Comparative effectiveness of glucosamine, chondroitin, acetaminophen or celecoxib for the treatment of knee and/or hip osteoarthritis: a network ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Comparative effectiveness of glucosamine, chondroitin,
acetaminophen or celecoxib for the treatment of knee
and/or hip osteoarthritis: a network meta-analysis
X. Zhu1, D. Wu1, L. Sang1, Y. Wang3, Y. Shen2, X. Zhuang1, M. Chu1, L. Jiang4,1
1
Department of Epidemiology, and 2Department of Health Statistics, School of Public Health,
Nantong University, Jiangsu Province, P.R. China;
3
Affiliated Hospital of Nantong University, Nantong University, Jiangsu Province, P.R. China,
4
Collaborative Research Center, Shanghai University of Medicine and Health Sciences,
Shanghai, P.R. China.
Abstract
Objective
To compare the efficacies of oral glucosamine, chondroitin, the combination of glucosamine and chondroitin,
acetaminophen and celecoxib on the treatment of knee and/or hip osteoarthritis.
Methods
We searched electronic databases including PubMed, Embase, and Cochrane Library and the reference lists of relevant
articles published from inception to October 23, 2017. A Bayesian hierarchical random effects model was used to
examine the overall effect size among mixed multiple interventions.
Results
We identified 61 randomised controlled trials of patients with knee and/or hip osteoarthritis. There was no obvious
difference in the results between the traditional meta-analysis and the network meta-analysis. The network meta-analysis
demonstrated that celecoxib was most likely the best option (SMD, -0.32 [95% CI, -0.38 to -0.25]) for pain, followed by
the combination of glucosamine and chondroitin. For physical function, all interventions were significantly superior to
oral placebo except for acetaminophen. In terms of stiffness, glucosamine (SMD, -0.36 [95% CI, -0.67 to -0.06]) and
celecoxib (SMD, -0.29 [95% CI, -0.51 to -0.08]) were significantly better compared to placebo. In view of safety,
compared to placebo only, celecoxib and acetaminophen presented significant differences.
Conclusion
Given the effectiveness of these non-steroidal anti-inflammatory drugs and symptomatic slow-acting drugs, oral
celecoxib is more effective than placebo on relieving pain and improving physical function, followed by the combination
of glucosamine and chondroitin. Acetaminophen is likely the least efficacious intervention option. This information,
accompanied by the tolerability and economic costs of the included treatments, would be conducive to making decisions
for clinicians.
Key words
osteoarthritis, treatment, glucosamine, chondroitin, acetaminophen, celecoxib
Clinical2018
Clinical and Experimental Rheumatology and Experimental Rheumatology 2018; 36: 595-602.Efficacy of oral preparations for the treatment of OA / X. Zhu et al.
Xiaoyue Zhu, MD* Introduction (12, 13). Furthermore, acetaminophen
Dandong Wu, MD* Osteoarthritis (OA), which is charac- (paracetamol), commonly known as a
Lingli Sang, MD terised by progressive cartilage matrix non-prescription medication for over
Yidan Wang, MD
degradation, subchondral bone sclerosis 50 years, is often recommended as the
Yi Shen, MD
Xun Zhuang, PhD and osteophyte formation, is the most first-line therapy because of its cheap
Minjie Chu, PhD** common degenerative joint disease and price and low risk of gastrointesti-
Liying Jiang, PhD** primarily affects weight-bearing joints nal adverse effects compared to other
*These authors contributed equally to such as the knee and hip (1, 2). Present- NASIDs such as aspirin (10). Celecox-
this paper as co-first authors. ly, OA has emerged as a major public ib is a selective NSAID that has been
**These authors contributed equally to health concern and continues to affect considered the first specific inhibitor
this paper as co-corresponding authors. approximately 10% of men and 18% of of cyclo-oxygenase-2 (COX-2) by the
Please address correspondence to: women over 60 years of age (3), with American Food and Drug Administra-
Dr Liying Jiang, total DALYs increasing by 35% and tion (FDA) in December 1998(14). Re-
Collaborative Research Center, age-standardised DALY rates increas- gardless of its gastrointestinal adverse
Shanghai University of Medicine ing by 4% between 1990 and 2015. It is effects, celecoxib has become a typi-
and Health Sciences, a leading cause of pain, disability, and cal inhibitor of COX-2 and reduces its
Shanghai, 200120, P.R. China.
E-mail: J_meili@126.com
socioeconomic costs worldwide (4). related signs and symptoms (15); it is
Pain symptoms associated with OA also recommended by OARSI guide-
and
Dr Minjie Chu
may result in increased walking dis- lines (11). The effects of glucosamine
E-mail: minjie0830@126.com ability and all-cause mortality (5). and chondroitin on knee and/or hip OA
Received on July 25, 2017; accepted in Therefore, the alleviation and control compared to a placebo have been stud-
revised form on November 17, 2017. of pain is an important consideration in ied by a previous meta-analysis (16).
© Copyright Clinical and the clinical practice of OA treatments. In addition, a meta-analysis on the ef-
Experimental Rheumatology 2018. Although there are many symptomatic ficiency and safety of acetaminophen
interventions, most are non-specific has also been conducted (17). Most
and lack effective disease-modifying importantly, a clinical trial conducted
medical treatments. Non-steroidal anti- in 2014 suggested that a certain dosage
inflammatory drugs (NSAIDs) are the of acetaminophen can provide effec-
most widely used, and symptomatic tive relief of signs and symptoms (18).
slow-acting drugs (SYSADOAs) for However, available studies investigat-
OA are accessible in clinical practice. ing the comparative effects between
Glucosamine and chondroitin are es- NSAIDs and SYSADOAs are limited.
sential SYSADOAs; they are naturally At present, the effectiveness of SYSA-
occurring compounds in the body that DOAs for OA treatment is conflicting
function as the principal substrates in based on the results of several RCTs
the biosynthesis of proteoglycan (6). (12, 13, 19). Additionally, compared to
Glucosamine and chondroitin are both a placebo, the effects of acetaminophen
partially absorbed and then reach the have been illustrated by a previous
joints, where they relieve joint pain meta-analysis. Moreover, a comparison
and slow the rate of joint destruction between acetaminophen and chondroi-
and cartilage loss (7, 8). As a result, tin, particularly glucosamine and chon-
glucosamine and/or chondroitin are droitin in combination, has not been
available as over-the-counter products conducted. Therefore, the comparative
(9). However, recently, the efficacy of effectiveness of these treatments for
glucosamine, chondroitin, or the com- OA must be explored.
bination of the two has been widely A Bayesian network meta-analysis in-
discussed, triggering a fierce contro- tegrates evidence from all RCTs, which
versy. International guidelines for their increases the statistical power by com-
Funding: this study was supported by management have provided an equivo- bining evidence from direct and indirect
the Research Innovation Program for
College Graduates of Nantong University
cal recommendation of glucosamine comparisons and examining the rela-
(YKC16019) and the Jiangsu Students’ and chondroitin (10). However, they tive effects that have few comparisons.
Platform for Innovation and Entrepreneur- are not recommended according to the Moreover, it also presents a uniform
ship Training Program (201710304058Z). Osteoarthritis Research Society Inter- and reasonable method to identify the
This study did not warrant institutional national (OARSI) guidelines published differences among those intervention
review board approval because no human in 2014 (11). In addition, their effec- groups (20). Based on the existing evi-
subjects were involved. tiveness is conflicting based on several dence, we have assessed and examined
Competing interests: none declared. randomised controlled trials (RCTs) the efficacy and safety of glucosamine,
596 Clinical and Experimental Rheumatology 2018Efficacy of oral preparations for the treatment of OA / X. Zhu et al.
chondroitin, the combination of glu- eligibility and extracted the data in ac- those suggested outcomes when more
cosamine and chondroitin, celecoxib or cordance with a preconfigured form. than one pain scale was given for a
acetaminophen for primary OA. Any disagreements were resolved trial. Among these scales, global pain
through discussion with a third review- has precedence over pain on walking
Methods er (L.Y.J.). For each study, the patients’ and the Western Ontario and McMas-
Search strategy characteristics including mean age, sex, ter Universities Osteoarthritis Index
We conducted this network meta- mean duration of symptoms, BMI, du- (WOMAC) pain subscale (26, 27).
analysis following the PRISMA exten- ration of follow-up, type of outcome Similarly, data on function and stiffness
sion statement (21). We systematically (pain, function, stiffness and AEs), trial were extracted with the same method.
searched electronic databases includ- design, trial size, details of intervention, If the global function score was not re-
ing PubMed, Embase, and Cochrane treatment duration and results were in- ported, the walking disability, function
Library based on logic combinations dividually extracted. For crossover subscale of the WOMAC or Lequesne
of keywords and text words associated trials, we extracted data from the first Index was applied instead.
with OA to extract concerned RCTs period only to avoid possible carryover The standard mean difference (SMD)
from inception to October 23, 2017. The effects. Data of intention-to-treat analy- was used to calculate the difference
Internet-based search used the follow- ses were used whenever possible. between various intervention arms be-
ing terms: “arthritis”, “osteoarthritis”, cause different studies assessed the
“OA”, “joint disease”, “glucosamine”, Quality assessment same outcome by employing different
“GH”, “GS”, “chondroitin”, “CH”, The Cochrane Risk of Bias Tool was scales. SMD expresses the size of the
“CS”, “acetaminophen”, “paraceta- used to evaluate the methodological intervention effect in each study relative
mol”, “celecoxib”, “celebrex”, and the quality of the included studies (v. 5.3) to the variability observed in that study
corresponding free terms. The search (24). The tool evaluates seven potential by dividing the pooled SD of the dif-
was restricted to the English language risks of bias: random sequence genera- ferences between two interventions (28,
and studies of human participants. We tion, allocation concealment, blinding 29). The effect size was transformed
then screened the reference lists of all of participants, blinding of outcome back to the difference units of the
obtained articles, including relevant assessment, incomplete outcome data, WOMAC visual analogue scale (VAS),
reviews, to avoid missing relevant ar- selective reporting and other bias. Each which is the most commonly used scale
ticles. We also searched Clinical Trials. item was judged by the following cri- and is based on a median pooled SD of
gov for progressive trials. teria: low risk of bias, uncertain risk 2.5 cm to assess pain on a scale of 0 to
of bias, and high risk of bias. Studies 10 cm. A standardised WOMAC func-
Inclusion and exclusion criteria that included three or more high risk tion score (0-10) was transformed by
Studies were included if they met the of bias areas were considered to have the SMD, which is based on a median
following criteria: (1) RCTs; (2) stud- poor methodological quality. The qual- pooled SD of 2.1 units. A change of 2
ies about primary hip and/or knee OA ity of evidence on pain, function and points on the 0–10 scale was interpreted
patients with clinical and/or radiologic stiffness was evaluated by the Grading as a clinically significant improvement
diagnosis; (3) studies covering at least of Recommendations, Assessment, De- (30). A negative effect size indicated
two of the following treatments: glu- velopment, and Evaluation (GRADE) a better treatment effect on pain relief
cosamine, chondroitin, the two in com- system (25). The quality of evidence and function improvement. The abso-
bination, acetaminophen, celecoxib, was presented as high, moderate, low or lute changes in pain, function and stiff-
and placebo; and (4) extractable data very low. Two reviewers independently ness from baseline were also evaluated
reporting on the pain, function, stiffness evaluated each study. by a classical meta-analysis.
and adverse events (AEs) of patients.
The exclusion criteria were as follows: Outcome measures Statistical analysis
(1) studies of non-randomised or uncon- The primary outcomes of this network Bayesian meta-analysis integrates both
trolled trials; (2) treatments described meta-analysis were pain intensity, func- direct evidence from head-to-head
unclearly; (3) studies or data reported tion improvement and stiffness score studies and indirect evidence from all
repeatedly; and (4) trial arms with sub- from baseline to the end of treatment original trials. The Bayesian Markov
therapeutic doses (celecoxib not equal using certain dosages of celecoxib, Chain Monte Carlo is a method used
to 200 mg/day; acetaminophen below acetaminophen, glucosamine, chon- to estimate posterior densities for un-
3000 mg/day;Efficacy of oral preparations for the treatment of OA / X. Zhu et al.
servative and appropriate than the fixed Fig. 1. Network of
effects model, was used to examine the treatment comparisons
included in the analy-
overall effect size among mixed multi- sis for pain.
ple treatments of OA with non-inform- The size of every cir-
ative prior distributions. Before pooling cle reflects the number
of participants.
the data with a random-effects model The width of every
within a Bayesian framework, the com- line corresponds to the
parative effects were initially analysed number of direct com-
parisons; the number
by the traditional pairwise meta-analy- shown beside the line
sis method. For continuous outcomes, represents the number
the summary effect size was calculated of trials.
No connecting line
as the SMD along with 95% credible
between 2 treatments
intervals (CIs). For the count data, the indicates no direct
relative risk (RR) with 95% CI was used comparison.
to present the effect size. It was possible
to rank the superior orders among the
included interventions according to the
posterior probabilities, and we reported The baseline characteristics of the in- cosamine and chondroitin and acetami-
the value as the surface under the cu- cluded studies are shown in Supple- nophen.
mulative ranking (SUCRA). The best mentary file 1: Table S1 (the references Fifty-six studies (22,128 participants)
treatment effect has a SUCRA value of of the included studies are provided). contributed to the network meta-anal-
100%, whereas the worst treatment ef- Forty-seven trials covered participants ysis of pain-related outcomes. Table I
fect has a SUCRA value of 0%. Several with only knee OA, two trials con- presents the effect sizes and the related
sensitivity analyses on the primary out- tained participants with only hip OA, 95% CIs of the network meta-analysis
comes were performed to explore the and twelve trials included patients with about the changes in pain score between
heterogeneity according to the sample knee and/or hip OA. different interventions at the last follow-
size and the study quality. We also cal- up period. All treatments showed a sig-
culated the consistency of the network Risk of bias nificantly better effect compared to pla-
determined by the difference in effect The risk of bias of the included trials cebo. When the SMD was transformed,
sizes from direct and indirect compari- is summarised in Supplementary file 1: glucosamine had a value of -0.33 cm
sons in one loop. Publication bias was Table S2. None of the studies had poor (95% CI, -0.60 to -0.10 cm), chon-
examined through visual inspection of methodological quality. Randomisa- droitin was -0.53 cm (95% CI, -0.83
funnel plot asymmetry. WinBUGS (v. tion was mentioned in all trials, and to -0.28 cm), the combination of glu-
1.4.3, MRC Unit, Cambridge, UK), all studies were judged to have a low cosamine and chondroitin was -0.58 cm
STATA (v. 13.1, StataCorp, College Sta- risk of bias for blinding to patients. (95% CI, -0.98 to -0.18 cm), celecoxib
tion, TX), and Review Manage (v. 5.3, The quality of evidence was measured was -0.80 cm (95% CI, -0.95 to -0.63
Oxford, UK) were used for the analyses. by the GRADE system (Table I). The cm), and acetaminophen was -0.35 cm
quality grade was downgraded primar- (95% CI, -0.65 to -0.05 cm). All inter-
Results ily due to indirectness and imprecision ventions met the pre-specified minimal
Study selection and characteristics (see details in Supplementary file 1: clinically significant improvement.
The summary of the study search and Tables S3-S5). The model fit well for Celecoxib was statistically significantly
selection is presented in the Appendix pain, function and stiffness outcomes superior to acetaminophen (SMD, -0.18
Supplementary file 2: Fig. S1. Among (Supplementary file 2: Fig. S11). Com- [95% CI, -0.31 to -0.05]). Compared to
the 3359 records identified and se- parison-adjusted funnel plots showed celecoxib, glucosamine showed a worse
lected from the literature search, 3060 no evidence of asymmetry (Supple- effect (SMD, 0.18 [95% CI, 0.07 to
irrelevant articles were excluded. Af- mentary file 2: Fig. S5–S7). 0.29]). According to the SUCRA related
ter screening and reading the full text to pain, the top three ranked treatments
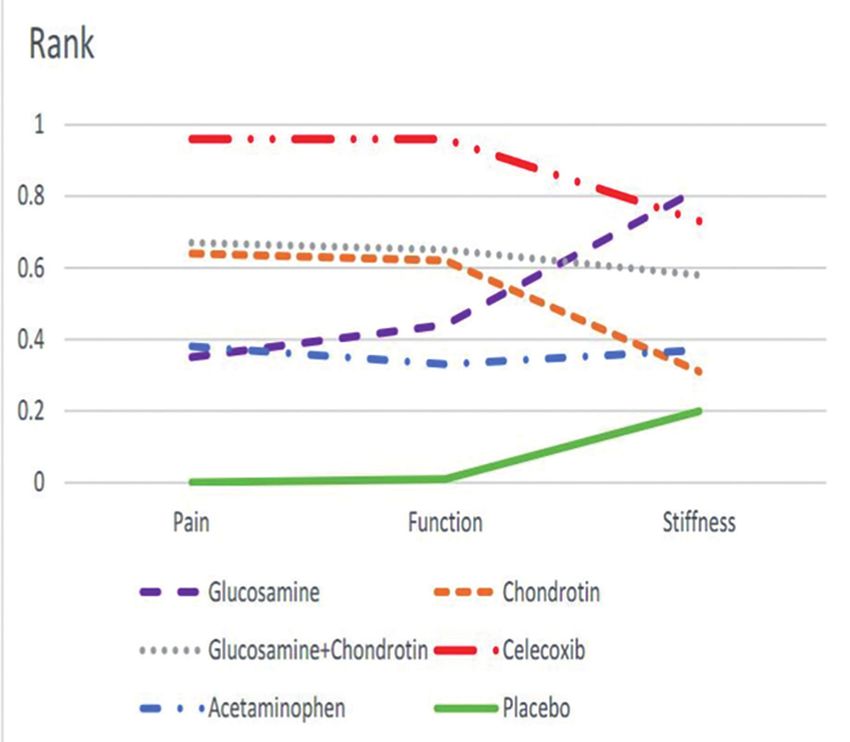
of 299 articles, 58 articles (61 RCTs) Pain were celecoxib (96%), the combination
met the inclusion criteria and were in- Figure 1 shows the network of the inter- of glucosamine and chondroitin (67%)
cluded in the network meta-analysis, 3 ventions included in this study for pain. and chondroitin (64%) (Fig. 2). No in-
of which reported the results of two tri- Six nodes indicated different interven- consistencies were detected between the
als. Therefore, 61 RCTs were employed tions of drugs with a specific daily dose. direct and indirect evidence (Supple-
to assess the efficacies of oral glucosa- Celecoxib (200 mg/day) was the most mentary file 2: Fig. S8).
mine, chondroitin, the combination commonly studied drug. However,
of the glucosamine and chondroitin, there were few direct comparisons be- Function
celecoxib and acetaminophen for pa- tween chondroitin and acetaminophen Forty-five articles (47 RCTs) with
tients with knee and/or hip OA. or between the combination of glu- 19,727 patients contributed to the net-
598 Clinical and Experimental Rheumatology 2018Efficacy of oral preparations for the treatment of OA / X. Zhu et al.
Table I. Estimates of the treatment effect on pain, function and stiffness.
Interventions Pain, SMD (95% CI) Function, SMD (95% CI Stiffness, SMD (95% CI)
Network Direct GRADE Network Direct GRADE Network Direct GRADE
meta-analysis comparison meta-analysis comparison meta-analysis comparison
Glucosamine
Chondroitin 0.08(-0.06,0.22) 0.03(-0.10,0.16) High 0.04(-0.09,0.18) 0.05(-0.08,0.17) High -0.32(-0.85,0.20) -0.07(-0.22.0.09) High
Glucosamine+Chondroitin 0.09(-0.09,0.27) 0.10(-0.05,0.24) High 0.05(-0.12,0.22) 0.12(-0.01,0.24) High -0.14(-0.69,0.39) 0.09(-0.07,0.24) Moderate
Celecoxib 0.18(0.07,0.29) -0.04(-0.44,0.37) Moderate 0.14(0.02,0.25) -0.06(-0.56,0,44) Moderate -0.06(-0.44,0.29) 0.13(-0.02,0.29) Moderate
Acetaminophen 0.01(-0.15,0.15) -0.09(-0.36,0.17) Low -0.04(-0.21,0.12) -0.05(-0.32,0.22) Moderate -0.28(-0.84,0.26) NA Moderate
Placebo -0.13(-0.24,-0.04) -0.10(-0.25,0.05) High -0.17(-0.28,-0.07) -0.12(-0.26,0.01) High -0.36(-0.67,-0.06) -0.30(-0.60,-0.00) High
Chondroitin
Glucosamine+Chondroitin 0.02(-0.17,0.19) 0.05(-0.17,0.27) High 0.01(-0.17,0.18) 0.08(-0.05,0.20) High 0.18(-0.44,0.79) 0.15(-0.00,0.31) High
Celecoxib 0.10(-0.03,0.23) 0.15(-0.00,0.31) High 0.09(-0.03,0.21) 0.16(0.00,0.31) High 0.26(-0.23,0.74) 0.20(0.05,0.36) High
Acetaminophen -0.07(-0.24,0.09) NA Moderate -0.08(-0.26,0.09) NA Moderate 0.04(-0.61,0.68) NA Moderate
Placebo -0.21(-0.33,-0.11) -0.21(-0.36,-0.07) High -0.22(-0.33,-0.11) -0.22(-0.36,-0.08) High -0.04(-0.50,0.42) 0.03(-0.09,0.15) Moderate
Glucosamine+Chondroitin
Celecoxib 0.09(-0.07,0.25) 0.00(-0.11,0.12) High 0.08(-0.07,0.24) 0.04(-0.12,0.19) High 0.08(-0.40,0.56) 0.06(-0.06,0.17) High
Acetaminophen -0.09(-0.29,0.11) NA Moderate -0.09(-0.30,0.11) -0.24(-0.52,0.04) High -0.14(-0.79,0.51) NA Moderate
Placebo -0.23(-0.39,-0.07) -0.10(-0.22,0.33) High -0.23(-0.38,-0.08) -0.12(-0.24,0.01) High -0.21(-0.69,0.26) -0.07(-0.21,0.07) High
Celecoxib
Acetaminophen -0.18(-0.31,-0.05) -0.18(-0.31,-0.05) High -0.18(-0.33,-0.03) NA Low -0.22(-0.70,0.26) -0.25(-0.54,0.03) Moderate
Placebo -0.32(-0.38,-0.25) -0.32(-0.37,-0.27) High -0.31(-0.38,-0.25) -0.32(-0.37,-0.27) High -0.29(-0.51,-0.08) -0.28(-0.36,-0.21) High
Acetaminophen
Placebo -0.14(-0.26,-0.02) -0.14(-0.21,-0.06) High -0.14(-0.27,0.01) -0.16(-0.31, 0.00) High -0.08(-0.53,0.38) -0.17(-0.34,0.01) High
CI: Confidence interval; NA: Not applicable; GRADE: Grading of Recommendations, Assessment, Development, and Evaluation.
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
work meta-analysis of physical func- network meta-analysis of stiffness out- 1.12 to 2.95]), whereas acetaminophen
tion outcomes (Supplementary file 2: comes (Supplementary file 2: Fig. S3). showed a similar value (RR, 1.97 [95%
Fig. S2). All interventions except for Compared to placebo, glucosamine CI, 1.11 to 3.52]). The safety and tolera-
acetaminophen were statistically sig- (SMD, -0.36 [95% CI, -0.67 to -0.59]) bility analyses are presented in Table II.
nificantly better than oral placebo in and celecoxib (SMD, -0.29 [95% CI,
the aspect of function improvement -0.51 to -0.08]) were significantly su- Sensitivity analysis
(Table I). After being transformed, the perior. Other comparisons showed To confirm the robustness of the result,
difference for glucosamine was -0.36 no statistical significance in terms of we also conducted sensitivity analy-
units (95% CI, -0.59 to -0.15 units), stiffness (Table I). The SUCRA rank ses for those outcomes. A sensitivity
chondroitin was -0.46 units (95% CI, was presented as follows (Fig. 2): glu- analysis of the sample size and meth-
-0.69 to -0.23 units), the combination cosamine (82%), celecoxib (73%), the odological quality of the included stud-
of glucosamine and chondroitin was combination of glucosamine and chon- ies did not show any major changes in
-0.48 units (95% CI, -0.80 to -0.17 droitin (58%), acetaminophen (37%), pain, function and stiffness outcomes
units), celecoxib was -0.65 units (95% chondroitin (31%) and placebo (20%). (Supplementary file 1: Table S6).
CI, -0.80 to -0.53 units), and acetami- No significant inconsistencies were de-
nophen was -0.29 units (95% CI, -0.57 tected between the direct and indirect Discussion
to -0.02 units). According to the SU- evidence (Supplementary file 2: Fig. We estimated the effectiveness of dif-
CRA of function (Fig. 2), celecoxib S10). ferent interventions including glu-
was the best treatment (96%), followed cosamine, chondroitin, the combina-
by the combination of glucosamine and Safety tion of glucosamine and chondroitin,
chondroitin (65%), chondroitin (62%) Forty-one articles (44 RCTs) reported celecoxib and acetaminophen. In our
and glucosamine (44%), with placebo the withdrawal of patients due to AEs, study, we performed four individual
as the worst treatment (1%). No incon- and 38 studies reported the number of outcome-oriented network meta-analy-
sistencies were detected between the patients with AEs (Supplementary file ses. The pooled effect sizes suggested
direct and indirect evidence (Supple- 2: Fig. S4). Diarrhoea, abdominal pain, that all interventions may alleviate pain
mentary file 2: Fig. S9). nausea and headache were the most symptoms and improve function. The
commonly reported AEs. Compared to recommended dosage of oral celecoxib
Stiffness glucosamine, the celecoxib treatment is more effective than placebo on re-
Twenty-nine articles (30 RCTs) with option exhibited a relatively higher lieving pain and improving physical
12,404 participants contributed to the incidence of AEs (RR, 1.82 [95% CI, function, followed by the combina-
Clinical and Experimental Rheumatology 2018 599Efficacy of oral preparations for the treatment of OA / X. Zhu et al.
similar findings of the latest RCT (19).
A recent meta-analysis indicated that
celecoxib would lead to significant im-
provements in pain compared to place-
bo (35). Cao and colleagues combined
24 RCTs and indicated that oral 200mg
daily celecoxib was effective for pain
relief (36). The finding was similar to
our analysis. Machado and colleagues
conducted a pair-wise meta-analysis
and reported that acetaminophen had
a significant but small effect on hip
and/or knee OA patients compared to
placebo within 12 weeks(17). We also
found that acetaminophen was the least
efficacious drug when comprehensively
evaluated. Another network meta-anal-
ysis indicated that celecoxib was signif-
Fig. 2. The rank of efficacy of pain, function and stiffness. icantly superior to placebo but inferior
Data were pooled as the RR (relative risk) and its related 95% CI; G+C=glucosamine+ chondroitin. to acetaminophen, which was contrary
to our findings (30). In our study, dos-
Table II. Adverse event results. age was restricted and the RCTs includ-
Comparison RR (95%CI) ed met these criteria, and such results
could be comparable and reasonable.
Chondroitin vs. Glucosamine 1.67 (0.93,3.01) All of the treatments in our analysis were
G+C vs. Glucosamine 1.70 (0.86,3.37)
based on the recommendations from
Celecoxib vs. Glucosamine 1.82 (1.12,2.95)
Acetaminophen vs. Glucosamine 1.97 (1.11,3.52) the latest clinical practice guidelines.
Placebo vs. Glucosamine 1.05 (0.66,1.66) We compared typical SYSADOAs and
G+C vs. Chondroitin 1.02 (0.53,1.96) NSAIDs in the treatment of OA. Chon-
Celecoxib vs. Chondroitin 1.09 (0.69,1.72) droitin and glucosamine are believed
Acetaminophen vs. Chondroitin 1.18 (0.67,2.08)
to play a significant role in relieving
Placebo vs. Chondroitin 0.63 (0.41,0.96)
Celecoxib vs. G+C 1.07 (0.61,1.88) joint pain and slowing the rate of carti-
Acetaminophen vs. G+C 1.16 (0.59,2.29) lage loss. As shown in previous studies,
Placebo vs. G+C 0.62 (0.35,1.09) glucosamine inhibited prostaglandin
Acetaminophen vs. Celecoxib 1.08 (0.72,1.63) release, and chondroitin stimulated col-
Placebo vs. Celecoxib 0.58 (0.47,0.71)
lagen synthesis (37-39). However, the
Placebo vs. Acetaminophen 0.53 (0.36,0.78)
standard intervention focused on symp-
Data were pooled to obtain the relative risk and its related 95% CI; G+C: glucosamine+chondroitin. tom relief with analgesics and NSAIDs.
Presently, acetaminophen is the most
tion of glucosamine and chondroitin. pain and function from baseline infor- commonly prescribed over-the-counter
Acetaminophen is likely the least ef- mation. Conversely, a traditional meta- drug, and celecoxib was first specific
ficacious option. In terms of stiffness analysis suggested that glucosamine inhibitor of cyclo-oxygenase-2 (40).
improvement, glucosamine showed a and chondroitin can present a certain Indeed, previous meta-analyses have
superior effect compared with placebo, efficacy in treating OA symptoms (33, compared the use of SYSADOAs for
whereas acetaminophen did not signifi- 34). However, the findings of a Bayes- OA disease (16, 33). Several network
cantly differ from placebo. There was ian network meta-analysis indicated meta-analyses were estimated for knee
no significant difference of safety in that glucosamine, chondroitin and the OA but were only concerned about dif-
the comparisons between SYSADOAs combination of the two did not result in ferent NSAID treatments (16, 30, 41,
and placebo. Compared with placebo a relevant reduction of joint pain com- 42). Given the above reasons, we se-
and glucosamine, celecoxib and aceta- pared to placebo (16). The evidence lected and then conducted a more com-
minophen was a risk factor of AEs, of previous study was limited and the prehensive mixed comparison of those
whereas celecoxib and acetaminophen result may not be reliable, because treatments on knee and/or hip OA.
were recommended in clinical practice. only one RCT of combined group was SYSADOAs provide lasting pain relief
Our network meta-analysis indicated included. Nevertheless, in our study, and function improvement in OA treat-
that glucosamine and the combination four RCTs covering the combination ment (43, 44) and beneficial effects that
of glucosamine and chondroitin showed of glucosamine and chondroitin were develop slowly over time(45). Chon-
a greater significant improvement in measured, which could support the droitin and glucosamine were tested in
600 Clinical and Experimental Rheumatology 2018Efficacy of oral preparations for the treatment of OA / X. Zhu et al.
several clinical trials in osteoarthritis. results were validated by the model fit such as the combination of SYSADOAs
In spite of the controversy surrounding and absence of inconsistency. Funnel and NSAIDs were usual in clinical ex-
the SYSADOAs, they were commonly plots also showed no asymmetry, and perience; furthermore, our study will
used to control symptoms of OA in the risk of publication bias was not rec- help highlight the potential role of the
western countries. So, an understanding ognised. What is more, GRADE was glucosamine and chondroitin combina-
of chondroitin and glucosamine con- used to evaluate the quality of the evi- tion in the future. Therefore, the above
sumption is of significance for public dence, which provide a more compre- information, along with the safety pro-
health. The evidence in our study pre- hensive evidence-based review. file and relative costs of included treat-
sented that SYSADOAs have a compa- Some limitations must be acknowl- ment, should be conducive to clinicians
rable efficacy in both outcome of pain edged. Firstly, variation length of fol- when making care decisions tailored to
and function improvement, especially low-up time point might contribute to individual patient needs.
for the combination of glucosamine the evidence of significant heterogene-
and chondroitin. Furthermore, glucosa- ity. Fortunately, no obvious evidence References
mine seems greater in stiffness score of inconsistency was observed in this 1. ANDRIANAKOS AA, KONTELIS LK, KARAM-
ITSOS DG et al.: Prevalence of symptomatic
and much safer in terms of AEs. Given network meta-analysis. Secondly, the knee, hand, and hip osteoarthritis in Greece.
the reasons above, we do not oppose tolerability of specific kinds of AEs (di- The ESORDIG study. J Rheumatol 2006; 33:
the use of glucosamine and chondroi- arrhoea, abdominal pain, nausea, head- 2507-13.
tin, which were not recommended ac- ache) cannot be proven due to the inad- 2. FELSON DT, ZHANG Y: An update on the
epidemiology of knee and hip osteoarthritis
cording to the Osteoarthritis Research equate reporting of adverse event data. with a view to prevention. Arthritis Rheum
Society International (OARSI) guide- Thirdly, radiological grounds probably 1998; 41: 1343-55.
lines published in 2014. In fact, we mean more sensitivity and included 3. GLYN-JONES S, PALMER AJ, AGRICOLA R et
al.: Osteoarthritis. Lancet 2015; 386: 376-87.
recommend that the future guidelines mild cases (47). We were unable to con- 4. DALYs GBD, Collaborators H. Global, re-
reconsider the oral treatment option of duct subgroup analysis for OA grade gional, and national disability-adjusted life-
chondroitin and glucosamine for the because of original data restraints. years (DALYs) for 315 diseases and injuries
clinical treatment of OA. Considering Moreover, the results between the di- and healthy life expectancy (HALE), 1990-
2015: a systematic analysis for the Global
the aspect of safety, the current study rect and indirect comparisons identi- Burden of Disease Study 2015. Lancet 2016;
provides valuable information to help fied inconsistencies for pain (glucosa- 388: 1603-58.
physicians make treatment decisions mine vs. celecoxib and glucosamine vs. 5. NUESCH E, DIEPPE P, REICHENBACH S, WIL-
LIAMS S, IFF S, JUNI P: All cause and disease
for patients with OA. acetaminophen) and function (glucosa-
specific mortality in patients with knee or hip
Notably, a comprehensive and rigor- mine vs. celecoxib). This may be due osteoarthritis: population based cohort study.
ous literature search strategy was per- to the limited numbers of head-to-head BMJ 2011; 342: d1165.
formed in our network meta-analysis, comparisons between these interven- 6. CONTE A, VOLPI N, PALMIERI L, BAHOUS I,
RONCA G: Biochemical and pharmacokinetic
which insured that it was unlikely to tions. Researches among SYSADOAs aspects of oral treatment with chondroi-
miss other relevant trials. To mini- and NSAIDs are still required due to tin sulfate. Arzneimittelforschung 1995; 45:
mise bias, the study selection, quality the limitations on the quality and quan- 918-25.
assessment and data extraction were tity of the current available evidence. 7. PERSIANI S, ROTINI R, TRISOLINO G et al.:
Synovial and plasma glucosamine concentra-
completed independently by two re- tions in osteoarthritic patients following oral
viewers. Several sensitivity analyses of Conclusion crystalline glucosamine sulphate at therapeu-
RCTs with more than 100 patients per There were no obvious differences in tic dose. Osteoarthritis Cartilage 2007; 15:
764-72.
arm were conducted to make the results the results between the traditional meta-
8. BATTISTI WP, KATZ NP, WEAVER AL et al.:
more sensible and comprehensive. In analysis and the network meta-analysis. Pain management in osteoarthritis: a fo-
accordance with the pre-specified in- For the two typical options of NSAIDS, cus on onset of efficacy--a comparison of
clusion criteria, the articles included acetaminophen had a significant but rofecoxib, celecoxib, acetaminophen, and
nabumetone across four clinical trials. J Pain
in our study had achieved our expected small effect in patients with hip or knee 2004; 5: 511-20.
methodological quality. OA, whereas celecoxib was relatively 9. YANG S, EATON CB, McALINDON TE, LAP-
Unlike conventional meta-analyses, our outstanding. Glucosamine and chon- ANE KL: Effects of glucosamine and chon-
analysis integrated all available high- droitin were categorised as SYSADOAs droitin supplementation on knee osteoarthri-
tis: an analysis with marginal structural mod-
quality RCT evidence concerning typi- that provide lasting pain relief and func- els. Arthritis Rheumatol 2015; 67: 714-23.
cal oral medicines of SYSADOAs and tion improvement in OA. SYSADOAs 10. ZHANG W, NUKI G, MOSKOWITZ RW et al.:
NSAIDs to assess their effects on treat- are generally safe and well tolerated, in OARSI recommendations for the manage-
ment of hip and knee osteoarthritis: part
ing knee and/or hip OA. The integration view of the well-established beneficial
III: Changes in evidence following system-
of direct and indirect comparisons led effects of NSAIDs and SYSADOAs, atic cumulative update of research published
to a more precise outcome than a pair- long-term use of the combination of through January 2009. Osteoarthritis Carti-
wise meta-analysis (46). This method chondroitin and glucosamine should be lage 2010; 18: 476-99.
11. McALINDON TE, BANNURU RR, SULLIVAN
provided indirect effect estimate where given preference. MC et al.: OARSI guidelines for the non-
direct comparisons were not available. In fact, combination therapy is common surgical management of knee osteoarthritis.
The accuracy and robustness of the in practice. Treatment interventions Osteoarthritis Cartilage 2014; 22: 363-88.
Clinical and Experimental Rheumatology 2018 601Efficacy of oral preparations for the treatment of OA / X. Zhu et al.
12. CLEGG DO, REDA DJ, HARRIS CL et al.: statement on the suspension of the market- als. Medicine (Baltimore) 2016; 95: e3585.
Glucosamine, chondroitin sulfate, and the ing authorisation for Bextra (valdecoxib) in 36. ZENG C, WEI J, LI H et al.: Comparison be-
two in combination for painful knee osteo- the European Union [online].(2005) Avail- tween 200 mg QD and 100 mg BID oral
arthritis. N Engl J Med 2006; 354: 795-808. able at: http://www.ema.europa.eu/docs/ celecoxib in the treatment of knee or hip os-
13. FRANSEN M, AGALIOTIS M, NAIRN L et al.: en_GB/document_library/Public_state- teoarthritis. Sci Rep 2015; 5: 10593.
Glucosamine and chondroitin for knee osteo- ment/2009/12/WC500018391.pdf. (Date of 37. du SOUICH P: Absorption, distribution and
arthritis: a double-blind randomised placebo- access: 01/03/2015). mechanism of action of SYSADOAS. Phar-
controlled clinical trial evaluating single 24. Green JPTHaS. Corchrane Reviewers’ Hand- macol Ther 2014; 142: 362-74.
and combination regimens. Ann Rheum Dis book 5.1.0. Review Manage 2011. 38. CALAMIA V, RUIZ-ROMERO C, ROCHA B et
2015; 74: 851-8. 25. GUYATT GH, OXMAN AD, VIST GE et al.: al.: Pharmacoproteomic study of the effects
14. DATTO C, HELLMUND R, SIDDIQUI MK: GRADE: an emerging consensus on rating of chondroitin and glucosamine sulfate on
Efficacy and tolerability of naproxen/esome- quality of evidence and strength of recom- human articular chondrocytes. Arthritis Res
prazole magnesium tablets compared with mendations. BMJ 2008; 336: 924-6. Ther 2010; 12: R138.
non-specific NSAIDs and COX-2 inhibitors: 26. JUNI P, REICHENBACH S, DIEPPE P: Osteoar- 39. HENROTIN Y, LAMBERT C: Chondroitin and
a systematic review and network analyses. thritis: rational approach to treating the indi- glucosamine in the management of osteoar-
Open Access Rheumatol 2013; 5: 1-19. vidual. Best Pract Res Clin Rheumatol 2006; thritis: an update. Curr Rheumatol Rep 2013;
15. ESSEX MN, O’CONNELL MA, BEHAR R, BAO 20: 721-40. 15: 361.
W: Efficacy and safety of nonsteroidal anti-in- 27. JUHL C, LUND H, ROOS EM, ZHANG W, 40. McGETTIGAN P, HENRY D: Use of non-ste-
flammatory drugs in Asian patients with knee CHRISTENSEN R: A hierarchy of patient- roidal anti-inflammatory drugs that elevate
osteoarthritis: summary of a randomized, pla- reported outcomes for meta-analysis of knee cardiovascular risk: an examination of sales
cebo-controlled study. Int J Rheum Dis 2016; osteoarthritis trials: empirical evidence from and essential medicines lists in low-, middle-,
19: 262-70. a survey of high impact journals. Arthritis and high-income countries. PLoS Med 2013;
16. WANDEL S, JUNI P, TENDAL B et al.: Effects 2012; 2012: 136245. 10: e1001388.
of glucosamine, chondroitin, or placebo in 28. COOPER HM, HEDGES LV: The Handbook of 41. da COSTA BR, REICHENBACH S, KELLER N
patients with osteoarthritis of hip or knee: research synthesis. New York: Russell Sage et al.: Effectiveness of non-steroidal anti-in-
network meta-analysis. BMJ 2010; 341: Foundation, 1994: xvi, 573 p. flammatory drugs for the treatment of pain in
c4675. 29. COOPER HM, HEDGES LV, VALENTINE JC: knee and hip osteoarthritis: a network meta-
17. MACHADO GC, MAHER CG, FERREIRA PH The handbook of research synthesis and me- analysis. Lancet 2016; 387: 2093-105.
et al.: Efficacy and safety of paracetamol for ta-analysis. 2nd ed. New York: Russell Sage 42. KONGTHARVONSKUL J, WORATANARAT P,
spinal pain and osteoarthritis: systematic re- Foundation, 2009: xvi, 615 p. McEVOY M et al.: Efficacy of glucosamine
view and meta-analysis of randomised place- 30. BANNURU RR, SCHMID CH, KENT DM, plus diacerein versus monotherapy of gluco-
bo controlled trials. BMJ 2015; 350: h1225. VAYSBROT EE, WONG JB, McALINDON TE: samine: a double-blind, parallel randomized
18. PRIOR MJ, HARRISON DD, FRUSTACI ME: Comparative effectiveness of pharmacologic clinical trial. Arthritis Res Ther 2016; 18:
A randomized, double-blind, placebo-con- interventions for knee osteoarthritis: a sys- 233.
trolled 12 week trial of acetaminophen ex- tematic review and network meta-analysis. 43. MORREALE P, MANOPULO R, GALATI M,
tended release for the treatment of signs and Ann Intern Med 2015; 162: 46-54. BOCCANERA L, SAPONATI G, BOCCHI L:
symptoms of osteoarthritis. Curr Med Res 31. HE J, ENTSUAH R: A mixture model using Comparison of the antiinflammatory efficacy
Opin 2014; 30: 2377-87. likelihood-based and Bayesian approaches of chondroitin sulfate and diclofenac sodium
19. HOCHBERG MC, MARTEL-PELLETIER J, for identifying responders and non-respond- in patients with knee osteoarthritis. J Rheu-
MONFORT J et al.: Combined chondroitin sul- ers in longitudinal clinical trials. Pharm Stat matol 1996; 23: 1385-91.
fate and glucosamine for painful knee osteo- 2014; 13: 327-36. 44. HERRERO-BEAUMONT G, IVORRA JA, Del
arthritis: a multicentre, randomised, double- 32. YU J, HUTSON AD, SIDDIQUI AH, KEDRON CARMEN TRABADO M et al.: Glucosamine
blind, non-inferiority trial versus celecoxib. MA: Group sequential control of overall tox- sulfate in the treatment of knee osteoarthritis
Ann Rheum Dis 2016; 75: 37-44. icity incidents in clinical trials - non-Bayes- symptoms: a randomized, double-blind, pla-
20. THIJS V, LEMMENS R, FIEUWS S: Network ian and Bayesian approaches. Stat Methods cebo-controlled study using acetaminophen
meta-analysis: simultaneous meta-analysis of Med Res 2016; 25: 64-80. as a side comparator. Arthritis Rheum 2007;
common antiplatelet regimens after transient 33. DONOHOE M: Efficacy of glucosamine and 56: 555-67.
ischaemic attack or stroke. Eur Heart J 2008; chondroitin for treatment of osteoarthritis. 45. NOACK W, FISCHER M, FORSTER KK, ROVATI
29: 1086-92. JAMA 2000; 284: 1241; author reply 1242. LC, SETNIKAR I: Glucosamine sulfate in os-
21. HUTTON B, SALANTI G, CALDWELL DM et 34. RICHY F, BRUYERE O, ETHGEN O, CUCHER- teoarthritis of the knee. Osteoarthritis Carti-
al.: The PRISMA extension statement for AT M, HENROTIN Y, REGINSTER JY: Structur- lage 1994; 2: 51-9.
reporting of systematic reviews incorporat- al and symptomatic efficacy of glucosamine 46. LU G, ADES AE: Combination of direct and in-
ing network meta-analyses of health care in- and chondroitin in knee osteoarthritis: a com- direct evidence in mixed treatment compari-
terventions: checklist and explanations. Ann prehensive meta-analysis. Arch Intern Med sons. Stat Med 2004; 23: 3105-24.
Intern Med 2015; 162: 777-84. 2003; 163: 1514-22. 47. HART DJ, DOYLE DV, SPECTOR TD: Incidence
22. Tylenol (acetaminophen) professional pro- 35. XU C, GU K, YASEN Y, HOU Y: Efficacy and and risk factors for radiographic knee osteo-
ducted information. 2010. safety of celecoxib therapy in osteoarthritis: arthritis in middle-aged women: the Ching-
23. European Medicines Agency. EMEA public a meta-analysis of randomized controlled tri- ford Study. Arthritis Rheum 1999; 42: 17-24.
602 Clinical and Experimental Rheumatology 2018You can also read

















































