Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of Attention-Deficit/Hyperactivity Disorder in Children and Adolescents
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL PRACTICE GUIDELINE
Clinical Practice Guideline for the
Diagnosis, Evaluation, and Treatment of
Attention-Deficit/Hyperactivity
Disorder in Children and Adolescents
Mark L. Wolraich, MD, FAAP,a Joseph F. Hagan, Jr, MD, FAAP,b,c Carla Allan, PhD,d,e Eugenia Chan, MD, MPH, FAAP,f,g
Dale Davison, MSpEd, PCC,h,i Marian Earls, MD, MTS, FAAP,j,k Steven W. Evans, PhD,l,m Susan K. Flinn, MA,n
Tanya Froehlich, MD, MS, FAAP,o,p Jennifer Frost, MD, FAAFP,q,r Joseph R. Holbrook, PhD, MPH,s
Christoph Ulrich Lehmann, MD, FAAP,t Herschel Robert Lessin, MD, FAAP,u Kymika Okechukwu, MPA,v
Karen L. Pierce, MD, DFAACAP,w,x Jonathan D. Winner, MD, FAAP,y William Zurhellen, MD, FAAP,z SUBCOMMITTEE ON CHILDREN AND
ADOLESCENTS WITH ATTENTION-DEFICIT/HYPERACTIVE DISORDER
Attention-deficit/hyperactivity disorder (ADHD) is one of the most common abstract
neurobehavioral disorders of childhood and can profoundly affect children’s a
Section of Developmental and Behavioral Pediatrics, University of
academic achievement, well-being, and social interactions. The American Academy Oklahoma, Oklahoma City, Oklahoma; bDepartment of Pediatrics, The
of Pediatrics first published clinical recommendations for evaluation and Robert Larner, MD, College of Medicine, The University of Vermont,
Burlington, Vermont; cHagan, Rinehart, and Connolly Pediatricians,
diagnosis of pediatric ADHD in 2000; recommendations for treatment followed PLLC, Burlington, Vermont; dDivision of Developmental and Behavioral
in 2001. The guidelines were revised in 2011 and published with an accompanying Health, Department of Pediatrics, Children’s Mercy Kansas City, Kansas
City, Missouri; eSchool of Medicine, University of Missouri-Kansas City,
process of care algorithm (PoCA) providing discrete and manageable steps by Kansas City, Missouri; fDivision of Developmental Medicine, Boston
which clinicians could fulfill the clinical guideline’s recommendations. Since the Children’s Hospital, Boston, Massachusetts; gHarvard Medical School,
Harvard University, Boston, Massachusetts; hChildren and Adults with
release of the 2011 guideline, the Diagnostic and Statistical Manual of Mental Attention-Deficit/Hyperactivity Disorder, Lanham, Maryland; iDale
Disorders has been revised to the fifth edition, and new ADHD-related research Davison, LLC, Skokie, Illinois; jCommunity Care of North Carolina,
has been published. These publications do not support dramatic changes to Raleigh, North Carolina; kSchool of Medicine, University of North
Carolina, Chapel Hill, North Carolina; lDepartment of Psychology, Ohio
the previous recommendations. Therefore, only incremental updates have been University, Athens, Ohio; mCenter for Intervention Research in Schools,
made in this guideline revision, including the addition of a key action statement Ohio University, Athens, Ohio; nAmerican Academy of Pediatrics,
Alexandria, Virginia; oDepartment of Pediatrics, University of
related to diagnosis and treatment of comorbid conditions in children and Cincinnati, Cincinnati, Ohio; pCincinnati Children’s Hospital Medical
adolescents with ADHD. The accompanying process of care algorithm has also Center, Cincinnati, Ohio; qSwope Health Services, Kansas City, Kansas;
r
American Academy of Family Physicians, Leawood, Kansas; sNational
been updated to assist in implementing the guideline recommendations. Center on Birth Defects and Developmental Disabilities, Centers for
Throughout the process of revising the guideline and algorithm, numerous Disease Control and Prevention, Atlanta, Georgia; tDepartments of
Biomedical Informatics and Pediatrics, Vanderbilt University, Nashville,
systemic barriers were identified that restrict and/or hamper pediatric clinicians’ Tennessee; uThe Children’s Medical Group, Poughkeepsie, New York;
ability to adopt their recommendations. Therefore, the subcommittee created
a companion article (available in the Supplemental Information) on systemic
To cite: Wolraich ML, Hagan JF, Allan C, et al. AAP
barriers to the care of children and adolescents with ADHD, which identifies the
SUBCOMMITTEE ON CHILDREN AND ADOLESCENTS WITH
major systemic-level barriers and presents recommendations to address those ATTENTION-DEFICIT/HYPERACTIVE DISORDER. Clinical Practice
barriers; in this article, we support the recommendations of the clinical practice Guideline for the Diagnosis, Evaluation, and Treatment of
guideline and accompanying process of care algorithm. Attention-Deficit/Hyperactivity Disorder in Children and
Adolescents. Pediatrics. 2019;144(4):e20192528
Downloaded from www.aappublications.org/news by guest on October 25, 2021
PEDIATRICS Volume 144, number 4, October 2019:e20192528 FROM THE AMERICAN ACADEMY OF PEDIATRICSINTRODUCTION implementation of such a resource. In care to the patient and his or her
This article updates and replaces the response, this guideline is supported family. There is some evidence that
2011 clinical practice guideline by 2 accompanying documents, African American and Latino children
revision published by the American available in the Supplemental are less likely to have ADHD
Academy of Pediatrics (AAP), “Clinical Information: (1) a process of care diagnosed and are less likely to be
Practice Guideline: Diagnosis and algorithm (PoCA) for the diagnosis treated for ADHD. Special attention
Evaluation of the Child with and treatment of children and should be given to these populations
Attention-Deficit/Hyperactivity adolescents with ADHD and (2) an when assessing comorbidities as they
Disorder.”1 This guideline, like the article on systemic barriers to the relate to ADHD and when treating for
previous document, addresses the care of children and adolescents with ADHD symptoms.3 Given the
evaluation, diagnosis, and treatment ADHD. These supplemental nationwide problem of limited access
of attention-deficit/hyperactivity documents are designed to aid PCCs to mental health clinicians,4
disorder (ADHD) in children from age in implementing the formal pediatricians and other PCCs are
4 years to their 18th birthday, with recommendations for the evaluation, increasingly called on to provide
special guidance provided for ADHD diagnosis, and treatment of children services to patients with ADHD and to
care for preschool-aged children and and adolescents with ADHD. Although their families. In addition, the AAP
adolescents. (Note that for the this document is specific to children holds that primary care pediatricians
purposes of this document, and adolescents in the United States should be prepared to diagnose and
“preschool-aged” refers to children in some of its recommendations, manage mild-to-moderate ADHD,
from age 4 years to the sixth international stakeholders can modify anxiety, depression, and problematic
birthday.) Pediatricians and other specific content (ie, educational laws substance use, as well as co-manage
primary care clinicians (PCCs) may about accommodations, etc) as patients who have more severe
continue to provide care after needed. (Prevention is addressed in conditions with mental health
18 years of age, but care beyond this the Mental Health Task Force professionals. Unfortunately, third-
age was not studied for this guideline. recommendations.2) party payers seldom pay
appropriately for these time-
Since 2011, much research has PoCA for the Diagnosis and consuming services.5,6
Treatment of Children and
occurred, and the Diagnostic and
Adolescents With ADHD To assist pediatricians and other
Statistical Manual of Mental Disorders,
In this revised guideline and PCCs in overcoming such obstacles,
Fifth Edition (DSM-5), has been
accompanying PoCA, we recognize the companion article on systemic
released. The new research and DSM-
that evaluation, diagnosis, and barriers to the care of children and
5 do not, however, support dramatic
treatment are a continuous process. adolescents with ADHD reviews the
changes to the previous
The PoCA provides recommendations barriers and makes recommendations
recommendations. Hence, this new
for implementing the guideline steps, to address them to enhance care for
guideline includes only incremental
although there is less evidence for the children and adolescents with ADHD.
updates to the previous guideline.
One such update is the addition of PoCA than for the guidelines. The
a key action statement (KAS) about section on evaluating and treating
comorbidities has also been expanded ADHD EPIDEMIOLOGY AND SCOPE
the diagnosis and treatment of
coexisting or comorbid conditions in in the PoCA document. Prevalence estimates of ADHD vary
children and adolescents with ADHD. on the basis of differences in research
Systems Barriers to the Care of methodologies, the various age
The subcommittee uses the term
Children and Adolescents With ADHD
“comorbid,” to be consistent with the groups being described, and changes
DSM-5. There are many system-level barriers in diagnostic criteria over time.7
that hamper the adoption of the best- Authors of a recent meta-analysis
Since 2011, the release of new practice recommendations contained calculated a pooled worldwide ADHD
research reflects an increased in the clinical practice guideline and prevalence of 7.2% among children8;
understanding and recognition of the PoCA. The procedures estimates from some community-
ADHD’s prevalence and recommended in this guideline based samples are somewhat higher,
epidemiology; the challenges it raises necessitate spending more time with at 8.7% to 15.5%.9,10 National survey
for children and families; the need for patients and their families, data from 2016 indicate that 9.4% of
a comprehensive clinical resource for developing a care management children in the United States 2 to
the evaluation, diagnosis, and system of contacts with school and 17 years of age have ever had an
treatment of pediatric ADHD; and the other community stakeholders, and ADHD diagnosis, including 2.4% of
barriers that impede the providing continuous, coordinated children 2 to 5 years of age.11 In that
Downloaded from www.aappublications.org/news by guest on October 25, 2021
2 FROM THE AMERICAN ACADEMY OF PEDIATRICSnational survey, 8.4% of children 2 to developmentally capable of Centers of the US Agency for
17 years of age currently had ADHD, compensating for their weaknesses), Healthcare Research and Quality
representing 5.4 million children.11 for most children, retention is not (AHRQ).23 These questions assessed
Among children and adolescents with beneficial.22 4 diagnostic areas and 3 treatment
current ADHD, almost two-thirds areas on the basis of research
were taking medication, and published in 2011 through 2016.
METHODOLOGY
approximately half had received The AHRQ’s framework was guided
behavioral treatment of ADHD in the As with the original 2000 clinical
by key clinical questions addressing
past year. Nearly one quarter had practice guideline and the 2011
diagnosis as well as treatment
received neither type of treatment of revision, the AAP collaborated with
interventions for children and
ADHD.11 several organizations to form
adolescents 4 to 18 years of age.
a subcommittee on ADHD (the
Symptoms of ADHD occur in subcommittee) under the oversight of The first clinical questions pertaining
childhood, and most children with the AAP Council on Quality to ADHD diagnosis were as follows:
ADHD will continue to have Improvement and Patient Safety. 1. What is the comparative
symptoms and impairment through
The subcommittee’s membership diagnostic accuracy of approaches
adolescence and into adulthood.
included representation of a wide that can be used in the primary
According to a 2014 national survey,
range of primary care and care practice setting or by
the median age of diagnosis was
subspecialty groups, including specialists to diagnose ADHD
7 years; approximately one-third of
primary care pediatricians, among children younger than
children were diagnosed before
developmental-behavioral 7 years of age?
6 years of age.12 More than half of
these children were first diagnosed pediatricians, an epidemiologist from 2. What is the comparative
by a PCC, often a pediatrician.12 As the Centers for Disease Control and diagnostic accuracy of EEG,
individuals with ADHD enter Prevention; and representatives from imaging, or executive function
adolescence, their overt hyperactive the American Academy of Child and approaches that can be used in the
and impulsive symptoms tend to Adolescent Psychiatry, the Society for primary care practice setting or by
decline, whereas their inattentive Pediatric Psychology, the National specialists to diagnose ADHD
symptoms tend to persist.13,14 Association of School Psychologists, among individuals aged 7 to their
Learning and language problems are the Society for Developmental and 18th birthday?
common comorbid conditions with Behavioral Pediatrics (SDBP), the 3. What are the adverse effects
ADHD.15 American Academy of Family associated with being labeled
Physicians, and Children and Adults correctly or incorrectly as having
Boys are more than twice as likely as with Attention-Deficit/Hyperactivity ADHD?
girls to receive a diagnosis of Disorder (CHADD) to provide
4. Are there more formal
ADHD,9,11,16 possibly because feedback on the patient/parent
neuropsychological, imaging, or
hyperactive behaviors, which are perspective.
genetic tests that improve the
easily observable and potentially
This subcommittee met over a 3.5- diagnostic process?
disruptive, are seen more frequently
year period from 2015 to 2018 to The treatment questions were as
in boys. The majority of both boys
review practice changes and newly follows:
and girls with ADHD also meet
identified issues that have arisen
diagnostic criteria for another mental 1. What are the comparative safety
since the publication of the 2011
disorder.17,18 Boys are more likely to and effectiveness of pharmacologic
guidelines. The subcommittee
exhibit externalizing conditions like and/or nonpharmacologic
members’ potential conflicts were
oppositional defiant disorder or treatments of ADHD in improving
identified and taken into
conduct disorder.17,19,20 Recent outcomes associated with ADHD?
consideration in the group’s
research has established that girls
deliberations. No conflicts prevented 2. What is the risk of diversion of
with ADHD are more likely than boys
subcommittee member participation pharmacologic treatment?
to have a comorbid internalizing
on the guidelines. 3. What are the comparative safety
condition like anxiety or
depression.21 and effectiveness of different
Research Questions monitoring strategies to evaluate
Although there is a greater risk of The subcommittee developed a series the effectiveness of treatment or
receiving a diagnosis of ADHD for of research questions to direct an changes in ADHD status (eg,
children who are the youngest in evidence-based review sponsored by worsening or resolving
their class (who are therefore less 1 of the Evidence-based Practice symptoms)?
Downloaded from www.aappublications.org/news by guest on October 25, 2021
PEDIATRICS Volume 144, number 4, October 2019 3In addition to this review of the
research questions, the subcommittee
considered information from a review
of evidence-based psychosocial
treatments for children and
adolescents with ADHD24 (which, in
some cases, affected the evidence
grade) as well as updated information
on prevalence from the Centers for
Disease Control and Prevention.
Evidence Review
This article followed the latest
version of the evidence base update
format used to develop the previous 3
clinical practice guidelines.24–26
Under this format, studies were only
included in the review when they met
a variety of criteria designed to
ensure the research was based on
a strong methodology that yielded
confidence in its conclusions.
The level of efficacy for each
treatment was defined on the basis of
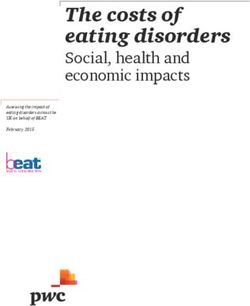
child-focused outcomes related to FIGURE 1
AAP rating of evidence and recommendations.
both symptoms and impairment.
Hence, improvements in behaviors on
the part of parents or teachers, such
sites/default/files/pdf/cer-203-adhd- demonstrated a preponderance of
as the use of communication or
final_0.pdf. benefits over harms, the KAS provides
praise, were not considered in the
a “strong recommendation” or
review. Although these outcomes are The evidence is discussed in more
“recommendation.”27 Clinicians
important, they address how detail in published reports and
should follow a “strong
treatment reaches the child or articles.25
recommendation” unless a clear and
adolescent with ADHD and are,
Guideline Recommendations and Key compelling rationale for an
therefore, secondary to changes in the
Action Statements alternative approach is present;
child’s behavior. Focusing on
clinicians are prudent to follow
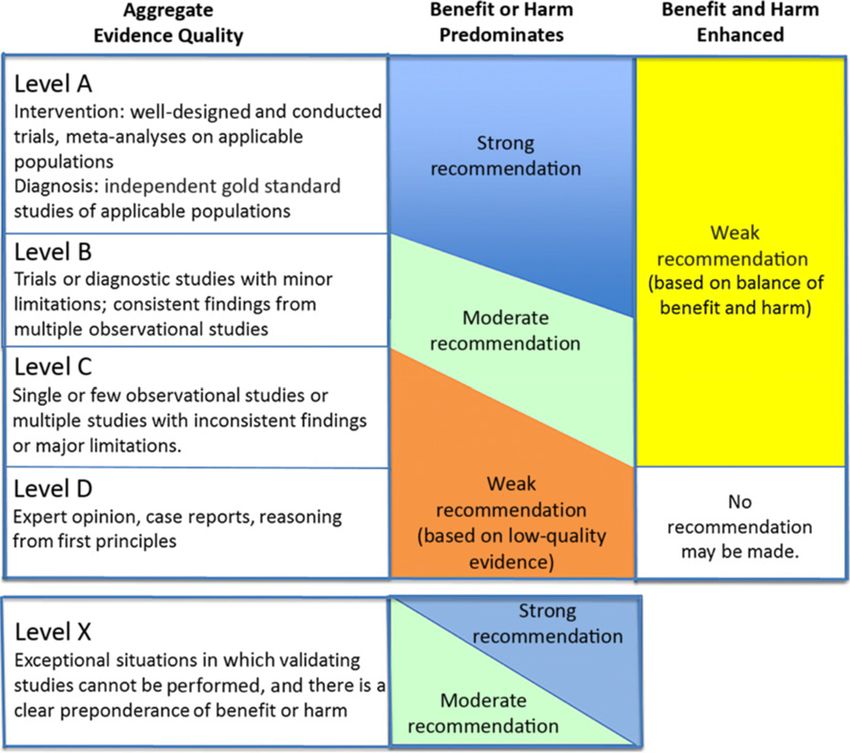
improvements in the child or The AAP policy statement, a “recommendation” but are advised
adolescent’s symptoms and “Classifying Recommendations for to remain alert to new information
impairment emphasizes the Clinical Practice Guidelines,” was and be sensitive to patient
disorder’s characteristics and followed in designating aggregate preferences27 (see Fig 1).
manifestations that affect children evidence quality levels for the
and their families. available evidence (see Fig 1).27 The When the scientific evidence
AAP policy statement is consistent comprised lower-quality or limited
The treatment-related evidence relied
with the grading recommendations data and expert consensus or high-
on a recent review of literature from
advanced by the University of quality evidence with a balance
2011 through 2016 by the AHRQ of
Oxford Centre for Evidence Based between benefits and harms, the KAS
citations from Medline, Embase,
Medicine. provides an “option” level of
PsycINFO, and the Cochrane Database
recommendation. Options are clinical
of Systematic Reviews. The subcommittee reached consensus
interventions that a reasonable
on the evidence, which was then used
The original methodology and report, health care provider might or might
to develop the clinical practice
including the evidence search and not wish to implement in the
guideline’s KASs.
review, are available in their entirety practice.27 Where the evidence
and as an executive summary at When the scientific evidence was at was lacking, a combination of
https://effectivehealthcare.ahrq.gov/ least “good” in quality and evidence and expert consensus
Downloaded from www.aappublications.org/news by guest on October 25, 2021
4 FROM THE AMERICAN ACADEMY OF PEDIATRICSwould be used, although this These KASs provide for consistent (Table 2). (Grade B: strong
did not occur in these and high-quality care for children and recommendation.)
guidelines, and all KASs adolescents who may have symptoms
achieved a “strong suggesting attention disorders or The basis for this recommendation is
recommendation” level except problems as well as for their families. essentially unchanged from the
for KAS 7, on comorbidities, In developing the 7 KASs, the previous guideline. As noted, ADHD is
which received a recommendation subcommittee considered the the most common neurobehavioral
level (see Fig 1). requirements for establishing the disorder of childhood, occurring in
diagnosis; the prevalence of ADHD; approximately 7% to 8% of children
As shown in Fig 1, integrating the effect of untreated ADHD; the and youth.8,18,28,29 Hence, the number
evidence quality appraisal with an efficacy and adverse effects of of children with this condition is far
assessment of the anticipated balance treatment; various long-term greater than can be managed by the
between benefits and harms leads to outcomes; the importance of mental health system.4 There is
a designation of a strong coordination between pediatric and evidence that appropriate diagnosis
recommendation, recommendation, mental health service providers; the can be accomplished in the primary
option, or no recommendation. value of the medical home; and the care setting for children and
common occurrence of comorbid adolescents.30,31 Note that there is
Once the evidence level was conditions, the importance of insufficient evidence to recommend
determined, an evidence grade was addressing them, and the effects of diagnosis or treatment for children
assigned. AAP policy stipulates that not treating them. younger than 4 years (other than
the evidence supporting each KAS be parent training in behavior
prospectively identified, appraised, The subcommittee members with the management [PTBM], which does not
and summarized, and an explicit link most epidemiological experience require a diagnosis to be applied); in
between quality levels and the grade assessed the strength of each instances in which ADHD-like
of recommendation must be defined. recommendation and the quality of symptoms in children younger than
Possible grades of recommendations evidence supporting each draft KAS. 4 years bring substantial impairment,
range from “A” to “D,” with “A” being PCCs can consider making a referral
the highest: Peer Review for PTBM.
• grade A: consistent level A studies; The guidelines and PoCA underwent
• grade B: consistent level B or extensive peer review by more than KAS 2
extrapolations from level A studies; 30 internal stakeholders (eg, AAP
To make a diagnosis of ADHD, the
• grade C: level C studies or committees, sections, councils, and
PCC should determine that DSM-5
extrapolations from level B or level task forces) and external stakeholder
criteria have been met, including
C studies; groups identified by the
documentation of symptoms and
subcommittee. The resulting
• grade D: level D evidence or impairment in more than 1 major
comments were compiled and
troublingly inconsistent or setting (ie, social, academic, or
reviewed by the chair and vice chair;
inconclusive studies of any level; occupational), with information
relevant changes were incorporated
and obtained primarily from reports from
into the draft, which was then
• level X: not an explicit level of reviewed by the full subcommittee.
parents or guardians, teachers, other
evidence as outlined by the Centre school personnel, and mental health
for Evidence-Based Medicine. This clinicians who are involved in the
level is reserved for interventions KASS FOR THE EVALUATION, child or adolescent’s care. The PCC
that are unethical or impossible to DIAGNOSIS, TREATMENT, AND should also rule out any alternative
test in a controlled or scientific MONITORING OF CHILDREN AND cause (Table 3). (Grade B: strong
fashion and for which the ADOLESCENTS WITH ADHD recommendation.)
preponderance of benefit or harm
KAS 1 The American Psychiatric Association
is overwhelming, precluding
rigorous investigation. The pediatrician or other PCC should developed the DSM-5 using expert
initiate an evaluation for ADHD for consensus and an expanding research
Guided by the evidence quality and any child or adolescent age 4 years to foundation.32 The DSM-5 system is
grade, the subcommittee developed 7 the 18th birthday who presents with used by professionals in psychiatry,
KASs for the evaluation, diagnosis, academic or behavioral problems and psychology, health care systems, and
and treatment of ADHD in children symptoms of inattention, primary care; it is also well
and adolescents (see Table 1). hyperactivity, or impulsivity established with third-party payers.
Downloaded from www.aappublications.org/news by guest on October 25, 2021
PEDIATRICS Volume 144, number 4, October 2019 5TABLE 1 Summary of KASs for Diagnosing, Evaluating, and Treating ADHD in Children and Adolescents
KASs Evidence Quality, Strength of Recommendation
KAS 1: The pediatrician or other PCC should initiate an evaluation for ADHD for any child or Grade B, strong recommendation
adolescent age 4 years to the 18th birthday who presents with academic or behavioral
problems and symptoms of inattention, hyperactivity, or impulsivity.
KAS 2: To make a diagnosis of ADHD, the PCC should determine that DSM-5 criteria have been Grade B, strong recommendation
met, including documentation of symptoms and impairment in more than 1 major setting
(ie, social, academic, or occupational), with information obtained primarily from reports
from parents or guardians, teachers, other school personnel, and mental health
clinicians who are involved in the child or adolescent’s care. The PCC should also rule out
any alternative cause.
KAS 3: In the evaluation of a child or adolescent for ADHD, the PCC should include a process Grade B, strong recommendation
to at least screen for comorbid conditions, including emotional or behavioral conditions
(eg, anxiety, depression, oppositional defiant disorder, conduct disorders, substance use),
developmental conditions (eg, learning and language disorders, autism spectrum
disorders), and physical conditions (eg, tics, sleep apnea).
KAS 4: ADHD is a chronic condition; therefore, the PCC should manage children and Grade B, strong recommendation
adolescents with ADHD in the same manner that they would children and youth with
special health care needs, following the principles of the chronic care model and the
medical home.
KAS 5a: For preschool-aged children (age 4 years to the sixth birthday) with ADHD, the PCC Grade A, strong recommendation for PTBM
should prescribe evidence-based PTBM and/or behavioral classroom interventions as the
first line of treatment, if available.
Methylphenidate may be considered if these behavioral interventions do not provide Grade B, strong recommendation for methylphenidate
significant improvement and there is moderate-to-severe continued disturbance in the
4- through 5-year-old child’s functioning. In areas in which evidence-based behavioral
treatments are not available, the clinician needs to weigh the risks of starting
medication before the age of 6 years against the harm of delaying treatment.
KAS 5b. For elementary and middle school-aged children (age 6 years to the 12th birthday) Grade A, strong recommendation for medications
with ADHD, the PCC should prescribe FDA-approved medications for ADHD, along with Grade A, strong recommendation for training and behavioral
PTBM and/or behavioral classroom intervention (preferably both PTBM and behavioral treatments for ADHD with family and school
classroom interventions). Educational interventions and individualized instructional
supports, including school environment, class placement, instructional placement, and
behavioral supports, are a necessary part of any treatment plan and often include an IEP
or a rehabilitation plan (504 plan).
KAS 5c. For adolescents (age 12 years to the 18th birthday) with ADHD, the PCC should Grade A, strong recommendation for medications
prescribe FDA-approved medications for ADHD with the adolescent’s assent. The PCC is Grade A, strong recommendation for training and behavioral
encouraged to prescribe evidence-based training interventions and/or behavioral treatments for ADHD with the family and school
interventions as treatment of ADHD, if available. Educational interventions and
individualized instructional supports, including school environment, class placement,
instructional placement, and behavioral supports, are a necessary part of any treatment
plan and often include an IEP or a rehabilitation plan (504 plan).
KAS 6. The PCC should titrate doses of medication for ADHD to achieve maximum benefit with Grade B, strong recommendation
tolerable side effects.
KAS 7. The PCC, if trained or experienced in diagnosing comorbid conditions, may initiate Grade C, recommendation
treatment of such conditions or make a referral to an appropriate subspecialist for
treatment. After detecting possible comorbid conditions, if the PCC is not trained or
experienced in making the diagnosis or initiating treatment, the patient should be
referred to an appropriate subspecialist to make the diagnosis and initiate treatment.
The DSM-5 criteria define 4 3. attention-deficit/hyperactivity standard most frequently used by
dimensions of ADHD: disorder combined presentation clinicians and researchers to render
1. attention-deficit/hyperactivity (ADHD/C) (314.01 [F90.2]); and the diagnosis and document its
disorder primarily of the 4. ADHD other specified and appropriateness for a given child.
inattentive presentation (ADHD/I) unspecified ADHD (314.01 The use of neuropsychological
(314.00 [F90.0]); [F90.8]). testing has not been found to
2. attention-deficit/hyperactivity As with the previous guideline improve diagnostic accuracy in
disorder primarily of the recommendations, the DSM-5 most cases, although it may have
hyperactive-impulsive classification criteria are based on benefit in clarifying the child
presentation (ADHD/HI) (314.01 the best available evidence for or adolescent’s learning
[F90.1]); ADHD diagnosis and are the strengths and weaknesses. (See the
Downloaded from www.aappublications.org/news by guest on October 25, 2021
6 FROM THE AMERICAN ACADEMY OF PEDIATRICSTABLE 2 KAS 1: The pediatrician or other PCC should initiate an evaluation for ADHD for any child or adolescent age 4 years to the 18th birthday who
presents with academic or behavioral problems and symptoms of inattention, hyperactivity, or impulsivity. (Grade B: strong recommendation.)
Aggregate evidence Grade B
quality
Benefits ADHD goes undiagnosed in a considerable number of children and adolescents. Primary care clinicians’ more-rigorous identification
of children with these problems is likely to decrease the rate of undiagnosed and untreated ADHD in children and adolescents.
Risks, harm, cost Children and adolescents in whom ADHD is inappropriately diagnosed may be labeled inappropriately, or another condition may be
missed, and they may receive treatments that will not benefit them.
Benefit-harm The high prevalence of ADHD and limited mental health resources require primary care pediatricians and other PCCs to play
assessment a significant role in the care of patients with ADHD and assist them to receive appropriate diagnosis and treatment. Treatments
available have good evidence of efficacy, and a lack of treatment has the risk of impaired outcomes.
Intentional vagueness There are limits between what a PCC can address and what should be referred to a subspecialist because of varying degrees of skills
and comfort levels present among the former.
Role of patient Success with treatment is dependent on patient and family preference, which need to be taken into account.
preferences
Exclusions None.
Strength Strong recommendation.
Key references Wolraich et al31; Visser et al28; Thomas et al8; Egger et al30
PoCA for more information on should conduct a clinical interview children younger than 18 years (ie,
implementing this KAS.) with parents, examine and observe preschool-aged children, elementary
the child, and obtain information and middle school–aged children, and
Special Circumstances: Preschool-Aged from parents and teachers through adolescents) and are only minimally
Children (Age 4 Years to the Sixth DSM-based ADHD rating scales.40 different from the DSM-IV. Hence, if
Birthday) Normative data are available for the clinicians do not have the ADHD
DSM-5–based rating scales for ages Rating Scale-5 or the ADHD Rating
There is evidence that the diagnostic
criteria for ADHD can be applied to 5 years to the 18th birthday.41 There Scale-IV Preschool Version,42 any
preschool-aged children.33–39 A are, however, minimal changes in the other DSM-based scale can be used to
review of the literature, including the specific behaviors from the DSM-IV, provide a systematic method for
multisite study of the efficacy of on which all the other DSM-based collecting information from parents
methylphenidate in preschool-aged ADHD rating scales obtained and teachers, even in the absence of
children, found that the DSM-5 normative data. Both the ADHD normative data.
criteria could appropriately identify Rating Scale-IV and the Conners
children with ADHD.25 Rating Scale have preschool-age Pediatricians and other PCCs should
normative data based on the DSM-IV. be aware that determining the
To make a diagnosis of ADHD in The specific behaviors in the DSM-5 presence of key symptoms in this age
preschool-aged children, clinicians criteria for ADHD are the same for all group has its challenges, such as
TABLE 3 KAS 2: To make a diagnosis of ADHD, the PCC should determine that DSM-5 criteria have been met, including documentation of symptoms and
impairment in more than 1 major setting (ie, social, academic, or occupational), with information obtained primarily from reports from parents
or guardians, teachers, other school personnel, and mental health clinicians who are involved in the child or adolescent’s care. The PCC should
also rule out any alternative cause. (Grade B: strong recommendation.)
Aggregate evidence Grade B
quality
Benefits Use of the DSM-5 criteria has led to more uniform categorization of the condition across professional disciplines. The criteria are
essentially unchanged from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV), for children up to
their 18th birthday, except that DSM-IV required onset prior to age 7 for a diagnosis, while DSM-5 requires onset prior to age 12.
Risks, harm, cost The DSM-5 does not specifically state that symptoms must be beyond expected levels for developmental (rather than chronologic) age
to qualify for an ADHD diagnosis, which may lead to some misdiagnoses in children with developmental disorders.
Benefit-harm The benefits far outweigh the harm.
assessment
Intentional vagueness None.
Role of patient Although there is some stigma associated with mental disorder diagnoses, resulting in some families preferring other diagnoses, the
preferences need for better clarity in diagnoses outweighs this preference.
Exclusions None.
Strength Strong recommendation.
Key references Evans et al25; McGoey et al42; Young43; Sibley et al46
Downloaded from www.aappublications.org/news by guest on October 25, 2021
PEDIATRICS Volume 144, number 4, October 2019 7observing symptoms across multiple many adolescents have multiple be aware that adolescents are at
settings as required by the DSM-5, teachers. Likewise, an adolescent’s greater risk for substance use than
particularly among children who do parents may have less opportunity to are younger children.44,45,47 Certain
not attend a preschool or child care observe their child’s behaviors than substances, such as marijuana, can
program. Here, too, focused checklists they did when the child was younger. have effects that mimic ADHD;
can be used to aid in the diagnostic Furthermore, some problems adolescent patients may also attempt
evaluation. experienced by children with ADHD to obtain stimulant medication to
are less obvious in adolescents than enhance performance (ie, academic,
PTBM is the recommended primary
in younger children because athletic, etc) by feigning symptoms.48
intervention for preschool-aged
adolescents are less likely to exhibit
children with ADHD as well as Trauma experiences, posttraumatic
overt hyperactive behavior. Of note,
children with ADHD-like behaviors stress disorder, and toxic stress are
adolescents’ reports of their own
whose diagnosis is not yet verified. additional comorbidities and risk
behaviors often differ from other
This type of training helps parents factors of concern.
observers because they tend to
learn age-appropriate developmental
minimize their own problematic
expectations, behaviors that
behaviors.43–45 Special Circumstances: Inattention or
strengthen the parent-child
Hyperactivity/Impulsivity (Problem
relationship, and specific Despite these difficulties, clinicians Level)
management skills for problem need to try to obtain information
behaviors. Clinicians do not need to from at least 2 teachers or other Teachers, parents, and child health
have made an ADHD diagnosis before sources, such as coaches, school professionals typically encounter
recommending PTBM because PTBM guidance counselors, or leaders of children who demonstrate behaviors
has documented effectiveness with community activities in which the relating to activity level, impulsivity,
a wide variety of problem behaviors, adolescent participates.46 For the and inattention but who do not fully
regardless of etiology. In addition, the evaluation to be successful, it is meet DSM-5 criteria. When assessing
intervention’s results may inform the essential that adolescents agree with these children, diagnostic criteria
subsequent diagnostic evaluation. and participate in the evaluation. should be closely reviewed, which
Clinicians are encouraged to Variability in ratings is to be may require obtaining more
recommend that parents complete expected because adolescents’ information from other settings and
PTBM, if available, before assigning behavior often varies between sources. Also consider that these
an ADHD diagnosis. different classrooms and with symptoms may suggest other
different teachers. Identifying problems that mimic ADHD.
After behavioral parent training is
implemented, the clinician can reasons for any variability can Behavioral interventions, such
obtain information from parents and provide valuable clinical insight into as PTBM, are often beneficial for
teachers through DSM-5–based the adolescent’s problems. children with hyperactive/impulsive
ADHD rating scales. The clinician behaviors who do not meet full
Note that, unless they previously
may obtain reports about the diagnostic criteria for ADHD.
received a diagnosis, to meet DSM-5
parents’ ability to manage their As noted previously, these programs
criteria for ADHD, adolescents must
children and about the child’s core do not require a specific diagnosis
have some reported or documented
symptoms and impairments. to be beneficial to the family. The
manifestations of inattention or
Referral to an early intervention previous guideline discussed
hyperactivity/impulsivity before age
program or enrolling in a PTBM the diagnosis of problem-level
12. Therefore, clinicians must
program can help provide concerns on the basis of the
establish that an adolescent had
information about the child’s Diagnostic and Statistical Manual for
manifestations of ADHD before age
behavior in other settings or with Primary Care (DSM-PC), Child and
12 and strongly consider whether
other observers. The evaluators for
a mimicking or comorbid condition, Adolescent Version,49 and made
these programs and/or early suggestions for treatment and care.
such as substance use, depression,
childhood special education teachers The DSM-PC was published in 1995,
and/or anxiety, is present.46
may be useful observers, as well. however, and it has not been revised
In addition, the risks of mood and to be compatible with the DSM-5.
Special Circumstances: Adolescents anxiety disorders and risky sexual Therefore, the DSM-PC cannot be
(Age 12 Years to the 18th Birthday) behaviors increase during used as a definitive source for
Obtaining teacher reports for adolescence, as do the risks of diagnostic codes related to ADHD and
adolescents is often more challenging intentional self-harm and suicidal comorbid conditions, although it can
than for younger children because behaviors.31 Clinicians should also be used conceptually as a resource for
Downloaded from www.aappublications.org/news by guest on October 25, 2021
8 FROM THE AMERICAN ACADEMY OF PEDIATRICSenriching the understanding of condition will alter the treatment and the medical home (Table 5).
problem-level manifestations. of ADHD. (Grade B: strong recommendation.)
The SDBP is developing a clinical As in the 2 previous guidelines, this
KAS 3 practice guideline to support recommendation is based on the
clinicians in the diagnosis of evidence that for many individuals,
In the evaluation of a child or
treatment of “complex ADHD,” which ADHD causes symptoms and
adolescent for ADHD, the PCC should
includes ADHD with comorbid dysfunction over long periods of time,
include a process to at least screen
developmental and/or mental health even into adulthood. Available
for comorbid conditions, including
conditions.67 treatments address symptoms and
emotional or behavioral conditions
(eg, anxiety, depression, oppositional function but are usually not curative.
Special Circumstances: Adolescents Although the chronic illness model
defiant disorder, conduct disorders, (Age 12 Years to the 18th Birthday)
substance use), developmental has not been specifically studied in
conditions (eg, learning and language At a minimum, clinicians should children and adolescents with ADHD,
assess adolescent patients with newly it has been effective for other chronic
disorders, autism spectrum
diagnosed ADHD for symptoms and conditions, such as asthma.68 In
disorders), and physical conditions
signs of substance use, anxiety, addition, the medical home model has
(eg, tics, sleep apnea) (Table 4).
depression, and learning disabilities. been accepted as the preferred
(Grade B: strong recommendation.)
As noted, all 4 are common comorbid standard of care for children with
The majority of both boys and girls conditions that affect the treatment chronic conditions.69
with ADHD also meet diagnostic approach. These comorbidities make
it important for the clinician to The medical home and chronic illness
criteria for another mental approach may be particularly
disorder.17,18 A variety of other consider sequencing psychosocial and
medication treatments to maximize beneficial for parents who also have
behavioral, developmental, and ADHD themselves. These parents can
physical conditions can be comorbid the impact on areas of greatest risk
and impairment while monitoring for benefit from extra support to help
in children and adolescents who are them follow a consistent schedule for
evaluated for ADHD, including possible risks such as stimulant abuse
or suicidal ideation. medication and behavioral programs.
emotional or behavioral conditions or
a history of these problems. These Authors of longitudinal studies have
include but are not limited to learning KAS 4 found that ADHD treatments are
disabilities, language disorder, ADHD is a chronic condition; frequently not maintained over
disruptive behavior, anxiety, mood therefore, the PCC should manage time13 and impairments persist into
disorders, tic disorders, seizures, children and adolescents with ADHD adulthood.70 It is indicated in
autism spectrum disorder, in the same manner that they would prospective studies that patients with
developmental coordination disorder, children and youth with special ADHD, whether treated or not, are at
and sleep disorders.50–66 In some health care needs, following the increased risk for early death, suicide,
cases, the presence of a comorbid principles of the chronic care model and increased psychiatric
TABLE 4 KAS 3: In the evaluation of a child or adolescent for ADHD, the PCC should include a process to at least screen for comorbid conditions, including
emotional or behavioral conditions (eg, anxiety, depression, oppositional defiant disorder, conduct disorders, substance use), developmental
conditions (eg, learning and language disorders, autism spectrum disorders), and physical conditions (eg, tics, sleep apnea). (Grade B: strong
recommendation.)
Aggregate evidence Grade B
quality
Benefits Identifying comorbid conditions is important in developing the most appropriate treatment plan for the child or adolescent with
ADHD.
Risks, harm, cost The major risk is misdiagnosing the comorbid condition(s) and providing inappropriate care.
Benefit-harm There is a preponderance of benefits over harm.
assessment
Intentional vagueness None.
Role of patient None.
preferences
Exclusions None.
Strength Strong recommendation.
Key references Cuffe et al51; Pastor and Reuben52; Bieiderman et al53; Bieiderman et al54; Bieiderman et al72; Crabtree et al57; LeBourgeois et al58;
Chan115; Newcorn et al60; Sung et al61; Larson et al66; Mahajan et al65; Antshel et al64; Rothenberger and Roessner63; Froehlich et al62
Downloaded from www.aappublications.org/news by guest on October 25, 2021
PEDIATRICS Volume 144, number 4, October 2019 9TABLE 5 KAS 4: ADHD is a chronic condition; therefore, the PCC should manage children and adolescents with ADHD in the same manner that they would
children and youth with special health care needs, following the principles of the chronic care model and the medical home. (Grade B: strong
recommendation.)
Aggregate evidence quality Grade B
Benefits The recommendation describes the coordinated services that are most appropriate to manage the condition.
Risks, harm, cost Providing these services may be more costly.
Benefit-harm assessment There is a preponderance of benefits over harm.
Intentional vagueness None.
Role of patient Family preference in how these services are provided is an important consideration, because it can increase adherence.
preferences
Exclusions None
Strength Strong recommendation.
Key references Brito et al69; Biederman et al72; Scheffler et al74; Barbaresi et al75; Chang et al71; Chang et al78; Lichtenstein et al77; Harstad and
Levy80
comorbidity, particularly substance Recommendations for the Treatment 6 years against the harm of delaying
use disorders.71,72 They also have of Children and Adolescents With treatment (Table 6). (Grade B: strong
lower educational achievement than ADHD: KAS 5a, 5b, and 5c recommendation.)
those without ADHD73,74 and Recommendations vary depending on
increased rates of incarceration.75–77 the patient’s age and are presented A number of special circumstances
Treatment discontinuation also for the following age ranges: support the recommendation to
places individuals with ADHD at initiate PTBM as the first treatment
a. preschool-aged children: age of preschool-aged children (age
higher risk for catastrophic
4 years to the sixth birthday; 4 years to the sixth birthday) with
outcomes, such as motor vehicle
crashes78,79; criminality, including b. elementary and middle ADHD.25,83 Although it was limited to
drug-related crimes77 and violent school–aged children: age 6 years children who had moderate-to-
reoffending76; depression71; to the 12th birthday; and severe dysfunction, the largest
interpersonal issues80; and other c. adolescents: age 12 years to the multisite study of methylphenidate
injuries.81,82 18th birthday. use in preschool-aged children
revealed symptom improvements
The KASs are presented, followed by after PTBM alone.83 The overall
To continue providing the best care, it
information on medication, evidence for PTBM among
is important for a treating
psychosocial treatments, and special preschoolers is strong.
pediatrician or other PCC to engage in
circumstances.
bidirectional communication with
teachers and other school personnel PTBM programs for preschool-aged
as well as mental health clinicians KAS 5a children are typically group programs
involved in the child or adolescent’s For preschool-aged children (age and, although they are not always
care. This communication can be 4 years to the sixth birthday) with paid for by health insurance, they
difficult to achieve and is discussed in ADHD, the PCC should prescribe may be relatively low cost. One
both the PoCA and the section on evidence-based behavioral PTBM evidence-based PTBM, parent-child
systemic barriers to the care of and/or behavioral classroom interaction therapy, is a dyadic
children and adolescents with ADHD interventions as the first line of therapy for parent and child. The
in the Supplemental Information, as is treatment, if available (grade A: PoCA contains criteria for the
the medical home model.69 strong recommendation). clinician’s use to assess the quality of
Methylphenidate may be considered PTBM programs. If the child attends
if these behavioral interventions do preschool, behavioral classroom
Special Circumstances: Inattention not provide significant improvement interventions are also recommended.
or Hyperactivity/Impulsivity and there is moderate-to-severe In addition, preschool programs (such
(Problem Level) continued disturbance in the 4- as Head Start) and ADHD-focused
Children with inattention or through 5-year-old child’s organizations (such as CHADD84) can
hyperactivity/impulsivity at the functioning. In areas in which also provide behavioral supports. The
problem level, as well as their evidence-based behavioral issues related to referral, payment,
families, may also benefit from the treatments are not available, the and communication are discussed in
chronic illness and medical home clinician needs to weigh the risks of the section on systemic barriers in
principles. starting medication before the age of the Supplemental Information.
Downloaded from www.aappublications.org/news by guest on October 25, 2021
10 FROM THE AMERICAN ACADEMY OF PEDIATRICSTABLE 6 KAS 5a: For preschool-aged children (age 4 years to the sixth birthday) with ADHD, the PCC should prescribe evidence-based behavioral PTBM
and/or behavioral classroom interventions as the first line of treatment, if available (grade A: strong recommendation). Methylphenidate may be
considered if these behavioral interventions do not provide significant improvement and there is moderate-to-severe continued disturbance in
the 4- through 5-year-old child’s functioning. In areas in which evidence-based behavioral treatments are not available, the clinician needs to
weigh the risks of starting medication before the age of 6 years against the harm of delaying treatment (grade B: strong recommendation).
Aggregate evidence Grade A for PTBM; Grade B for methylphenidate
quality
Benefits Given the risks of untreated ADHD, the benefits outweigh the risks.
Risks, harm, cost Both therapies increase the cost of care; PTBM requires a high level of family involvement, whereas methylphenidate has some
potential adverse effects.
Benefit-harm Both PTBM and methylphenidate have relatively low risks; initiating treatment at an early age, before children experience repeated
assessment failure, has additional benefits. Thus, the benefits outweigh the risks.
Intentional vagueness None.
Role of patient Family preference is essential in determining the treatment plan.
preferences
Exclusions None.
Strength Strong recommendation.
Key references Greenhill et al83; Evans et al25
In areas in which evidence-based The evidence is particularly strong for it is best to introduce components at
behavioral treatments are not stimulant medications; it is sufficient, the start of high school, at about
available, the clinician needs to but not as strong, for atomoxetine, 14 years of age, and specifically focus
weigh the risks of starting extended-release guanfacine, and during the 2 years preceding high
methylphenidate before the age extended-release clonidine, in that school completion.
of 6 years against the harm of order (see the Treatment section, and
delaying diagnosis and treatment. see the PoCA for more information on Psychosocial Treatments
Other stimulant or nonstimulant implementation). Some psychosocial treatments for
medications have not been children and adolescents with ADHD
adequately studied in children in KAS 5c have been demonstrated to be
this age group with ADHD. For adolescents (age 12 years to the effective for the treatment of ADHD,
18th birthday) with ADHD, the PCC including behavioral therapy and
KAS 5b should prescribe FDA-approved training interventions.24–26,85 The
For elementary and middle medications for ADHD with the diversity of interventions and
school–aged children (age 6 years to adolescent’s assent (grade A: strong outcome measures makes it
the 12th birthday) with ADHD, the recommendation). The PCC is challenging to assess a meta-analysis
PCC should prescribe US Food and encouraged to prescribe evidence- of psychosocial treatment’s effects
Drug Administration (FDA)–approved based training interventions and/or alone or in association with
medications for ADHD, along with behavioral interventions as treatment medication treatment. As with
PTBM and/or behavioral classroom of ADHD, if available. Educational medication treatment, the long-term
intervention (preferably both PTBM interventions and individualized positive effects of psychosocial
and behavioral classroom interven- instructional supports, including treatments have yet to be determined.
tions). Educational interventions school environment, class Nonetheless, ongoing adherence
and individualized instructional placement, instructional placement, to psychosocial treatment is
supports, including school environment, and behavioral supports, are a key contributor to its beneficial
class placement, instructional a necessary part of any treatment effects, making implementation of
placement, and behavioral supports, plan and often include an IEP or a chronic care model for child health
are a necessary part of any a rehabilitation plan (504 plan) important to ensure sustained
treatment plan and often include an (Table 8). (Grade A: strong adherence.86
Individualized Education Program recommendation.) Behavioral therapy involves training
(IEP) or a rehabilitation plan (504 Transition to adult care is an adults to influence the contingencies
plan) (Table 7). (Grade A: strong important component of the chronic in an environment to improve the
recommendation for medications; care model for ADHD. Planning for behavior of a child or adolescent in
grade A: strong recommendation for the transition to adult care is an that setting. It can help parents and
PTBM training and behavioral ongoing process that may culminate school personnel learn how to
treatments for ADHD implemented after high school or, perhaps, after effectively prevent and respond to
with the family and school.) college. To foster a smooth transition, adolescent behaviors such as
Downloaded from www.aappublications.org/news by guest on October 25, 2021
PEDIATRICS Volume 144, number 4, October 2019 11TABLE 7 KAS 5b: For elementary and middle school–aged children (age 6 years to the 12th birthday) with ADHD, the PCC should prescribe US Food and
Drug Administration (FDA)–approved medications for ADHD, along with PTBM and/or behavioral classroom intervention (preferably both PTBM
and behavioral classroom interventions). Educational interventions and individualized instructional supports, including school environment,
class placement, instructional placement, and behavioral supports, are a necessary part of any treatment plan and often include an
Individualized Education Program (IEP) or a rehabilitation plan (504 plan). (Grade A: strong recommendation for medications; grade A: strong
recommendation for PTBM training and behavioral treatments for ADHD implemented with the family and school.)
Aggregate evidence Grade A for Treatment with FDA-Approved Medications; Grade A for Training and Behavioral Treatments for ADHD With the Family and
quality School.
Benefits Both behavioral therapy and FDA-approved medications have been shown to reduce behaviors associated with ADHD and to improve
function.
Risks, harm, cost Both therapies increase the cost of care. Psychosocial therapy requires a high level of family and/or school involvement and may lead
to increased family conflict, especially if treatment is not successfully completed. FDA-approved medications may have some
adverse effects and discontinuation of medication is common among adolescents.
Benefit-harm Given the risks of untreated ADHD, the benefits outweigh the risks.
assessment
Intentional vagueness None.
Role of patient Family preference, including patient preference, is essential in determining the treatment plan and enhancing adherence.
preferences
Exclusions None.
Strength Strong recommendation.
Key references Evans et al25; Barbaresi et al73; Jain et al103; Brown and Bishop104; Kambeitz et al105; Bruxel et al106; Kieling et al107; Froehlich et al108;
Joensen et al109
interrupting, aggression, not symptoms. The positive effects of setting. Less research has been
completing tasks, and not complying behavioral therapies tend to persist, conducted on training interventions
with requests. Behavioral parent and but the positive effects of medication compared to behavioral treatments;
classroom training are well- cease when medication stops. nonetheless, training interventions
established treatments with Optimal care is likely to occur when are well-established treatments to
preadolescent children.25,87,88 Most both therapies are used, but the target disorganization of materials
studies comparing behavior therapy decision about therapies is heavily and time that are exhibited by
to stimulants indicate that stimulants dependent on acceptability by, and most youth with ADHD; it is likely
have a stronger immediate effect on feasibility for, the family. that they will benefit younger
the 18 core symptoms of ADHD. Training interventions target skill children, as well.25,89 Some training
Parents, however, were more satisfied development and involve repeated interventions, including social
with the effect of behavioral therapy, practice with performance feedback skills training, have not been shown
which addresses symptoms and over time, rather than modifying to be effective for children with
functions in addition to ADHD’s core behavioral contingencies in a specific ADHD.25
TABLE 8 KAS 5c: For adolescents (age 12 years to the 18th birthday) with ADHD, the PCC should prescribe FDA-approved medications for ADHD with the
adolescent’s assent (grade A: strong recommendation). The PCC is encouraged to prescribe evidence-based training interventions and/or
behavioral interventions as treatment of ADHD, if available. Educational interventions and individualized instructional supports, including school
environment, class placement, instructional placement, and behavioral supports, are a necessary part of any treatment plan and often include
an IEP or a rehabilitation plan (504 plan). (Grade A: strong recommendation.)
Aggregate evidence Grade A for Medications; Grade A for Training and Behavioral Therapy
quality
Benefits Training interventions, behavioral therapy, and FDA-approved medications have been demonstrated to reduce behaviors associated
with ADHD and to improve function.
Risks, harm, cost Both therapies increase the cost of care. Psychosocial therapy requires a high level of family and/or school involvement and may lead
to unintended increased family conflict, especially if treatment is not successfully completed. FDA-approved medications may have
some adverse effects, and discontinuation of medication is common among adolescents.
Benefit-harm Given the risks of untreated ADHD, the benefits outweigh the risks.
assessment
Intentional vagueness None.
Role of patient Family preference, including patient preference, is likely to predict engagement and persistence with a treatment.
preferences
Exclusions None.
Strength Strong recommendation.
Key references Evans et al25; Webster-Stratton et al87; Evans et al95; Fabiano et al93; Sibley and Graziano et al94; Langberg et al96; Schultz et al97; Brown
and Bishop104; Kambeitz et al105; Bruxel et al106; Froehlich et al108; Joensen et al109
Downloaded from www.aappublications.org/news by guest on October 25, 2021
12 FROM THE AMERICAN ACADEMY OF PEDIATRICSYou can also read