Cleveland Clinic Health System: A Comprehensive Framework for a Health System Patient Safety Initiative
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Q Manage Health Cair
Vot, 14. No. 2, |j|,i. ao-90
© :dU05 LippincoU WilHiims & Wilkins. tnr.
Cleveland Clinic Health System: A
Comprehensive Framework for a Health System
Patient Safety Initiative
Deborah M. Nadzam, PhD, RN; P. Mardeen Atkins, MPA, RN, CPHQ;
D, Michael Waggoner, MD; Richard Shonk, MD, PhD
The Cleveland Clinic Health System (CCHS) is BACKGROUND
committed to the enhancement of patient safety
throughout the CCHS. Tbis article describes the The Cleveland Clinic: Health System (CCHS) is a
CCHS patient safety initiative, the development, not-for-profit health system organized between 1996
objectives, strategies, goals, and activities. and 1998 through the merger of not-for-profit orga-
nizations located in northeast Ohio. It consists of 9
acute care hospitals, a children's rehabilitation hos-
pital, physician group practices, a physician orga-
nization for contracting, and other units providing
support services such as home health care and
nurse-on-call. The Cleveland Clinic is a large refer-
ral hospital and serves local, national, and inter-
national patients. Two of the acute care hospitals
are medium-sized tertiary care community hospitals,
each with approximately 400 beds, providing full
services including cardiac surgery (excluding trans-
plants). The remaining 6 acute care hospitals are
smaller community-based general hospitals.
The CCHS's strategic approach and infrastruc-
ture to performance measurement and improvement
embraces 3 main initiatives: (1) clinical services,
(2) patient satisfaction, and (3) patient safety. The in-
frastructure to support these 3 initiatives has been
established to meet the measurement and improve-
ment priorities of the CCHS. The infrastructure serves
as the measurement and analysis backbone of the
CCHS performance plan. The CCHS Strategic Per-
formance Measurement and Improvement Plan de-
scribes tbe 3 strategic initiatives and associated goals.
Figure 1 depicts the structural model of the CCHS
Strategic Performance Measurement and Improve-
ment Plan. Kac:b side of the performance pyramid
From thn Quality Institute (Drs Nadzam and Shonk), Pa-
tient Safety and Patient Satisfaction (Ms Atkins), and Med-
Key words: event reporting, medical errors, patient ical Opem/io/j.s. Eastern Region (Dr Waggoner), Cleveland
safety, safety framework and strategies Clinic Health System, Cleveland. Ohia.
80
Cleveland Clinic Health System 81
Patient LAUNCHING THE PATIENT SAFETY
INITIATIVE
Unit'ciircgiver
The CCHS patient safety initiative is coordinated
through the Ql. Coordination by the QI helps to
Division/
dcpanment*
achieve the primary objective by facilitating the set-
ting of system-level goals, sharing safe practices
across the CCHS organizations, aggregating and an-
Hospital'oulpatient sellings alyzing events reported at CCHS sites, and dissemi-
nating results of event analyses and process alerts.
Region
The CCHS Patient Safety Team (Safety Team) was
formed in 2000 and represents all CCHS hospitals.
CCHS It includes individuals from a variety of disciplines:
medical staff leaders, chief nurse executives, quality
Clinical Pmcessn and Oulcomc«
managers, a pharmacy director, risk managers, om-
*Rercn Io clinical and suppnn dcpariinciiu
budsman personnel, general counsel, environmen-
tal safety specnalist, laboratory technologist, and staff
Figure 1. Structural model ot the CCHS Strategic Performance from the QI. The safety team accepted the charge to
and Improvement Plan. provide general direction and oversight for the CCHS
patient safety plan and quickly developed a concep-
tual framework to focus its activities for prevention
represents 1 of the 3 strategic initiatives. The hase of harm to patients.
of the pyramid represents the CCHS level. Levels
supported by CCHS are regional, hospital/outpntient, CONCEPTUAL FRAMEWORK
division/dupartment, and unit/caregiver. Initiatives
for each level are based on the CCHS plan. All lev- The safety team outlined 7 strategies to achieve
els' activities point to the patient and communities the primary objective of prevention of harm to pa-
we serve—the rocipient{s) of care (at the top of the tients: promotion of a culture of safety; increased re-
figure). Under the guidance of the CCHS Medical porting of adverse events and error-prone processes;
Operations Council (physician leaders of each hos- enhanced communication between health care pro-
pital). The Quality Inslitute (Q!) manages tho CCHS fessionals and patients about patient safety issues
performance improvement initinlives. in collabora- and solutions: increased learning from analysis of
tion with multiple CCHS teams and the regional and reported adverse events; focused process redesign
hospital staffs.' when and where indicated: promotion of the appro-
Patient safety is an integral component of the CCHS priate application of technology; and focused edu-
strategic approach to performance improvement. The cation about now safety enhancement issues (eg, re-
framework is integrated with the 2 other primary per- designed processes, retraining, application of new
formance improvement initiatives—clinical services technology, evidence-based findings from the liter-
and patient satisfaction. The CCHS patient safely ini- ature). Figure 2 displays the relationship of the 7
tiative supports one side of the pyramid (shaded strategies to each other. As noted in Figure 2, it is
on Fig 1) and provides the basic expectations for also expected that contribution to the scientific body
CCHS facilities'.safety plans at regional, hospital, and of knowledge (eg, presentations and publications)
smaller organizational unit levels. The single most will result from these activities. The safety team pro-
important objective of the CCHS patient safety initia- ceeded with developing the CCHS annual patient
tive is to prevent barm to the patient. safety plan based on the 7 strategies, defining goals
82 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 14, ISSUE 2, APRIL-JUNE 2005
I. Promotion of a
Culture otSafetv
2. Increased Reporting
of Adverse Events and
Error-prone Processes
4. Increased Learning from
3. Increased
Analysis of Reported Adverse
Communication
Events
about Safety
Issues
5. Focused 6. Promotion of 7. Pociised
Process the Appropriate Education about
Redesign Application of New Safet)
Technologv Enhancement
Activities
Contribution
to Scientific
Prevention Literature
of Patient
I larm
Figure 2. Seven strategies for patient safety (reducing occurrence and minimizing risk of adverse events).
and activities for each (see Fig 3 for a sample page of An environment in which patienls. their fam-
the 2001 work plan). ilies, and organization staff and leaders can
A brief description of each strategy depicted in identify and maiiage actual and potential risks
Figure 2 follows. to patient safety. This environment encourages
recognition and acknowledgement of risk to pa-
Strategy 1: Promotion of a culture of safety tient safety and medical/health care errors; the
initiation of actions to reduce these risks; the
The intent of this strategy is to support and pro- internal reporting of what has been found and
mote a culture of safety across the CCHS. The Joint the actions taken; a focus on processes and sys-
Commission on Accreditation of Healthcare Orga- tems; and minimization of individual blame or
nizations's definition of "culture of safety" was retribution for involvement in a medical/health
adopted: care error. It encourages organizational learning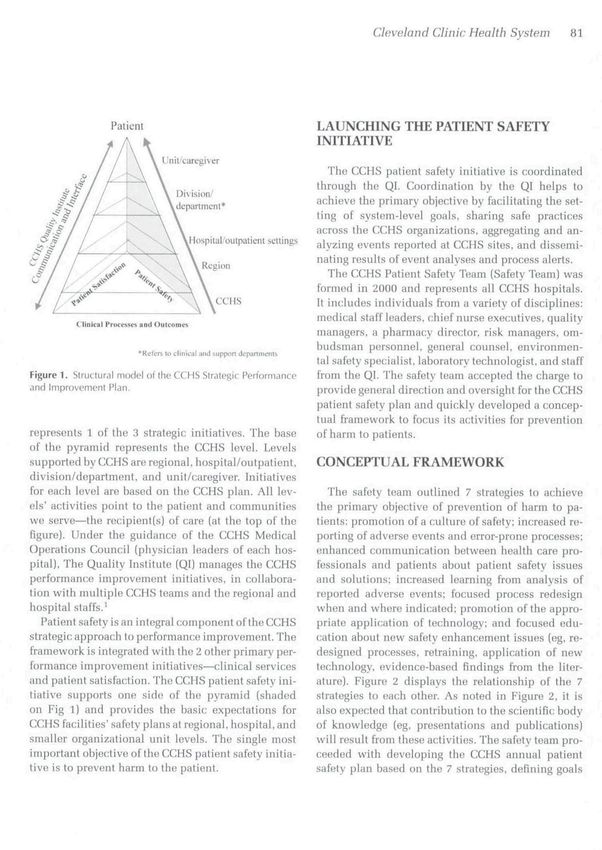
Cleveland Clinic Health System 83
10
01 c d) -2
S! -9 c o c o ro
ra O) O cr TJ "u
t is .w — _ra
Ol> (11
Q S ra O l ?•
CJ
ro
to
_
d) XJ
ra
O
ra Q ^ T^
(D
"TO
to ^
O
E
Q.
II o .ro o
I/] ro • D "D ^ C o ^
g.|-a,N
.S5 (D
d) o a;
inii
:ian
ipo
1 := H» ra = d) d)
Q. K
Q- ._
S CL d) E
ro « S
E g S o
O 0) E 9-O
— >• Q. O O Q) o
O £ CO -6 c w
CQ CQ o
c
>•- o
o ^
'c
E
o
ro c
t: tn
E 6i ID 13 ra Q.fc
9vent
repo
a) "D
X ro CD C31 C
ro LU -9 ^ £ .C ra 5
c
>- to o to tu
10 • o
u. O .•K 5 ra ro
c "o in
O tl. g o
S O
o
^ ™ CO .3 B
o ra
« o :^ •a X
1
liS'
i n Q.
o a, 'c ro d)
istra
ra ra to
ro
0) O
JO
Q) O CL ro
C Q. o
d)
y t " O
a
O LU
O >. ro
ntit
0) 3
LLJ E o re ra o o ra o Tj -— 3 •— o X U- V
z CC to
O o ra '35 C-:^ Ol "o ^ $ d)
oO ID d)
O £ CL O CLLU '- cy CO -a- O cn d) n Q o o O o
CO < CO CO CQ
01
Q. "D ro
O C a
9> u>
•o "S P I
B c OJ c
u
0 O c — u
1 £ E dJ
in .i "re
q E D Q. Q-
00
o
^ ^ ra ra ra ra u
•U .£ "D Q. Q.
ro !« _ (0
Q. O
the
5 ifl S "> o. >
o .EG ro o dJ c O >. (1) a. ^ c ro
ra c
tiv
"o ro - -c: S c d)
0. ^ X ^ Q) ra S-= OJ
2J 5 F 3 — .
o ^ -S > £ Q)
!= ra O I a. ^ o 15 O O
3 w O O o =; •E -52 .c N
o 2- S o E .>• §* c in ^
i 5> £ f to (1) ^ d)
ro CO E .£ o 2
1- o 10 £ o < :s
CO -^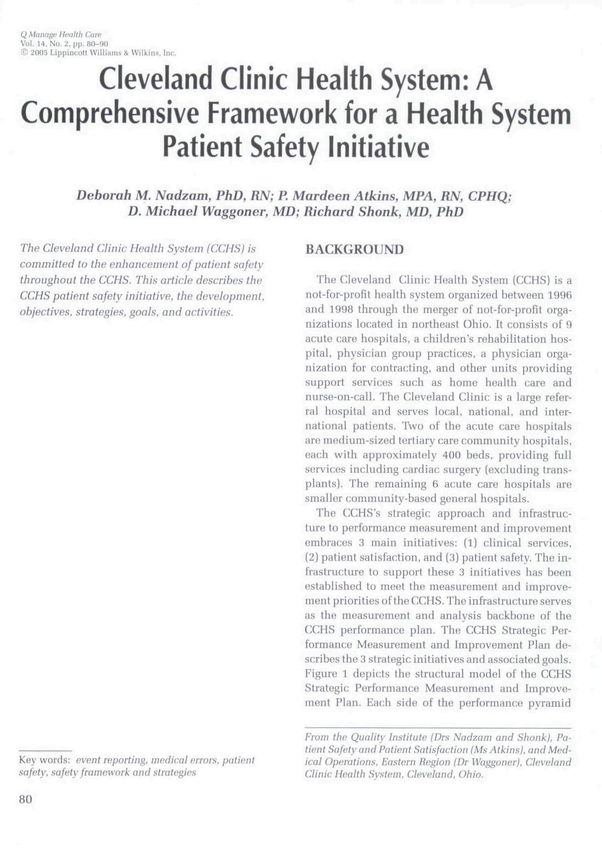
84
Raiated JCAHO Task (The activity to be dona Responsible Maasurea of Education
Goals safety standards and the time frame needed) person effectiveness requiremmt
A structure to oversee patient LD5
safety is in place for the Implementation of Safety Initiative
CCHS and at each CCHS
hospital
The scope of the patient safety LD5
initiative is defined Definition of scope of initiative and
The culture and commitment to types of occurrences to report
patient safety is highly visible
throughout the organization
CCHS hospitals successfully
adopt a nonpunitive approach
to adverse event
assessmentand resolution
Education initiatives for HR4,2
managers, employees, and Education of employees. Orientation
physicians are developed and and ongoing
QUALITY MANAGEMENT IN HEALTM CARE/VOLUME
implemented IM.1
A comprehensive needs assessment.
Consider the following questions,
as appropriate: what are the
barriers to effective communication
among caregivers?
Processes for ensuring accurate,
timely, and complete vert3al and
written communication among
caregivers and all others involved
in the use of data
•D
T3
O
14, ISSUE 2, APKII.-JUNE 2005Cleveland Clinic Health System 85
about mediral/health care errors and supports the event occurred, and what system changes are in-
the sharing of that knowledge to effect behav- dicated to prevent similar events from occurring in
ioral changes in it and other health care organi- future. Increased reporting of a//adverse events and
zations to improve patient safety. error-prone processes will provide more data upon
which to assess system pt^rformance. Trends and pat-
A primary characteristic of a culture of safety is a terns will be more easily identified. Several of the
nonpunitive approach to the reporting of errors, with hospitals within the system approached this strat-
a focus on the process or system involved instead egy by providing a pharmacist to concurrently re-
ofthe individual employees.*^"" The safely team be- view medication orders on the patient care units. Be-
lieved that without this culture, achievement of the sides promoting a coUegial and educational milieu
other 6 strategies and corresponding objectives and the number of medication errors reported showed a
goals would he compromised. Improving the process dramatic increase.
or system will result in organizational performance
improvement—a culture of gain. To promote a cul- Strategy 3: Enhanced comnwnication hetween
ture of safety, CCHS leadership adopted a nonpuni- health care professionals and patients ahout
tive stance with regard to reporting of adverse events. patient safety issues and solutions
Disciplinary action is not taken against employees
The intent of the third strategy is to promote
who report or are involved in an adverse event upon
open communication among health care profession-
discovery as long as the employee is willing to fully
als about the occurrence of an adverse event, as
cooperate with the management in investigating the
well as jibout the identification of a "broken" pro-
factors that lead to the event to determine the sys-
cess thai could lead to an adverse event. This was
tem/process issues involved and provided that none
accomplished in many ways but was probably best
ofthe exceptions listed below are present:
demonstrated by the system's implementation of sur-
1. Intentional acts to harm or deceive; gical site marking and the taking of "time outs." Sur-
2. Reckless or intentional disregard for standard geons, anesthesiologists, nurses, and patients all par-
operating procedures; ticipated in a common effort to prevent errors.
3. In the event that staff performance/competency In addition, enhanced communication with pa-
is a root cause for an adverse event, management tients and families may serve immediately to pre-
will make every reasonable effort to determine vent tbe occurrence of an adverse event, as well as to
if the involved staff member can reliably deliver identify processes needing redesign. Patient-centered
safe care through further education and counsel- care is 1 of the fi aims for the 21st century health
ing. If it appears that a staff member cannot prac- care system and should also be viewed as a method
tice in a reliably safe manner, the situation will for reducing errors tbat reach the patient.'" For ex-
be treated as a staff performance/competency is- ample, encouraging patients and family members to
sue through the usual process. question caregivers about new medications and treat-
ments could actually identify an error about to hap-
Strategy 2: Increased reporting of adverse events pen, if the caregiver realizes that a medication or
and error-prone processes treatment is actually not ordered for the question-
The intent of the second strategy is to encourage ing patient; the •'iioar-miss" error is prevented and
tbe reporting of al 1 adverse events and errors (includ- a system prohlem that almost led to an error may be
ing those that did not reach tho patient). Increased uncovered.""^" Key to involving tbe patient and fam-
reporting of adverse events and errors is highly de- ily in care at CCHS hospitals was the implementation
pendent on the existence of a nonpunitive culture. of a decision to show a videotaped message to newly
Major adverse events—sentinel events—are currently admitted patients. The message features hospital ex-
identified, reported, and analyzed to determine how ecutives speaking directly to the patient and family86 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 14, ISSUE 2, APRIL-JUNE 2005
about specific ways in which they can get involved reduce the occurrence and/or minimize the risk of ad-
in their care. While not overtly describing error-prone verse events. Although partially dependent on anal-
processes, the general ititent of the message is to "be ysis of adverse events (Strategy 4), such solutions
part of your care; be involved; and ask questions." may be identified through external sources as well.
In addition, this strategy focuses on improved use of
Strategy 4: Increased teaming from analysis af existing technology, Iticluding medical devices. For
reported adverse events example, the system has benefited from collective ap-
The intent of the fourth strategy is to enhance proaches to exploring patient identification technol-
the current use of data related to adverse events. ogy and intravenous pump safety features.
Increased learning is dependent upon increased re-
porting (Strategy 2) and improved analysis."^"^'^^"^^ Strategy 7: Focused education ahout new safety
Each CCHS hospital independently benefits from in- enhancement issues
creased reporting if enhanced atialysis follows. Cen- The intent of lhe seventh strategy is to educate
tralizing the reporting and analysis of adverse events health care professionals about general and specific
across the entire CCHS further enhances the ability to activities related to the enhancement of patient safety
identify both effective and probhnnatic trends. Shar- and reduction of adverse events. This strategy will de-
ing and learning from each otber also leads to sys- pend on content from the previous strategies, as well
tem changes that could prevent future adverse events as from external sources. Education of the patient
throughout CCHS. This strategy was best exemplified and family is also included in this strategy, which
in oiu- experience by the analysis of the medication includes a focus on involving tbe patient/family in
errors data, especially those errors that did not reach his or her care to maximize safety and reduce the oc-
the patient. These data were enhanced by the pharma- currence of adverse events. One way the system pro-
cist initiative referred to under Strategy 2 and demon- motes the culture of safety and at the same time pro-
strate how these strategies are interdependent. motes its own best performers is by highlighting their
efforts and outcomes at our ann ual Patient Safety con-
Strategy 5: Focused process redesign when and ference where they present along with invited nation-
where indicated ally known speakers.
Tbe intent of the fifth strategy is to fix system prob-
lems identified through the analysis of reported ad- Implementation
verse events. This strategy is dependent on increased Once the safety team defined specific goals for the
learning from analysis of events (Strategy 4}. By en- 7 strategies, system-level activities were identified,
hanced analysis of sentinel events, and of trends and with hospital-level activities stated (when indicated).
patterns of other reported adverse events and near The CCHS patient safety annual work plan is
misses, the organization can identify processes that hased on the primary objective and outlines-related
are in need of redesign. Through the reporting of goals and activities at the CCHS level and at the re-
comparative data at our Medical Operations Council, gional/hospital level to implement the safety initia-
the system was able to effect measmable improve- tive. Most of the activities proposed for regions and
ment from sharing of best practices, for example, the hospitals allow for flexible interpretation and imple-
impIetTietitation of a common process for specimen mentation to meet local needs.
labeling. Eacb CCHS hospital developed a patient safety
plan that is derived from the CCHS initiative, but in-
Strategy 6: Promatian of the appropriate cludes more detail and specificity of the local needs
application of technology and activities to meet the CCHS safety goals. Over-
The intent of the sixth strategy is to evaluate and se- sight responsibility for hospital-level plans is deter-
lectively implement technological solutions that will mined by each hospital, altbougb periodic updatesCleveland Clinic Heolth System 87
about hospital-level activities are provided to the QI. breaks in skin integrity. Additional measures
Table 1 lists specific: activities for each strategy in may be added and defined. Measures may change
place across the CCHS. on an annual basis.
• Improvement in physician and employee per-
TOPIC-SPECIFIC SAFETY TEAMS ception of culture as nonpunitive with regard to
reporting of adverse events.
Tbere are 3 additional safely-relatod totims, also • Increase in reporting of errors.
staffed by tbe QI: Medication Systems. Skin Integrity, • Report of feeling actively involved in patient's
and Even! Reporting. Tbe Medication Systoms team care by patients and families.
includes a registered nurse and a pbarmacist from
each CCHS bospital. This team addresses process is-
sues primarily related to tbe safe preparation, dis- Summary
pensation, and administration of medications. At the The systemwide patient safety initiative as de-
request of tbe CCHS chief nurse executives, tbe QI scribed in this article is well underway at the CCHS.
launcbed tbe Skin Integrity team. Its primary goal including activities for each of our 7 strategies. A
is to prevent nosocomial pressure ulcers and effec- cbange in the human resource's policy related to es-
tively treat pressure ulcers present on inpatient ad- tablishing a nonpunitive culture represents a key first
mission. Following a systemwide prevalence study step in redefining the culture. Heightened awareness
in January 2001. subcommittees of the; team de- of safety is also facilitating the cultural shift. Addi-
veloped standardized protocols for prevention and tional activities will be implemented this year to fur-
treatment, conducted a system- wide continuing ed- ther engage tbe patient in care, an activity that is botb
ucation initiative (witb subsequent new curricula for dependent upon and supportive of a culture of safety.
educating nursing staff on new protocols), and stan- Significant progress has also been made in tbe es-
dardized products used in tbese clinical activities. tablishment of standardized mechanisms for report-
Annual prevalence studies continue to demonstrate ing and analyzing adverse events across all system
improved identification of Stage 1 ulcers, witb de- hospitals; the systemwide use of MedMARx, annual
creased progression to more advanced stages. Tho pressure ulcer prevalence studies, and the implemen-
Event Reporting team's goal is to implement an online tation of a standard event-reporting system all sup-
reporting system for CCHS. A committee of risk man- port better reporting and analysis of, and learning
agers and quality managers selected wbieb events to from, various adverse events.
report, definitions of terms, and a database; format. Communication with employees and medical staff
All CCHS hospitals are collecting standardized data. bas been heightened through printed material, dis-
at least in hard copy form. In the sbort term, event cussion at existing committees (systemwide. re-
data are entered into a Microsoft Access database ap- gional, and bospital), and the Intranet. The first an-
plication and submitted to Iht; QI. Tbe QI aggregates nual patient safety awareness week was held in 2002,
data for various teams and managers' review and wbich included activities at each hospital and con-
considered action. In tbe long term, an online sys- tinuing education initiatives. Communication with
tem is planned for tbe entire CCHS. patients is ongoing. The videotaped message to en-
courage patient and family partir:ipation in care de-
Measures of effectiveness of patient scribed above wa.s initially piloted on 2 adult medical
safety initiative surgical units in 2002, witb subsequent implemen-
Tbe CCHS patient safety initiative's effectiveness tation into standard operating procedure at CCHS
will be demonstrated by hospitals.
• Reduction in measured key adverse events in- Tbe 3 strategies associated with change (focused
cluding falls witb injuries, adverse drug events. redesign, application of technology, and education)88 QLIALITV MANAGEMENT LN HEALTH CARE/VOLUME 14, ISSUE 2. APRII-JUNE 2005
Table 1
CCHS ACTIVITIES UNDERWAY FOR EACH STRATEGY*
Stratagyl—Promotion of a culture of safety
Executive leadership support for CCHS. regional and hospital safety plans
Itientifiration of designatRti pationt safety offic:er at oach hospital
Nonpiinitivn policy in place at ail lorations
Employee survey regarding safely culture conducted at all locations at least once
Statement to the public by former CEO (Attachment 5)
Strategy 2—Increased reporting of adverse events and error-prone processes
Standardized reporting of adverse events—all CCHS hospitals {Attachment 6)
Common definitions of events
Common data elements
Reporting tools
Medication errors using MedMarx
Device failure using MedSun—FDA project. CCHS was the first health system in Iliis project
Specimen handling is.sues roported by laboratory personnel
Wrong site surgery monitoring reported by OR personnel
Analysis and reporting—data sent to tbe QI for aggregation and reporting at health-system level monthly and quarterly
Questions added to patient experience survey regarding safety
Annual pressure ulcer prevalence study conducted since 2001 across all CCHS hospitals
Strategy 3—Enhanced communication between health core professionals and patients about patient saftely issues and
solutions
Sharing of events and safe practice strategies at CCHS team meetings
Proactive focus on 3 high-risk areas identified by the CCHS Medical Operations Council
Engaging patient/family/pubiic: inpatient admission videotaped message from eac:h hospital's executive team members
Newsletter articles
Creation of CCHS Intrannt site focused on patient safety, with links to nil hospitals' sites
Conducted annual educational events since 2001. with external keynote speakers
Tracking of exlernal priorities, with communication and action as indicated
Service alerts from patients, prompting response and action as indicated
Summary reports about reported events disseminated to CCHS Patient Safety team
Strategy -1 —Increased learning from analysis of reported adverse events and communication
Identification of:
High-risk areas
Need for standard order sets—insulin and heparin drips
New skin care protocols and produi:ts
Need to improve compliance with national patient safety goals
Educational needs
Patient identification issues
Need to improve reporting of equipment failures
Need to re-educate abuut event reporting
Reaffirmed need to improve link between quality and risk management
Strategy 5 — Focused process redesignnhpn and nhere indicated
Developed algorithm for chemotherapy administration
Evaluated patient identification products
Redesigned process nnd forms for ensuring cnrrnct surgical site/patient/procedure/location
Redcsignnd process for giving/receiving verbal orders
Implenientod "unauthorized abbrnviations" list
Improved clinical alarm monitoring
Ongoing evaluation of relationship between nusocomial infections and mortality
Implementation of one phone numbnr for all of CCHS to rnport device-related events
[continues]Cleveland Clinic Health System 89
Table 1
CCHS ACTIVITIES UNDERWAY FOR EACH STRATEGY* (continued)
Strategy 6 —Promntinn of the appropriate application of technologv
Electronic medical reccjrd implemented in filtn'elajid Clinic ambulatory settings (2.5 miliion visits annually); launched
inipleni(!ntHlian of inpatient correlntn in 2004
Inpatient electronic medical record implementation has commenced in 4 of the 8 CCHS comnuiiiity hospitals
Evaluating use of barcoding for medication use, blood products, and specimen labeling
Active review of now |)atient identification products, with a CCHS and local teams at hospitals
Innovative usn of educ;ati()n channels on hospital TV networks to teach patients about safety and about being
participants in tbeir care
Elimination of free-flow pumps
Strategy 7— Focused education ahout new safety enhancement activities
All CCHS hospitals include patient safety content in new employee orientation
Annual continuing education programs (described above under Strategy 3)
Targeted in-.service.s
Intravenous pump use
Skin care
Abbreviations
Standard order protocols
•CCHS indicates ClevHiand Clijiii: Health Systems.
aro being mnt through spetufic projects, as mentioned 3. Instilute of Medicine. To Err Is Humnn. Washington, DC: Na-
above (medication, skin caro). as well as through clin- tional Academy Press; 2000.
4. Cook Rl, WcKjds DO. Operating til ihe sh.irp end: tbe com-
ical teams' review of the literature and external orga- plexity of hunijn error. In: Bo^ner MS, f d . Human Error in
nizations' activities (eg, Joint Commission on Accred- Medicine. Hillside, NI: Elbaum;1994:255-310.
itatinn of Healthciue Organizations. National Quality 5. Reason |T. Understanding adverseevents: human factors. Qujl
Healthcare. 199.S:4(2):fiO-89.
Forum, Centers for Medirart! and Medic:ai(l Services,
b. Makinj; the Business Case lor Patient Safely: A Symposium for
Centers for Disease Control and Prevention). Healrh care CEOs. Septemt>er 26-27, 2002;
The CCHS's patient safety initiative has been suc- 7. Washington, DC. Sprmsored by Ihe Agency for Healthcare
cessfully lannrhed. with each hospital actively par- Research and equality. Joint Commission on Accredilalion of
Healthcare Organizalions, Cenlcrs for Medicaid and Medi-
ticipating in initiative-defiued strategies. Together, care Services. 7. Gershon RR. Karkashian CD, Grosch |W,
the CCHS hospitals, clinicians, employees, and pa- et al. Hospital safety climate and its relationship with safe work
tients continue to emphasize expectations of vigi- practices and workplact' exposure incidents. Am I Inlec Con-
trot. 2OOO;28:211-221.
lance and the provision of safe, effective, high-quality
8. Diaz Rl, Clarera DO. Safely climate and atlitude as evaluation
care throughout the system. measures of organizational safety. Accid Anal Prev.
1997;9(5):643-650.
9. Zoha D. Safety climate in industrial organizations: fheorelical
and applied implications, i Appl Psychot. 1980;6.5:9(>~in2.
REFERENCES 10. Instilute of Medicint". Crossing the Quality Chasm. Washing-
ton, DC: National Academy Press; 2002.
DM, VVctH[.;90 QUALITY MANAGEMENT IN HEALTH CARE/VOLUME 14, ISSUE 2, ApKiL-JuNt; 2005
14. GuaddKnoIr E, Ward P. Patient participation in decision- 21. Nolan TW. System changes to improve patient safety. BM).
making. SocSciMed. 1998;47(3):329-339. 2O02;320:771-773.
15. Korsch BM. Gozzi EK, Francis V. Gaps in doctor-patient com- 22. Berwick DM. A user's manual for the lOM's "Quality Chasm"
munication. Pediatrics. 19f.8;42(5):855. report. Health All 2002:21(31:80-90.
16. Coulter A. After Bristol: pulting patients at the centre. BMJ. 23. Reason |T, Carlhers I, deLeval MR. Diagnosing vulnerable
2002;324(7338):648-651. systems syndrome: an essential prerequisite to reflective risk
17. Roter DL. PatienI particip.ition in the patient-provider inter- management. Qual Health Care. 2001 .lOisuppI 2):ii 2 1 -
action: the effects of palieni (^ueslion asking on the quality of ii2.S.
interaction, satisfaction and compliance. Health EducMonof-r. 24. Report of the QUIC lo the President.Doing What Counts for
1977:5(41:281-315. Patient Safety: Federal Actions to Reduce Medical Errors and
18. lohnson GL, Ramaprasad A. Patient-physician relationships in Their Impact. Quality tnteragency Coordination Task Force.
the information age. Mjrk Health Ser^. 2OOO;2n(l):2a-27. Rockville, Md: Agency tor Healthcare Research and Quality;
19. Emanuel E), Emanuel LL- Four models of the physician-patient February 21, 1999.
relationship. lAMA. 1992,267:2221-2226. 25. National Coordinating Council on Medication Error Report-
20. Jewell SE. Patient participation: what does it mean to nurses? ing and Prevention. About medication errors. Available at:
iAdvNurs. 1994;19:433^38. httpy/www.nccmerp.org/. Accessed lune 2002.You can also read