Cuidados post PCR adultos - Pablo Aguilera F Instructor adjunto Programa Medicina de Urgencia Curso de Reanimación 2012
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Cuidados post PCR
adultos
Pablo Aguilera F
Instructor adjunto
Programa Medicina de Urgencia
Curso de Reanimación 2012
www.urgenciauc.cl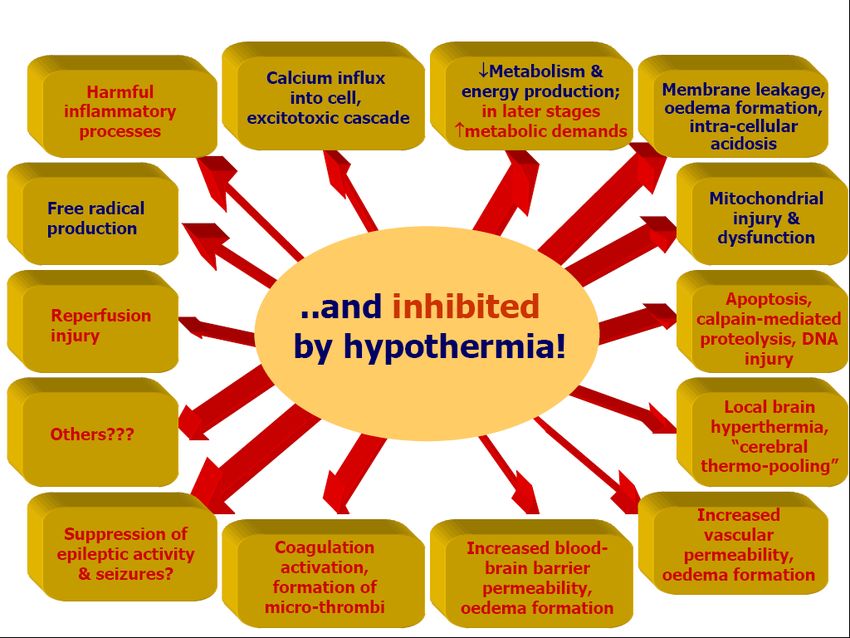
Cadena de sobrevida
Cuidados post PCR= Síndrome post PCR

Introducción • ¿Sirve de algo reanimar personas en PCR? • Mayores costos, baja sobrevida, escases de recursos. • Evolución en el tiempo... • Nuevas terapias específicas en sindrome post PCR
Introducción • “Enfermedad post reanimación”. • Acuñado por Dr.Vladimir Negovsky 1970 • 2008 nace término SPPCR guías ILCOR • “No sólo ROSC es importante sino secuelas funcionales” • Conceptos de reanimación cardiocerebral o CCR
Reanimación Cardiocerebral (CCR) • Representa una serie de de terapias específicas destinadas para mejorar la perfusión durante RCP. • Implementado en Wisconsin año 2003. • Particularmente útil en pacientes con PCR presenciado: Reserva funcional de O2
ordingly, is a arrest who receive prompt bystander resuscitation efforts.
U.S., as a cause Most bystanders who witness a cardiac arrest are willing to
ths combined alert EMS but are not willing to initiate bystander rescue
in 1974 (19), efforts because they are not willing to perform mouth-to-
elines in 1992
(7) for emer- Pilares CCR
mouth ventilation. Training and certification in basic life
Three Pillars of Cardiocerebral Resuscitation
CLS, with rare
HCA remains Table 1 Three Pillars of Cardiocerebral Resuscitation
rvival rates in 1. CCC (compression-only cardiopulmonary resuscitation) by anyone who
90; and in Los witnesses unexpected collapse with abnormal breathing (cardiac arrest).
gher than 1%, 2. Cardiocerebral resuscitation by emergency medical services (arriving during
circulatory phase of untreated ventricular fibrillation [e.g., !5 min])
l futility (22).
a. 200 CCCs (delay intubation, second person applies defibrillation pads and
e who receive initiates passive oxygen insufflation).
ose with rapid b. Single direct current shock if indicated without post-defibrillation pulse
ea et al. (29), check.
with witnessed c. 200 CCCs prior to pulse check or rhythm analysis.
ed their EMS d. Epinephrine (intravenous or intraosseous) as soon as possible.
mmediate chest e. Repeat (b) and (c) 3 times. Intubate if no return of spontaneous circulation
after 3 cycles.
alysis of post-
f. Continue resuscitation efforts with minimal interruptions of chest
recommended compressions until successful or pronounced dead.
% (29). 3. Post-resuscitation care to include mild hypothermia (32°C to 34°C) for
CPR has here- patients in coma post-arrest. Urgent cardiac catheterization and percutaneous
coronary intervention unless contraindicated.
nt pathophysi-
in which the CCC " continuous chest compression.Cardiocerebral resuscitation was begun in November 2003 11.
in Tucson, Arizona, and by 2007 was being used throughout
the majority of the state. In 2005, the AHA updated their
guidelines and incorporated some of the changes made with 12.
Por qué cambiar
CCR (52). In 2008, the AHA published a science advisory
statement supporting chest compressions only for bystander
response to adult cardiac arrest (71). Table 3 compares
13.
current aspects of CCR with the AHA 2005 guidelines and
conceptos?...
their 2008 advisory statement.
Uninterrupted perfusion to the heart and brain by CCC
14.
prior to defibrillation during cardiac arrest is essential to
JACCneurologically
Vol. 53, No. 2, normal
2009 survival. The low incidence of
n January 13, 2009:149–57
bystander-initiated resuscitation efforts in patients with cardiac 15.
arrest is a major public health problem. We have long advo-
cated CCC CPR by bystanders as a solution to this critical 16.
) oxygen (3). This is referred issue because eliminating mouth-to-mouth “rescue breathing”
will go a long way toward increasing the incidence of 17.
n. bystander-initiated resuscitation efforts. It is exciting to see that
ned in Figure 1. a technique (chest compression–only CPR) that had not been
heretofore formally taught results in the same or better neuro-
logically normal survival rates than those achieved with tech-
niques taught for decades. CCR also changes the approach of
those delivering ACLS. These changes resulted in dramatic
and Walworth counties in (250% to 300%) improvement in survival of patients most
18.
2004 (3). Using a historical likely to survive: those with witnessed cardiac arrest and
shockable rhythm. More aggressive post-resuscitation care, 19.
rs following the 2000 AHA including hypothermia and emergent cardiac catheterization 20.
atic increase in neurologically and PCI, is required to save even more victims of sudden
he mean survival to hospital cardiac arrest. 21.
c function was 15% in the 3 Reprint requests and correspondence: Dr. Gordon A. Ewy, 22.
year when CCR was provided University of Arizona Sarver Heart Center, University of Arizona
College of Medicine, Tucson, Arizona 85724. E-mail: gaewy@ 23.
all number of witnessed arrests aol.com.
ieve, suggesting a significant Neurologically Normal Survival of 24.
m et al. (5) 3-year experience Figure 2 Patients With Witnessed Out-of-Hospital
Cardiac Arrest and a Shockable RhythmREFERENCES
ted. Neurologic intact survival 25.
1. Ewy G. Cardiocerebral resuscitation: the new cardiopulmonary resus-
40% (including 1 patient who This figure contrasts the percent of patients with witnessed out-of-hospital car- 2005;111:2134 – 42.
citation. Circulation
2. Kern KB, Valenzuela TD, Clark LL, et al. An alternative approach to 26.
s, there may well have been a diac arrest and a shockable electrocardiographic rhythm upon arrival of emer-
advancing resuscitation science. Resuscitation 2005;64:261– 8.
gency medical services (EMS) who survived neurologically intact before MJ, Kennedy KW, Ewy GA. Cardiocerebral resuscitation
3. Kellum 27.
the first year. Nevertheless, in (cardiopulmonary resuscitation [CPR]) and after the institution ofimproves survival of patients with out-of-hospital cardiac arrest. Am J
cardiocerebral
essed cardiac arrest and shock- Med 2006;119:335– 40.
resuscitation (CCR). Of note is the fact that only 1 patient in the CCR group
aramedics, there was dramatic received hypothermia therapy post-resuscitation. The approach used by EMS
during the CPR period was that of the 2000 American Heart Association andFisiopatología • Componentes del SPPCR – Daño Cerebral post PCR – Disfunción Miocárdica post PCR – Respuesta Sistémica a isquemia/reperfusión – Persistencia de Patología precipitante de PCR
Isquemia global y reperfusión
10Neumar et al Post–Cardiac Arrest Syndrom
from 8% to 16%.22,23 Although this is clearly a po
Phase Goals
ROSC these patients can and should be considered
Immediate donation. A number of studies have reported no d
transplant outcomes whether the organs were ob
20 min
Limit ongoing injury
Early appropriately selected post– cardiac arrest patie
Prevent Recurrence
Organ support
other brain-dead donors.23–25 Non– heart-beating
tion has also been described after failed resuscitat
6-12 hours after in- and out-of-hospital cardiac arrest,26,27 bu
Intermediate generally been cases in which sustained ROSC
achieved. The proportion of cardiac arrest patie
the critical care unit and who might be suitable
beating donors has not been documented.
Despite variability in reporting techniques,
72 hours
Prognostication
little evidence exists to suggest that the in-hospi
rate of patients who achieve ROSC after cardia
changed significantly in the past half-century. T
Recovery artifactual variability, epidemiological and in
post– cardiac arrest studies should incorporate w
standardized methods to calculate and report mo
at various stages of post– cardiac arrest care,
long-term neurological outcome.16 Overriding th
a growing body of evidence that post– cardiac
impacts mortality rate and functional outcome.
Disposition
Rehabilitation
Rehabilitation IV. Pathophysiology of Post–Car
Arrest Syndrome
The high mortality rate of patients who initia
ROSC after cardiac arrest can be attributed t
pathophysiological process that involves mult
Although prolonged whole-body ischemia init
Figure. Phases of post– cardiac arrest syndrome. global tissue and organ injury, additional dam
during and after reperfusion.28,29 The unique
51 children who survived out-of-hospital cardiac arrest had post– cardiac arrest pathophysiology are often su
either pediatric CPC 1 to 2 or returned to their baseline on the disease or injury that caused the cardiac ar
neurological state.20 The CPC is an important and useful as underlying comorbidities. Therapies that focus
outcome tool, but it lacks the sensitivity to detect clinically ual organs may compromise other injured organ sObjetivos generales del
manejo
• Mantener adecuada oxigenación.
• Mantener perfusión de órganos
• Soporte de sistemas dañados
• Resolución de causa de baseGlobal ischemia-reperfusion
injury
post-resuscitation disease
Ischemia
VF = ventricular fibrillation
ROSC= return of spontaneous circulation
13Table 1. Post–Cardiac Arrest Syndrome: Pathophysiology, Clinical Manifestations, and Potential Treatments
Syndrome Pathophysiology Clinical Manifestation Potential Treatments
Post– cardiac arrest brain ● Impaired cerebrovascular ● Coma ● Therapeutic hypothermia177
injury autoregulation ● Seizures ● Early hemodynamic
● Cerebral edema (limited) ● Myoclonus optimization
● Postischemic ● Cognitive dysfunction ● Airway protection and
neurodegeneration ● Persistent vegetative state mechanical ventilation
● Secondary Parkinsonism ● Seizure control
● Cortical stroke ● Controlled reoxygenation
● Spinal stroke (SaO2 94% to 96%)
● Brain death ● Supportive care
Post–cardiac arrest myocardial ● Global hypokinesis ● Reduced cardiac output ● Early revascularization of
171, 373
dysfunction (myocardial stunning) ● Hypotension AMI
● ACS ● Dysrhythmias ● Early hemodynamic
● Cardiovascular collapse optimization
● Intravenous fluid97
● Inotropes97
● IABP13,160
● LVAD161
● ECMO361
Systemic ischemia/reperfusion ● Systemic inflammatory ● Ongoing tissue hypoxia/ischemia ● Early hemodynamic
response response syndrome ● Hypotension optimization
● Impaired vasoregulation ● Cardiovascular collapse ● Intravenous fluid
● Increased coagulation ● Pyrexia (fever) ● Vasopressors
● Adrenal suppression ● Hyperglycemia ● High-volume hemofiltration374
● Impaired tissue oxygen ● Multiorgan failure ● Temperature control
delivery and utilization ● Infection ● Glucose control223,224
● Impaired resistance to ● Antibiotics for documented
infection infection
Persistent precipitating ● Cardiovascular disease ● Specific to cause but complicated ● Disease-specific interventions
pathology (AMI/ACS, by concomitant PCAS guided by patient condition
cardiomyopathy) and concomitant PCAS
● Pulmonary disease
(COPD, asthma)
● CNS disease (CVA)
● Thromboembolic disease
(PE)
● Toxicological (overdose,
poisoning)
● Infection (sepsis,
pneumonia)
● Hypovolemia
(hemorrhage,
dehydration)
AMI indicates acute myocardial infarction; ACS, acute coronary syndrome; IABP, intra-aortic balloon pump; LVAD, left ventricular assist device; EMCO, extracorporeal
membrane oxygenation; COPD, chronic obstructive pulmonary disease; CNS, central nervous system; CVA, cerebrovascular accident; PE, pulmonary embolism; and
PCAS, post– cardiac arrest syndrome.
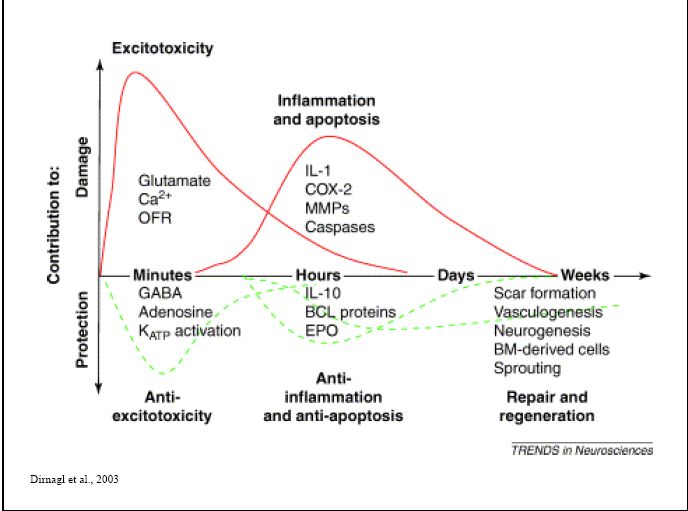
excitotoxicity, disrupted calcium homeostasis, free radical Prolonged cardiac arrest can also be followed by fixed orDaño cerebral post PCR • Causa frecuente de morbi-mortalidad de pacientes. • En algunos trabajos es la causa de un 70% de mortalidad. • Causa: Mala tolerancia a la isquemia y respuesta a la reperfusión.
Daño cerebral post PCR • Mecanismos involucrados complejos: • Toxicidad por neuromediadores • Dis-regulación de la homeostasis del calcio • Formación de radicales libres • Activación de cascadas de proteasas • Activación de mecanismos apoptóticos
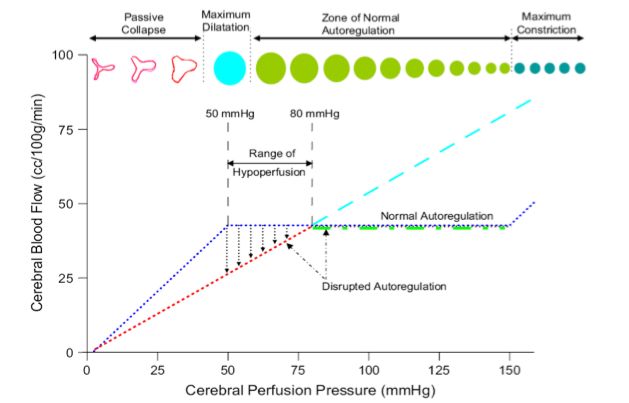
Daño cerebral post PCR • Se altera la auto-regulación de flujo cerebral. • Infartos e isquemia en regiones cerebrales. • Trombosis microvascular. • Más significativo si PCR es prolongado • Reperfusión hiperémica como causal de daño y edema.
Edema
Rango de
perfusión
FSC (ml/100gr/min
Hipotenso normal
Hipertenso
Isquemia
PAM (mm Hg)Brain injury after cardiac arrest
4 min 4-10 min > 10 min
Duration of CA
Electrical Circulatory Metabolic
Electrical & Circulatory reduction of the
duration of global ischemia (primary brain
injury)
Metabolic attenuation of post-resuscitation
disease due to reperfusion injury (secondary
brain injury)
4Hypothermia after cardiac arrest
Hipotermia terapéutica
a treatment that after
Hypothermia cardiac arrest
works !
a treatment that works !
number needed to treat : 6
Curr Opin Crit Care, 2003;9:205
Crit Care Med, 2005;33(2):414
number needed to treat : 6
30
Curr Opin Crit Care, 2003;9:205
Crit Care Med, 2005;33(2):414 30Hipotermia terapéutica • Trabajos RCT 2002 • Australiano y Europeo • Hipotermia Leve ( 32-34 grados).
36
36Crit Care Med 2004
25Enfermedad post
Reanimación
hipotermia
26Hypothermia after cardiac arrest
a treatment that works !
* * * * * *
529529
patients involved
pacientes in 6 studies
en 6 estudios 29Therapeutic hypothermia
duration of cardiac arrest
Irrespective to the presence of shock or the
initial rhythm, the predicted benefit of
hypothermia is strongly dependent on
the duration of cardiac arrest
27
Oddo M, Crit Care Med, 2006;34(7):1865Protocolo0de0Hipotermia0Inducida Protocolo Hipotermia UC
Medicina0de0UrgenciaV0Unidad0de0Cuidados0Intensivos0PUC
Nombre: Fecha: Rut: Rut:
•Paro Cardiorrespiratorio (cualquier ritmo, cualquier lugar)
Hora0Inicio: Lugar0inicio0de0hipotermia:00UCI0000000000000URGENCIA
en paciente mayores 15 años.
Criterios0de0Inclusión0(debe0cumplir0todos) Criterios0de0Exclusión •Duración maniobras resucitación < 45 minutos. Evaluar
Post0PCR0(cualquier0ritmo0como0causa0es0eligible) Orden0de0no0reanimar,0status0basal0pobre,0enfermedad0 •Retorno a circulación espontanea (RCE)
Criterios
0Duración0maniobras0menos0300min0hasta0 terminal Exclusión
(En Hoja
recuperación0pulso. Hemorragia0intracerebral0acRva •Paciente en coma Protocolo)
Menos0de060horas0desde0recuperación0pulso0hasta0el0 PCR0de0eRología0traumáRca
minuto. Crioglobulinemia
Comatoso0(0no0obedece0órdenes) Embarazo0(relaRva/0consulta0gineVobs)
PAM0>0650con0no0más0de0un0vasopresor. Cirugía0Mayor0reciente0(relaRva) Ingresar en
Sepsis0como0causa0PCR0(0relaRva) Paciente candidato Hipotermia carpeta
Hipotermia
Examen0neurológico
Apertura(ocular((((((((((((((((Verbal(((((((((((((((((((((((((((((((((((Motor(((((((((((((((((((((((((((((Troncoencéfalo
Espontánea0…..000*00000000000Orientado………000*00000000000000Obedece…….000000000000000000Pupilas0reacRvas0000000000000000SI00000000NO000000000000000 Registrar Historia Clínica
Voz……………….0 0*00000000000Confuso…………00.0*00000000000000Localiza……….00000000000000000Corneales0000000000000000000000000000SI00000000NO0 Discutir -Avisar a equipo
Protocolo Con
Monitorización
Dolor0……………0 00000000000000Inapropiada……00000000000000000000ReRra………….00000000000000000Respiración0espontánea000SI00000000NO0 Hipotermia
Ninguna………..00000000000000000Sonidos…………..0000000000000000000DecorRca…….00000000000000000Ojos0de0Muñeca0000000000000000SI00000000NO0 Familiares (según protocolo)
0 00000000000000Ninguno…………..000000000000000000Descerebra… Exámenes iníciales - Solicitar cama UCI
0 00000000000000Intubado0………..0000000000000000000Ninguno………
ROT00000000000000000000000000000000000Bicipital00I000D0000000000000000000000000Rotuliano00000I0000000D000000000Aquiliano00000000000I000000D
Indicar0fármacos0sedantes0o0Relajantes0musculares0al0momento0del0examen
Item(que(presente((*)(excluye(paciente(de(protocolo
Protocolo Traslado
Iden>ficar(caso(elegible.(Ac>var(equipo(hipotermia(UrgenciaEUCI.
1. DiscuRr0caso0con0residente0de0UCI0o0staff0(0deben0estar0de0acuerdo0con0la0hipotermia0y0debe0haber0cama0de0UCI0disponible0en0las0
UCI Inicio de Hipotermia
siguientes0horas)0.0Evaluar0causas0eRológicas0PCR0,0evaluar0necesidad0de0acRvación0hemodinamia.
2. ECG0y00eventual0Ecocardiograca00por0cardiología.
3. Hora0discusión:0______________0.0Si0paciente0no0es0elegible0por0UCI,00indique0razón0_____________________________000
4. Enviar0exámenes0de0sangre0con:0ELPV0CELLDYNV0COAGULACIÓNV0LACTATO0VENOSOV0GASES0VENOSOSV0ENZIMAS0CARDÍACASV0LIPASAV0
AMILASAVCLASIFICACIÓN
5. 20Vías0venosas0periféricas0gruesas
6. Foley0y0medir0diuresis0
7. Exponer0paciente0completamente
Sedación y Control
Temperatura
8. Preparar0para0monitoreo0hemodinámico0invasivo0en0servicio0de0urgencia relajo laboratorio
9. Registrar0temperatura0corporal0rectal0o0esofágica:0_______________ central 33°C según protocolo
Muscular
10. Preparar0sedación0con0midazolam0–fentanyl.0Para0SAS0score001V2
11. Inicio0infusión0de0SF00,9%0a04°C0.0Máximo0bolo030cc/kg0.0Velocidad0infusión00~1000ml/min0con0apuradores0de0suero0.0Hora0_______
12. Si0temperatura0inicial0es000800Rtular00con0norV0adrenalina__________________________0000Dosis0máxima0:_______________________
0
Notas: Aguilera, Alvizú et al
Notas:Disfunción Miocárdica post
RCP
• “Stunning” miocárdico
• Disfunción transitoria
• IC menor a 2
• 48- 72 horas de duración
• Enfermedad coronaria asociada
• Reperfusión precoz en todos los pacientesReperfusión Miocárdica
• Protocolo intervencional
• Hipotermia + angiografía precoz
•
JACC Vol. 53, No. 2, 2009 Ewy and Kern 157
68 pacientes
January 13, 2009:149–57 Cardiocerebral Resuscitation
•
28. Bohm K, Rosenqvist M, Herlitz J, Hollenberg J, Svensson L. Survival 50. Wik L, Hansen TB, Fylling F, et al. Delaying defibrillation to give
15 vivos
is similar after standard treatment and chest compression only in
out-of-hospital bystander cardiopulmonary resuscitation. Circulation
basic cardiopulmonary resuscitation to patients with out-of-hospital
ventricular fibrillation: a randomized trial. JAMA 2003;289:1389 –95.
2007;116:2908 –12. 51. Wik L, Kramer-Johansen J, Myklebust H, et al. Quality of cardiopul-
•
29. Rea TD, Helbock M, Perry S, et al. Increasing use of cardiopulmonary monary resuscitation during out-of-hospital cardiac arrest. JAMA
96% tenían lesiones coronarias
resuscitation during out-of-hospital ventricular fibrillation arrest: sur-
vival implications of guideline changes. Circulation 2006;114:2760 –5.
2005;293:299 –304.
52. International Liaison Committee on Resuscitation. 2005 international
30. Steen S, Liao Q, Pierre L, Paskevicius A, Sjöberg T. The critical consensus on cardiopulmonary resuscitation and emergency cardiovas-
• importance of minimal delay between chest compressions and subse- cular care science with treatment recommendations. Resuscitation
82% con lesiones criticas
quent defibrillation: a haemodynamic explanation. Resuscitation 2003;
58:249 –58.
2005;67:181–341.
53. Aufderheide T, Sigurdsson G, Pirrallo R, et al. Hyperventilation-
31. Becker L, Berg R, Pepe P, et al. A reappraisal of mouth-to-mouth induced hypotension during cardiopulmonary resuscitation. Circula-
•
tion 2004;109:1960 –5.
OR 27
ventilation during bystander-initiated cardiopulmonary resuscitation. A
statement for healthcare professionals from the Ventilation Working
Group of the Basic Life Support and Pediatric Life Support Subcommit-
54. Aufderheide TP. The problem with and benefit of ventilations: should
our approach be the same in cardiac and respiratory arrest? Curr Opin
tees, American Heart Association. Circulation 1997;96:2102–12. Crit Care 2006;12:207–12.
55. Schoenenberger RA, von Planta M, von Planta I. Survival after failed
32. Standards and guidelines for cardiopulmonary resuscitation (CPR) and
out-of-hospital resuscitation. Are further therapeutic efforts in the
emergency cardiac care (ECC). JAMA 1986;255:2905– 89.
emergency department futile? Arch Intern Med 1994;154:2433–7.
33. SOS-KANTO Study Group. Cardiopulmonary resuscitation by by-
56. Sunde K, Pytte M, Jacobsen D, et al. Implementation of a standardised
standers with chest compression only (SOS-KANTO): an observa- treatment protocol for post resuscitation care after out-of-hospital
tional study. Lancet 2007;369:920 – 6. cardiac arrest. Resuscitation 2007;73:29 –39.
34. Ewy GA. Cardiac arrest— guideline changes urgently needed. Lancet 57. Hypothermia after Cardiac Arrest Study Group. Mild hypothermia to
2007;369:882– 4. improve the neurologic outcome after cardiac arrest. N Engl J Med
35. Abella BS, Aufderheide TP, Eigel B, et al. Reducing barriers for 2002;346:549 –56.
implementation of bystander-initiated cardiopulmonary resuscitation. ARespuesta sistémica a isquemia/reperfusión • Estado de Shock más severo • RCP suple la necesidad de manera parcial y muchas veces precaria. • Se activan cascadas inmunológicas y de coagulación que incrementan las infecciones y disfunciones.
Respuesta sistémica a isquemia/reperfusión • Micro trombosis • SIRS post ROSC • Terapia orientada por metas
Persistencia de patología precipitante de PCR • SCA • Enfermedades pulmonares • Hemorragia • Sepsis • Toxidromes • Alteraciones HEL • Otras
Estrategias terapéuticas • Monitoreo estricto • Optimización hemodinámica precoz guiada por metas. • Oxigenación • Ventilación • Soporte Circulatorio. • Manejo SCA
Estrategias terapéuticas • Sedación y RNM • Manejo de convulsiones • Control glicemia • Neuroprotección farmacológica. • Disfunción Adrenal. • Falla Renal
Cuidados post PCR en situaciones especiales • Post hipotermia • Post trombolisis • Etc etc etc etc.
Pronósticos • No existen protocolos de pronósticos establecido • Predicción Multimodal pareciera ser lo mejor. • No es útil los criterios clásicos
Neumar et al Post–Cardiac Arrest Syndrom
from 8% to 16%.22,23 Although this is clearly a po
Phase Goals
ROSC these patients can and should be considered
Immediate donation. A number of studies have reported no d
transplant outcomes whether the organs were ob
20 min
Limit ongoing injury
Early appropriately selected post– cardiac arrest patie
Prevent Recurrence
Organ support
other brain-dead donors.23–25 Non– heart-beating
tion has also been described after failed resuscitat
6-12 hours after in- and out-of-hospital cardiac arrest,26,27 bu
Intermediate generally been cases in which sustained ROSC
achieved. The proportion of cardiac arrest patie
the critical care unit and who might be suitable
beating donors has not been documented.
Despite variability in reporting techniques,
72 hours
Prognostication
little evidence exists to suggest that the in-hospi
rate of patients who achieve ROSC after cardia
changed significantly in the past half-century. T
Recovery artifactual variability, epidemiological and in
post– cardiac arrest studies should incorporate w
standardized methods to calculate and report mo
at various stages of post– cardiac arrest care,
long-term neurological outcome.16 Overriding th
a growing body of evidence that post– cardiac
impacts mortality rate and functional outcome.
Disposition
Rehabilitation
Rehabilitation IV. Pathophysiology of Post–Car
Arrest Syndrome
The high mortality rate of patients who initia
ROSC after cardiac arrest can be attributed t
pathophysiological process that involves mult
Although prolonged whole-body ischemia init
Figure. Phases of post– cardiac arrest syndrome. global tissue and organ injury, additional dam
during and after reperfusion.28,29 The unique
51 children who survived out-of-hospital cardiac arrest had post– cardiac arrest pathophysiology are often su
either pediatric CPC 1 to 2 or returned to their baseline on the disease or injury that caused the cardiac ar
neurological state.20 The CPC is an important and useful as underlying comorbidities. Therapies that focus
outcome tool, but it lacks the sensitivity to detect clinically ual organs may compromise other injured organ sPost-Cardiac Arrest Syndrome Management
Who needs this? Getting Started:
Algoritmo propuesto!
Resuscitated patients with: Stat ECG, echocardiogram, & cardiology consult (Please see TH
GCS Motor score < 6 protocol for instructions regarding Stat ECG, Echo & Cards consult)
No other reason for coma Stat head CT if deemed medically necessary
Initiate therapeutic hypothermia (TH) & place radial or femoral a-line
Not DNR B/C or DNI status
Insert PreSep® CVC in subclavian or internal jugular vein
Notify Super SAR for ICU bed and EEG fellow for EEG
If pregnant, consult Ob/Gyn
Use 2 liters of 4 C saline < 80 > 100
(peripheral IV preferred) if
MAP
initiating TH
500 ml IVF over 5 min q 20
min until CVP > 8
If no CHF, continue IVF to get
CVP > 8 > 80
MAP > 80, CVP > 8, but < 20
PA catheter if CVP >15 or > 5
liters IVF or CHF or
significant vasopressor need
< 80
Start IV NTG at 10 mcg/min. Titrate to
MAP < 100. Assure adequate CVP
If EF is normal, use Norepinephrine (1-20 mcg/min) Consider Furosemide if CHF
If EF, start Dobutamine (2.5-20 mcg/kg/min); If If tachycardic or ACS* w/ normal EF &
MAP , add Norepinephrine Scv02 then consider Esmolol
Ongoing hypotension, consider 2nd vasopressor
If severe hypotension-> IABP
80-100
(Consider > 65 if ACS*, CHF, Shock)
Yes No
ScvO2 65%
If evidence of shock is present:
Optimize CVP if not already done (up to 20)
Transfuse PRBC’s if hemoglobin 10 mg/dL
Dobutamine if not already initiated
Consider RHC if CVP>15 or escalating vasopressors
No ScvO2You can also read

















































