections and stillbirths. The RMNCH DB/CP/Rev2010), New York: UN, Macedonia. 2009.
continuum of care provides several Department of Economic and Social 22. Keeping the promise: united to
opportunities to prevent, diagnose Affairs, Population Division, 2011. achieve the Millennium Development
and treat NCDs. The Global Strategy 11. Turkey demographic and health survey Goals. Resolution. General Assembly,
for Women’s and Children’s Health 2008. Ankara: Hacettepe University Sixty-fifth session, Agenda items 13
recommends that health services for Institute of Population Studies, Mini and 15. New York: UN, 2010.
No.73 - 2011The Millennium Development Goals, social
determinants and sexual and reproductive
health: an overview in Europe
T
he social determinants of health Figure 1. Maternal mortality rate in selected western and eastern European
are directly linked to develop- countries, latest available data (3).
ment and therefore will directly
contribute to Europe’s ability to reaching,
or not, the set Millennium Development
Goals (MDGs) for the year 2015. Beyond
that year, the health sector will transform
these goals into a new challenge, called
“Health 2020”.
As an essential part of the WHO
Regional Office for Europe’s Member
States public health landscape, sexual and
reproductive health (SRH) is particularly
sensitive to the social determinants of
health. These determinants influence to
which extent a man or woman of repro-
ductive age can benefit from SRH services
in his or her country and thus, his or her
SRH health outcomes. In this article we
will highlight how these factors impact Economic and social status experience continued missed opportuni-
both the supply and demand side of SRH The relationship between poor SRH and ties for equitable access to care.
services and how this contributes to the poverty has been well established; not
accessibility, quality and affordability of only is the burden of ill SRH outcomes Migration and internally displaced
offered SRH services. greater in low resource settings, but populations (IDPs)
also greatest among the populations in While not traditionally thought of as a
Culture, ethnic diversity and age the lowest wealth quintiles in these low social determinant of health, experience
The countries that make up the European resource countries. Throughout Europe in the European Region with migrants
Region are diverse, with many different varying rates of utilization of antenatal and IDPs has clearly shown that migra-
ethnicities, cultural practices and age care and maternal mortality rates are tion is an important determinant that
groups. All of these factors have a rela- seen (figure 1 and 2). The correlation must be considered when addressing SRH
tionship with how SRH is perceived and between income and poor SRH indica- programmes and policies and improv-
practiced. For example early marriage and tors is easy to interpret; higher maternal ing SRH outcomes for individuals and
childbearing may be more common among mortality rates are seen in countries with communities. Armed conflicts disrupt
certain ethnic groups. Such practices may lower incomes level and greater utiliza- health services and IDPs in countries with
impact negatively on SRH as studies have tion of antenatal care services among territorial disputes are often unders-
shown that women who experience preg- higher income groups compared to lower erved in the field of SRH services and at
nancy and childbirth at a young age are at income groups. However, the relationship increased risk to adverse SRH outcomes.
increased risk of morbidity and mortality between poverty and poor SRH utiliza- Such conflicts also pose a threat to the
12 (1, 2). From a supply side such groups tion and outcomes is complex and may implementation of the national SRH
may be excluded from SRH services due reflect a variety of other issues that influ- agenda of countries, weakening the health
to issues such as lack of cultural sensitivi ence these inequities, such as: inability systems ability to deliver services and
ty and/or language barriers that limit the to access services due to opportunity its responsiveness for well implemented
interaction between the client and care costs; social exclusion due to discrimina- quality control mechanisms.
provider. Age may also affect the ability to tion and marginalization of select lower
access or receive services. While adoles- socio-economic or ethnic population Programmatic and policy gaps
cents may feel uncomfortable accessing groups; inability to demand equal and fair Many countries in the eastern part of the
traditional SRH health services for infor- treatment from providers due to feelings European Region find themselves in a
mation about SRH, societal attitudes and of exclusion; and inequitable distribution transitional period, moving away from
beliefs towards sexuality of adolescents of SRH services favouring higher income a centrally planned economy towards a
can also limit access to care through poli- areas (urban vs. rural). All of these factors merit-based society in a system of free
cies that prevent Youth Friendly Health interact together to create a complex envi- market mechanisms. In this era of finan-
Services or fail to recognize the rights of ronment that ensures that those who are cial crises and donor fatigue it is para-
adolescents to also have positive SRH. most vulnerable to poor SRH outcomes mount to rely more and more on eachSandra Tamar
Elisabeth Khoma-
Roelofs suridze
Figure 2. Use of antenatal care by different socio-economic groups stakeholders of the relationship between
in the European Region, latest available data (3). social determinants of health and SRH.
Reducing inequities in SRH requires in-
volvement not only of the health systems
but also education, labour and social
sectors. Advocacy about these inequities
should occur at all levels and across all
sectors in order to diminish the health
risks faced by all populations, particularly
vulnerable and marginalized groups.
Europe has an ambitious agenda wishing
to ensure universal access to SRH services
for all its citizens, relying on European
standards of care. It is time to act, learn
Figure 3. Age-standartized death rate (SDR) of cervical cancer among 0-64, from each other’s best practices and
per 100 000 and the coverage rate within the national screening implement the commitments that have
programmes in selected countries, latest available data (3). been made in 2000 on the UN MDGs and
in Cairo at the International Conference
on Population and Development. With
the right commitment and the right
instruments to map and address the
social determinants of health and SRH,
we will quickly get closer to a society with
reduced inequalities and more accessible
and affordable care.
H.E. Sandra Elisabeth Roelofs,
WHO Europe Goodwill Ambassador
for health-related MDGs,
Chairperson of National Reproduc-
tive Health Council, Georgia,
Tamar Khomasuridze, MD, PhD,
country’s own resources, local public- health care system will help close this gap UNFPA AR, Georgia
private partnerships, creative co-financing and improve outcomes. Taken this one
schemes of federal, regional and mu- step further and incorporating health For correspondence contact:
nicipal governments and strengthening education on reproductive tract cancers geoccm@caucasus.net
of the medical insurance infrastructure and screening into the education sector
(increasing the insurance base can lead helps strengthen the efforts and coverage
to inclusion of more SRH services in the of the health system. Countries who have References 13
basic care package). Such actions require recognized these gaps and have imple- 1. Mayor S. Pregnancy and childbirth
coordination among the stakeholders of mented well organized national screening are leading causes of death in teenage
the existing donor, government and civil programmes with a high coverage rate girls in developing countries. BMJ,
society community in order to ensure achieve much better outcomes in terms of 2004;328:1152-1159.
programmatic and policy gaps are mini- cervical cancer morbidity and mortality 2. DuPlessis HM, Bell R, Richards
mized and that synergy exists between (figure 3). T.Adolescent pregnancy: Understand-
sectors. For example, national policies ing the impact of age and race on
that address reproductive tract cancers Conclusion outcomes. J Adolescent Health, 1997;
need to recognize that lack of organized National ownership of an area like SRH 20: 187-197.
population-based preventive and early can only be reached through increased 3. WHO Health For All Database. Ac-
detection services leads to negative SRH political commitment and strong con- cessed September 24 2011 at: http://
outcomes. Implementation of screening tinuous lobbying for SRH and rights of www.euro.who.int/en/what-we-do/
and early detection, a very cost-efficient individuals and populations. Essential to data-and-evidence/databases/europe-
measure, into each country’s primary this commitment is recognition by all key an-health-for-all-database-hfa-db2
No.73 - 2011You can also read