Combatting Opioid Use Disorder with Medication-Assisted Therapy: Psychiatry ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Combatting Opioid Use Disorder with
Medication-Assisted Therapy:
Strategies for Success
Arwen Podesta, MD, ABPN, FASAM, ABIHM
Assistant Professor of Psychiatry, Tulane University
Medical Director, ACER LLC
Owner/Psychiatrist, Podesta Wellness
President, Louisiana Chapter of American Society of Addiction Medicine
New Orleans, Louisiana
Supported by educational grants from Alkermes, Inc. and Indivior Inc.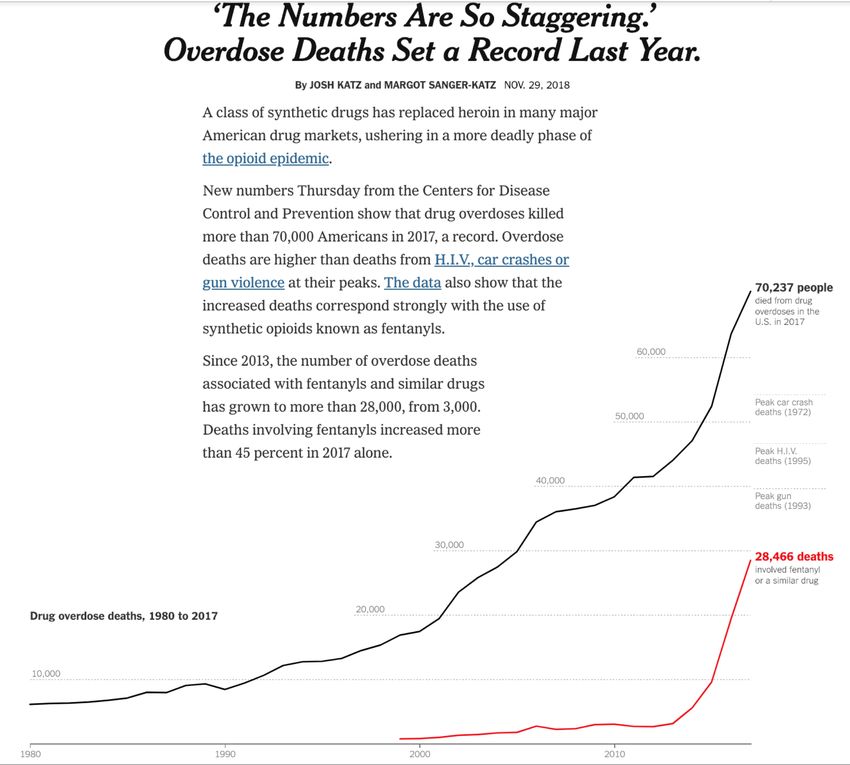
Faculty Disclosure • Dr. Podesta: Consultant—Kaleo, Pear Therapeutics, JayMac Pharmaceuticals; Speakers Bureau—Alkermes, Orexo, US WorldMeds.
Disclosure
• The faculty have been informed of their responsibility to disclose to the
audience if they will be discussing off-label or investigational use(s) of drugs,
products, and/or devices (any use not approved by the US Food and Drug
Administration).
– Dr. Podesta will be discussing off-label use of medications in this
presentation and will identify those medications.
• Applicable CME staff have no relationships to disclose relating to the subject
matter of this activity.
• This activity has been independently reviewed for balance.
• Brand names are included in this presentation for participant clarification
purposes only. No product promotion should be inferred.
Learning Objectives • Investigate barriers to successful implementation of medication- assisted therapy (MAT) for opioid use disorder (OUD) • Compare currently available pharmacotherapies for OUD including available formulations, divergence risk, and comorbid considerations • Review current evidence-based guidelines and best practices for MAT for OUD • Identify specific requirements and barriers for OUD treatment in specialized settings such as the criminal justice system and the Veterans Health Administration, as well as inpatient and outpatient settings
PRE-ACTIVITY QUESTIONS
Question 1 Which of the following pharmacotherapies are available in extended-release formulations for the treatment of OUD? A. Buprenorphine and naloxone B. Naltrexone and naloxone C. Buprenorphine and naltrexone D. Buprenorphine only
Question 2 How do you rate your ability to implement MAT across specific treatment settings? A. Excellent B. Very good C. Good D. Fair E. Poor
The Opioid
Epidemic by
the Numbers
2016 and 2017 Data
www.hhs.gov/opioids/sites/default/files/2
018-09/opioids-infographic.pdf.
Accessed February 4, 2019.The New York Times.
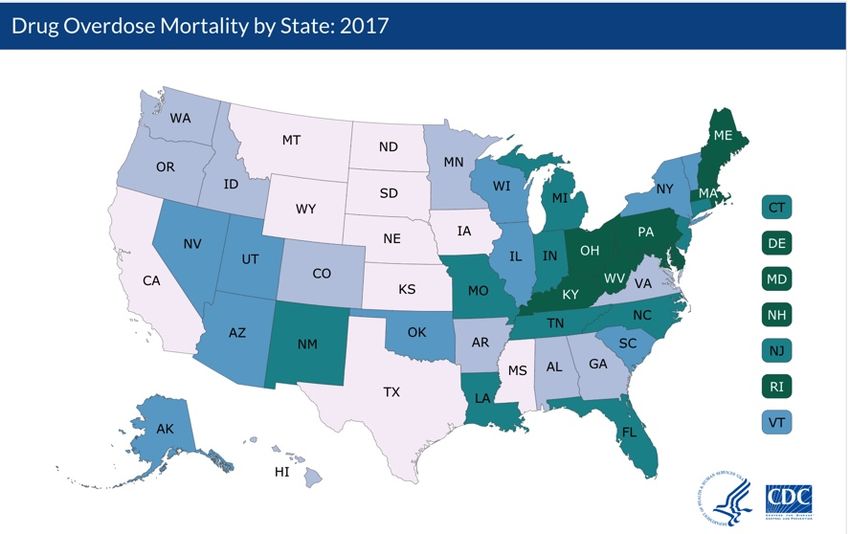
Drug Overdose Mortality
2017 (per 100,000)
Centers for Disease Control and Prevention. Drug Overdose Mortality by State.
www.cdc.gov/nchs/pressroom/sosmap/drug_poisoning_mortality/drug_poisoning.htm. Accessed February 4, 2019.3 Waves of the Rise in Opioid Overdose Deaths
10
Other Synthetic Opioids
Deaths per 100,000 Population
9
(eg, Tramadol and Fentanyl,
8 prescribed or illicitly manufactured)
7 Commonly Prescribed Opioids
(Natural & Semi-Synthetic Opioids
6
and Methadone)
5
Heroin
4
3
2
1
0
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Year Wave 3: Rise in Synthetic Opioid Overdose Deaths
Wave 1:
Rise in Prescription Opioid Overdose Deaths Wave 2:
Rise in Heroin Overdose Deaths
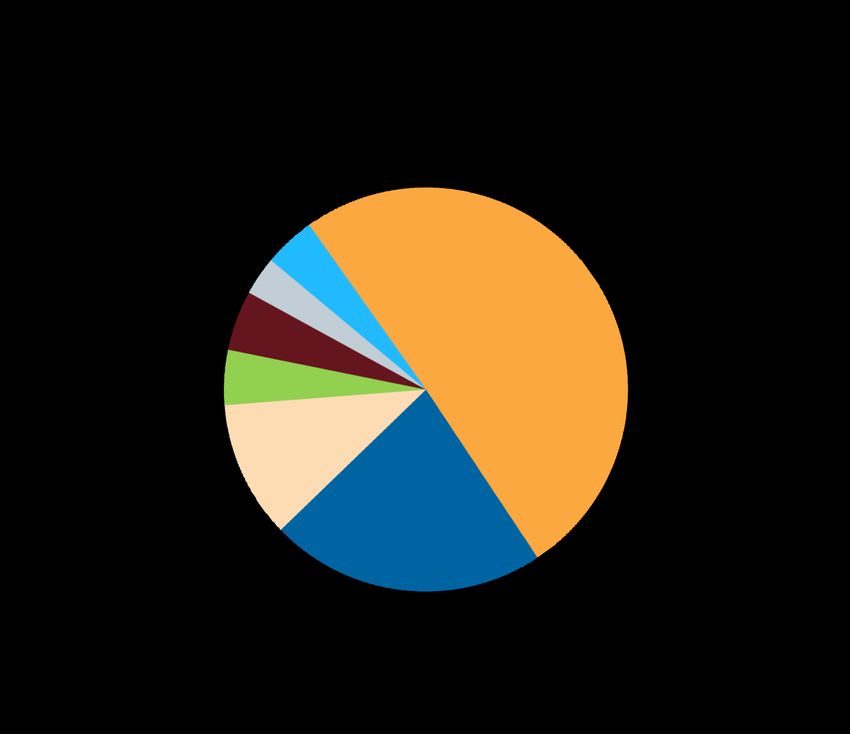
Centers for Disease Control and Prevention. Understanding the Epidemic. www.cdc.gov/drugoverdose/epidemic/index.html. Accessed February 4, 2019.Where Do People Get Nonmedically Used
Opioid Pills?
Source of Prescription Pain Relievers for the Most Recent Nonmedical Use
among Past Year Users Aged 12 or Older: Annual Averages, 2013 and 2014
Other 4.1%
From more than one doctor 3.1%
Bought from drug dealer or other stranger 4.8% 50.5%
From a
friend or relative
Took from friend or relative without asking 4.4%
for free
Bought from friend or relative 11.0%
From one doctor 22.1%
Lipari RN, et al. How people obtain the prescription pain relievers they misuse. The CBHSQ Report: January 12, 2017. Center for
Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, Rockville, MD.
www.samhsa.gov/data/sites/default/files/report_2686/ShortReport-2686.html. Accessed February 4, 2019.Strategies for Slowing Opioid Use Disorder Growth
• Drug availability • Treatment
– Decrease prescribing – Access and coverage of evidence-
• September 2018: FDA Education based practices
Blueprint for Health Care Providers – “Cover the opioid receptor”
Involved in the Treatment and • Overdose prevention
Monitoring of Patients with Pain
– “Cover the opioid receptor”
• CDC guidelines for prescribing
Opioid Pain Medications – Family/community education
• DEA and state CDS regulations for • Overdose reversal
prescribing Opioid Pain – Naloxone availability, use, training
Medications
– DEA/pharmacy drug take backs (get it
out of your medicine cabinets!)
– Law Enforcement of illicits
FDA Education Blueprint for Health Care Providers Involved in the Treatment and Monitoring of Patients with Pain. September 2018.
www.accessdata.fda.gov/drugsatfda_docs/rems/Opioid_analgesic_2018_09_18_FDA_Blueprint.pdf. Accessed February 14, 2019. CDC Guideline for Prescribing Opioids for Chronic Pain.
www.cdc.gov/drugoverdose/prescribing/guideline.html. Accessed February 14, 2019. United States Drug Enforcement Agency. DEA Brings In Record Number Of Unused Pills During 15th
Annual National Prescription Drug Take Back Day. May 07, 2018. www.dea.gov/press-releases/2018/05/07/dea-brings-record-number-unused-pills-during-15th-annual-national. Accessed
February 4, 2019. SAMHSA-HRSA Center for Integrated Health Solutions. Medication Assisted Treatment (MAT). www.integration.samhsa.gov/clinical-practice/mat/mat-overview. National
Institutes of Health, National Institute on Drug Abuse. Medications to Treat Opioid Use Disorder. Is naloxone accessible? www.drugabuse.gov/publications/medications-to-treat-opioid-
addiction/naloxone-accessible. Accessed February 4, 2019.Rationale for Medication-Assisted Treatment (MAT)
• Abstinence-based treatment – high relapse after treatment
• Detoxification combined with psychosocial treatment – relapse
rates remain at 90% or higher
• High relapse rates confirmed among those using heroin OR
prescription opioids
• Maintenance MAT with higher treatment retention than tapering off
MAT (66% vs 11%)
Gossop M, et al. Addiction. 2003;98(3):291-303. Weiss RD, et al. Arch Gen Psychiatry. 2011;68(12):1238-1246. Mattick RP, et al. Cochrane
Database Syst Rev. 2009;(3):CD002209. Nielsen S, et al. Cochrane Database Syst Rev. 2016;(5):CD011117. Fiellin DA, et al. JAMA Intern
Med. 2014;174(12):1947-1954.Guidelines for MAT
Case Example
• 45-year-old physicist, divorcing father of 4. Referred to me at IOP from his
employer after random UDT +opi and +oxy
• Upon evaluation found to be using oxycodone 20 mg, 2 to 3 ×/day
(unprescribed). He has been getting from “associates” for over 2 years.
Opioids give him energy
• He first took an opioid during college after a soccer injury and surgery. They
gave him energy, but he took the course and stopped
• A few years ago, he and his wife started a separation process and he began
feeling low mood, low energy, and not motivated. During his 20-year college
reunion, someone offered him oxycodone, and he felt GREAT! And more
“normal”
• He was able to find pills from family and friends, and took on and off,
especially for hard emotional or deep work days. About 3 months prior to
seeing me, he began taking daily after physical dependence ensued (dealer).
2 months ago he was introduced to heroin ($)
IOP = intensive outpatient program; UDT = urine drug test.What to Do?
Detoxification / Withdrawal Management
• Alpha agonists to reduce noradrenergic overactivity (lofexidine*, clonidine)
• Opioid agonist-assisted (tapering opioid doses, eg, buprenorphine)
• Symptomatic relief
– Nonsteroidal anti-inflammatory drugs, National Acupuncture Detoxification
Association (NADA) technique, benzodiazepines, dicyclomine, sleep aids
• Patient education
• Support, structure, TLC
• Restricted access to opioids
• Concurrent treatment of underlying and comorbid conditions
Adetunji B, et al. Psychiatry. 2004;1(3):32-35. Center for Substance Abuse Treatment. Clinical Guidelines for the Use of Buprenorphine in
the Treatment of Opioid Addiction. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2004. (Treatment
Improvement Protocol (TIP) Series, No. 40.) Ziaaddini H, et al. Iran Red Crescent Med J. 2014;17(1):e18202. Lin JG, et al. Evid Based
Complement Alternat Med. 2012;2012:739045.Detoxification / Withdrawal Management (cont’d)
• Lofexidine (FDA approved for opioid withdrawal symptoms, 2018)
– First non-opioid medication developed for use in opioid withdrawal
management
• Selective alpha-2 receptor agonist
– Indication
• Mitigation of symptoms associated with opioid withdrawal
• Facilitation of completion of opioid discontinuation treatment
– Dose
• 3 × 0.18 mg, QID × 7 days = total of 2.16 mg/day; the total daily dosage
should not exceed 2.88 mg (16 tablets) and no single dose should
exceed 0.72 mg (4 tablets) (dispense #96 tabs)
• +7 more days with dosing guided by symptoms
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/.Detoxification / Withdrawal Management (cont’d)
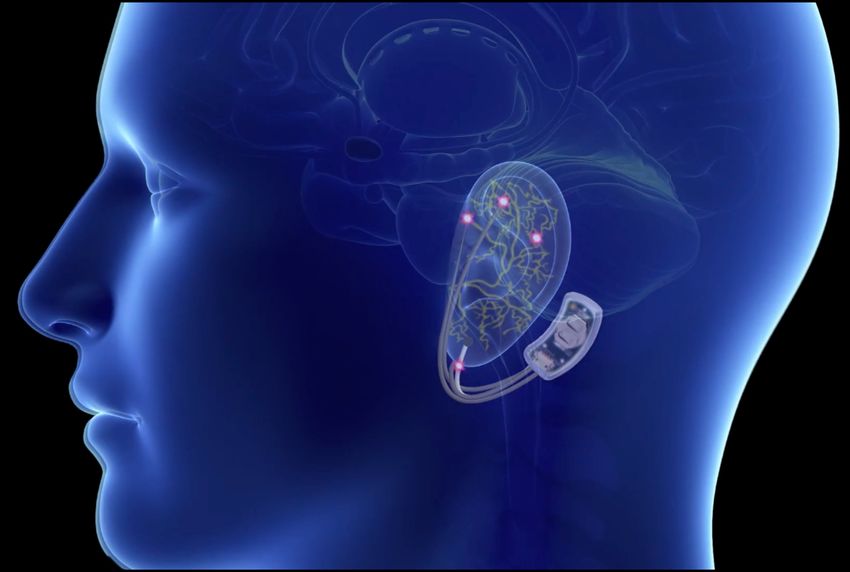
• Neuromodulation with
percutaneous nerve field
stimulator
• FDA approved November 2017
to help reduce opioid
withdrawal symptoms
Miranda A, et al. Am J Drug Alcohol Abuse. 2018;44(1):56-63.Pharmacotherapies for Opioid Use Disorder
All Work at the μ-Opioid Receptor
• Methadone (FDA approved 1947)
– μ-opioid FULL agonist
• Buprenorphine (FDA approved 2002)
– μ-opioid PARTIAL agonist
• Naltrexone (FDA approved for OUD 1984, AUD 1994)
– μ-opioid antagonist
OUD = opioid use disorder; AUD = alcohol use disorder.
Cavacuiti C (Ed). Principles of Addiction Medicine: The Essentials. Philadelphia, PA: Lippincott Williams & Wilkins; 2011. Knudsen HK, et
al. J Addict Med. 2011;5(1):21-27. The American Society of Addiction Medicine. Advancing Access to Addiction Medications.
www.asam.org/docs/default-source/advocacy/aaam_implications-for-opioid-addiction-treatment_final. Accessed February 4, 2019. US
Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/index.cfm.Opioid Receptor Activation
100
90
80 Full Agonist
Receptor Activation
(methadone)
70
Partial Agonist
60 (buprenorphine)
50 Antagonist
40
(naltrexone/naloxone)
30
20
10
0
-10 -9 -8 -7 -6 -5 -4
Log Dose of Opioid
Center for Substance Abuse Treatment. Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction. Rockville
(MD): Substance Abuse and Mental Health Services Administration (US); 2004. (Treatment Improvement Protocol (TIP) Series, No. 40.)Methadone
(FDA approved 1947)
• μ-opioid FULL agonist
• Quick absorption, slow elimination, long half-life
• Effects last 24 hours; once-daily dosing maintains constant blood level
• Daily dosing
– Pill, sublingual tablet, liquid, DISKET®
• Average daily dose 20–100 mg
• OTP clinic only
• Street value – medium
• Black box warning
– Respiratory depression
– QT prolongation
OTP = opioid treatment program.
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/index.cfm.Buprenorphine
(FDA approved 2002)
• μ-opioid PARTIAL agonist
• Implant, 6-month Probuphine®
• Monthly injectable Sublocade™
• Daily sublingual/buccal
– Suboxone®, Subutex®, Zubsolv®, Bunavail®
• Average daily dose 8–24 mg (equivalent to standard buprenorphine
dose, varies based on formulation)
• Mandatory certification from DEA
• Ceiling effect
• Street value – low/medium (often used to bridge to treatment)
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/index.cfm.Naltrexone
(FDA approved for OUD 1984, AUD 1994)
• μ-opioid antagonist
• Oral, monthly injectable (Vivitrol®)
• Decreases positive reinforcing effects
• Decreases cue-induced cravings
• Street value – none
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/index.cfm.Diversion, Street Price
Drug StreetRx Crowdsourcing Drug Diversion Survey Silk Road Marketplace
Mean, US$ (95% CI) Mean, US$ (95% CI) Mean, US$ (95% CI)
Hydromorphone $3.29 (2.74–3.96) $4.47 (3.57–5.59) $3.55 (3.09–4.08)
Buprenorphine $2.13 (1.69–2.69) $2.35 (1.97–2.80) $2.58 (2.13–3.13)
Oxymorphone $1.57 (1.27–1.95) $1.64 (1.29–2.10) $1.58 (0.73–3.43)
Methadone $0.96 (0.71–1.29) $1.16 (1.01–1.37) $0.93 (0.65–1.34)
Oxycodone $0.97 (0.90–1.04) $0.86 (0.78–0.93) $0.99 (0.83–1.18)
Hydrocodone $0.81 (0.74–0.89) $0.90 (0.84–0.97) $0.97 (0.90–1.05)
Morphine $0.52 (0.40–0.68) $0.67 (0.59–0.75) $0.42 (0.37–0.48)
Tramadol $0.05 (0.03–0.07) $0.09 (0.07–0.12) $0.02 (0.01–0.03)
Morphine values differ between Drug Diversion Survey and Silk Road based on statistical test for possibility of random error (PBuprenorphine Sublingual vs Methadone
58% Bup 73% Hi Meth 20% Low 40% Bup 39% Hi Meth 19% Low
(8 mg/day)
Mean Negative Urine Sample (%)
(60 mg/day) Meth (20 Meth
100 mg/day) 100
90 90
80 80
70
Retained (%)
70
60 60
50 50
40 40
30 30
20 20
10 10
0 0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Study Week Study Week
Johnson RE, et al. JAMA. 1992;267(20):2750-2755.Buprenorphine Sublingual vs Methadone • Both medications are highly effective, though buprenorphine has greater safety profile • Reduced opioid use, reduced mortality for both • In general, better retention with methadone • Results regarding opioid use are mixed; some studies favor buprenorphine, some favor methadone • Context/setting of treatment is quite different in the United States – opioid treatment program vs office-based practice
Mortality Risk during and after Opioid Substitution Treatment:
Systematic Review and Meta-analysis of Cohort Studies
• Meta-analysis from cohort studies published prior to 2016
• People who were dependent on opioids during and after opioid
substitution treatment, ie, buprenorphine and methadone
• The data suggests that buprenorphine “could be more effective
than methadone in reducing mortality, especially from overdose”
Methadone Buprenorphine
(per 1000 person years) (per 1000 person years)
In treatment 11.3 4.3
Out of treatment 36.1 9.5
Sordo L, et al. BMJ. 2017;357:j1550.Sublingual vs Implant Buprenorphine
• Long-acting implant buprenorphine vs placebo
– Retain 6 months (64% vs 26%) (n=114 vs 54)
– Opioid-free (64% vs “too many dropouts”)
• Long-acting implant vs 8-mg sublingual buprenorphine
– Retain 6 months (64% vs 64%) (n=114 vs 119)
– Opioid-free (31% vs 33%)
Rosenthal RN, et al. Addiction. 2013;108(12):2141-2149. Ling W, et al. JAMA. 2010;304(14):1576-1583.Sustained Release Injectable Buprenorphine
• Monthly subcutaneous injection in abdominal area following > 1 week
of sublingual buprenorphine, FDA approved November 2017
• Recommended dose: 300 mg/month × 2 months, then 100 mg/month
• Side effects of injectable buprenorphine
– Injection site reaction: Pain, itching, redness
– Body: Headache, depression, constipation, nausea, vomiting, back
pain
– Because it’s a gel, it causes a solid mass when in contact with body
fluids, so can cause possible pulmonary emboli if administered IV
– Access restricted to certified health care settings and pharmacies
• Monthly injection designed to improve adherence, reduce diversion,
and reduce unintended exposure
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/index.cfm.Sustained Release Injectable Buprenorphine for
Opioid Use Disorder
• Phase 3 study, N=504
• Injectable buprenorphine vs placebo × 6 months
– 6 once-monthly injectable buprenorphine 300 mg doses
– 2 once-monthly injectable buprenorphine 300 mg doses
followed by 4 once-monthly 100 mg doses
– 6 once-monthly injections of placebo
– All received individual drug counseling
– “Successful outcome” defined as ≥ 80% opioid-free weeks
(Weeks 5–24)
• Success rate: 28.4% (300 mg/100 mg), 29.1% (300 mg/300mg),
2% (placebo)
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/index.cfm.Oral vs Depot Naltrexone: Opioid Use Disorder
• Retention and opioid-free urine compared in 2 separate
randomized trials involving naltrexone (not directly comparing oral
vs depot)
– Long-acting injectable (n=42)
– Oral (n=69)
• Retention and opioid use at 8 weeks post-detoxification
• Long-acting depot vs oral naltrexone
– Days retained: Depot, 42 vs Oral, 32
– Opioid-free urine: Depot, 0.52 vs Oral, 0.37
Brooks AC, et al. J Clin Psychiatry. 2010;71(10):1371-1378.X-BOT Study: Buprenorphine-Naloxone vs
Injectable Extended-Release Naltrexone
• US multisite trial in NIDA Clinical Trials Network: N=570, 8 sites, 24-
week trial
• Recruited as inpatients, treated as outpatients
• Flexible randomization schedule
• 94% of buprenorphine-naloxone patients were inducted, 72% of
extended-release naltrexone patients (PAverage Opioid Craving
100
• Subjective opioid craving
90 declined rapidly from
Opioid Craving Score (VAS)
Per-protocol BUP-NX (n=270)
80
Per-protocol XR-NTX (n=204)
baseline in both treatment
70 groups
60
• Average opioid craving
50
was initially less for the
40 XR-NTX group (P=.0012
30 at week 7) than for the
20
BUP-NX group, then
converged by week 24
10
(P=.20)
0
0 2 4 6 8 10 12 14 16 18 20 22 24
Study Week
Craving was self-reported with an opioid-craving VAS, range 0–100.
VAS = visual analog scale; XR-NTX = extended-release naltrexone; BUP-NX = buprenorphine-naloxone.
Lee JD, et al. Lancet. 2018;391(10118):309-318.Extended-Release Naltrexone vs Sublingual Buprenorphine-
Naloxone for Relapse Prevention in Opioid Use Disorder
• 12-week multicenter outpatient open-label RCT, N=159
• 5 urban addiction clinics in Norway (2012–2015)
• n=80 extended-release naltrexone and n=79 buprenorphine-naloxone à
n=105 completed
• Buprenorphine-naloxone mean dose 11.2 mg
• Randomization occurred after detoxification completed
• No significant differences between groups in
– Proportion total number of days opioid negative urine tests
– Retention
– Use of heroin and other illicit opioids
– Extended-release naltrexone patients reported less heroin craving, more
treatment satisfaction
RCT = randomized controlled trial.
Tanum L, et al. JAMA Psychiatry. 2017;74(12):1197-1205.Sublingual Buprenorphine-Naloxone vs
Extended-Release Naltrexone: Summary
• Both medications are equally effective once people start them
• Starting extended-release naltrexone is challenging because it
requires detoxification and opioid abstinence first
• Major research challenge: Find optimal ways to get patients from
opioid use to naltrexoneUsing Very Low-Dose Naltrexone to Initiate
Treatment with Extended-Release Naltrexone
Discharge 1 hour after
Randomization XR-NTX injection
on Day 1/1a
Naltrexone + BUP taper
BUP lead-in Naloxone Post-XR-NTX
Screening challenge Follow-up
(4 mg*) observation
and
Days Outpatient Resident PBO-N + BUP taper XR-NTX Days 9–11 Day 22 Day 36
-26 to -6 Days Days injection
Post-
-5 to -3† -2 to -1 Treatment period XR-NTX
(Days 1‡/1a–7) outpatient
Day 8/8a§ monitoring
BUP taper
begins
Residential period Days -2 to 8/8a
*Participants maintained on < 4 mg BUP at Day -5 continued on their current dose until the treatment period taper called for further decrease. †There
was an option for earlier residential admission at the study clinician’s discretion. ‡Participants who did not qualify for randomization on Day 1
received Day -1 BUP dosing and repeat Day 1 assessments and procedures on the following day (Day 1a). §Participants who did not qualify to
receive XR-NTX on Day 8 received Day 7 study drug naltrexone/PBO-N, and completed Day 7 assessments and procedures. Day 8 assessments
and procedures were repeated the following day (Day 8a).
BUP = buprenorphine; PBO-N = placebo naltrexone.
Mannelli P, et al. The transition from buprenorphine maintenance to XR-NTX: a randomized double-blind study. Presented at: American
Society of Addiction Medicine Annual Conference; April 12–15, 2018; San Diego, CA.Using Very Low-Dose Naltrexone to Initiate
Treatment with Extended-Release Naltrexone (cont’d)
• Rates of transition to extended-release naltrexone were
comparable across groups: naltrexone/buprenorphine (46.0%) vs
naltrexone/PBO-B (40.5%) vs PBO-N/PBO-B (46.0%)
• A 7-day detoxification protocol with naltrexone alone or naltrexone
+ buprenorphine provided similar rates of induction to extended-
release naltrexone as placebo
• For those inducted onto extended-release naltrexone,
management of opioid withdrawal symptoms prior to induction
was achieved in a structured outpatient setting using a well-
tolerated, fixed-dose ancillary medication regimen common to all
3 groups
Mannelli P, et al. The transition from buprenorphine maintenance to XR-NTX: a randomized double-blind study. Presented at: American
Society of Addiction Medicine Annual Conference; April 12–15, 2018; San Diego, CA.Case Example • 45-year-old physicist, divorcing father of 4. Referred to me at IOP from his employer after random UDT +opi and +oxy • Upon evaluation found to be using oxycodone 20 mg, 2 to 3 ×/day (unprescribed). He has been getting from “associates” for over 2 years. Opioids give him energy • He first took an opioid during college after a soccer injury and surgery. They gave him energy, but he took the course and stopped • A few years ago, he and his wife started a separation process and he began feeling low mood, low energy, and not motivated. During his 20-year college reunion, someone offered him oxycodone, and he felt GREAT! And more “normal” • He was able to find pills from family and friends, and took on and off, especially for hard emotional or deep work days. About 3 months prior to seeing me, he began taking daily after physical dependence ensued (dealer). 2 months ago he was introduced to heroin ($)
Case Example (cont’d) • Psychiatric Hx: No formal, but sometimes social anxiety • Medical Hx: ACL repair in college. Hypertension. Takes irbesartan 150 mg • Allergies: NKDA • Family Hx: Father with Hx depression, maternal grandmother Hx with alcoholism. Brother with anxiety and Hx benzodiazepine UD • BMI: ~ 28 • Labs: CBC, CMP, TSH – WNL; Homocysteine – 15; Vitamin D – 18; MTHFR – 677 heterozygous, 1298 heterozygous
Case Example (cont’d) Course of Treatment: • Began buprenorphine 8 mg, 2 in day; Vitamin D; activated folate. Effective. Energy, mood, focus, motivation good. Completed IOP. Back to work • Continued to see me outpatient. Stable. New relationship. Wanted to stop buprenorphine • Lofexidine protocol, then naltrexone oral 3 days, then extended- release naltrexone injection. Effective, no cravings, but lower energy and mood. Added bupropion XL 150 mg then 300 mg. Mostly effective
Case Example (cont’d) • Missed 3rd injection during breakup with girlfriend. Found oxycodone pill. Took. Continued daily for 2 weeks. Resurfaced to my clinic • Restarted buprenorphine, in different SL form. Educated RE: injectable buprenorphine. Ordered, took 2 weeks to fulfill. Received injection. Effective. Now on 3rd injection
Comparison/Qualities of the 3 Treatments for
Opioid Use Disorder
Agonist Therapy Partial Agonist Therapy Antagonist Therapy
Binds to μ-Opioid Receptor Yes Yes Yes
Activates μ-Opioid Receptor Yes
Yes No
to Release Dopamine but not to the extent of a full agonist
Daily sublingual film, sublingual tablet, Daily oral medication or
Daily
Administration buccal film, 6-month subdermal monthly intramuscular
oral concentration
implant, or extended-release injection injection
Sublingual film, sublingual tablet, or
buccal film can be initially provided
Daily oral can be provided
in a physician’s office then as a
Provided at as take-home medication.
Setting take-home medication.
certified OTP settings Monthly injection requires
The 6-month subdermal implant
HCP administration.
and extended-release injection
require HCP administration.
Schedule II Schedule III
DEA Schedule Not scheduled
controlled substance controlled substance
Requires Detoxification No No Yes
Requires Counseling Yes Yes Yes
Kosten TR, et al. Sci Pract Perspect. 2002;1(1):13-20. US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products.
www.accessdata.fda.gov/scripts/cder/daf/.Treatments in Special Populations
Criminal Justice Population
• Diversion Courts • Barriers
• Drug Courts – Access, buy in
• Deflection – Education
– Misuse of the systemCriminal Justice Population
Pregnant Women
• Co-managed by OB/GYN and addiction specialist
• Agonist or partial agonist Tx (patient choice and access)
– OK in breastfeeding
– NOWS: Buprenorphine < Methadone
• Antagonist in some cases (benefit vs risk)
NOWS = neonatal opioid withdrawal syndrome.
American Society of Addiction Medicine. The ASAM National Practice Guideline for the Use of Medications in the Treatment of Addiction
Involving Opioid Use. 2015. www.asam.org/docs/default-source/practice-support/guidelines-and-consensus-docs/asam-national-practice-
guideline-supplement.pdf. Accessed February 14, 2019. Jones HE, et al. Addiction. 2012;107 Suppl 1:28-35.Adolescents
• Agonists, partial agonists, and antagonists may be considered
– Virtually no studies
– Indicated for 18+
• Federal Code on opioid Tx – 42 CFR 8.12 offers an exception for
patients aged 16+17 who have a documented history of 2+ prior
unsuccessful withdrawal attempts and have parental consent
• Psychosocial Tx recommended
American Society of Addiction Medicine. The ASAM National Practice Guideline for the Use of Medications in the Treatment of Addiction
Involving Opioid Use. 2015. www.asam.org/docs/default-source/practice-support/guidelines-and-consensus-docs/asam-national-practice-
guideline-supplement.pdf. Accessed February 14, 2019.Veterans Health Care Administration
• Population with high rates of
trauma + substance abuse + Working
comorbid mental health issues
Your Body
Power of Energy
& Surroundings
the Mind Flexibility Physical
• Embracing a Patient Centered Relaxing
&
Healing
&
Emotional
Care model with emphasis on Spirit & Personal
Whole Health Soul
Growing
&
ME
Development
Personal Life
&
Connecting Work Life
Family, Food & Drink
Friends, & Nourishing
Coworkers Recharge
&
Relationships Fueling
Sleep
&
Refresh
Self Professional Whole
ME Care Care Community
Health
US Department of Veterans Affairs. Whole Health For Life. www.va.gov/PATIENTCENTEREDCARE/features/More_Than_Medicine.asp.
Accessed February 4, 2019.Implementing
• All levels of care should screen and have tools to treat and/or
refer
– Emergency room, primary care, outpatient addiction/behavioral
health, IOP, partial hospital program (PHP), residential
treatment center, hospital-based treatment
• Appropriate level of care for patients
• Chronic care model
• Hub+Spoke system (Vermont)
Srivastava A, et al. Can Fam Physician. 2017;63(3):200-205. State of Vermont Blueprint for Health. Hub and Spoke.
https://blueprintforhealth.vermont.gov/about-blueprint/hub-and-spoke/. Accessed February 4, 2019. Substance Abuse and Mental Health
Services Administration. TIP 63: Medications for Opioid Use Disorder. https://store.samhsa.gov/product/TIP-63-Medications-for-Opioid-
Use-Disorder-Full-Document-Including-Executive-Summary-and-Parts-1-5-/SMA18-5063FULLDOC. Accessed February 4, 2019.Implementing (cont’d)
• Continuity of care
• Resources
• Counselors
• Community
• Family
• Medication (X#, methadone OTP)
Srivastava A, et al. Can Fam Physician. 2017;63(3):200-205. State of Vermont Blueprint for Health. Hub and Spoke.
https://blueprintforhealth.vermont.gov/about-blueprint/hub-and-spoke/. Accessed February 4, 2019. Substance Abuse and Mental Health
Services Administration. TIP 63: Medications for Opioid Use Disorder. https://store.samhsa.gov/product/TIP-63-Medications-for-Opioid-
Use-Disorder-Full-Document-Including-Executive-Summary-and-Parts-1-5-/SMA18-5063FULLDOC. Accessed February 4, 2019.Child Care
Services
Family Vocational
Services Services
Intake Processing /
Assessment
Housing /
Mental Health
Transportation Detoxification Services
Services Behavioral Therapy Substance Use
and Counseling Monitoring
Treatment Plan
Clinical and Case Self-Help / Peer
Management Support Groups
Financial Pharmacotherapy Medical
Services Services
Continuing Care
Legal Educational
Services Services
AIDS / HIV
Services
Friedmann PD, et al. Addiction. 2004;99(8):962-972.Barriers
• Detoxification à Treatment
• Stigma
• Access to care
• Public education, knowledge
Jones HE, et al. Addiction. 2012;107 Suppl 1:28-35. Sharma A, et al. Curr Psychiatry Rep. 2017;19(6):35.In Conclusion
• Addiction is a complex disorder • X number, DEA waiver
• Use a chronic care approach • Therapists/Counselors
• Resources for complementary
• Multi-modal, individualized approaches
treatment is essential • Treatment programs to refer to and
• Multiple courses of treatment from
may be required for success – Facilitated referral best
• Adequate time frame is • Community-based peer support
needed—3+ months to programs
produce stable behavior – 12 Step, includes Refuge
change—the longer the better Recovery, Self-Management and
Recovery Training (SMART),
• Relapse is likely Alcoholics Anonymous (AA), etc.POST-ACTIVITY QUESTIONS
Question 1 Which of the following pharmacotherapies are available in extended-release formulations for the treatment of OUD? A. Buprenorphine and naloxone B. Naltrexone and naloxone C. Buprenorphine and naltrexone D. Buprenorphine only
Question 2 How do you rate your ability to implement MAT across specific treatment settings? A. Excellent B. Very good C. Good D. Fair E. Poor
Q&A
You can also read

















































