"Charcot" Sarah Rincker, DPM, FACFAS - A Multi-Disciplinary Road to Success - PeaceHealth
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Sarah Rincker, DPM, FACFAS “Charcot” A Multi-Disciplinary Road to Success
Disclosure I have received no financial or in-kind support from any commercial or other organization.
“A chronic, progressive condition of bones, joints, and soft tissues, most commonly occurring in the area of the foot and ankle as a result of peripheral neuropathy” *There have been no reported cases of CN developing in the absence of neuropathy.
History 1703 - Musgrave - Venereal Disease 1831 - Mitchell - Spinal Lesions and Rheumatism of LE 1868 - Charcot - Spinal Damage from Tabes Dorsalis Demonstration of Arthropathic Affections of Locomotor Ataxia @ 7th International Medical Congress in 1881 Established as a distinct pathological entity 1936 Jordan - DM a possible cause

Ulcers & Amputation Risk Charcot neuropathic osteoarthropathy increases the affected patient’s risk of foot ulcer by more than 30-fold. (15-31%) 63 % of persons with Charcot foot eventually develop a foot ulcer Using Medicare data, Wrobel and Mayfield demonstrated that diabetes increases the risk of major amputation by 10-fold. According to Sohn et al. 2010, the risk of amputation in those patients with Charcot foot is 6.6 % in the community, and more than double in VA patients at 14.7 %. When Charcot Foot occurs with foot ulcer, the patient is at a 12-fold higher risk of amputation than patients with Charcot alone Charcot Foot has also been described to be an independent risk factor for mortality after controlling for foot ulcer and other comorbid conditions

Pathophysiology

Two Main Theories: My Patient Explanation Neurotraumatic Theory: The inciting event is trauma. Without the presence of protective sensation, the patient continues to bear weight, eventually leading to a clinical scenerio that mimics a hypertrophic non-union. Johnson Neurovascular Theory: Autonomic peripheral neuropathy creates a high-flow vascular state which increases blood flow. This “washes out” structural calcium from the bone, leading to localized osteopenia and mechanically induced deformity associated with continued weight-bearing. Saltzman The truth is likely a combination of both theories.

Osteoclastogenesis The Details
Classify

Sanders Classification: Anatomic Location Clearly highlights the midfoot as the most targeted area for Charcot development. It has been hypothesized that limited ankle joint range of motion coupled with neuropathy and obesity may predispose the mid-foot for breakdown.
Eichenholz Classification (1966) J Diabetes Res. 2016
Classification: Stage 0 A prodromal state of the disease (Shibata: Leprotic patients; Sella: Diabetic Patients) Foot demonstrates changes including redness, swelling, warmth, and pain, signs typically representing inflammation, in the neuropathic patient. These signs and symptoms are antecedent to foot architecture breakdown, seen in the later stages of CN.
Diagnosis
Diagnosis: History Patient is often not aware of any injury 0.1-29% of DM with PN However trauma has been reported in 22-53% of cases Previous Pancreas or Kidney Transplant Previous foot surgery Iron Deficiency Diabetic Nephropathy Rheumatoid Arthritis Osteomyelitis Obesity Revascularization Elevated HbA1c Peripheral Sensory Neuropathy (Accepted Necessary Condition) Autonomic Neuropathy
Diagnosis Signs of Inflammation Difficult to differentiate between Gout attack, DVT, Cellulitis, and Phlegmon with Osteomyelitis 50% of patients have pain Usually bounding pulses unless obscured by edema Late Stage: Fracture/joint dislocation; rocker bottom foot with possible ulceration; critical limb ischemia more common
Temperature Gradient Armstrong and Lavery 1997: N=39 Unilateral acute Charcot foot after 15 min’ rest avg 8.8 ± 2.3 °F higher temperature compared to the contralateral joint of interest. In a separate study, the same team reported specific mean joint differences of 7.3 °F, 8.0 °F, and 8.8 °F for the ankle Chopart, and Lisfranc’s joint respectively. Najafi 2012: the temperature difference between CN affected and contralateral foot is magnified after walking 50 steps; ( = 1 . 2 0 and = 0 . 5 2 at baseline versus = 1 . 9 4 and = 0 . 7 0 at 50 steps).
Labs Nonspecific and Non definitive Patients with CN may have Leukocytosis Elevated hsCRP and ESR as seen with other inflammatory conditions. Hemoglobin A1C elevation of > 7 % is common
The Late Foot Look White Arrow: Instability of the foot, and dorsal collapse of the forefoot Black Arrow: Gastrocsoleus contraction and plantar inclination of calcaneus
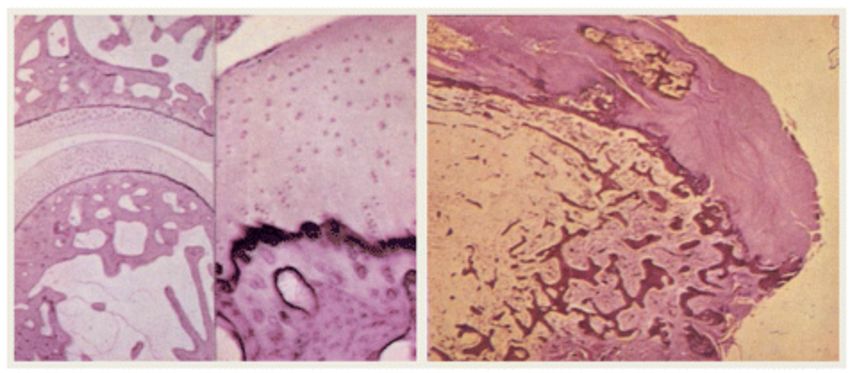
Histology Usually used to differentiate Osteomyelitis from Charcot In patients with a normal joint, the articular cartilage is smooth, chondrocytes line up in regular rolls and subchondral cancellous bone is intact. In joints affected by CN there are degenerating fibrillary remains of cartilage, absence of cartilage, and fibro osseous tissue, characteristics of reactive bone with presence of woven bone that was immature and structurally disorganized. Further the bone marrow spaces were infiltrated with hypervascular, myxoid tissue with spindle fibroblasts, increase in the number of Howship’s lacunae and a decreased number of osteocytes.
Diagnostic Imaging The diagnosis of active Charcot foot is primarily based on history and clinical findings but should be confirmed by imaging. Inflammation plays a key role in the pathophysiology of the Charcot foot and is the earliest clinical finding. The occurrence of acute foot/ankle fractures or dislocations in neuropathic individuals is considered active CN because of the inflammatory process of bone healing, even in the absence of deformity. X-rays should be the initial imaging performed, and one should look for subtle fractures or subluxations if no obvious pathology is visible. MRI or nuclear imaging can confirm clinical suspicions in the presence of normal-appearing radiographs.
Imaging X-Ray Changes on X-Ray are delayed and have low sensitivity Late changes are shown
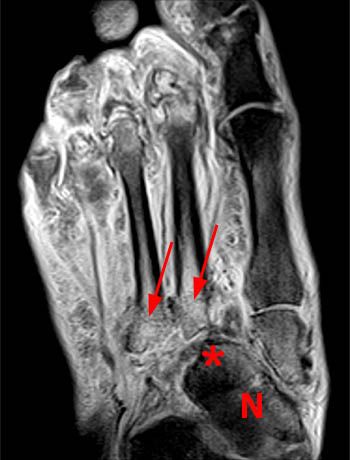
MRI Very valuable method for the early stages of the illness when X-ray imaging alone results in practically normal findings. An important finding is edema of the bone marrow of two or more bones, edema of the adjacent soft tissues, and fluid in several joints or cortical fractures. If conservative treatment is begun during this phase the condition is “reversible”
Nuclear Medicine If patient cannot get MRI Order both: Bone scan: High sensitivity and low specificity WBC label: Highly sensitive and specific for infection, but difficult to differentiate bone and soft tissue Sulfer Colloid LFDG-PET/CT
Charcot vs Osteomyelitis Active CN and Acute Osteomyelitis have the same clinical symptoms. (Chronic may be masked). No wound: very unlikely Osteomyelitis Wound >2cm^2 or deeper than 3mm, high predictive value of Osteomyelitis Probe to bone (38-94% sensitivity and 85-98% specificity) >70mm/hr ESR, likely osteomyelitis Imaging per above Bone Biopsy: GOLD STANDARD
Conservative Treatment Offloading Antiresorptive Therapy Bone-Growth Stimulator Protective Weightbearing
Offloading If you suspect Charcot: immediately offload and immobilize Total contact casting (TCC) is the “gold standard” to offload and immobilize. (2-3 days then weekly to avoid pistoning as the edema subsides) It is imperative to continue casting until the edema has subsided and the temperatures are then within 2° C of the contralateral foot. If the patient can be nonweightbearing, they do heal faster (avg 1-103months stage 1) Noncompliance of offloading has been shown to increase healing time ~6months Diabetic shoe on non-charcot limb Evidence of healing on X-Rays and MRI with clinical findings, transition to custom molded shoes, AFO, or CROW
Antiresorptive Therapy Proposed because bone turnover is excessive in patients with active Charcot. Currently there are conflicting reports on specific uses. Systematic reviews of clinical trials have indicated bisphosphonates are ineffective and may even be harmful to the resolution time of the acute phase of Charcot. In contrast, other 51 studies at the same level of evidence have supported their use, suggesting that bisphosphonates may improve resolution time of the acute phase by reducing skin temperature and disease activity. 52
Bone Growth Stimulators There is limited evidence for usage, but conducted studies have validated utilization as an adjunct therapy. Acute stage and Time of Surgical Fusion Diabetic bone marrow is very poor to heal due to being very soft. Additionally, there is decreased mobilization of stem cells from the bone marrow due to microangiopathy, neuropathy, stem cell rare fraction, and excess fat deposition in the diabetic population.
Protective Weightbearing Required after an active episode has coalesced and quieted. Utilizing some type of custom-molded shoe with rocker bottom, ankle foot orthosis, or CROW walker is recommended. is limited evidence for usage, but conducted studies have validated utilization as an adjunct therapy.
Surgical Treatment Primarily based on expert opinion; however, those who benefit most from surgery tend to be those patients who are recalcitrant to bracing, have tried custom CROW walker or patellar tracking orthosis brace and custom-molded shoes, and who continue to see breakdown. There is low-quality evidence and certainly no randomized controlled trials have been performed to perpetrate which surgical treatment works best for each specific type of Charcot, but the time to refer to an experienced surgeon is when bracing is no longer an option or the foot/ankle becomes unstable. Surgical treatment generally has been advised for resection of infected bone, removing bony prominences that could not be accommodated in orthotic shoewear, or correcting significant deformities that could not be accommodated with therapeutic footwear, custom ankle-foot orthoses, or CROW walkers. 54
Surgical Goal Lower extremity stability Infection free Plantigrade foot Brace vs Shoe
Prognostic Surgical Success Indicators Wukich et al in 2016 published the only robust study to date on this topic, reporting a 40% prevalence rate of PAD in 85 patients with CN The presence of renal disease confers a 3.7-fold increased likelihood for a major LEA—a rate much higher than that reported in other studies. Delay in healing > 30 days after index closure is associated with a 2.6 times increased likelihood of major amputation.
Prognostic Surgical Success Indicators Postop OM imparts a 2.4-fold increased likelihood for a major amputation. Preop OM has been show to increase risk of major amputations by 3.4x (non-charcot patients) Eradication with Wide resection Cultures and ID consult
Prognostic Surgical Success Indicators The presence of a Charcot-related foot wound at presentation increased the likelihood of a major lower extremity amputation by a factor of 6. Other risk factors that were associated with major amputation in patients included active infection at presentation, nonunion/ instability after reconstruction, and a postoperative wound problem. The overall rate of successful limb salvage in patients deemed reconstructive candidates was 90%.
N=285 Our avg Patient
Major Amputation Risks
Charcot Summary Diagnostics and Treatment
Acute Charcot Pathway of Clinical Care
Acute Charcot Pathway of Clinical Care
Acute Charcot Pathway of Clinical Care
Acute Charcot Pathway of Clinical Care
Acute Charcot Pathway of Clinical Care
Acute Charcot Pathway of Clinical Care
Wound Care Debridement Vascular Optimization Infection Control Blood Sugar Control Offloading TCC, iTCC, CROW Ex Fix Surgery
Diabetic Offloading Diabetics compliance is a major issue: Snyder RJ, et al. JAPMA. 2014 Non-removable offloading to heal plantar neuropathic forefoot ulcer (i.e. TCC); Therapeutic footwear for prevention of plantar foot ulcer recurrence, not enough evidence to support a specific offloading for any other type of ulcer: Bus, et al on behalf of IWGDF. Diabetes/Metabolism Research & Reviews. 2015 5/7 Studies showed non-removable devices lead to higher healing rate than removable: Cochrane Review 2013. TCC has significantly higher percentage rate and time of healing than offloading sandal or walking boot: Lavery, et al., International Wound Journal. 2014. TCC decreases forefoot pressure by 65-84% and heel pressure by 45%. Birke, Hartsell, Wertsch
TCC CROW iTCC
My Humble Practice TCC (or iTCC) NO infection Any stage of Charcot CROW Infection Some Stage 2 and 3 patients who need more aggressive wound care treatment then q week
What if it doesn’t work or reulcerates? External Fixator for offloading Surgery to address the deformity Exostectomy if Stable Reconstruction if Unstable Osteomyelitis ID c/s Surgery: reconstruction, exostectomy, debridement, amputation
Exostectomy
Reconstruction A long road to recovery
NPWT Since its initial development, NPWT has gained widespread acceptance for a broad range of wound indications, including those found among diabetic CN. NPWT can be used to treat CN wounds produced as a result of neuropathy and deformity, following debridement of infection or amputation, and in reconstructive soft tissue and osseous procedures. Several studies emphasize that treatment outcomes are often based on the specific techniques and materials used for NPWT application, therefore additional suitably powered, high-quality clinical trials are needed to fully determine efficacy. Careful patient and procedure selection along with appropriate technique is imperative for successful use of NPWT in the diabetic CN foot and ankle.
References • NIDDK NIH Summary Report Charcot Workshop, co-sponsored by NIH’s Office of Rare Diseases (2008), http://archives.niddk.nih.gov/ neuroarthropathy/SummaryReport.pdf,/neuroarthropathy/summaryreport.pdf • Sohn M-W, Lee Todd A, Stuck R, Frykberg R, Budiman-Mak E. Mortality risk of Charcot arthropathy compared with that of dibaetic foot ulcer and diabetes alone. Diabetes Care. 2009;32:816–21.PubMed CentralView ArticlePubMedGoogle Scholar • Rogers L, Frykberg R, Armstrong D, Boulton A, Edmonds M, Georges H, et al. The Charcot Foot in Diabetes. Diabetes Care. 2011;34(9):2123– 9.PubMed CentralView ArticlePubMedGoogle Scholar • Wukich D, Sung W, Wipf AM, Armstrong D. The consequences of complacency: managing the effects of unrecognized Charcot feet. Diabet Med. 2011;28:195–8.View ArticlePubMedGoogle Scholar • Eichenholtz SN. Charcot Joints. IL, USA: Springfield; 1966. Charles C. Thomas.Google Scholar • Shibata T, Tada K, Hashizume C. The results of arthrodesis of the ankle for leprotic neuroarthropathy. J Bone Joint Surg Am. 1990;72:749– 56.PubMedGoogle Scholar • Sella E, Barrette C. Staging of Charcot Neuroarthropathy Along the Medial Column of the Foot in the Diabetic Patient. J Foot Ankle Surg. 1999;38(1):34–40.View ArticlePubMedGoogle Scholar • Ndip A, Williams A, Jude E, Serracino-Inglott F, Richardson S, Smyth JV, et al. The RANKL/RANK/OPG Signaling Pathway Mediates Medial Arterial Calcification in Diabetic Charcot Neuroarthropathy. Diabetes. 2011;60(8):2187–96.PubMed CentralView ArticlePubMedGoogle Scholar • Wukich D, Sung W. Charcot arthropathy of the foot and ankle: modern concepts and management review. J Diabetes Complications. 2009;23(6): 409–26.View ArticlePubMedGoogle Scholar • Pakarinen TK, Laine J, Honkonen E, Peltonen J, Oksala H, Lahtela J. Charcot Arthropathy of the Diabetic Foot. Current Concepts and Review of 36 Cases. Scand J Surg. 2002;91(2):195–201.PubMedGoogle Scholar
References Sommer TC, Lee TH. Charcot foot: the diagnostic dilemma. Am Family Physcian. 2001;64:1591–8.Google Scholar Sinha S, Munichoodappa C, Kozak G. Neuroarthropathy (Charcot Joints) In Diabetes Mellitus. Medicine. 1972;51(3):191–210.View ArticlePubMedGoogle Scholar Fabrin J, Larsen K, Holstein PE. Long term follow up in diabetic Charcot feet with spontaneous onset. Diabetes Care. 2000;23(6):6796–800.View ArticleGoogle Scholar Lavery L, Armstrong D, Wunderlich R, Tredwell J, Boulton A. Diabetic Foot Syndrome: Evaluating the prevalence and incidence of foot pathology in Mexican Americans and non-hispanic whites from a diabetes disease management cohort. Diabetes Care. 2003;26(5):1435–8.View ArticlePubMedGoogle Scholar Koeck FX, Bobrik V, Fassold A, Grifka J, Kessler S, Straub R. Marked loss of sympathetic nerve fibers in chronic Charcot foot of diabetic origin compared to ankle joint osteoarthritis. J Orthop Res. 2009;27(6):736–41.View ArticlePubMedGoogle Scholar Mabilleau G, Petrova N, Edmonds ME, Sabokbar A. Number of Circulating CD14-Positive Cells and the Serum Levels of TNF-alpha are Raised in Acute Charcot Foot. Diabetes Care. 2011;34(3):33.View ArticleGoogle Scholar Frykberg R, Belczyk R. Epidemiology of the Charcot Foot. Clin Podiatr Med Surg. 2008;25(1):17–28.View ArticlePubMedGoogle Scholar Petrova NL, Foster VM, Edmonds ME. Calcaneal bone mineral density in patients with Charcot neuropathic osteoarthropathy: differences between Type 1 and Type 2 diabetes. Diabet Med. 2005;22:756–61.View ArticlePubMedGoogle Scholar Matricali GA, Bammens B, Kuypers D, Flour M, Mathieu C. Diabetic Nephropathy but not HbA1c is predictive for frequent complications of Charcot feet –long term follow up of 164 patients with 195 acute Charcot feet. Exp Clin Endocrinol Diabetes. 2012;120(30):335–9.Google Scholar
References Samann A. Diabetic Nephropathy but not HbA1c is predictive for frequent complications of Charcot feet –long term follow up of 164 patients with 195 acute Charcot feet. Exp Clin Endocrinol Diabetes. 2012;120(30):335–9.PubMedGoogle Scholar Munson M, Wrobel J, Holmes C, Hanauer D. Data Mining for Identifying Novel Associations amnd Temporal Relationships with Charcot Foot. J Diabetes Res. 2014;2014:214353.PubMed CentralView ArticlePubMedGoogle Scholar Wrobel JS, Mayfield J, Reibar G. Geographic Variation of Lower-Extremity Major Amputation in Individuals With and Without Diabetes in the Medicare Population. Diabetes Care. 2001;24(5):860–4.View ArticlePubMedGoogle Scholar Sohn MW, Stuck R, Pinzur M, Lee T, Budiman-Mak E. Lower-Extremity Amputation Risk after Charcot Arthropathy and Diabetic Foot Ulcer. Diabetes Care. 2010;33:98–100.PubMed CentralView ArticlePubMedGoogle Scholar Rogers L, Bevilacqua N. Imaging of the Charcot Foot. Clin Podiatr Med Surg. 2008;25:43–51.View ArticlePubMedGoogle Scholar Rogers L, Frykberg R. The Charcot Foot. Med Clin N Am. 2013;97:847–56.View ArticlePubMedGoogle Scholar Sanders LJ, Mrdjenovich D. Anatomical patterns of bone and joint destruction in neuropathic diabetics. Diabetes. 1991;40 Suppl 1:529A.Google Scholar Sanders LJ, Frykberg RG. Diabetic Neuropathic Osteoarthropathy: The Charcot Foot, 297–338. In: Frykberg RG, editor. The High Risk Foot In Diabetes Mellitus. New York: Churchill Livingstone; 1991.Google Scholar Armstrong D, Lavery L. The natural history of acute Charcot’s arthropathy in a diabetic foot specialty clinic. Diabet Med. 1997;14:357–63.View ArticlePubMedGoogle Scholar Armstrong DG, Lavery LA, Liswood PJ, Todd WF, Tredwell JA. Infrared dermal thermometry for the high-risk diabetic foot. Phys Ther. 1997;77(2):169– 75. discussion 176–7.PubMedGoogle Scholar
References Petrova NL, Edmonds ME. Charcot neuro-osteoarthropathy-current standards. Diabetes Metab Res Rev. 2008;24 Suppl 1:S58–61.View ArticlePubMedGoogle Scholar Wrobel JS, Connolly JE, Beach ML. Associations between static and functional measures of joint function in the foot and ankle. J Am Podiatr Med Assoc. 2004;94(6):535–41.View ArticlePubMedGoogle Scholar Armstrong DG, Lavery LA. Monitoring healing of acute Charcot’s arthropathy with infrared dermal thermometry. J Rehabil Res Dev. 1997;34:317–21.PubMedGoogle Scholar Najafi B, Wrobel JS, Grewal G, Menzies RA, Talal TK, Zirie M, et al. Plantar Temperature Response to Walking in Diabetes with and without Acute Charcot: The Charcot Activity Response Test. J Aging Res. 2012;2012:140968.PubMed CentralView ArticlePubMedGoogle Scholar Najafi B, Crews RT, Wrobel JS. The Importance of Time Spent Standing for those at Risk of Diabetic Foot Ulceration. Diabetes Care. 2010;33(11): 2448–50.PubMed CentralView ArticlePubMedGoogle Scholar Stuck RM, Sohn MW, Budiman-Mak E, Lee TA, Weiss KB. Charcot Arthropathy Risk Elevation in the Obese Diabetic Population. Am J Med. 2008;121(11):1008–14.View ArticlePubMedGoogle Scholar Geschickter CF, Cannon A. Colour Atlas of Pathology: Central Nervous System. London, Philadelphia: Pitman Medical Publishing Co. Ltd; 1963. Lippingcott.Google Scholar La Fontaine J, Shibuya N, Sampson W, Valderrama P. Trabecular Quality and Cellular Characteristics of Normal, Diabetic, and Charcot Bone. J Foot Ankle Surg. 2011;50:648–53.View ArticlePubMedGoogle Scholar Chantelau E, Gruetzner G. Is the Eichenholtz classification still valid for the diabetic Charcot Foot? Swiss Med Wkly. 2014;144:w13948. The European Journal of Medical Sciences.PubMedGoogle Scholar
References Palestro CJ, Love C, Tronco GG, Tomas JN, Rini JN. Combined Labeled Leukocyte and Technetium 99 m Sulfur Colloid Bone Marrow Imaging for Diagnosing Musculoskeletal Infection 1. RadioGraphics. 2006;26:859–70.View ArticlePubMedGoogle Scholar Van Nostrand D, Abreu SH, Callaghan JJ, Atkins FB, Stoops HC, Savory CG. In-111–labeled white blood cell uptake in noninfected closed fracture in humans: prospective study. Radiology. 1988;167:495–8.View ArticlePubMedGoogle Scholar Hayashida K, Ochi T, Fujimoto M, Owaki H, Shimaoka Y, Ono K, et al. Bone marrow changes in adjuvant-induced and collagen-induced arthritis. Interleukin-1 and interleukin-6 activity and abnormal myelopoiesis. Arthritis Rheum. 1992;35:241–5. 660. 15.View ArticlePubMedGoogle Scholar Rosenberg AE. Robbins and Cotran pathologic basis of disease. 7th ed. Philadelphia, Pa: Elsevier Saunders; 2005. p. 1273–324.Google Scholar Littenberg B, Mushlin A. Technetium Bone Scanning in the Diagnosis of Osteomyelitis: A Meta-analysis of Test Performance. J Gen Intern Med. 1992;7:158–63.View ArticlePubMedGoogle Scholar Schauwecker DS. The scintigraphic diagnsosi of osteomyelitis. Am J Roentgenol. 1992;158:9–18.View ArticleGoogle Scholar Thakur ML, Lavender R, Silvester D, Segal A. Indium 111 Labeled Autologous Leukocytes in Man. J Nuc Med. 1977;18:1014–21.Google Scholar Boc SF, Brazzo K, Lavian D. Acute Charcot foot changes versus osteomyelitis: does Tc-99 m HMPAO labeled leukocytes scan differentiate? JAPMA. 2001;7(91):365–8.Google Scholar Morbach H, Schneider P, Schwarz T, Hofmann C, Neubauer H, Duren C, et al. Comparison of magnetic resonance imaging and 99mTechnetium- labelled methylene diphosphonate bone scintigraphy in the initial assessment of chronic non-bacterial osteomyelitis of childhood and adolescents. Clin Exp Rheumatol. 2012;30:578–82.PubMedGoogle Scholar Palestro CJ, Mehta MM, Patel M, Freemanm SJ. Marrow versus infection in the Charcot joint: Indium-Ill leukocyte and technetium-99 m sulfur colloid scintigraphy. J Nucl Med. 1998;39:346–50.PubMedGoogle Scholar
References Palestro CJ, Torres MA. Radionuclide imaging in orthopedic infections. Semin Nucl Med. 1997;27:334–45.View ArticlePubMedGoogle Scholar Milne T, Rogers JR, Kinnear EM, Martin HV, Lazzarini PA, Quinton TR, et al. Developing an evidence-based clinical pathway for the assessment, diagnosis and management of acute Charcot Neuro-Arthropathy: a systematic review. J Foot Ankle Res. 2013;6:30.PubMed CentralView ArticlePubMedGoogle Scholar Irie K. Calcitonin gene-related peptide (CGRP)-containing nerve fibers in bone tissue and their involvement in bone remodeling. Microsc Res Tech. 2002;58:85–90.View ArticlePubMedGoogle Scholar Burns PR. The pathogenesis of Charcot neuroarthropathy: current concepts. Diabet Foot Ankle. 2012. doi:10.3402/dfa.v3i0.12236.Google Scholar Weitzmann NM. The Role of Inflammatory Cytokines, the RANKL/OPG Axis, and the Immunoskeletal Interface in Physiological Bone Turnover and Osteoporosis. Scientifica. 2013;2013:125705. doi:10.1155/2013/125705.PubMed CentralView ArticlePubMedGoogle Scholar Mabilleau G. Increased osteoclastic activity in acute Charcot’s osteoarthropathy: the role of receptor activator of nuclear factor-kappaB ligand. Diabetologia. 2008;51:1035–40.PubMed CentralView ArticlePubMedGoogle Scholar Sinha S, Munichoodappa C, Kozak G. Neuro-arthropathy (Charcot joints) in diabetes mellitus. Medicine. 1971;51:191–210.View ArticleGoogle Scholar Cofield RH, Motrisin M, Beabout JW. Diabetic neuroarthropathy in the foot: patient characteristics and patterns of radiographic changes. Foot Ankle Int. 1983;4:15–22.View ArticleGoogle Scholar Sanders L, Frykberg R. Charcot neuroathropathy of the foot. In: Bowker J, Pfeifer M, editors. The Diabetic Foot. 6th ed. Mosby: St. Louis; 2001. p. 439–66.Google Scholar
Thank You! Cell: 614-600-9075
You can also read