DELIVERING AN INTEGRATED SERVICE FOR CANCER PATIENTS.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DELIVERING AN INTEGRATED SERVICE FOR
CANCER PATIENTS.
– NO HEALTH WITHOUT MENTAL HEALTH
Dr Asanga Fernando @asangafern
Macmillan Consultant Liaison (Cancer) Psychiatrist &
Clinical Director of simulation & clinical skills,
St George’s University Hospitals NHS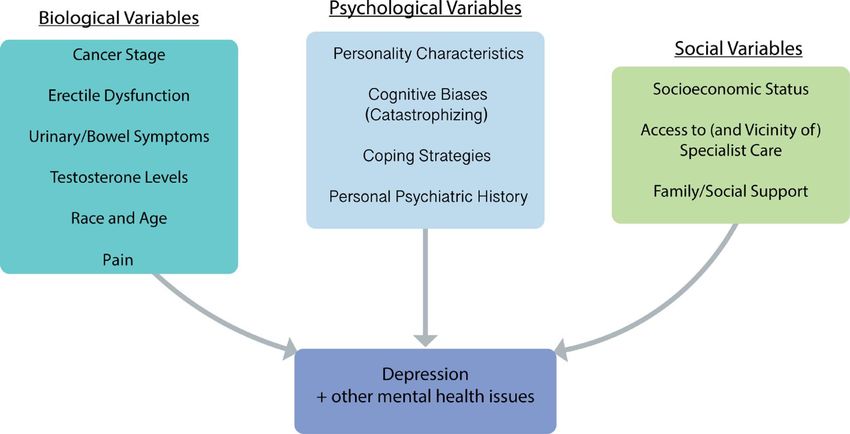
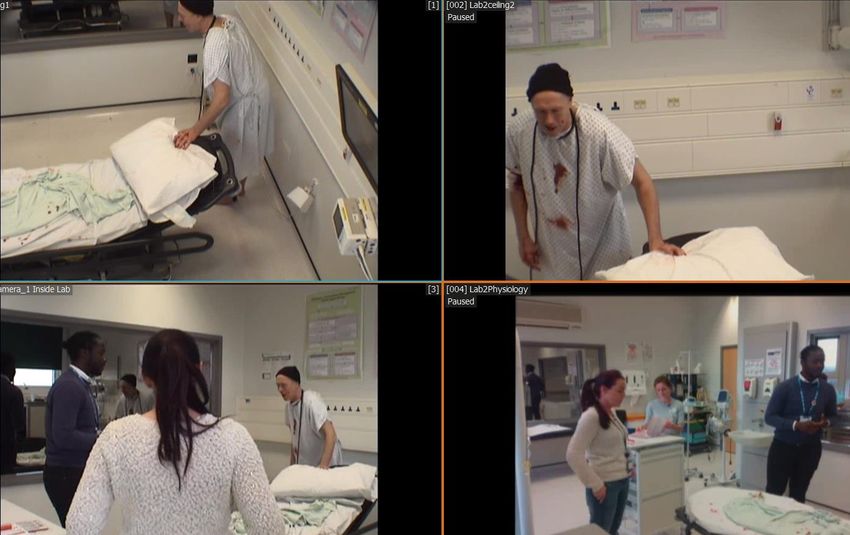
LEARNING OBJECTIVES • Delivering Integrated services for Mental health and Cancer • supporting the mental health needs of people living with and beyond cancer • Our experience and my role as a Macmillan Consultant Liaison Psychiatrist • Cancer Simulation and Education • Interactive Discussion - what does good look like? What should we be measuring?
THE RANGE – PSYCHOLOGICAL
DISTRESS
Cancer Psychiatry 2019
NO HEALTH WITHOUT MENTAL HEALTH • 25% within 1 year of Dx, 10% level 4 (NICE 2004) • Poorer Functioning, QoL, Cancer specific probs (DHD) • Adverse impact on carers, families • Reduced adherence to cancer Rx • Likely reduction in life expectancy • Increased Cost (Naylor et al.2012) & length of stay Cancer Psychiatry 2019

PATIENTS WITH EXISTING SMI
A STORY WITH AN UNHAPPY ENDING
TREATMENT OF PRE-EXISTING MH
• Cancer is over-represented in SMI population
• (Dalton et al 2002, Hung et al 2014) – Cancer incidence in MH units vs
matched gen pop – severe depression assoc with doubling of cancers.
• Particularly assoc with EtOH, substance misuse, smoking (also
Lichtermann et al 2001)
• SMI complicates and delays access to cancer care
• Pt factors
• Neglect
• Suicidality
• Amotivation
• Psychomotor retardation
• Paranoia, persec. Delusions
• Systemic factors
• Access to smoking cessation,
• Screening – breast, cervical
• LT patients, prisoners, housebound.
Cancer Psychiatry 2019TREATMENT OF PRE-EXISTING MH • Care driven by Multi-Agency approach • Accompanying staff, transport, support workers, supported housing, social • Thought Sx, Behavioural Sx, Cognitive Sx – cancer worsens all of these – think about how this is likely to impact upon engagement. • Treatment decision making & Mental Capacity issues – commonplace. • Delays to MH treatment: • LT psychotherapy/ group • Disruption of regular monitoring of risk, MSE by CMHT • Hosp admission may lead to lapse in depot admin • Surgery – may affect oral absorption • Medication Interactions Cancer Psychiatry 2019
CANCER PATIENTS WITH PSYCHIATRIC CO-MORBIDITY
DEPRESSION • (Mitchell, A. J., Chan, M et al 2011) – 16.3%, (70 studies, 10,071 pts) (anxiety – 10.3%) • (Massie, 2004) – varied, but up to 38% with Major depression • Varies with Tumour type: Lung>Gynae>Breast>Colorectal>GU (Walker et al. 2014a) • 73% patients receive no adequate, evidenced based Rx (Walker et al. 2014 b) • Screening for depression doesn’t help with Rx? (Meijer et al. 2011) • Undertreated by GPs • Increases with severity of illness • Sharpe et al (2004) 9%@ OPD, Rayner et al (2011) 36% advanced disease • Elderly Ca patients - condition most associated with disability and morbidity (Parpa et al. 2015) Cancer Psychiatry 2019
FIGURE 1: BIOPSYCHOSOCIAL FACTORS ASSOCIATED WITH DEPRESSION IN MEN WITH
PROSTATE CANCER TAKEN FROM: FERVAHA, G., IZARD, J. P., TRIPP, D. A., RAJAN, S.,
LEONG, D. P., & SIEMENS, D. R. (2019, JANUARY). DEPRESSION AND P ROSTATE CANCER: A
FOCUSED REVIEW FOR THE CLINICIAN. IN UROLOGIC ONCOLOGY: SEMINARS AND ORIGINAL
INVESTIGATIONS. ELSEVIER
Cancer Psychiatry 2019DEPRESSION & SUICIDALITY
• SMR 4-6.8 X age & sex matched population
• 2014 – 6122 deaths
• Men 45-59 (3x than women)
• Over 50% Hx Drug/EtOH misuse
• Burden – lung, UGI, Head and Neck (Robson et al. 2010; Robinson et al 2009)
• Head and Neck & Lung Ca >50% of Cancer suicides
• Comorbid loss of speech, tasting food, unable to seal mouth, disfigurement -
risk factors.
• Consider:
• EtOH
• Economic factors
• Dynamic factors – esp pain, agitation
• Functioning
Cancer Psychiatry 2019PSYCHIATRY OF CANCER
TREATMENTSTREATMENTS & PSYCHOLOGICAL
IMPACT – PROSTATE CANCER
• Surgery (Prostatectomy)
• Incontinence • Androgen Deprivation Therapy
• Erectile dysfunction • Loss of libido
• Decisional crisis/regret • Weight redistribution
• Hot flashes
• Radiotherapy • Fatigue
• Painful urinary frequency • Cognitive Impairment – 50%3–5
• Bowel irritation/
Diarrhoea/Incontinence
• Specific newer agents with less cognitive
• 6/12 post-radiotherapy, 16% severe effect6
anxiety, 6% severe depression1,2
• Chemotherapy
1. Andreyev HJN, et al. The Lancet Oncology 2010;11(4):310-312; 2. Andreyev HJN, et al. The Lancet 2013;382(9910):2084-2092;
2. van Tol-Geerdink JJ, et al. Radiotherapy and Oncology 2011;98(2):203-206; 3. Gonzalez BD, et al. Journal of Clinical Oncology
2015;33(18):2021;
4. Cherrier MM, et al. Psycho‐Oncology 2009;18(3):237-247; 5. Nelson CJ, et al. Cancer 2008;113(5):1097-1106; 6. Sternberg CN, et
al. Lancet Oncol 2014;15(11):1263-8.STEROIDS Cancer Psychiatry 2019
END OF LIFE & SURVIVORSHIP
END OF LIFE CHALLENGES • Desire for Hastened death: • Strongly Associated with depression & with Sx burden, QoL • Phys Sx such as fatigue increase DHD • DHD is unstable over time • If depression is present, Rx reduces DHD • Non malignant disease have greater odds of DHD • EoLC, opiates (opiate toxicity), falls, delirium, capacity, TEP, Advanced care planning • Dynamic factors – pain, thirst, breathless, constipation, opiates • MDT approach, effective psychiatric intervention can help improve QoL at the end of life • Utilise Hospices Cancer Psychiatry 2019
AN INTEGRATED SERVICE – WHAT
DOES GOOD LOOK LIKE?
AND WHO SHOULD GET TO DECIDE?CLINICAL INTEGRATION • Example - Cancer Psychological Support (CaPS) team at St George’s. • Co-located and embedded within Cancer services • Multi-professional • Ability to see carers • Same electronic records as Oncology, Surgery, Primary care • Rapid access to medication record • Presence at MDTs • Clinical integration also helps develop education, research and audit • Patient group involvement • Commissioning • New ways of working • Pathway approach • Data and Outcomes – which ones matter? Are they important to patients? HR-QoL? Fxt? • Education
A CANCER JOURNEY
• Survivorship
(Primary care)
Secondary • Surgery
• Transfer of Care
Primary • Diagnosis
• transfer of care
Care • Chemotherapy
• Immunotherapy
Survivorship • End of Life care –
Care • Co-morbidity (TREATME • Radiotherapy
/ End of Life Secondary care
NT) • Hospice/ Comm
• Supportive pall
• Carers
HEE funded Primary Immunotherapy CAMhELS, CAMhELS (int)
Care Resource SACT Communication DNACPR (int)
Toolkit Surgery CARERS
Primary careINTEGRATION ACROSS THE PATHWAY • HEE funded Transforming Primary Care Educational toolkit for people living with and beyond (developed by HEE, St George’s, TCST, Macmillan) • Cancer Rehab • Personalised Care • Stratified Follow Up • Cancer Care Reviews • Psychological Support • Bridging the gaps – Primary and Secondary care medications?
W: www.gapssimulation.com E: asanga.fernando@kcl.ac.uk
T: @GAPSsimulation @asangafern
CAMHELSKNOWLEDGE BASED QUESTIONS
Knowledge Based Questions
• 4 questions 3.5
• Total 74 responses 3
• Increased from 31% to 74%
2.5
• Highly Significant difference,
p=0.0001 2
1.5
1
0.5
0
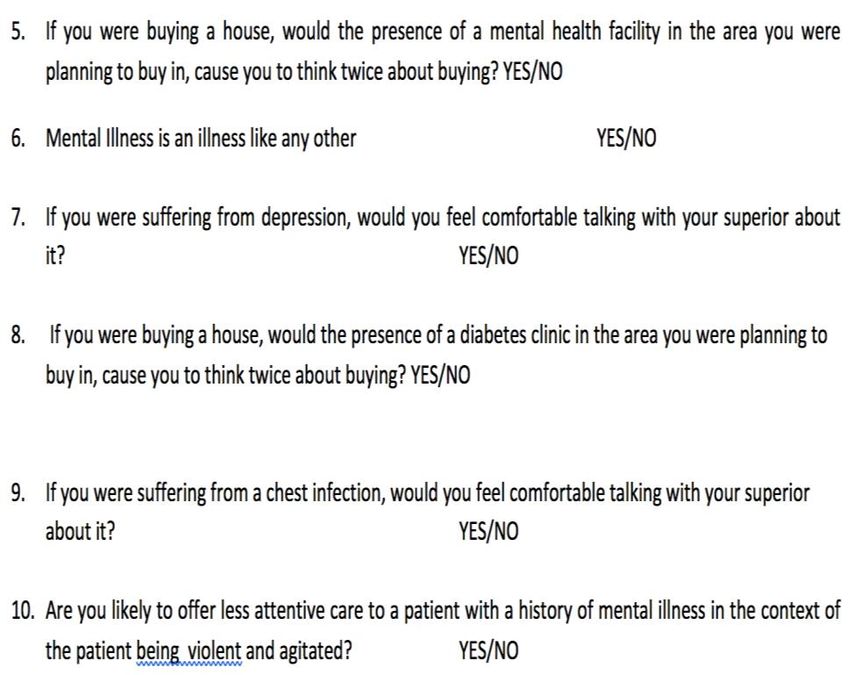
PRE POSTATTITUDE BASED QUESTIONS
Have the participants
changed their views Attitude Based Questions (%)
towards mental co- 100.0
p=0.8 p=0.11 p=0.0001 p=0.01
90.0
morbidity? 80.0
p=0.061 p=0.013
76.3 76.7
81.3 79.7
72.2 73.9
72.0
70.0 68.0
63.5 63.9
60.0
53.151.6
50.0
40.0
30.0
20.0
10.0
0.0
Q5 Q6 Q7 Q8 Q9 Q10
PRE POSTCONFIDENCE BASED QUESTIONS
Confidence Based Questions Questions
100.0
90.0
81.8 83.8
79.2
85.8 85.0
11 Risk assessment in suicidal
80.0
66.6
73.8
67.9
73.2 72.9 patient
70.0
60.0 12 Screening for depression
50.0
13 Managing an agitated
40.0 patient
30.0
14 Managing a patient at the
20.0
10.0
end of life
0.0 15 Breaking bad news
Q11 Q12 Q13 Q14 Q15
PRE POST
Highly statistically significant
p=0.0001
improvement in confidence
for each stem, p=0.0001,
paired t-testQUALITATIVE FINDINGS • Trainees Don’t actually get to practice Breaking Bad News • HCA’s don’t feel supported by Nurses • All clinicians are scared to highlight difficulties with co-morbidity unless they feel able to do anything about it • People highlight that there is less active treatment of depression at the end of life
CAMHELS
• Better integration
between cancer, mental
health and EoLC
CANCER • EDUCATIONALLY
CLINICALLY
• RESEARCH
• SERVICE DESIGN
Mental End of
health Life
• Better Collaboration
internally and
internationally (Aus, SL)L O N D O N I N T E G R AT E D PAT H W AY F O R C A N C E R P S Y C H O S O C I A L S U P P O R T
as per NICE IOG 2004
NICE Level 1 NICE Level 2 General Hospital
Holistic Liaison Psychiatry
All hospital staff Level 2 assessment
hospital
e.g. clinic, ward, administrative
Needs 1 & first-line input 2
Plan
e.g. by Clinical Nurse Specialist
NICE Level 3&4
PERSONALISED CARE
Psycho-oncology team
(incl. counselling, clinical psychology,
oncology psychiatry, psychotherapy etc)
support for
self-management
information resources
4
consultation
social prescribing training &
Patients & third sector supervision
Carers
social care
digital Level 3/4
Community Palliative
community
Care Services specialists
IAPT - Community
Primary Care
Psychological Therapies
Cancer
GPs, primary care staff & ‘care Care 3
navigator’ roles Plan
Comm. & Specialist
Mental Health
C specialist support
B enhanced support
A universal support
V5.6L O N D O N I N T E G R AT E D PAT H W AY F O R C A N C E R P S Y C H O S O C I A L S U P P O R T
as per NICE IOG 2004
NICE Level 1 NICE Level 2 General Hospital
Holistic Liaison Psychiatry
All hospital staff Level 2 assessment
hospital
e.g. clinic, ward, administrative
Needs 1 & first-line input 2
Plan
e.g. by Clinical Nurse Specialist
NICE Level 3&4
PERSONALISED CARE
Psycho-oncology team
(incl. counselling, clinical psychology,
oncology psychiatry, psychotherapy etc)
support for
self-management
information resources
4
social prescribing
Patients & third sector
Carers
social care
digital Level 3/4
Community Palliative
community
Care Services specialists
IAPT - Community
Primary Care
Psychological Therapies
Cancer
GPs, primary care staff & ‘care Care 3
navigator’ roles Plan
Comm. & Specialist
Mental Health
C specialist support
B enhanced support
A universal support
V5.6A universal support B enhanced support
C specialist support
Healthcare system all Level 1 care, plus:
all Level 1&2 care, plus:
• underlying principle: how to prevent distress and promote adjustment Level 2
• prompt, efficient, reliable systems e.g. for appointments and reporting • specialist clinical assessment of distress &
• assessment of significant distress &
• effective communication between staff/services across the pathway mental health in the context of cancer
psychological issues identified in HNA or
• developing a comprehensive biopsychosocial
routine cancer care
Level 1 care – All psychological formulation or multidimensional
• first-line psychological interventions to
diagnostic profile
• compassionate communication enhance self-management e.g. relaxation,
• active listening worry tree, structured problem-solving,
Level 3
• timely information, advice and links with social care e.g regarding motivational interviewing
employment, finances, benefits etc • consultation and advice from specialist • assess and deliver interventions with complex
• facilitating access to peer support, open groups, online forums, service (e.g. Level 3-4 psycho-oncology presentations that include cancer and
• third sector organisations service to guide Level 2 input) psychosocial factors
• social prescribing • signposts/refers to specific cancer • psychological interventions e.g. counselling,
• digital resources psychological care resources e.g. structured solution-focused therapy, focused on cancer-
support groups related difficulties
Keyworker – e.g. clinical nurse specialist
Community • IAPT Step 3: High-intensity unidisciplinary
• meets person at diagnosis to establish a reliable relationship
interventions (non-cancer specific) e.g. CBT,
• develops a holistic understanding of the impact of cancer on the person • Primary Care-level 2 support from a trained
counselling for depression.
• maintains a reliable single point of contact throughout primary care nurse/other professional
• guides the person in effective self-management • IAPT Step 2 : low-intensity interventions, e.g.
Level 4
• identifies needs, signposts to specific resources and reviews impact guided self-help for anxiety or depression,
• advocates psychosocial perspective in MDT psycho-educational groups, computerised • embedded within cancer MDT input
CBT (non-cancer specific) • assess and intervene with complex
Personalised care psychological, psychotherapeutic or
pharmacological interventions
• HNA – holistic needs assessment and care plan, at key points in
• management of non-acute risk
pathway
• enabling effective liaison of mental health &
• EOT – end of treatment review, includes HNA and treatment summary
related services to cancer MDT
(TS)
• HWBE – health & wellbeing event
• CCR – cancer care review in primary careReferral Criteria (i)
Acute/Hospital Context
1 Level 1 > 2 2 Level 2 > Psycho-oncology
All staff to request or implement Level 2 input when: Clinical judgement, taking into account:
• HNA or other screening identifies heightened distress (e.g. DT>5, • Keyworker observes pattern of poor psychological adjustment
GAD/PHQ>9) over time
• patient or carer self-identify poor coping or psychological issues • Level 2 assessment identifies significant severity, persistence and
that affect function functional impact of distress, and background complexities/
• clinical impression of persistent significant distress in clinical vulnerabilities e.g. trauma, multiple losses, relevant mental
encounters health history
• clinician concerns about difficulties with decisions, adherence, • Level 2 input (e.g. ‘worry tree’, sleep hygiene) has not proved
treatments. sufficient
• Holistic care requires multiprofessional coordination
• When there is clinical evidence of significant concerns relating (hospital/mental health) and/or multidisciplinary input (e.g.
to treatment, mental health or risk, direct referral to Level 3/4 psychosexual rehabilitation)
would be appropriate.Referral Criteria (ii)
Primary / Community Context
3 GP > Psycho-oncology GP > IAPT
Clinical judgement, taking into account: Clinical judgement, taking into account:
• undergoing active cancer tests & treatments, or • Meets general criteria for IAPT g mild/moderate anxiety
unstable/advancing/progressive disease and/or depression
• significant cancer /treatment consequences (e.g. epilepsy, • Medically stable/cancer remission/cancer ‘in the
GvHD, neutropenia, dysphagia), requiring multidisciplinary
background’
input.
• Few hospital cancer-related contacts/routine follow up
• Frequent and/or ongoing hospital contact for cancer care
• Nil or mild/well-managed physical consequences of
• Psychosocial factors impacting adversely on:
treatment
- accessing cancer tests/treatment adherence
• link to pre-existing issues, e.g. previous anxiety disorder
-decision-making (e.g treatment decisions )
-health self-management (e.g medication adherence_ - re-activated by cancer uncertainty
-cancer rehab • unidisciplinary input sufficient
• requires multiprofessional coordination with cancer mdt and • No acute mental health risk concerns
other services (e.g. mental health) and/or multidisciplinary
input (e.g. psychosexual rehabilitation)
• Usually seen for up to 12-18 months after End Of TreatmentReferral Criteria (iii)
Psycho-oncology teams leading service coordination and sharing
4
expertise across the pathway
Psycho-oncology teams will :
• Across the whole pathway, coordinate and collaborate with other enhanced & specialist
services (e.g. general hospital liaison psychiatry, community and specialist mental health,
palliative care, primary care, IAPT, third-sector providers and others) to ensure the
delivery of personalised care with a safe, individualised, comprehensive and clear plan.
• provide consultation, expert advice and training on cancer and psychological issues to a
range of professionals across the whole pathway
The aim of this function overall will be to ensure:
• patients are offered all relevant choices
• all people with pre-existing SMI have optimal cancer treatment
• GPs , primary care staff and cancer MDTs are offered clear and reliable advice on how
cancer care and mental health / psychological care will be coordinatedCONCLUSIONS • Delivering Integrated services for Mental health and Cancer • supporting the mental health needs of people living with and beyond cancer • Our experience and my role as a Macmillan Consultant Liaison Psychiatrist • Cancer Simulation and Education • Interactive Discussion - what does good look like? What should we be measuring?
REFERENCES
• Naylor, C., Parsonage, M., McDaid, D., Knapp, M., Fossey, M., & Galea, A. (2012). The Kings Fund. Long term conditions and mental health. The cost of
comorbidities.
• Dalton, S. O., Mellemkjær, L., Olsen, J. H., Mortensen, P. B., & Johansen, C. (2002). Depression and cancer risk: a register-based study of patients
hospitalized with affective disorders, Denmark, 1969–1993. American journal of epidemiology, 155(12), 1088-1095.
• Hung, Y. N., Yang, S. Y., Huang, M. C., Lin, S. K., Chen, K. Y., Kuo, C. J., & Chen, Y. Y. (2014). Cancer incidence in people with affective disorder:
nationwide cohort study in Taiwan, 1997–2010. The British Journal of Psychiatry, 205(3), 183-188.
• Lichtermann, D., Ekelund, J., Pukkala, E., Tanskanen, A., & Lönnqvist, J. (2001). Incidence of cancer among persons with schizophrenia and their
relatives. Archives of general psychiatry, 58(6), 573-578.
• Mitchell AJ, et al. The lancet oncology 2011;12(2):160–174
• Massie MJ. J Natl Cancer Inst Monogr 2004;32:57–71
• Walker J, et al. The Lancet Psychiatry 2014;1(5):343–350
• Sharpe, M., Walker, J., Hansen, C. H., Martin, P., Symeonides, S., Gourley, C., ... & Murray, G. (2014). Integrated collaborative care for comorbid
major depression in patients with cancer (SMaRT Oncology-2): a multicentre randomised controlled effectiveness trial. The Lancet, 384(9948),
1099-1108.
• Meijer, A., Roseman, M., Milette, K., Coyne, J. C., Stefanek, M. E., Ziegelstein, R. C., ... & de Jonge, P. (2011). Depression screening and patient
outcomes in cancer: a systematic review. PLoS One, 6(11), e27181.
• Strong, V., Sharpe, M., Cull, A., Maguire, P., House, A., & Ramirez, A. (2004). Can oncology nurses treat depression? A pilot project. Journal of
advanced nursing, 46(5), 542-548.
• Rayner, L., Lee, W., Price, A., Monroe, B., Sykes, N., Hansford, P., ... & Hotopf, M. (2011). The clinical epidemiology of depression in palliative care
and the predictive value of somatic symptoms: cross-sectional survey with four-week follow-up. Palliative Medicine, 25(3), 229-241.
• Parpa, E., Tsilika, E., Gennimata, V., & Mystakidou, K. (2015). Elderly cancer patients’ psychopathology: a systematic review: aging and mental health.
Archives of gerontology and geriatrics, 60(1), 9-15.
Cancer Psychiatry 2019REFERENCES
• Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta psychiatrica scandinavica, 67(6), 361-370.
• Zung, W. W. (1965). A self-rating depression scale. Archives of general psychiatry, 12(1), 63-70.
• Walker, J., Postma, K., McHugh, G. S., Rush, R., Coyle, B., Strong, V., & Sharpe, M. (2007). Performance of the Hospital Anxiety and
Depression Scale as a screening tool for major depressive disorder in cancer patients. Journal of psychosomatic research, 63(1), 83-91.
• Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ‐9: validity of a brief depression severity measure. Journal of general
internal medicine, 16(9), 606-613.
• Lloyd-Williams, M., Friedman, T., & Rudd, N. (2000). Criterion validation of the Edinburgh Postnatal Depression Scale as a screening
tool for depression in patients with advanced metastatic cancer. Journal of pain and symptom management, 20(4), 259-265.
• Pitman, A., Suleman, S., Hyde, N., & Hodgkiss, A. (2018). Depression and anxiety in patients with cancer. Bmj, 361, k1415.
• Breitbart, W., Rosenfeld, B., Tobias, K., Pessin, H., Ku, G. Y., Yuan, J., & Wolchok, J. (2014). Depression, cytokines, and pancreatic
cancer. Psycho‐oncology, 23(3), 339-345.
• Delattre, J. Y., Krol, G., Thaler, H. T., & Posner, J. B. (1988). Distribution of brain metastases. Archives of neurology, 45(7), 741-744.
• Darnell, R., Darnell, R. B., & Posner, J. B. (2011). Paraneoplastic syndromes (Vol. 79). OUP USA.
• Robinson, D., Renshaw, C., Okello, C., Møller, H., & Davies, E. A. (2009). Suicide in cancer patients in South East England from 1996
to 2005: a population-based study. British journal of cancer, 101(1), 198.
• Robson, A., Scrutton, F., Wilkinson, L., & MacLeod, F. (2010). The risk of suicide in cancer patients: a review of the literature.
Psycho‐oncology, 19(12), 1250-1258.
• Warrington, T. P., & Bostwick, J. M. (2006, October). Psychiatric adverse effects of corticosteroids. In Mayo Clinic Proceedings (Vol. 81,
No. 10, pp. 1361-1367). Elsevier.
• Hodgkiss, A. (2016). Biological psychiatry of cancer and cancer treatment. Oxford University Press.
Cancer Psychiatry 2019DELIVERING AN INTEGRATED SERVICE FOR
CANCER PATIENTS.
– NO HEALTH WITHOUT MENTAL HEALTH
Dr Asanga Fernando @asangafern
Macmillan Consultant Liaison (Cancer) Psychiatrist &
Clinical Director of simulation & clinical skills,
St George’s University Hospitals NHSYou can also read