Depressive Symptoms and AIDS-Related Mortality Among a Multisite Cohort of HIV-Positive Women
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
RESEARCH AND PRACTICE
Depressive Symptoms and AIDS-Related Mortality
Among a Multisite Cohort of HIV-Positive Women
| Judith A. Cook, PhD, Dennis Grey, BA, Jane Burke, MS, Mardge H. Cohen, MD, Alejandra C. Gurtman, MD, Jean L. Richardson, DrPH,
Tracey E. Wilson, PhD, Mary A. Young, MD, and Nancy A. Hessol, MSPH
Previous research has confirmed associations
Objectives. We examined associations between depressive symptoms and
between depression and immune suppression AIDS-related mortality after controlling for antiretroviral therapy use, mental
and other negative health outcomes, such as health treatment, medication adherence, substance abuse, clinical indicators,
disability and mortality.1–3 Recently, attention and demographic factors.
has turned to the effects of depression on the Methods. One thousand seven hundred sixteen HIV-seropositive women com-
health of individuals whose immune systems pleted semiannual visits from 1994 through 2001 to clinics at 6 sites. Multivari-
have been affected by HIV infection. Yet, the ate Cox and logistic regression analyses estimated time to AIDS-related death and
relationship between depression and HIV dis- depressive symptom severity.
ease progression is not well understood. For Results. After we controlled for all other factors, AIDS-related deaths were
example, Sambamoorthi et al.4 found relation- more likely among women with chronic depressive symptoms, and symptoms
were more severe among women in the terminal phase of their illness. Mental
ships between depression and HIV infection
health service use was associated with reduced mortality.
status, declines in immune function, acceler-
Conclusions. Treatment for depression is a critically important component of
ated disease progression, increased disability, comprehensive care for HIV-seropositive women, especially those with end-stage
shorter survival, and greater probability of disease. (Am J Public Health. 2004;94:1133–1140)
death. Conversely, studies by Lyketsos et al.5
and Vedhara et al.6 challenge the characteri-
zation of depression as an independent or
even a significant determinant of HIV disease Study (HERS)14—has confirmed a link be- than surviving women of meeting criteria for
progression. An additional complicating factor tween chronic depressive symptomatology depression at the 2 study visits preceding
has been suggested by a recent study that and poor AIDS-related outcomes. Among a their deaths?
found use of protease inhibitors reduces both cohort of HIV-seropositive women who were
depressive and clinical symptoms.7 followed from 1993 through 2000 (demo- METHODS
The existence of a potential association graphic and clinical factors were controlled),
between women’s depression and HIV dis- the women who had chronic depressive Study Background
ease progression is of interest to both health symptoms were twice as likely to die as the Between October 1994 and November
care providers and patients for several rea- women who reported no depressive symp- 1995, 2059 HIV-seropositive women were
sons. First, women’s rate of depression is toms or only intermittent ones. enrolled in the Women’s Interagency HIV
twice as high as that of men among the gen- We attempted to replicate and expand the Study (WIHS) at 6 medical and university
eral population.8 Second, HIV-seropositive HERS cohort findings by using the same vari- consortia sites nationwide: Brooklyn, NY;
women who have high levels of depressive able definitions and types of statistical analy- Bronx, NY; Chicago, Ill; Los Angeles, Calif;
symptomatology are significantly less likely ses and by exploring the effects of 3 addi- San Francisco, Calif; and Washington, DC.
to use highly active antiretroviral therapies.9 tional factors: adherence to highly active Over the next 7.5 years, participants com-
Third, depression is associated with poor antiretroviral treatment (HAART) and other pleted WIHS study visits at 6-month inter-
adherence to antiretroviral treatment regi- HIV-related therapies, use of mental health vals. Specific responses to items in the inter-
mens,10,11 which in turn is associated with services, and occurrence of depressive symp- view protocol prompted interviewers to offer
poor disease outcomes, such as mortality.12 toms during the terminal phase of AIDS- respondents referrals to medical or psychoso-
Finally, depression is a significant predictor related illness. Three research questions were cial services, such as gynecologic care or sub-
of non–AIDS-related deaths (e.g., those addressed. First, do depressive symptoms pre- stance abuse treatment.
caused by accident, drug overdose, violence, dict time to AIDS-related mortality among a
and non–AIDS-associated malignancies) cohort of HIV-seropositive women? Second, Measures
among HIV-seropositive women.13 does use of mental health services lower the Depressive symptoms. We used the Center
Only 1 previous study of a cohort of HIV- likelihood of AIDS-related mortality? Third, for Epidemiologic Studies Depression Scale
seropositive women—the longitudinal study do women in the terminal phase of their (CES-D),15 a 20-item Likert-scaled instrument,
of the 4-site HIV Epidemiologic Research AIDS-related illnesses show higher likelihood to assess depressive symptoms. The CES-D
July 2004, Vol 94, No. 7 | American Journal of Public Health Cook et al. | Peer Reviewed | Research and Practice | 1133 RESEARCH AND PRACTICE
has excellent reliability, validity, and factor lies or friends. Deaths were classified as caused tor of mortality distinct from treatment. Men-
structure among numerous subgroups,15 and by AIDS if the cause was an AIDS-defined tal health service use was defined as receipt
it is commonly used in studies of HIV popula- opportunistic infection/malignancy (consistent of care from a mental health professional or
tions, including women.7 Its sensitivity for the with 1993 Centers for Disease Control and counselor that was self-reported at 1 or more
Diagnostic and Statistical Manual of Mental Prevention clinical surveillance conditions), or study visits. Indicator variables represented 5
Disorders, Third Edition16 (DSM-III), diagnosis if the stated cause was organ failure or non- of the 6 study sites; Chicago served as a sixth
of major depression is excellent, in the 80% specific infection and the CD4 count at the arbitrary reference category.
to 90% range, with somewhat lower speci- last study visit was less than 200 cells per
ficity (70%–80%).17,18 In an earlier analysis milliliter. This methodology has been de- Statistical Analysis
of the WIHS cohort’s level of depressive scribed elsewhere.13 We analyzed 13 waves of semiannual data
symptoms, Cook et al.9 demonstrated that Independent measures. Women were con- from the HIV-seropositive sample of the
various ways of analyzing the CES-D (the sidered to be on a HAART regimen if they WIHS to predict time to AIDS-related death.
standard cutoff of 16, a more stringent cutoff followed the International AIDS Society– We used the Kaplan–Meier survival analysis
of 23, and an interval-level version of the USA panel20 and the US Department of to test for differences in survival function ac-
subscale that excluded somatic items similar Health and Human Services/Henry J. Kaiser cording to depressive symptom chronicity,
to HIV symptoms) produced virtually identi- Family Foundation Panel21 guidelines. All and we used proportional hazards analysis
cal associations with antiretroviral therapy use other antiretroviral therapy combinations to examine the effect of depressive symp-
and with the woman’s demographic charac- were defined as non-HAART combination toms after we controlled for potentially con-
teristics. Thus, the standard cutoff score of 16 therapy, and use of a single antiretroviral founding factors. Data from women whose
was used in our study. therapy was defined as monotherapy. deaths were caused by non–AIDS-related
We used 2 measures of longitudinal depres- At each study visit, HIV antibody status, causes (n = 144) were retained in the analy-
sive symptoms to test the study hypotheses. HIV-1 RNA, and CD4 T-lymphocyte count sis until the time of death, when they were
First, following Ickovics et al.,19 depression were determined with standard flow cytome- right-censored. We used multiple logistic re-
chronicity was defined as the proportion of try at laboratories participating in the Na- gression analysis to predict the likelihood of
study visits at which the women’s self-reported tional Institutes of Health (NIH) Quality As- meeting “probable depression” criteria at the
CES-D scores met or exceeded the clinical surance Program. Viral load was classified as final 2 study visits for all women to examine
cutoff for probable cases of depression. In this less than 4000 versus greater than 4000. the association between depressive symptoms
operationalization, or way of computing a de- CD4 levels were assessed as low (< 200), and end-stage disease.
pressive symptom variable, scores that indi- moderate (200–500), and high ( > 500).
cated depression at 75% or more of the study Study participants’ race/ethnicity was cate- RESULTS
visits were classified as chronic, 26% to 74% gorized as African American, Hispanic/Latina,
were classified as intermittent, and no more White, and other. Illicit drug use was catego- Sample characteristics. Participants who had
than 25% were classified as none or few. Sec- rized as use of crack, cocaine, or heroin at less than 3 study visits (n = 343) were ex-
ond, following Lyketsos et al.’s5 “conservative” any time during the study. Those with high cluded from the sample so depression chronic-
definition, scores of 16 or higher on the CES-D school degrees or any postsecondary educa- ity could be assessed longitudinally. When
at 2 consecutive study visits were used to de- tion at baseline were coded as “1” and as “0” compared with the women who were in-
fine recent depression. In our study, this was otherwise. Age at baseline was measured in cluded in the analysis (n = 1716), those with
operationalized as scoring above the cutoff decades. Employment status at baseline was less than 3 study visits were significantly less
(1) at the last 2 study visits preceding death defined as any paid work (full- or part-time). likely to be employed (13% vs 22%) or to
among women with AIDS-related deaths, and Presence of clinical symptoms at baseline in- have used a HAART regimen for 12 or more
(2) at the last 2 study visits completed for all cluded 1 or more HIV/AIDS-related symp- months (1% vs 49%). The 2 groups did not
surviving women. The first operationalization toms: fever, diarrhea, memory problems, differ significantly on any other variables. The
of depression chronicity was used to test hy- numbness, weight loss, confusion, and night demographic characteristics of the study’s
potheses 1 and 2, and the second operational- sweats. Women who reported nonadherence 1716 women at baseline closely resembled
ization of recent depression was used to test hy- to any HIV treatment at any study visit were those of the larger HIV-seropositive WIHS
pothesis 3. classified as nonadherent and as adherent cohort.23 Two fifths (41%) reported illicit drug
AIDS-related mortality. Information was otherwise. This single-item operationalization use before baseline, and 39% did so during
collected on all participants’ deaths, malignan- is similar to one that was used successfully by the study. Baseline CD4 counts were below
cies, tuberculosis, and AIDS. Cause of death Wilson et al.22 in a previous analysis of med- 200 cells for 25% of the women, and viral
was coded from death certificates and from ication adherence among the WIHS cohort. loads were greater than 4000 for 68%. Use
information obtained electronically via the Those women who reported no HIV-related of a HAART regimen for 1 year or more was
National Death Index, local death registries, therapies were included in the adherent clas- reported by 49% of the women, and 14% re-
hospital records, physician reports, and fami- sification, because nonadherence is a predic- ported use of a non-HAART combination
1134 | Research and Practice | Peer Reviewed | Cook et al. American Journal of Public Health | July 2004, Vol 94, No. 7 RESEARCH AND PRACTICE
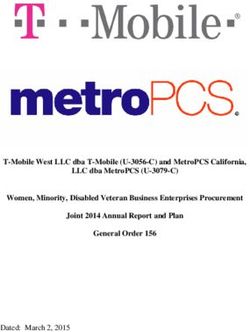
therapy for 1 year or more. Only 5% re- one third of the cohort. Over two thirds symptoms. These curves differ significantly
ported use of monotherapy for 1 year or (69%) reported use of mental health services (log-rank test = 20.22, df = 2, P < .001 ), which
more, and 32% reported no use of an anti- at 1 or more study visits. indicates that chronic depression predicts
retroviral therapy or use for less than 1 year. Relationship between depressive symptoms mortality. Whereas only 6% of the women
At baseline, more than half (58%) the and time to death. Two hundred ninety-four who had few or no depressive symptoms, and
women reported HIV-related clinical symp- (17%) of the women died during the 13 only 7% of the women who had intermittent
toms. Less than half (45%) were classified as waves of study visits completed over a symptoms, died from AIDS-related causes,
adherent at all study visits; 37% reported 7.5-year period by 1716 women: 147 (9%) nearly double this proportion (13%) of the
perfect adherence, and 8% reported no treat- died from AIDS-related causes, and an addi- women who had chronic depressive symp-
ment. For the remaining 55%, the mean tional 147 women (9%) died as a result of toms did die from AIDS-related causes. We
number of visits at which nonadherence was other causes (accidents, violent crime, sui- eliminated the somatic symptoms from the
reported was 3. cide, or non–HIV-related diseases). Of those depression measure but retained a cutoff of
Approximately one third of the women who died from AIDS-related causes, 66% 16 to test a more stringent measure of
(32%) reported depressive symptoms at a had CES-D scores greater than or equal to chronic depressive symptoms, which pro-
level that exceeded the CES-D clinical cutoff 16 at their last study visit (the mean number duced virtually identical results (log-rank
at 75% or more of their study visits. Another of days between death and last visit was test = 12.94, df = 2, P < .01) .
third (37%) reported depressive symptoms 146), and 52% had CES-D scores that ex- Relationships among mortality and depres-
intermittently, and the final third (31%) re- ceeded the cutoff at their last 2 visits before sive symptoms and baseline features. The third
ported depressive symptoms at few or none death. column of Table 1 shows bivariate odds ra-
of their study visits. Close to half the women Figure 1 shows the Kaplan–Meier survival tios for AIDS-related mortality and other po-
(47%) exceeded the CES-D clinical cutoff at curves for mortality caused by AIDS for each tential predictors. Women who had chronic
their last study visit, and one third (35%) did of the 3 groups of women: those with chronic depressive symptoms were more than twice
so at their last 2 consecutive visits, which in- depressive symptoms, those with intermittent as likely to die compared with those who
dicated recent depression among one half to symptoms, and those with infrequent or no had limited or no symptoms. AIDS-related
mortality also was more likely among those
who received monotherapy and those who
had low baseline CD4 cell counts, high viral
1.0 loads, and HIV-related symptoms at base-
line. Mortality was less likely among those
who reported mental health service use and
those who were on a HAART regimen or a
non-HAART combination therapy. Mortality
Cumulative Survival
also was associated with adherence, which
0.9 was a counterintuitive finding most likely
caused by the fact that women who had
more advanced disease were more likely to
have initiated therapy. None of the other
model variables was associated with AIDS-
related mortality.
0.8 Little or no depression We used a Cox proportional hazards
Intermittent depression model to estimate the effect of depressive
Chronic depression
symptom chronicity on mortality after we
controlled for all other model variables. As
shown in the last column of Table 1, the
women who had chronic depressive symp-
0.7 toms were significantly more likely to die
0 1 2 3 4 5 6
compared with the women who had intermit-
Years in Study tent or fewer symptoms. The remaining re-
sults mirror those of the bivariate analysis,
except that the positive association between
FIGURE 1—Kaplan–Meier survival curves, stratified by level of depressive symptoms.
mortality and adherence became nonsignifi-
cant (because of its spurious nature), as did
relationships between mortality and HIV
July 2004, Vol 94, No. 7 | American Journal of Public Health Cook et al. | Peer Reviewed | Research and Practice | 1135 RESEARCH AND PRACTICE
TABLE 1—Bivariate and Multivariate Associations Among AIDS-Related Mortality, Depressive symptoms and mortality and monotherapy.
Symptoms, and Confounding Factors Among HIV-Positive Women (N = 1716) Several potential interactions between model
variables were tested and were found to be
AIDS-Related Bivariate Odds Multivariate Relative nonsignificant: an interaction between de-
Variable Deaths, No. (%) Ratio (95% CI) Riska (95% CI)
pression and mental health service use and
Level of depression interactions between adherence and use of
Limited/no symptoms (n = 543) 35 (6) Reference different categories of HIV therapies.
Intermittent symptoms (n = 629) 43 (7) 1.1 (0.7, 1.7) 1.0 (0.6, 1.6) Finally, because of the time frame of our
Chronic symptoms (n = 534) 68 (13) 2.2 (1.4, 3.3) 1.7 (1.1, 2.7) study, it is possible that these results are bi-
Mental health service utilization ased by the fact that HAART became avail-
Used services during 82 (7) 0.5 (0.4, 0.7) 0.5 (0.3, 0.7) able only to those who survived for longer
study (n = 1187) periods of time. To control for this potential
No service use (n = 529) 65 (12) Reference bias, we restricted the sample to those women
Baseline CD4 cell count who were alive during the second half of
< 200 (n = 409) 104 (25) 27.9 (11.4, 68.6) 36.0 (13.9, 93.8) 1996 (because protease inhibitors became
200–500 (n = 785) 33 (4) 4.0 (1.6, 10.2) 4.7 (1.8, 12.3) commercially available at the beginning of
> 500 (n = 468) 5 (1) Reference 1996) and repeated the Cox regression analy-
Baseline viral load sis. The results (data not shown) were virtu-
≤ 4000 (n = 536) 5 (1) Reference ally identical to those in Table 1.
> 4000 (n = 1166) 142 (12) 13.8 (5.6, 33.6) 6.8 (2.7, 16.9) Relationships among depressive symptoms
Baseline HIV symptoms immediately preceding death, mortality, and
0 (n = 714) 42 (6) Reference confounding variables. While depressive symp-
≥ 1 (n = 999) 105 (11) 1.9 (1.3, 2.7) 1.3 (0.8, 1.9) tom chronicity is associated with mortality
Categorized antiretroviral therapy use owing to AIDS-related causes, the chronicity
during study measure fails to capture the level of depres-
Other (n = 554) 81 (15) Reference sive symptoms immediately before death. For
Monotherapy ≥ 12 mos (n = 93) 27 (29) 2.4 (1.6, 3.7) 0.8 (0.5, 1.3) example, the chronicity score of a woman
Non-HAART combination antiretroviral 17 (7) 0.4 (0.3, 0.7) 0.3 (0.1, 0.5) who exceeded the CES-D clinical cutoff at
therapy ≥ 12 mos (n = 231) the first 2 study visits but not the last 2 visits
HAART ≥ 12 mos (n = 838) 22 (3) 0.1 (0.1, 0.2) 0.1 (0.0, 0.1) would be identical to that of a woman who
Adherence to HIV treatment regimen exceeded the cutoff at the last 2 study visits
Adherence reported at every 82 (11) 1.7 (1.2, 2.3) 1.5 (1.0, 2.1) but not the first 2. To examine the effect of
visit (n = 775)
depressive symptoms during the immediate
Nonadherence at ≥ 1 65 (7) Reference
premortality period, we computed the propor-
visit (n = 938)
tions of women who met criteria for probable
Crack, cocaine, heroin use during study
depression at each study visit separately for
Any use (n = 663) 63 (10) 1.2 (0.9, 1.6) 0.9 (0.6, 1.4)
those who died from AIDS-related causes
No use (n = 1053) 84 (8) Reference
during the subsequent 6 months versus those
Baseline age, y
who survived until the next study visit. The
< 30 (n = 331) 27 (8) Reference
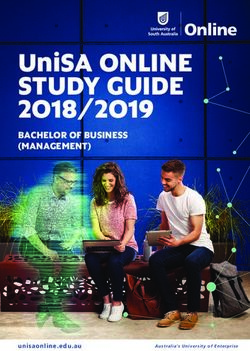
results (Figure 2) indicated that the propor-
30–39 (n = 829) 67 (8) 1.0 (0.6, 1.6) 0.7 (0.4, 1.2)
tion of women who had probable depression
40–49 (n = 469) 44 (9) 1.1 (0.7, 1.9) 0.7 (0.4, 1.2)
was higher among those who died during the
50–59 (n = 75) 8 (11) 1.5 (0.7, 3.2) 0.8 (0.4, 1.9)
following 6 months than among those who
≥ 60 (n = 12) 1 (8) 1.1 (0.1, 8.0) 0.7 (0.1, 5.7)
survived.
Employment status
Next, we used logistic regression analysis to
Not employed (n = 1334) 127 (10) Reference
examine the multivariate statistical association
Employed (n = 381) 20 (5) 0.8 (0.6, 1.0) 0.9 (0.5, 1.6)
between depressive symptoms and being in
Education
the terminal phase of AIDS-related illnesses.
At least high school or 87 (8) 0.8 (0.6, 1.2) 1.1 (0.7, 1.6)
Level of depressive symptoms was the depen-
equivalent (n = 1080)
dent measure, and we used Lyketsos et al.’s5
Less than high school (n = 636) 60 (9) Reference
“conservative” definition of meeting the
Continued CES-D cutoff at 2 consecutive study visits.
These were the last 2 study visits completed
1136 | Research and Practice | Peer Reviewed | Cook et al. American Journal of Public Health | July 2004, Vol 94, No. 7 RESEARCH AND PRACTICE
ent, who were employed, who had a high
TABLE 1—Continued
school or equivalent education, and who lived
Marital status in their own homes.
Married/living as married (n = 628) 57 (9) 1.1 (0.8, 1.6) 1.3 (0.9, 1.9) A multivariate logistic regression analy-
Single (n = 1088) 90 (8) Reference sis that controlled for all other factors
Residential status found that recent clinically significant lev-
Living in own home (n = 1193) 104 (9) 1.1 (0.8, 1.5) 1.1 (0.7, 1.6) els of depressive symptoms were associ-
Living elsewhere (n = 522) 43 (8) Reference ated with being in the terminal stage of ill-
Income status ness, using mental health services, having
< $12 000/year (n = 1103) 100 (9) 1.2 (0.8, 1.7) 1.0 (0.6, 1.5) HIV-related symptoms, and being aged 30
≥ $12 000/year (n = 613) 47 (8) Reference to 39 years. Recent depressive symptoms
Race/ethnicity were significantly less likely among those
African American (n = 962) 97 (10) 1.6 (1.0, 2.4) 1.0 (0.6, 1.7) who had been on a HAART regimen for
Hispanic/Latina (n = 405) 27 (7) 1.0 (0.6, 1.7) 0.8 (0.4, 1.4) 12 or more months.
Other (n = 384) 23 (7) Reference
DISCUSSION
Note. N = respondents with 3 or more study visits; CI = confidence interval; HAART = highly active antiretroviral therapy.
a
Risk estimate was calculated from the Cox proportional hazards model, which associated each variable with mortality while
the effects of all other variables in the table and the study site were controlled. Chronic depressive symptoms were signifi-
cantly associated with a greater likelihood of
AIDS-related mortality, even after we con-
trolled for clinical, substance use, and socio-
by all women, excluding those who died from cant depressive symptoms also were more demographic factors. However, despite the
non–AIDS-related causes (n = 144). likely among those women who used mental impact of depressive symptoms, women who
As shown in the middle column of Table 2, health services, who had CD4 counts below received mental health services were signifi-
the women who were in the terminal phase 200 cells and viral loads above 4000, who cantly less likely to die from AIDS-related
of their AIDS-related illnesses were more had HIV-related symptoms at baseline, who causes during the study period. These results
than twice as likely to report recent clinically reported illicit drug use, who were aged 30 to point to the importance of identifying and
significant depressive symptoms. More than 49 years, who received monotherapy, who treating depression—through both pharmaco-
half (52%) of the terminally ill women, but had incomes below $12 000 per year, and logical interventions and psychotherapeutic
less than one third (32%) of the nontermi- who were Hispanic/Latina. Depressive symp- treatment—as an essential element in the
nally ill women, met the “conservative” crite- toms were less likely among women who comprehensive clinical care of women who
ria for depressive symptoms. Clinically signifi- were on a HAART regimen, who were adher- have HIV.
Additionally, not only chronicity but also
recency of depressive symptoms was asso-
100
ciated with AIDS-related mortality. Of
those in the terminal phase of their ill-
90 Died
Survived nesses, more than half met CES-D–defined
80
clinical criteria for depression at the 2
70
study visits before their deaths. The high
Percentage
60 proportion of women who reported depres-
50 sive symptoms during the terminal phase of
40 their AIDS-related illnesses shows the im-
30 portance of including treatment for depres-
20 sion in end-of-life care protocols through
10
the use of antidepressants and other treat-
ments in hospice and similar programs.
0
2 3 4 5 6 7 8 9 10 11 Antiretroviral therapies clearly affected mor-
Study Visit Number tality: those who were on a HAART regimen
for a year or more were 90% less likely to ex-
perience AIDS-related mortality, and those
FIGURE 2—Percentage of HIV-positive women who met criteria for probable depression, by
who were on a combination antiretroviral ther-
subsequent 6-month survival status.
apy for a year or more were 70% less likely.
Moreover, in our study, the proportion of
July 2004, Vol 94, No. 7 | American Journal of Public Health Cook et al. | Peer Reviewed | Research and Practice | 1137 RESEARCH AND PRACTICE
TABLE 2—Bivariate and Multivariate Associations Among Depressive Symptoms, AIDS- women who reported recent depressive symp-
Related Mortality, and Confounding Factors Among HIV-Positive Women (N = 1569) toms was lowest among those who were on a
HAART regimen. The significantly lower pro-
Met Criteria for Clinical Bivariate Odds Multivariate Odds portion of women who had depressive symp-
Variable Depression, No. (%) Ratio (95% CI) Ratioa (95% CI)
toms among users of the most potent antiretro-
Stage of illness viral therapies shows the possible role of a
Teminal (n = 147) 76 (52) 2.3 (1.6, 3.3) 1.8 (1.1, 2.7) HAART regimen in combating depression7,24
Not terminal (n = 1422) 451 (32) Reference along with or in addition to the role of positive
Mental health service utilization mental health in promoting use of a HAART
Used services during 418 (39) 2.2 (1.7, 2.8) 2.2 (1.6, 2.9) regimen. Also important are associations be-
study (n = 1085) tween depression and AIDS-related mortality
No service use (n = 484) 109 (23) Reference in the context of unique factors related to
Baseline CD4 cell count women’s use of HAART regimens, such as
< 200 (n = 361) 142 (40) 1.4 (1.1, 1.9) 1.2 (0.8, 1.8) health insurance status,25 which could poten-
200–500 (n = 720) 232 (32) 1.0 (0.8, 1.4) 1.1 (0.8, 1.4) tially influence their access to both HIV and
> 500 (n = 439) 136 (31) Reference depression treatments.
Baseline viral load Our study’s methodology did not allow us
≤ 4000 (n = 502) 143 (28) Reference to establish a cause-and-effect relationship be-
> 4000 (n = 1046) 374 (36) 1.4 (1.1, 1.8) 1.2 (0.9, 1.5) tween depression and mortality, because both
Baseline HIV symptoms may be related to disease progression. How-
0 (n = 666) 132 (20) Reference ever, the multivariate survival analysis con-
≥1 (n = 900) 395 (44) 3.3 (2.6, 4.0) 2.4 (1.8, 3.0) trolled for 2 potent clinical indicators of HIV
Categorized antiretroviral therapy disease status (HIV viral load and CD4 cell
use during study count), and the significant relationship be-
Other (n = 490) 186 (38) Reference tween mortality and depressive symptoms re-
Monotherapy ≥ 12 mos (n = 77) 41 (53) 1.8 (1.1, 3.0) 1.8 (1.0, 3.2) mained consistent despite these controls. Fur-
Non-HAART combination antiretroviral 66 (33) 0.8 (0.6, 1.1) 0.8 (0.5, 1.2) thermore, post hoc analyses (data not shown)
therapy ≥ 12 mos (n = 203) of women who did not have AIDS at baseline
HAART ≥ 12 mos (n = 799) 234 (29) 0.7 (0.5, 0.8) 0.7 (0.5, 0.9) (i.e., CD4 > 200) revealed that those who had
Adherence to HIV treatment regimen chronic depressive symptoms were 2.3 times
Adherence reported at 207 (30) 0.8 (0.6, 0.9) 0.8 (0.6, 1.0) more likely to die than those who had limited
every visit (n = 684) or no depressive symptoms (P < .05), which
Nonadherence at ≥ 1 320 (37) Reference
indicated that chronic depression was related
visit (n = 882)
to mortality even among those who did not
Crack, cocaine, heroin use
have AIDS at baseline. Finally, women who
during study
died of AIDS-related causes were significantly
Any use (n = 599) 248 (42) 1.8 (1.4, 2.2) 1.1 (0.8, 1.4)
more likely to have had CES-D scores that in-
No use (n = 970) 279 (29) Reference
dicated “probable depression” at the 2 study
Baseline age, y
visits immediately preceding their deaths,
< 30 (n = 318) 78 (24) Reference
which established the temporally proximal, if
30–39 (n = 769) 274 (36) 1.7 (1.3, 2.3) 1.5 (1.1, 2.0)
not causal, nature of depression and mortality.
40–49 (n = 405) 154 (38) 1.9 (1.4, 2.6) 1.4 (1.0, 2.1)
Two caveats to our findings concern the
50–59 (n = 59) 21 (36) 1.7 (0.9, 3.1) 1.5 (0.8, 2.8)
use of the CES-D to measure depressive
≥ 60 (n = 9) 0 (0) 0.2 (0.0, 115.6) 0.1 (0.0, 2942.0)
symptoms and the use of death certificates to
Employment status
determine cause of death. With regard to the
Not employed (n = 1201) 454 (38) Reference
first study limitation, operationalization of
Employed (n = 367) 73 (20) 0.5 (0.4, 0.6) 0.8 (0.6, 1.1)
major depression through research-quality di-
Education
agnostic tools, such as the Structured Clinical
At least high school or 300 (30) 0.6 (0.5, 0.8) 0.8 (0.6, 1.0)
Interview for the DSM or the Composite In-
equivalent (n = 1000)
ternational Diagnostic Inventory, would have
Less than high school (n = 569) 227 (40) Reference
yielded a much higher-quality measure of de-
Continued pression as a syndrome, as would diagnostic
procedures performed by a clinician who uses
1138 | Research and Practice | Peer Reviewed | Cook et al. American Journal of Public Health | July 2004, Vol 94, No. 7 RESEARCH AND PRACTICE
Requests for reprints should be sent to Judith A. Cook,
TABLE 2—Continued PhD, Mental Health Services Research Program, Depart-
ment of Psychiatry, University of Illinois at Chicago, 104
Marital status S Michigan Ave, Suite 900, Chicago, IL 60603 (e-mail:
Married/living as married (n = 587) 186 (32) 0.9 (0.7, 1.1) 1.0 (0.7, 1.2) cook@ripco.com).
This article was accepted July 18, 2003.
Single (n = 982) 341 (35) Reference
Residential status
Living in own home (n = 1096) 344 (32) 0.7 (0.6, 0.9) 0.9 (0.7, 1.1)
Contributors
J. A. Cook, D. Grey, and J. Burke designed the study, an-
Living elsewhere (n = 473) 183 (39) Reference alyzed the data, and prepared the article. M. H. Cohen,
Income status A. C. Gurtman, J. L. Richardson, T. E. Wilson, M. A.
Young and N. A. Hessol contributed to the data inter-
< $12 000/year (n = 996) 386 (39) 2.0 (1.5, 2.4) 1.4 (1.0, 1.8)
pretation and the writing of the article. All authors re-
≥ $12 000/year (n = 573) 141 (25) Reference viewed drafts of the article and contributed revisions.
Race/ethnicity
African American (n = 865) 295 (34) 1.4 (1.0, 1.8) 1.1 (0.8, 1.5) Acknowledgments
Hispanic/Latina (n = 381) 143 (38) 1.6 (1.1, 2.2) 1.2 (0.8, 1.8) The WIHS is funded by the National Institute of Allergy
Other (n = 323) 89 (28) Reference and Infectious Diseases, with supplemental funding from
the National Cancer Institute, the National Institute of
Note. N = respondents with 3 or more study visits; CI = confidence interval; HAART = highly active antiretroviral therapy. Child Health and Human Development, the National In-
a
Odds estimates were calculated from the logistic regression model, which associated each variable with depression while stitute on Drug Abuse, and the National Institute of
the effects of all other variables in the table and the study site were controlled. Craniofacial and Dental Research (U01-AI-35004,
U01-AI-31834, U01-AI-34994, U01-AI-34989,
U01-HD-32632, U01-AI-34993, U01-AI-42590,
M01-RR00079 and M01-RR00083).
Data were collected by the Women’s Interagency
HIV Study (WIHS) Collaborative Study Group with
the Diagnostic and Statistical Manual of Mental substantial proportion of deaths classified as centers (principal investigators are listed in parentheses)
Disorders, Fourth Edition (DSM-IV).26 All of non–AIDS-related and most likely reduced at the New York City/Bronx Consortium (Kathryn
these approaches are highly preferable to use chances of false-positive results.13 Anastos); Brooklyn, NY (Howard Minkoff); the Wash-
ington DC Metropolitan Consortium (Mary Young); the
of a depression screening instrument, such as Connie Wofsy Study Consortium of Northern California
the CES-D, because of the latter’s limited CONCLUSIONS (Ruth Greenblatt); the Los Angeles County/Southern
specificity. However, the measure is both California Consortium (Alexandra Levine); the Chicago
Consortium (Mardge Cohen); and the Data Coordinat-
valid and reliable and is widely used in stud- The findings of our study highlight a num- ing Center (Alvaro Munoz).
ies of HIV-positive cohorts, which enables di- ber of important and clinically meaningful as-
rect comparisons with the results of previous sociations between depressive symptoms and
Human Participant Protection
studies. Moreover, the use of rigorous scien- outcomes of women who have HIV. They The Women’s Interagency HIV Study has been ap-
tific or clinical diagnostic tools among a popu- suggest that antiretroviral therapy alone does proved by the institutional review boards of all institu-
tions involved in our study. Written informed consent
lation of this size presents considerable logisti- not meet best-practice standards of care for
was obtained from all participants.
cal challenges and requires substantial this population, and therapy must be aug-
interrater and intersite reliability procedures mented by appropriate and sensitive mental
References
to warrant its expense and its increased sub- health treatment, particularly as HIV disease 1. Reichlin S. Mechanisms of disease: neuroendocrine-
ject burden. Our study also was limited by progresses. Thus, finding ways to reduce de- immune interactions. N Engl J Med. 1993;329:
1246–1253.
our inability to determine whether the mental pressive symptoms has the potential not only
health services received by the women were to prolong life but also to enhance its quality 2. Herbert TB, Cohen S. Depression and immunity:
a meta-analytical review. Psychol Bull. 1993;113:
consistent with practice guidelines for the among women who have HIV. 472–486.
treatment of depression that are based on rig- 3. Rovner BW, German PS, Brant LJ, Clark R, Bur-
orous research findings. ton L, Folstein MF. Depression and mortality in nursing
About the Authors homes. JAMA. 1991;265:993–996.
With regard to the second caveat, the Judith A. Cook, Dennis Grey, and Jane Burke are with the
causes of death obtained from death certifi- Department of Psychiatry, University of Illinois at Chi- 4. Sambamoorthi U, Walkup J, Olfson M, Crystal S.
cago. Mardge H. Cohen is with the Cook County Hospital, Antidepressant treatment and health services utilization
cates may have been inaccurate. However, among HIV-infected Medicaid patients diagnosed with
Core Center, Chicago Ill. Alejandra C. Gurtman is with the
once again, death certificate information is Department of Medicine, Mount Sinai Medical Center, depression. J Gen Intern Med. 2000;15:311–320.
commonly used in studies of this type and New York, NY. Jean L. Richardson is with the Department 5. Lyketsos CG, Hoover DR, Guccione M, et al. De-
can provide important epidemiological infor- of Preventive Medicine, University of Southern California, pressive symptoms as predictors of medical outcomes
Los Angeles. Tracey E. Wilson is with the Department of in HIV infection. JAMA. 1993;270:2563–2567.
mation that otherwise might not be available. Preventive Medicine and Community Health, State Univer-
6. Vedhara K, Giovanni S, McDermott M. Disease
Additionally, the algorithm used in our study sity of New York Health Sciences Center at Brooklyn. Mary
progression in HIV-positive women with moderate to
enhanced the linkage of AIDS clinical indica- A. Young is with the Department of Medicine, Georgetown
severe immunosuppression: the role of depression.
University Medical Center, Washington, DC. Nancy A.
tors (CD4 cell counts, viral load) to cause of Hessol is with the Department of Medicine, University of
Behav Med. 1999;25:43–47.
death, which may have accounted for the California, San Francisco. 7. Low-Beer S, Chan K, Yip B, et al. Depressive
July 2004, Vol 94, No. 7 | American Journal of Public Health Cook et al. | Peer Reviewed | Research and Practice | 1139 RESEARCH AND PRACTICE
symptoms decline among persons on HIV protease in- immunodeficiency virus. Clin Infect Dis. 2002;34:
hibitors. J Acquir Immune Defic Syndr. 2000;23: 529–534.
295–301.
23. Barkan SE, Melnick SL, Preston-Martin S, et al.
8. Kessler RC, McGonagle KA, Swartz M, Blazer DG, The Women’s Interagency HIV Study. Epidemiology.
Nelson CB. Sex and depression in the National Comor- 1998;9(2):117–125.
bidity Survey: I. Lifetime prevalence, chronicity and re-
currence. J Affective Disord. 1993;29:85–96. 24. Judd FK, Cockram AM, Komiti A, Mijch AM, Hoy J,
Bell R. Depressive symptoms reduced in individuals
9. Cook JA, Cohen MH, Burke J, et al. Effects of de- with HIV/AIDS treated with highly active antiretroviral
pressive symptoms and mental health quality of life on therapy: a longitudinal study. Aust N Z J Psychiatry.
use of highly active antiretroviral therapy among HIV- 2000;34:1015–1021.
seropositive women. J Acquir Immune Defic Syndr.
2002;30:401–409. 25. Cook JA, Cohen MH, Grey DD, et al. Use of
highly active antiretroviral therapy in a cohort of HIV-
10. Gordillo V, del Amo J, Soriano V, Gonzalez-Lahoz J.
seropositive women. Am J Public Health. 2002;92:
Sociodemographic and psychological variables influenc-
ing adherence to antiretroviral therapy. AIDS. 1999;
82–87. Public Health
13:1763–1769. 26. Diagnostic and Statistical Manual of Mental Disor-
ders, Fourth Edition. Washington, DC: American Psychi-
Management of
11. Kleeberger CA, Phair JP, Strathdee SA, Detels R,
Kingsley L, Jacobson LP. Determinants of heterogenous
atric Association; 1994. Disasters:
adherence to HIV-antiretroviral therapies in the Multi- The Practice Guide
center AIDS Cohort Study. J Acquir Immune Defic
Syndr. 2001;26:82–92. By Linda Young Landesman, DrPH, MSW
12. Paterson DL, Swindells S, Mohr J, et al. Adher-
ence to protease inhibitor therapy and outcomes in pa-
tients with HIV infection [published erratum appears in T he tragic events of September 11, 2001,
raised the stakes for public health. This
book is a desk and field manual for public
Ann Intern Med. 2002;136:253]. Ann Intern Med.
2000;133:21–30. health and safety practitioners who need
13. Cohen MH, French AL, Benning L, et al. Causes to quickly access information about disas-
of death among women with human immunodeficiency ter preparedness, response and recovery.
virus infection in the era of combination antiretroviral Public Health Management of Disasters is
therapy. Am J Med. 2002;113:91–98. the first comprehensive text in this rela-
14. Ickovics JR, Hamburger ME, Vlahov D, et al. Mor- tively new practice area as public health
tality, CD4 cell count decline, and depressive symp- leaders begin integrating health depart-
toms among HIV-seropositive women: longitudinal ments into the national emergency re-
analysis from the HIV epidemiology research study. sponse infrastructure.
JAMA. 2001;285:1466–1474. An epilogue addresses the response to
15. Radloff LS. The CES-D Scale: a self-report depres- and resources about the events of Septem-
sion scale for research in the general population. Appl ber 11.
Psychol Meas. 1977;1:385–401.
ISBN 0-87553-025-7
16. Diagnostic and Statistical Manual of Mental Disor- 2001 ❚ 250 pages ❚ softcover
ders, Third Edition. Washington, DC: American Psychi- $28.95 APHA Members
atric Association; 1980. $37.95 Nonmembers
17. Breslau N. Depressive symptoms, major depres- plus shipping and handling
sion, and generalized anxiety: a comparison of self-
reports on CES-D and results from diagnostic inter- American Public Health Association
views. Psychiatry Res. 1985;15:219–229. Publication Sales
18. Zimmerman M, Coryell W. Screening for major Web: www.apha.org
depressive disorder in the community: a comparison of E-mail: APHA@TASCO1.com
Tel: (301) 893-1894
measures. Psychol Assess. 1994;6:71–74.
FAX: (301) 843-0159 MD02J1
19. Ickovics JR, Thayaparan B, Ethier K. Women and
AIDS: a contextual analysis. In: Baum A, Revenson T,
Singer J, eds. Handbook of Health Psychology. Hillsdale,
NJ: Erlbaum; 2000:821–839.
20. Carpenter CC, Cooper DA, Fischl MA, et al. Anti-
retroviral therapy in adults: updated recommendations
of the International AIDS Society–USA Panel. JAMA.
2000;283(3):381–390.
21. US Dept of Health and Human Services/Henry J.
Kaiser Family Foundation. Panel on Clinical Practices
for the Treatment of HIV Infection. Guidelines for the
Use of Antiretroviral Agents in HIV-Infected Adults
and Adolescents [monograph online] 2002 Feb. Avail-
able at: http://hivatis.org. Accessed March 6, 2002.
22. Wilson, TE, Barron Y, Cohen M, et al. Adherence
to antiretroviral therapy and its association with sexual
behavior in a national sample of women with human
1140 | Research and Practice | Peer Reviewed | Cook et al. American Journal of Public Health | July 2004, Vol 94, No. 7You can also read