Current and Future Perspectives in the Treatment of High risk MDS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Current and Future Perspectives in the Treatment of High‐risk MDS
Current and Future Perspectives in the
Treatment of High‐risk MDS
Richard Stone, MD
Professor of Medicine
Harvard Medical School
Chief of Staff
Director, Adult Acute Leukemia Program
Dana‐Farber Cancer Institute
Boston, Massachusetts
Welcome to Managing MDS. I am Dr. Richard Stone, and today, I'm going to discuss the
current and future perspectives in the treatment of high‐risk myelodysplastic syndromes.
©2021 MediCom Worldwide, Inc. 1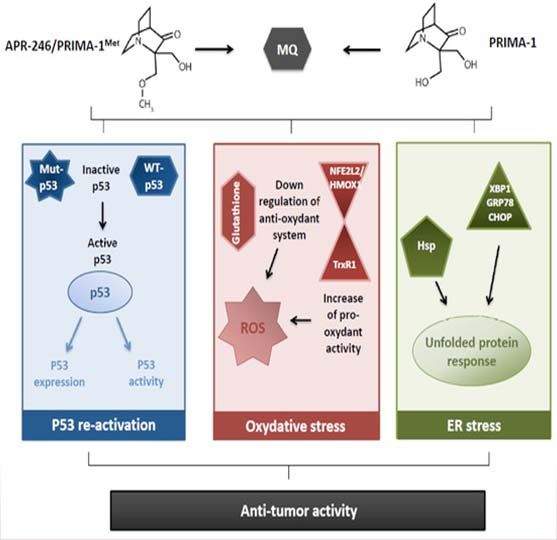
Current and Future Perspectives in the Treatment of High‐risk MDS
Disclosures
• Dr. Richard Stone has received honoraria as a consultant from AbbVie Inc.,
Agios, Amgen Inc., Arginex, Arog Pharmaceuticals, Inc., Astellas Pharma US,
Inc., Celator Pharmaceuticals, Inc., Celgene Corporation, Cornerstone
Therapeutics Inc., Fujifilm Corporation, Janssen Pharmaceuticals, Inc., Jazz
Pharmaceuticals plc, Novartis AG, Orsenix, LLC, Otsuka Pharmaceutical Co.,
Ltd., and Pfizer Inc.; as well as honoraria related to formal advisory activities
from Actinium Pharmaceuticals, Inc. He has received grant support related to
research activities from Agios, Arog, and Novartis. He has also disclosed he is
a steering committee and data safety monitoring board (DSMB) member of
Celgene and board member of Actinium.
Here are my disclosures.
©2021 MediCom Worldwide, Inc. 2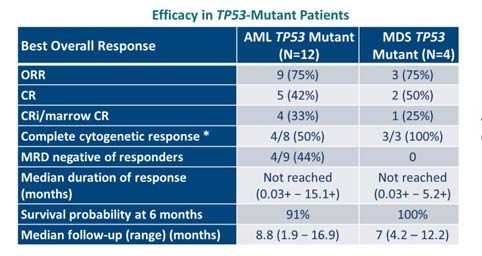
Current and Future Perspectives in the Treatment of High‐risk MDS
Myelodysplastic Syndromes: Outline
Genetics and prognosis
• Therapy of lower‐risk disease
– Lenalidomide in 5q‐
– Erythropoietin (EPO) +/‐ G‐CSF; lenalidomide + EPO
– Luspatercept*
Maybe: low‐dose hypomethylating agent (HMA), iron chelation
Horizon: roxadustat
• Therapy of higher‐risk disease
– HMA (including now: oral decitabine/cytidine deaminase inhibitor=ASTX727),* alloSCT if
possible, remains the standard
Maybe: add venetoclax, IDH inhibitor
Horizon: TP53 refolding, Anti‐CD47, CPI
*Luspatercept approved by the FDA April 2020; oral decitabine/cytidine approved by the FDA July 2020
The outline of my talk is going to center on high‐risk disease, but just briefly to mention on
low‐risk disease, we still use lenalidomide in 5q‐ patients. We use growth factors in non‐5q‐
low‐risk patients. We have a new drug called luspatercept to be used in patients who have
SF3B1 mutations or ring sideroblasts who have failed erythropoietin. In high‐risk disease
which I'll cover extensively today, the backbone is still hypomethylating agent therapy,
either IV or subQ azacitidine, IV decitabine, or now we have the oral decitabine/cytidine
deaminase inhibitor, a new drug which can be orally used. We transplant patients if
possible with high‐risk disease. We have some new therapies that are exciting to talk about
including the addition of venetoclax, TP53 refolding agents, anti‐CD47 antibodies, and
checkpoint inhibitors.
©2021 MediCom Worldwide, Inc. 3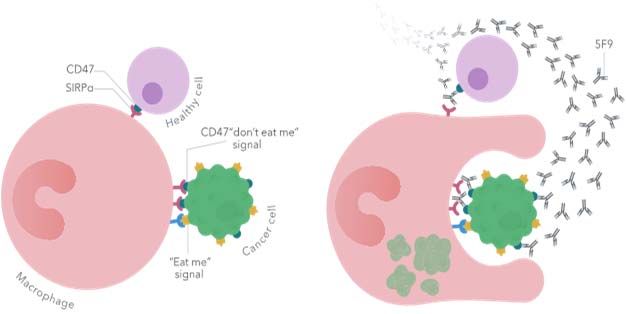
Current and Future Perspectives in the Treatment of High‐risk MDS
Risk Assessment in Myelodysplastic Syndromes
Key Information for MDS Risk Assessment in 2021
Host Factors
• Age
• Comorbid conditions
• Performance status
Disease Factors
• Proportion of marrow blasts
• Number and degree of peripheral blood cytopenias
• Cytogenetics/karyotype
• Transfusion burden
• Other marrow features: presence of heavy marrow fibrosis, ring sideroblasts (if low risk/
only anemic – to distinguish RA from RARS)
While not yet routinely part of risk assessment,
molecular features will become critical soon
Naqvi K, et al. J Clin Oncol. 2011;29(16):2240‐2246.
Now, when a patient comes in with possible MDS, we'd like to know their age, comorbid
status, performance status, disease factors including the proportion of marrow blasts,
cytopenias ‐ how many they have, cytogenetics ‐ if they're getting transfusions of the
marrow features, particularly ring sideroblasts and fibrosis, and while not yet routinely part
of risk assessment, molecular features will become critical soon, no doubt.
©2021 MediCom Worldwide, Inc. 4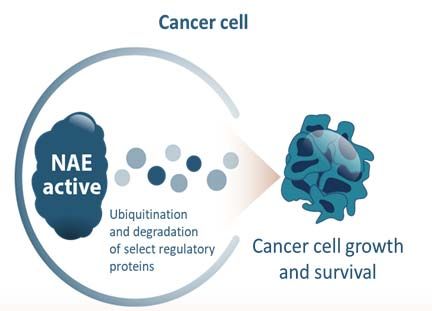
Current and Future Perspectives in the Treatment of High‐risk MDS
International Prognostic Scoring System (IPSS)
(1997) Risk Stratification
Score
Prognostic Variable 0 0.5 1.0 1.5 2.0
Marrow blasts (%) < 5% 5%‐10% ‐‐ 11%‐20% 21%‐30%
Karyotype class* Good Intermediate Poor ‐‐ ‐‐
# of cytopenias** 0 or 1 2 or 3 ‐‐ ‐‐ ‐‐
* Karyotype class: Good = normal, ‐Y, del(5q) alone, del(20q) alone; Poor = chromosome 7 abnormalities or complex; Intermediate = other karyotypes;
** Cytopenias: Hb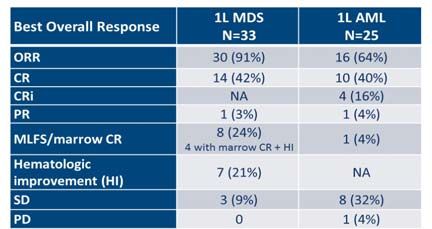
Current and Future Perspectives in the Treatment of High‐risk MDS
IPSS‐R
% pts (n=7,012; Median Median survival for Time until 25% of pts
Risk group Points
AML data on 6,485) survival, years pts under 60 years develop AML, years
Very low 0‐1.5 19% 8.8 Not reached Not reached
Low 2.0‐3.0 38% 5.3 8.8 10.8
Intermediate 3.5‐4.5 20% 3.0 5.2 3.2
High 5.0‐6.0 13% 1.5 2.1 1.4
Very high >6.0 10% 0.8 0.9 0.7
Based on cytogenetics, marrow blasts, hgb, ANC, plt
Using IPSS‐R:
27% of IPSS lower risk “upstaged”
18% of IPSS higher risk “downstaged”
Greenberg P, et al. Blood. 2012;120(12):2454‐2465.
A more exact but, unfortunately, a system which has five subcategories which is not
divisible by two, so we have to think about what to do with the intermediate groups is a
little bit more heavily weighted on the platelet count and all the cytogenetics and divides
folks, as I mentioned, into four subcategories, two of which are clearly high‐risk, and one of
which is sort of high‐risk intermediate.
©2021 MediCom Worldwide, Inc. 6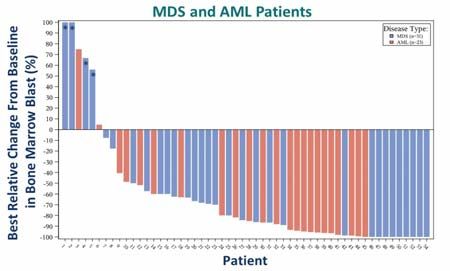
Current and Future Perspectives in the Treatment of High‐risk MDS
Impact of Mutations by IPSS Group
1.0 1.0
0.9 IPSS Low (n=110) 0.9 IPSS Low
IPSS Mut Absent
Low (n=87)
(n=110)
IPSS Int1 (n=185) IPSS Low Mut Present (n=23)
TP53 0.8 IPSS Int2 (n=101) 0.8 p < 0.001
0.7 IPSS High (n=32) 0.7 IPSS Int1 (n=185)
Overall Survival 0.6 0.6
Overall Survival
0.5 0.5
ETV6 0.4 0.4
0.3 0.3
0.2 0.2
0.1 0.1
0.0 0.0
ASXL1 0 1 2 3 4 5 6
Years
7 8 9 10 11 12 13 0 1 2 3 4 5 6
Years
7 8 9 10 11 12 13
1.0 1.0
0.9 IPSS Int1 Mut Absent (n=128) 0.9 IPSS Int2 Mut Absent (n=61)
IPSS Int1 Mut Present (n=57) IPSS Int2 Mut Present (n=40)
0.8 p < 0.001 0.8 p = 0.02
0.7 IPSS Int2 (n=101) 0.7 IPSS High (n=32)
EZH2 0.6 0.6
Overall Survival
Overall Survival
0.5 0.5
0.4 0.4
0.3 0.3
0.2 0.2
RUNX1 0.1 0.1
0.0 0.0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 0 1 2 3 4 5 6 7 8 9 10 11 12 13
Years Years
Bejar R, et al. N Engl J Med. 2011;364(26):2496‐2506.
We know now over a decade ago, my colleague, Ralph Bejar, did an important study where
he showed that the mutational spectrum will influence the prognosis. Namely, if you have
one of these five mutations in the left‐hand side of the slide, your prognosis slips by at least
one IPSS group.
©2021 MediCom Worldwide, Inc. 7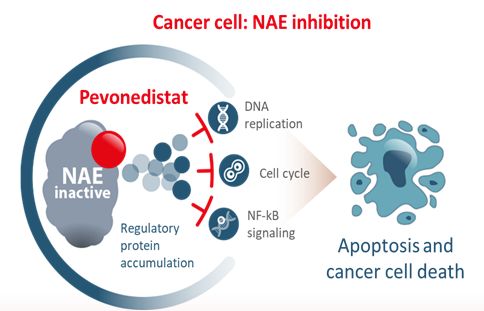
Current and Future Perspectives in the Treatment of High‐risk MDS
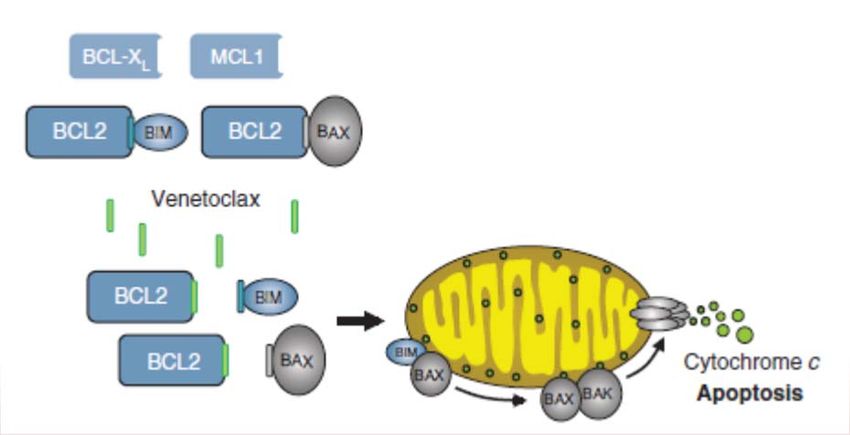
Venetoclax: BCL‐2 Selective Inhibitor
BCL‐2 overexpression allows cancer cells to evade
apoptosis by sequestering pro‐apoptotic proteins
Venetoclax binds to BCL‐2, freeing pro‐
apoptotic proteins that initiate apoptosis
Konopleva M, et al. Cancer Discov. 2016;6(10):1106‐1117. Permission request pending.
Now, we're going to talk about venetoclax a great deal. I just wanted to mention how it
works. It's a BCL‐2 inhibitor, and BCL‐2 is responsible for preventing program cell death or
apoptosis caused by cytotoxic stress such as chemotherapy or radiation therapy. The way
BCL‐2 works, it binds to these core makers in the mitochondrial cell membrane called Bim
and Bax. If you have a BCL‐2 inhibitor like venetoclax, the BCL‐2 cannot prevent pores from
being formed by Bim and Bax.
©2021 MediCom Worldwide, Inc. 8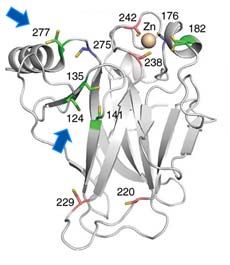
Current and Future Perspectives in the Treatment of High‐risk MDS
MDS: Novel Promising Strategies
APR‐246 for p53 mutant AML Anti‐CD47 antibody (5F9)
macrophage phagocytosis
Hu5F9‐G4 Mechanism of Ac on
Healthy
cell 5F9
CD47
SIFα
SIFα
Don’t Tumor cell
Macrophage
eat me CD47
signal
Tumor cell
Eat me
signal
Schurch CM. Front Oncol. 2018;8:152. Permission request pending.
A couple of other molecules I'll be talking about today. APR‐246, which is a so‐called P53
refolding agent, which works in this horrendous subtype of MDS with AML called P53
disease. A very exciting group of molecules called anti‐CD47 antibodies which cover up the
so‐called "don't eat me" signal on the surface of the MDS cell and allow the macrophages
to eat or kill the noxious cell.
©2021 MediCom Worldwide, Inc. 9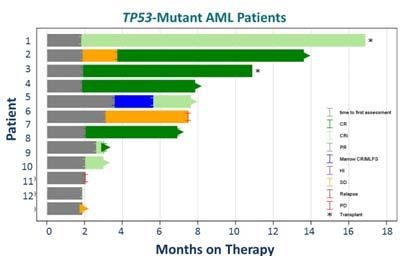
Current and Future Perspectives in the Treatment of High‐risk MDS
Introduction to Venetoclax + HMA in MDS
• 30% of MDS have intermediate‐2/high IPSS risk disease (median OS 0.4‐1.2 years)1
• Azacitidine (Aza) has been the standard of care for higher‐risk MDS based on AZA‐001 showing
median OS of 24.5 mo c/w doctor’s choice ‐9.4 mo2
– CR (17%), PR (12%), HI‐E (40%), HI‐N (19%), HI‐P (33%)
• To date, no doublet has produced superior results in RCT (eg, + HDAC inhib or len)3
• The BCL‐2 inhibitor venetoclax (Ven) combined with Aza induces rapid clinical responses in older
patients with AML*4
• Tolerability and efficacy of Ven combined with Aza in MDS unknown
• Phase 1 trial of IPSS Int‐2 or high (no t‐MDS,CMML, or OL),Current and Future Perspectives in the Treatment of High‐risk MDS
Safety, Efficacy, and Patient-Reported Outcomes
of Venetoclax in Combination With Azacitidine
for the Treatment of Patients With Higher-Risk
Myelodysplastic Syndrome: A Phase 1b Study
Jacqueline S. Garcia,1 Andrew H. Wei,2 Uma Borate,3 Chun Yew Fong,4 Maria R. Baer,5 Florian Nolte,6
Joseph Jurcic,7 Meagan A. Jacoby,8 Wan‐Jen Hong,9 Uwe Platzbecker,10 Olatoyosi Odenike,11
Ilona Cunningham,12 Ying Zhou,13 Bo Tong,13 Leah Hogdal,13 Rajesh Kamalakar,13 Jessica E. Hutti,13
Steve Kye,13 Guillermo Garcia‐Manero14
1Department of Medical Oncology, Dana‐Farber Cancer Institute, Boston, MA, USA; 2Department of Haematology, Alfred Hospital and Monash University,
Melbourne, VIC, Australia; 3Division of Hematology and Medical Oncology, Knight Cancer Institute, Oregon Health and Science University, Portland, OR,
USA; Olivia Newton John Cancer Research Institute, Austin Health, Melbourne, VIC, Australia; 5Greenebaum Comprehensive Cancer Center, University of
4
Maryland School of Medicine, Baltimore, MD, USA; 6Department of Hematology and Oncology, University Hospital Mannheim, Mannheim, Germany;
7Myelodysplastic Syndromes Center, Columbia University Medical Center, Columbia University, New York, NY, USA; 8Siteman Cancer Center at Barnes‐
Jewish Hospital and Washington University School of Medicine, St Louis, MO, USA; 9Genentech Inc., South San Francisco, CA, USA; 10Medical Clinic and
Policlinic 1, Hematology and Cellular Therapy, University Hospital Leipzig, Germany; 11University of Chicago Medicine and Comprehensive Cancer Center,
Chicago, IL, USA; 12Haematology Department, Concord Repatriation General Hospital, University of Sydney, Sydney, Australia; 13AbbVie, Inc., North
Chicago, IL, USA; 14Department of Leukemia, The University of Texas MD Anderson Cancer Center, Houston, TX, USA
American Society of Hematology (ASH) – 62nd Annual Meeting
December 5–8, 2020
My colleague, Dr. Garcia, presented this data at the recent ASH meeting where, indeed,
venetoclax was added to azacitidine.
©2021 MediCom Worldwide, Inc. 11Current and Future Perspectives in the Treatment of High‐risk MDS
Study Design
• Treatment cohorts (28‐day cycles); Aza 75 mg/m2 D1–7
Randomization phase Dose‐escalation phase Safety expansion 1 Safety expansion 2a
(28‐day Ven) (14‐day Ven) (14‐day Ven) (14‐day Ven)
Aza + Aza + Aza + Aza +
Ven 400 mg D1–28 (n=5) Ven 100 mg D1–14 (n=8) Ven 400 mg D1–14 (n=22) Ven 400 mg D1–14 (n=21)
Aza + Aza +
Ven 800 mg D1–28 (n=5) Ven 200 mg D1–14 (n=9) Key inclusion criteria Key exclusion criteria
• Adults ≥18 years • t‐MDS, CMML, u‐MDS/MPN
Aza Aza + • No prior MDS • Patients planned to undergo
(n=2) Ven 400 mg D1–14 (n=8)
treatment intensive chemotherapy or
• No DLTs during Cycle 1 • MTD not reached • IPSS ≥1.5b allo‐HSCTb
• 2 deaths in Cycle 2 (1 in • WBC was limited to
each combination cohort)
• Bone marrow blasts • CYP3A inducers within
≤10,000/μL
Protocol amendment toCurrent and Future Perspectives in the Treatment of High‐risk MDS
Response Rates and Transfusion Independence
100 5.1 • Median DoR: 12.9 months (min–max, 12.1–16.8)
1.3%
14.1 • Median DoR after CR: 13.8 months (min–max, 6.5–20.9)
80 • Median time to CR: 2.6 months (min–max, 1.2–19.6)
Patients, N=78 (%)
• For patients receiving Ven 400 mg (RP2D; n=51)b
60 39.7 ‒ 84% of patients achieved ORRa
47% achieved ORR by Cycle 2; 78% achieved ORR by Cycle 3
ORRa NE
40 ‒ 35% of patients achieved CR
79%
PD Transfusion independence rate n (% of N=78)
20 39.7 RBC and platelet 51 (65)
SD RBC 52 (67)
Platelet 60 (77)
0
a
ORR • A total of 16 patients (21%) went on to receive poststudy transplants;
7 received bone marrow transplant; and 9 received stem cell transplant
Data cutoff: June 30, 2020
aExcludes patients of Arm C (Aza only); ORR includes CR + mCR + PR; PR n=0; per IWG 2006*
bExcludes 5 patients from the randomization phase who received 28‐day Ven
Aza, azacitidine; CR, complete remission; DoR, duration of response; IWG 2006, International Working Group 2006; mCR, marrow CR;
NE, not evaluable; NR, not reported; ORR, objective response rate; PD, disease progression; PR, partial response; RBC, red blood cell;
RP2D, recommended phase 2 dose; SD, stable disease; Ven, venetoclax
*Cheson BD, et al. Blood. 2006;108(2):419‐425.; 4Garcia J, et al. Blood. 2020;136(Supplement 1):55‐57.
You can see for the bar graph on the left that the overall response rate is a whopping 79%,
roughly double than what you'd expect with azacitidine alone.
The complete remission rate is 39.7%, also double what you'd expect with azacitidine
alone, but remember, this is an uncontrolled trial. There were cytopenias, at least initially,
although the transfusion independence rate was pretty impressive as you can see on the
right. So should we be using azacitidine and venetoclax for high‐risk MDS patients today? I
would say no, not outside the context of a clinical trial. That indeed is an important
industrial sponsored trial of Aza plus or minus venetoclax in high‐risk MDS. Analogous to
the VIALE‐A study that was published in New England Journal of Medicine last summer
showing the benefit of that combination in older adults with AML.
©2021 MediCom Worldwide, Inc. 13Current and Future Perspectives in the Treatment of High‐risk MDS
OS for All Patients
1.0 +
Median time on the study: 16.4 months (95% CI, 15.2‒18.7)
++ + + +++ +
++++
+
++++++
++ ++ ++
+ + ++++
0.8
Probability of survival
++
+++++++ ++++ Survival estimates, % (95% CI)
+++ +++
+
+ +++ +
12‐mo 76.8 (64.7, 85.3)
0.6 ++ +
+ + ++
++
+ + + ++++ +
+
24‐mo 59.6 (43.0, 72.8)
0.4
+
0.2 OS, median (95% CI), months
All Ven + Aza patients 27.5 (18.2, NR)
+ Censored All Ven + Aza patients receiving Ven 400 mg (RP2D n=51) NR (17.7, NR)
0.0
0 3 6 9 12 15 18 21 24 27 30 33 36 39
Months
No. at risk
All Ven + Aza patients 78 66 59 46 38 36 20 15 7 2 1 1 1 0
All Ven + Aza patients 51 45 42 31 24 22 7 2 0
receiving Ven 400 mg (RP2D)
Data cutoff: June 30, 2020
Aza, azacitidine; CI, confidence interval; NR, not reached; OS, overall survival; RP2D, recommended phase 2 dose; Ven, venetoclax
Garcia J, et al. Blood. 2020;136(Supplement 1):55‐57.
You can see the median survival is not even reached for most of these patients, and so
that's encouraging as well, although again, the aforementioned phase 3 trial in MDS will
have overall survival as the primary endpoint.
©2021 MediCom Worldwide, Inc. 14Current and Future Perspectives in the Treatment of High‐risk MDS
Ven +/‐ Aza Not So Active in R/R HR MDS
ORR 40% 5%
ORR 27%
ORR 8%
Data cutoff: Aug 30, 2019.
ClinicalTrials.gov. NCT02966782.; Zeidan A, et al. ASH 2019. Abstract 565.
What about if you fail azacitidine, can you give venetoclax alone? You can, but the response
rate as you can see on the left is only 8%, and most of those are not complete responses,
of course. If you add venetoclax and keep giving the azacitidine,
the overall response rate is 40%, so it's potentially useful to a certain degree in people who
"failed" azacitidine.
©2021 MediCom Worldwide, Inc. 15Current and Future Perspectives in the Treatment of High‐risk MDS
Ven With or Without Aza in R/R MDS: PFS
Median PFS, Months (95% CI)
Ven monotherapy 3.3 (2.7, 5.2)
Ven + Aza combination 9.1 (5.9, NE)
Data cutoff: Aug 30, 2019.
Ven monotherapy: Ven 400 mg or 800 mg; Ven + Aza combination: Ven doses 100, 200, or 400 mg + Aza 75 mg/m2
ClinicalTrials.gov. NCT02966782.; Zeidan A, et al. ASH 2019. Abstract 565.
However, once you fail azacitidine as has been well known and shown many times over, the
prognosis is poor, you can see that with venetoclax monotherapy, the median survival is
about three months, and there's the progression‐free survival. Progression‐free survival is a
little bit longer if you add venetoclax to your ongoing azacitidine, it's still not very good.
©2021 MediCom Worldwide, Inc. 16Current and Future Perspectives in the Treatment of High‐risk MDS
ORAL HMA in MDS?
Oral Aza ‐ Useful in AML Maintenance and ASTX727 (Cedazuridine/Decitabine)
• Current HMA treatment poses significant patient burden due to 5 to 7 days per month of parenteral
administration in a clinic setting
• Oral bioavailability of HMAs decitabine and azacitidine is limited due to rapid degradation by CDA in
the gut and liver
O
NH 2
N N
N NH
O N CDA O
N
O O
HO H O
HO H O
Decitabine CDA inhibitor Inactive metabolite
• Cedazuridine is a novel CDA inhibitor
Wei A, et al. Blood. 2019;134 (Supplement_2):LBA‐3.; Garcia‐Manero G, et al. Blood. 2020;136(6):674‐683.
Now, oral HMA in MDS, yes, we can do that now. It's a drug whose developmental name
was ASTX727. It is cedazuridine which is a cytidine deaminase inhibitor. As you can see on
the chemical graphic on the bottom, it prevents the inactivation of decitabine if you give
oral, a pill with both cedazuridine and decitabine in it, you pretty much have the same drug
as you do with IV azacitidine.
©2021 MediCom Worldwide, Inc. 17Current and Future Perspectives in the Treatment of High‐risk MDS
ASCERTAIN Trial: Oral ASTX727 (Cedazuridine/Decitabine)
vs IV Decitabine, Phase 3 Study in MDS/CMM
• ASTX727 is an oral, fixed‐dose combination of cedazuridine and decitabine
Cycle 1 Cycle 2 ≥3 Cycles
(Int‐/high‐risk MDS; Oral ASTX727 IV Decitabine
CMML; AML 20% to 30% Sequence A 1 tablet x 5 d 1 h IV infusion x 5 d
blasts)
1:1 Oral ASTX727
At least 118 evaluable
Randomization 1 tablet x 5 d
patients with adequate PK in
Cycles 1 and 2 Sequence B
IV Decitabine Oral ASTX727
1 h IV infusion x 5 d 1 tablet x 5 d
Major entry criteria Primary endpoint
• Candidates for IV decitabine • Total 5‐d decitabine AUC equivalence (oral/IV 90% CI between 80% and 125%)
• ECOG PS 0 to 1 Secondary endpoints
• Life expectancy of ≥3 months • Efficacy: response rate; TI; duration of response; leukemia‐free and OS
• Adequate organ function • Safety of ASTX727
• One prior cycle of HMA is allowed • Max LINE‐1 demethylation
Garcia‐Manero G, et al. Blood. 2020;136(6):674‐683.
This ASCERTAIN trial, which was published last year by Garcia‐Manero in Blood showed that
the patient with this oral agent with these two drugs in it, the pill had these two drugs in it,
was bioequivalent to IV azacitidine for five days.
©2021 MediCom Worldwide, Inc. 18Current and Future Perspectives in the Treatment of High‐risk MDS
ASCERTAIN Trial: 5‐Day Decitabine AUC Equivalence
Decitabine IV DEC Oral ASTX727 Ratio of Geo LSM Intrasubject
5‐Day AUC0‐24 (h∙ng/mL) N Geo LSM N Geo LSM Oral/IV, % (90% CI) (% CV)
Primary analysis Paired* 123 864.9 123 855.7 98.9 (92.7, 105.6) 31.7
*Paired patient population: patients who received both ASTX727 and IV decitabine in the randomized first 2 cycles with adequate PK samples
• Study met its primary endpoint with high confidence: oral/IV 5‐day decitabine AUC ~99% with
90% CI of ~93% to 106%
• All sensitivity and secondary PK AUC analyses confirmed findings from primary analysis
• Demethylation similar to IV decitabine
• AEs similar to 5 d decitabine
• Efficacy data similar to that reported in phase 2 data: CR‐12%, marrow CR‐46%
Garcia‐Manero G, et al. Blood. 2020;136(6):674‐683.
It was basically a PK study showing that the drugs were equivalent almost 100% one to
one, and the response rates were what you'd expect with a decitabine alone. Marrow CR
rate was 46%, CR rate was 12%.
©2021 MediCom Worldwide, Inc. 19Current and Future Perspectives in the Treatment of High‐risk MDS
Enasidenib in Higher‐risk IDH2‐Mutated MDS:
Response Rates
Arm A (Untreated) Arm B (HMA‐Failure)
Total Aza + ENA ENA
(N = 31) (N = 13) (N = 18)
ORR, n (%) 21 (68) 11 (85) 10 (56)
Complete remission 8 (26) 3 (23) 5 (28)
Partial remission 1 (3) 0 (0) 1 (6)
Marrow complete remission 9 (29) 7 (54) 2 (11)
HI only 3 (10) 1 (8) 2 (11)
No response, n (%) 10 (32) 2 (15) 8 (44)
SD 9 (29) 2 (15) 7 (39)
PD 1 (3) 0 (0) 1 (6)
12 patients w R/R MDS rx w/ ivosidenib 500 mg/d: 5 (42%) CR
DiNardo CD, et al. N Engl J Med. 2020;383(7):617‐629.; Richard‐Carpentier G, et al. ASH 2019. Abstract 678.
Another oral agent which can occasionally use an MDS is enasidenib or, for that matter,
ivosidenib. These are drugs which were approved for relapsed/refractory AMLs with either
an IDH2 for enasidenib or an IDH1 for ivosidenib mutation. You can see here, the overall
response rate is pretty high for untreated patients receiving azacitidine plus enasidenib,
and for those who failed HMA already, single‐agent enasidenib had an appreciable
response rate with some CRs, so that's pretty good. It's an option for the rare patient who
has an IDH1 or IDH2 mutation, an IDH inhibitor either alone or with azacitidine.
©2021 MediCom Worldwide, Inc. 20Current and Future Perspectives in the Treatment of High‐risk MDS
Allogeneic Transplant in MDS: Approximation of
Life Expectancy (Years)
Immediate Transplant Transplant in 2 Years Transplant at Progression
Low 6.51 6.86 7.21
Int‐1 4.61 4.74 5.16
Int‐2 4.93 3.21 2.84
High 3.20 2.75 2.75
This is for fully HLA matched T cell replete myeloablative SCT
Update: Same applies in era of RIC allo SCT among patients 60‐70 years old*
*Koreth J, et al. J Clin Oncol. 2013;31(21):2662‐2670.; Cutler CS, et al. Blood. 2004;104(2):579‐585.
Now, the sine qua non for treatment of adults with high‐risk disease is transplant. Do we
transplant lower‐risk patients? No, we transplant higher‐risk patients. Based on this data
from Corey Cutler at my institution who showed that it's better to transplant patients who
have high‐risk disease attributed to a high risk by the IPSS to save years of life, but if they
have a low‐risk disease, you should wait until they progress. His colleague, Dr. Koreth,
showed the same thing in the era of RIC allo stem cell transplant.
©2021 MediCom Worldwide, Inc. 21Current and Future Perspectives in the Treatment of High‐risk MDS
TP53 Mutated MDS
Poor Prognosis Post‐SCT Due to Early Relapse
Survival
MDS No TP53 mutation
P < 0.0001
TP53 mutation
TP53 mutation No
Median OS = 8 months TP53 mutation
Relapse
Donor v no donor higher risk MDS:
TP53 mutation
n=384 48 v 27% 3 y OS in age 50‐75*
P < 0.0001
No TP53 mutation
* Cutler C. ASH 2020.; Lindsley C, et al. N Engl J Med. 2017;376(6):536‐547.
An important additional piece of data that Dr. Cutler was supplied was presented at ASH in
2020 where he showed that a donor versus no donor analysis in high‐risk MDS, that the
overall survival was greater in those patients who had a transplant as opposed to those
patients who were treated with chemotherapy alone. Of course, transplant is great, but not
so great if you have a P53 mutation. The relapse rate is incredibly high for those people
with P53‐mutant MDS who have a transplant. This was data from another colleague of
mine, Dr. Lindsley. There's a lot of focus on trying to improve the outcome for those with
P53‐mutated MDS.
©2021 MediCom Worldwide, Inc. 22Current and Future Perspectives in the Treatment of High‐risk MDS
Efficacy and Safety of Pevonedistat plus Azacitidine vs
Azacitidine Alone in Higher‐Risk Myelodysplastic Syndromes
(MDS) from Study P‐2001 (NCT02610777): Abstract #653
Mikkael A. Sekeres,1 Justin Watts,1 Atanas Radinoff,2 Montserrat Arnan Sangerman,3 Marco Cerrano,4 Patricia Font Lopez,5
Joshua F. Zeidner,6 Maria Diez Campelo,7 Carlos Graux,8 Jane Liesveld,9 Dominik Selleslag,10 Nikolay Tzvetkov,11
Robert J. Fram,12 Dan Zhao,12 Sharon Friedlander,12 Kevin Galinsky,12 Douglas V. Faller,12 Lionel Adès13
1Sylvester Comprehensive Cancer Center, University of Miami, Miami, FL, USA; 2University Hospital Sveti Ivan Rislki, Sofia, Bulgaria;
3InstitutCatalà d'Oncologia‐Institut d'Investigació Biomèdica de Bellvitge (IDIBELL), Hospitalet, Barcelona, Spain; 4Department of
Molecular Biotechnology and Health Sciences, Division of Hematology, University of Turin, Turin, Italy; 5Hospital General Universitario
Gregorio Marañón, Instituto de Investigación Sanitaria Gregorio Marañón (IiSGM), Madrid, Spain; 6University of North Carolina,
Lineberger Comprehensive Cancer Center, Chapel Hill, NC, USA; 7University Hospital of Salamanca, IBSAL Institute for Biomedical
Research of Salamanca, Salamanca, Spain; 8Université Catholique de Louvain, Centre Hospitalier Universitaire, Namur, Yvoir, Belgium;
9The James P Wilmot Cancer Institute, University of Rochester, Rochester, NY, USA; 10AZ Sint Jan Brugge‐Oostende, Brugge, Belgium;
11MHAT Dr. Georgi Stranski, Clinic of Haematology, Pleven, Bulgaria; 12Millennium Pharmaceuticals, Inc., Cambridge, MA, a wholly owned
subsidiary of Takeda Pharmaceutical Company Limited; 13Hôpital Saint‐Louis Hématologie Clinique, Paris, France
Oral presentation at the virtual 62nd Annual Meeting of the American Society of Hematology (ASH), December 5–8, 2020
Now, another drug which may be useful in high‐risk MDS is pevonedistat. This was
presented by my colleague, Dr. Sekeres.
©2021 MediCom Worldwide, Inc. 23Current and Future Perspectives in the Treatment of High‐risk MDS
Pevonedistat: First‐in‐Class Inhibitor of the
NEDD8‐activating Enzyme
• Inhibiting the NEDD8‐activating enzyme blocks ubiquitination of select proteins upstream of the proteasome1,2
• Treatment with pevonedistat disrupts cell cycle progression and cell survival, leading to cell death in cancers2,3
• Pevonedistat exhibits synergistic activity in combination with azacitidine in cellular and mouse xenograft models
of AML4
AML, acute myeloid leukemia; NAE, NEDD8‐activating enzyme; NEDD8, neural precursor cell expressed, developmentally
downregulated 8; NF‐kB, nuclear factor kappa‐light‐chain‐enhancer of activated B cells.
Sekeres MA, et al. Blood. 2020;136(Suppl. 1):653. 1Brownell JE, et al. Mol Cell. 2010;37:102‐111; 2Soucy TA, et al. Nature. 2009;458:732‐736.
3Soucy TA, et al. Clin Cancer Res. 2009;15:3912‐3916. 4Smith PG, et al. Blood. 2011;118:abstract 578. Permission request pending.
Mikkael used this drug which is an inhibitor of the NEDD8‐activating enzyme which blocks
ubiquitination of select proteins upstream of the proteasome. It's a neat mechanism of
action and has potential to be useful along with azacitidine getting rid of these block
ubiquitination of select proteins and then blocking the enzyme that blocks that can allow
these proteins to be degraded and promote apoptosis.
©2021 MediCom Worldwide, Inc. 24Current and Future Perspectives in the Treatment of High‐risk MDS
NCT02610777: Phase 2, Randomized, Open‐label,
Global, Multicenter Study
ITT patients included: Pevonedistat + azacitidine • Study powered on EFS
Pevonedistat: 20 mg/m2 (IV) on days 1, 3, 5
• Higher‐risk MDS (n=67) (defined as time to death
Randomization
Azacitidine: 75 mg/m2 (IV or SC) on days 1–5, 8, 9
or transformation to AML)
• Higher‐risk CMML (n=17) 1:1 as the original primary
Repeat every 28 days
• Low‐blast AML (n=36) N=120 endpoint
• Primary endpoint changed
– No previous HMAs to OS based on regulatory
Azacitidine
– Ineligible for allogeneic SCT 75 mg/m2 (IV or SC) on days 1–5, 8, 9 feedback
Results in the ITT population:1 Analyses in patients with higher‐risk MDS presented here:
• Median EFS: 21.0 vs 16.6 months • Focus on clinical and cytogenetic risk (IPSS‐R), and genetic factors that could
(HR: 0.67; 95% CI: 0.42–1.05; P=0.076) impact ORR and duration of response, as well as EFS and OS
• Post‐hoc analysis of patients with MDS assessed as high‐risk according to the
• Median OS: 21.8 vs 19.0 months
combined Cleveland Clinic model formula, which incorporates both clinical
(HR: 0.80; 95% CI: 0.51–1.26; P=0.334)
and genetic factors2
CI, confidence interval; CMML, chronic myelomonocytic leukemia; EFS, event‐free survival; HMA, hypomethylating agent; HR, hazard ratio;
IPSS‐R, Revised International Prognostic Scoring System; ITT, intent‐to‐treat; IV, intravenous; MDS, myelodysplastic syndromes; ORR,
overall response rate; OS, overall survival; SC, subcutaneous; SCT, stem cell transplant.
1Ades L, et al. J Clin Oncol. 2020;38(15_suppl):abstract 7506. 2Nazha A, et al. Leukemia. 2016;30:2214‐2220.
Sekeres MA, et al. Blood. 2020;136(Suppl. 1):653.
The proof in the pudding would be in a clinical trial. There is a clinical trial that allowed
people with high‐risk MDS, higher‐risk AML, or low blast count AML to go on. I'm going to
present the data that Mikkael presented at ASH in just patients with higher‐risk MDS. The
trial was simply pevonedistat plus azacitidine versus azacitidine alone.
©2021 MediCom Worldwide, Inc. 25Current and Future Perspectives in the Treatment of High‐risk MDS
CR Rate was Nearly Doubled, and Median Duration of
Response was Almost Tripled with Pevonedistat + Aza
Response‐evaluable patients with higher‐risk MDS (n=59):
P‐value (pevonedistat +
ORR 79% azacitidine vs azacitidine)
80
ORR 0.065 Pevonedistat 34.6 months
70 CR rate 0.050 + azacitidine (95% CI: 11.53–34.60)
13.1 months
ORR 57%
Azacitidine (95% CI: 12.02–NE)
60
52% CR 0 4 8 12 16 20 24 28 32 36 40
50
Patients (%)
Median duration of response (months)
27% CR
40
Pevonedistat +
30 azacitidine Azacitidine
3% PR
13% PR n=16 n=12
20
24% HI Median time to first CR or PR 3.83 4.29
10 17% HI among responders, months (range) (1.8–25.8) (2.0–13.2)
0
Pevonedistat
Pevo Azacitidine
Aza
+ azacitidine
CR, complete response; HI, hematologic improvement; NE, not evaluable; PR, partial response
Sekeres MA, et al. Blood. 2020;136(Suppl. 1):653.
The response rate in the combination was greater than the response rate with azacitidine
alone. If we look at the CR rate, it was doubled from 27%, which is high for azacitidine
alone, to 52% for the combination. The duration of response was also almost triple what it
was in azacitidine alone, so promising. It was not really powered to show a survival benefit,
and indeed, it didn't show a survival benefit compared to Aza alone.
©2021 MediCom Worldwide, Inc. 26Current and Future Perspectives in the Treatment of High‐risk MDS
EFS and OS Favored Pevonedistat + Aza Among
Patients with Higher‐risk MDS According to IPSS‐R
Pevonedistat Pevonedistat
+ azacitidine Azacitidine + azacitidine Azacitidine
n=32 n=35
EFS* n=32 n=35 OS
100 Median EFS, months 20.2 14.8 100 Median OS, months 23.9 19.1
Hazard ratio 0.539 (0.292–0.995) Hazard ratio 0.701 (0.386–1.273)
(95% CI) P=0.240
Probability of survival (%)
(95% CI) P=0.045
Probability of EFS (%)
75 75
50 50
25 25
Pevonedistat + azacitidine Pevonedistat + azacitidine
Azacitidine Azacitidine
0 0
0 3 6 9 12 15 18 21 24 27 30 33 36 39 0 3 6 9 12 15 18 21 24 27 30 33 36 39
Number at risk
Time (months) Number at risk
Time (months)
Pevonedistat 32 30 28 25 24 20 16 11 10 8 2 1 1 0 Pevonedistat 32 30 30 28 28 24 21 17 16 13 8 5 2 0
+ azacitidine + azacitidine
Azacitidine 35 29 23 22 18 12 9 6 5 4 0 0 0 0 Azacitidine 35 30 29 26 23 20 18 14 13 13 3 1 0 0
• Longer EFS was particularly evident in patients with IPSS‐R‐defined very‐high‐risk MDS
(n=26; HR: 0.47; 95% CI: 0.19–1.18) and high‐risk MDS (n=21; HR: 0.53; 95% CI: 0.17–1.72)
*EFS defined as time to death or transformation to AML in higher‐risk MDS.
Sekeres MA, et al. Blood. 2020;136(Suppl. 1):653.
But there was an event‐free survival benefit with the Pev plus Aza. They will be doing a
large phase 3 trial to try to show that Pev plus Aza is better than Aza in high‐risk MDS. Of
course, that's going to be a competitor to the Ven plus Aza vs Aza phase 3 trial in high‐risk
MDS. There are some people who say pevonedistat has a lower likelihood of
myelosuppression. That might be useful for some patients who can't tolerate the
myelosuppression inherent, the use of venetoclax plus azacitidine.
©2021 MediCom Worldwide, Inc. 27Current and Future Perspectives in the Treatment of High‐risk MDS
Targeting TP53 Mutations in MDS/AML via APR‐246
p53 R175H
p53 R175H
+
APR‐246
APR‐246 binds …restores wt p53 …and triggers cell cycle
covalently to p53… conformation & activity… arrest and apoptosis
Fersht A, et al. Protein Sci. 2010.; Zhang Q, et al. Cell Death Dis. 2018;9(5):439.; Furukawa H, et al. Cancer Sci. 2018;109(2):412‐421.;
Sallman D, et al. ASH 2019. Abstract 569. Permission request pending.
Let's talk about P53 targeting agents. This is a really interesting one called APR‐246, in
which the misfolded mutant protein can be rehabilitated and reactivated with the use of
this chemical, allegedly.
©2021 MediCom Worldwide, Inc. 28Current and Future Perspectives in the Treatment of High‐risk MDS
Response to Treatment in Evaluable Patients (n=45)
APR‐246 + Aza
Overall MDS AML MDS‐MPN + CMML
Evaluable patients, n 45 33 8 4
Overall response rate, n (%) 39 (87) 29 (88) 7 (88) 3 (75)
CR rate, n (%) 24 (53) 20 (61) 4 (50) 0 (0)
Duration of CR, months (median) [95% CI] 7.3 [5.8 – NE] 7.3 [5.8 – NE] 7.0 [3.3 – NE] NE
Discontinued for transplant, n (%) 22 (49) 17 (52) 4 (50) 1 (25)
• Median duration of follow‐up = 10.8 months
Sallman D, et al. ASH 2019.
Indeed, combining APR‐246, when presented last year, a very high response rate, you can
see 87%, again 53% CR rate, you think that would be enough to get the drug approved.
©2021 MediCom Worldwide, Inc. 29Current and Future Perspectives in the Treatment of High‐risk MDS
Overall Survival (ITT): APR‐246 + Aza
ITT Cohort
Median OS 10.8 Months (95% CI 8.1‐13.4)
Response 13.7 months (95% CI 10.8‐16.5)
Overall Survival
No Response 3.9 months (95% CI 1.9‐6.0)
Overall Survival
P < 0.0001
Time (months) Time (months)
CR
Non‐CR Response BMT 14.7 Months (95% CI 8.6‐20.9)
No Response No BMT 10.1 Months (95% CI 6.2‐14.0)
Overall Survival
Overall Survival
P < 0.0001 P = 0.1
Time (months)
Time (months)
44% cleared TP53 toCurrent and Future Perspectives in the Treatment of High‐risk MDS
Pivotal Phase 3 MDS Trial in TP53‐Mutant MDS
• Randomized study of frontline azacitidine ± APR‐246 in TP53‐mutant MDS
• Intermediate‐/high‐/very high‐risk TP53‐mutant MDS
• Primary endpoint: CR rate
• Secondary endpoints: ORR, DoR, PFS, LFS, OS, transplant rate
• Status
– Enrollment commenced in January 2019
– Currently targeting full enrollment in first quarter 2020
– Fast Track Designation for MDS: granted by FDA in April 2019
– Orphan Drug Designations for MDS: granted by FDA in April 2019 and EMA in July 2019
Press Release 12/20: primary EP not met
ClinicalTrials.gov. NCT03745716.
They started a phase 3 trial of APR‐246 plus Aza versus Aza alone, with a primary endpoint
being complete remission rate, not even survival, and a press release in December
suggested the primary endpoint was not met. We haven't seen the full data about that yet.
©2021 MediCom Worldwide, Inc. 31Current and Future Perspectives in the Treatment of High‐risk MDS
CD47
• Major macrophage immune checkpoint and "do not eat me" signal in myeloid malignancies including
MDS and AML
CD47 Expression in Patients With AML
• CD47 is a "do not eat me" signal on cancers that enables macrophage immune evasion
• Increased CD47 expression predicts worse prognosis in patients with AML
Veillette, A, et al. J Clin Oncol. 2019;37:1012‐1014.; Chao MP, et al. Curr Opin Immunol. 2012;24:225‐232.; Majeti R, et al. Cell.
2009;138(2):286‐299.; Sallman D, et al. ASH 2019. Abstract 569. Permission request pending.
Finally, CD47, as I mentioned earlier, covers up the "don't eat me" signal on the tumor cell,
in this case, the MDS cell, you know that CD47 high expression is a bad prognostic finding,
at least in AML.
©2021 MediCom Worldwide, Inc. 32Current and Future Perspectives in the Treatment of High‐risk MDS
Magrolimab (Formerly 5F9) Is a First‐in‐Class Macrophage
Immune Checkpoint Inhibitor Targeting CD47
Magrolimab
Control mAb: No Phagocytosis
Anti‐CD47 mAb: Phagocytosis
• CD47 is a “do not eat me” signal that is overexpressed in multiple cancers, including
acute myeloid leukemia, leading to macrophage immune evasion
• Magrolimab, an IgG4 anti‐CD47 monoclonal antibody (mAb), eliminates tumor Macrophages
cells through macrophage phagocytosis Cancer cells
• Magrolimab is being investigated in multiple cancers with >500 patients dosed
Sallman D, et al. ASH 2020. Permission request pending.
This drug, magrolimab, formerly called 5F9, is a first‐in‐class drug that covers up the signal.
You can see that it promotes phagocytosis in the bad‐guy cells, the blasts.
©2021 MediCom Worldwide, Inc. 33Current and Future Perspectives in the Treatment of High‐risk MDS
5F9005 Study Design: Magrolimab in Combination
With AZA in AML and MDS
Primary Objectives
1. Safety of magrolimab alone or with AZA
2. Efficacy of magrolimab + AZA in untreated AML/MDS
Magrolimab + AZA Combo
Safety Evaluation (N=6) Expansion Secondary Objectives
Untreated AML
ineligible for induction 1. Pharmacokinetics, pharmacodynamics, and
chemotherapy or immunogenicity of 5F9
Magro: 1, 30 mg/kg* weekly 2. Additional measures of efficacy (DOR, PFS, OS)
untreated MDS Magro: 1, 30 mg/kg* weekly
or Q2W
AZA: 75 mg/m2 D1−7
intermediate to very AZA: 75 mg/m2 D1−7
high risk by IPSS‐R Exploratory Objective
To assess CD47 receptor occupancy, markers of immune cell
activity, and molecular profiling in AML/MDS
• A magrolimab priming dose (1 mg/kg) and dose ramp‐up were utilized to mitigate on‐target anemia
* Dose ramp‐up from 1 mg/kg to 30 mg/kg by week 2, then 30 mg/kg maintenance dosing.
IPSS‐R: Revised International Prognostic Scoring System
Sallman D, et al. ASH 2020.
This trial was presented at ASH in AML/MDS of magrolimab plus azacitidine, and the
primary objective was to make sure it was safe. You have to ramp up the dose because of
the non‐target anemia that one sees due to the expression of CD47 on red cells. You can
get around that by revving up the dose.
©2021 MediCom Worldwide, Inc. 34Current and Future Perspectives in the Treatment of High‐risk MDS
Magrolimab + AZA Induces High Response Rates in
MDS and AML
Response assessments per 2006 IWG MDS criteria and 2017 AML ELN criteria. Patients with at
least 1 post‐treatment response assessment are shown; all other patients are on therapy and are
too early for first response assessment, except for 2 MDS patients not evaluable (withdrawal of
consent) and 3 AML patients (1 AE, 2 early withdrawal). Four patients not shown due to missing values;Current and Future Perspectives in the Treatment of High‐risk MDS
Magrolimab + AZA Eliminates Disease in AML and
MDS Patients with TP53 Mutation
*Responding patients with abnormal cytogenetics at baseline.
• Magrolimab + AZA has a high response rate with deep responses in TP53‐mutant AML and MDS patients
• The estimated 6‐months survival is 91% and 100% in AML and MDS patients, respectively
• Median duration and survival has not been reached, which compares favorably to current therapies
‒ Venetoclax + AZA in AML: ORR 47%, DOR 5.6 mo, OS 7.2 mo1
9/16 patients cleared TP53 VAF to less than 5%
DiNardo CD, et al. Blood. 2019;133(1):7‐17.; Sallman D, et al. ASCO 2020.
Sure, most of these patients showing here have AML with the P53 mutation, but the
response rate was good, 75% in both the MDS and AML. Again, the durability is a little
questionable, but it's a good start. We don't have anything else like this if this plays out in
subsequent trials. Some of the patients as I mentioned do clear their TP53 mutation.
©2021 MediCom Worldwide, Inc. 36Current and Future Perspectives in the Treatment of High‐risk MDS
Preliminary Median Overall Survival Is Encouraging
in Both TP53 Wild‐type and Mutant Patients
TP53 wild‐type (N=16) TP53 mutant (N=47)
12.9
Median OS, mo (range)
(0.2+, 28.4+)
95% CI, mo 8.21, 17.28
Overall Survival
Overall Survival
Median follow‐up, mo 4.7
18.9
Median OS, mo (range)
(2.7, 27.9+)
95% CI, mo 4.34, NE
Median follow‐up, mo 12.5
Months Months
The median OS is 18.9 months in TP53 wild‐type patients and 12.9 months in TP53‐mutant patients
This initial median OS data may compare favorably to venetoclax + hypomethylating agent combinations (14.7‐17.5 mo in all‐comers,1,3
5.2–7.2 mo in patients who are TP53 mutant2,3)
Additional patients and longer follow‐up are needed to further characterize the survival benefit
NE, not evaluable.
1DiNardo CD, et al. N Engl J Med. 2020;383(7):617‐629. 2Kim K, et al. ASH 2020. 3DiNardo CD, et al. Blood. 2019;133(1):7‐17.
Sallman D, et al. ASH 2020.
The survival in the wild type, it's quite good. The P53 mutant diseases in both AML and
MDS, you can see the median overall survival is 13 months. It's better than what we
normally see, but again, phase 3 trials will tell the tale.
©2021 MediCom Worldwide, Inc. 37Current and Future Perspectives in the Treatment of High‐risk MDS
Checkpoint Inhibition: Sabatolimab
(TIM‐3 Antibody) + HMA for High‐risk MDS
• 48 AML, 39 MDS, 12 CMML
• Most common AEs F&N, anemia/thrombocytopenia/neutropenia
• Few immune AAs >g3
• 2.1‐month median TTR
• Estimated 12‐month PFS 44%
TIM‐3 Ab + decitabine TIM‐3 Ab + azacitidine
n 19 20
evaluable 18 17
CR 33% 12%
Marrow CR 17% 29%
SD 11% 23%
ORR 61% 65%
Brunner A, et al. ASH 2020.
One more thing to talk about is sabatolimab, which is a TIM‐3 antibody. Again, used with
HMA here, the complete remission rate is 33% when added to decitabine, 12% when
added to azacitidine, overall response rate is 65%. Perhaps not as impressive as the
response rate ones that we were seeing with either the APR‐246 or the anti‐CD47, but still
encouraging. Most prior trials with checkpoint inhibitors in MDS haven't been this
favorable.
©2021 MediCom Worldwide, Inc. 38Current and Future Perspectives in the Treatment of High‐risk MDS
Proposed Treatment Algorithm for Patients
with MDS: 2021
MDS
Lower‐risk Higher‐risk
(IPSS low, INT‐1) (IPSS INT‐2, high)
(BM blastsCurrent and Future Perspectives in the Treatment of High‐risk MDS
Acknowledgements
• Clinical Team at DFCI:
– Dan DeAngelo, Martha Wadleigh, David Steensma, Jackie Garcia, Goyo Abel, Eric Winer, Marlise Luskin
– Ilene Galinsky, NP
– Andrian Penicaud, PA; Kat Edmonds, NP; Sarah Cahill, PA; Mary Girard, PA; Elizabeth Herrity, DNP
BMT Team: Alyea, Antin, Armand, Cutler, Ho, Koreth, Romee, Nikiforow, Soiffer
DFHCC Team: Avigan, Rosenblatt, Amrein, Fathi, Brunner, Hobbs, Graubert
• Scientific Team at Dana‐Farber/Harvard Cancer Center
– Ben Ebert, Andy Lane, Coleman Lindsley, Jim Griffin, Tony Letai, David Weinstock, David Frank, Kim Stegmeir, Donna
Neuberg, Tom Look, S. Armstrong, T. Graubert
• Worldwide Collaborators
– Alliance: R. Larson, G. Marcucci, W. Blum, G. Uy, G. Roboz, S. Mandrekar
– Worldwide: C. Schiffer, T. Fischer, H. Dohner, K. Dohner, C. Thiede, R. Schlenk, and others
• Slides
– G. Garcia‐Manero, D. Steensma, D. Sallman
I'd like to thank all of my colleagues at Dana‐Farber throughout the Harvard Cancer Center
and across the world who helped me put this talk together and done some of the similar
work in this field. I really thank you for viewing this activity. Please, have a good day.
©2021 MediCom Worldwide, Inc. 40You can also read

















































