DID GOLIATH OF GATH HAVE A MEDICAL CONDITION? - Dr. Yonit Marcus
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
DID GOLIATH OF GATH HAVE A
MEDICAL CONDITION?
Dr. Yonit Marcus
Case presentation
• A 58 year-old man
• Cab driver, married +2
• Family history= Mother-HTN
• Past medical history
• HTN
• 15 years
• Not controlled on multiple medications
• Verapamil SR 240 mg/day
• Doxazosin 2mg*2 /day
• Valsartan 80 mg /day
• OSA
• 5 years
• Sleeps with CPAP
• Bilateral carpal tunnel syndrome
per EMG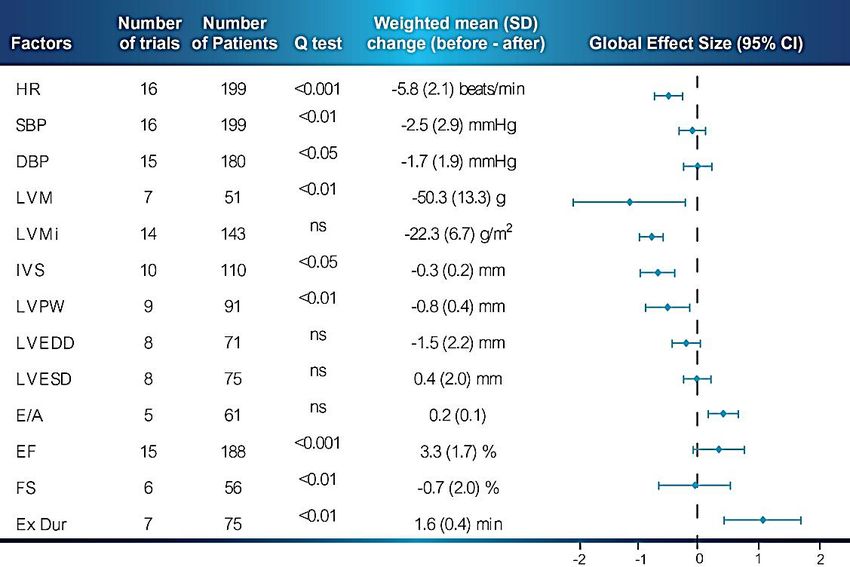
Case presentation
Multinodular goiter-
s/p Rt. hemithyroidectomy 2010-follicular
hyperplasia
Intubation at surgery was very hard
No Parathyroid tissue
Choanal atresia
2010 follow up at blood pressure clinic.
• Coarse and large hands
• Large nose
Suspected
• Nasal voice acromegaly
Current illness • No vision disturbance • No headache • Fatigue • PE: • Acral enlargement • Coarse and large nose • Multiple skin tags • Large tongue with teeth marks • ↑ BP • Lab • Blood sugar-N • Phosphor –H/N
2011 2001 1995

12/05/2011 IGF1 (7-47 nmol/L) 137 GH (0-5 ng/ml) 2.4 TSH (0.39-4 uIU/ml) 4.56 Free T4 (0.8-1.5 ng/dl) 1.1 Cortisol (mcg/dl) 10.3 Prolactin (1-18 ng/ml) 7 LH mIU/ml 2 FSH mIU/ml 6.5 Testosterone (1.81-7.72 ng/ml) 1.84 Normal response to 250 mcg ACTH stimulation test

75 gr OGTT Time (minutes) 60 90 120 GH (ng/ml) 7.25 7.34 8.29 Glucose mg/dl 131 142 150 In normal subjects GH level falls to less than 0.3ng/ml after OGTT

Pituitary MRI T1 with contrast •6*9 mm right pituitary mass •Possible extension to the left •Not in proximity with the optic chiasm
TOPICS
• Introduction
• Acromegalic CMP
• Prevalence of HTN
• Pathogenesis of HTN
• Reversibility with
treatment
Acromegaly : introduction • Prevalence: 40 to >100 cases per million • Diagnosis delayed: approx. 4-10 y • Approx. 40% diagnosed by internist • Others include: • Primary care practitioners, ophthalmologists, dentists, gynaecologists, rheumatologists and sleep disorder specialists • At time of diagnosis >75% macroadenoma
Acromegaly : introduction • Acromegaly is associated with a X2- to 3 increased morbidity and reduced life expectancy. • Excess mortality is mostly d/t CVS and cerebrovascular dis. and can be reduced when serum GH & IGF-I are ↓. • Determinants of mortality are cardiovascular complications, ↑GH concentrations, HTN, and heart dis.
Acromegalic comorbidities
Hypertension, cardiomyopathy, Cerebrovascular events, headache
valvular disease
Hypopituitarism, hypogonadism
Acromegaly
Respiratory comorbidities
complications,
sleep apnea
Osteoarthritis,
osteoporotic fractures
Glucose
intolerance/
diabetes mellitus Colon
polyps
Adaped from Colao, et al. Endocr Rev, 2004The acromegalic cardiomyopathy • Clear-cut LVH is found in most pts. at diagnosis, overall in those with long disease history, and interstitial fibrosis constitutes the main abnormality at histology • Subsequently, gradual impairment of heart architecture by increased extracellular collagen deposition, myofibrillar derangement, areas of monocyte necrosis, and lympho- mononuclear infiltration occurs, thus configuring a pattern of myocarditis.
The acromegalic cardiomyopathy • HTN is likely the most important factor aggravating cardiac hypertrophy and has higher prevalence in aged pt. • Studies of the coronary artery disease in acromegaly are very scant (reported between 3% and 37%).
Cardiomyopathy
• Hormonal control
improves LVH and cardiac
dysfunction
• SRL may cause
asymptomatic bradycardia
Acromegalic
Colao, et al. JCEM, 2004. Colao, et al. JCEM, 2008. De Marinis. Pituitary, 2008. Reproduced with kind permission from
Maison, et al.Acromegaly : prevalence of HTN • HTN is considered one of the most relevant negative prognostic factors for mortality in acromegaly. • The prevalence of HTN in acromegaly ranges from 18% - 60% in different series, and its incidence is higher than in the general population (ABPM? proper controls? m/p 40% vs. 8%). • Predominantly DBP, is less frequently related to a family history of HTN and is poorly related to IGF-1 levels • However, despite its importance, the physiopathological mechanisms of HTN have not yet been well clearly established.
Pathogenesis -1 • Increased plasma volume and an increase in the total exchangeable sodium pool. • Kamenicky et al , Endocrinology 2008 – found in GC rats, that GH, in concert with IGF-I, stimulates ENaC-mediated sodium transport in the late distal nephron, accounting for the pathogenesis of sodium retention in acromegaly.
Pathogenesis -2
• Reduced levels of Nitric oxide (NO) may contribute to
increased vascular resistance, increased platelet
aggregation, stimulation of VSMC proliferation.
• Platelet NO is reduced in acromegalic pts., compared
with controls.
• eNOS protein concentrations were significantly reduced in
the platelets of pt. compared with controls.
• The NO levels are inversely correlated with GH/IGF-1
and disease duration. This low expression and availability
of nitric oxide could be implicated in vascular alterations
and increased atherogenic risk affecting acromegalics.
Ronconi ;Blood Pressure. 2005Pathogenesis -3 • Aldosterone secretion and regulation are normal and so are ANP and the RAAS (Mulatero, et al JCEM 2006 – 344T/C CYP11B2 gene polymorphism is linked to the risk of HTN in pts. affected by acromegaly and so are Angiotensinogen MT and AT1R CC1166 genotype- in Turgut et al Mol Biol Rep- 2011). • There is no evidence for the activation of the adrenergic system ie plasma Epi/NE were normal both basally and after hyperinsulinemic clamp.
Pathogenesis -4 • Insulin resistance and diabetes is associated with higher BP and a non dipping effect on ABPM. • Increased cardiac output and cardiac index – SVR (both ↓ and ↑). • Endothelial dysfunction, according to Folkow’s hypothesis- the increased BP in GH excess could directly originate from an increased thickness of wall resistance vessels. Is there a direct negative effect of GH and IGF-I hypersecretion on endothelial function? • OSA
Obstructive sleep apnea • Repetitive nocturnal desaturations are associated with arterial and pulmonary HTN, AF and right heart failure in hypoxemic subjects. • OSA may affect 60–70% of acromegalics, M>F and more in HTN pts. • It is caused by pneumonomegaly, narrowing of the upper airways, hormonal rhinitis, nasal polyps and enlargement of the laryngeal cartilages, epiglottis, tongue (macroglossia) and pharyngeal structures. • There are contradictory results concerning OSA in pts, treated surgically and/or pharmacologically for acromegaly.
Obstructive Sleep apnea syndrome
OSA only partially reversible with
• Degree of OSA correlates
biochemical control of acromegaly
positively with the disease – a reduction in soft tissue swelling?
activity (IGF-I levels) but
+/- with the duration of the
disease
• The parameters of
the MetSy are positively
associated to the degree of
OSA in acromegalic pts.
Davi, et al. Eur J Endocrinol. 2008. & Rommler Sleep Breath (2012Treatment effects • Transsphenoidal adenomectomy has been reported to reduce the LVM and improve diastolic performance if dis. control is obtained . A prompt reduction in cardiac mass occurs in pts. treated with SSA • Beneficial effects of treatment with SSA were reported on HR as well (a direct effect on the conduction sys). • No significant difference in BP was demonstrated in more prolonged studies with octreotide, octreotide LAR or lanreotide or pegvisomant (Colao et al 2006).
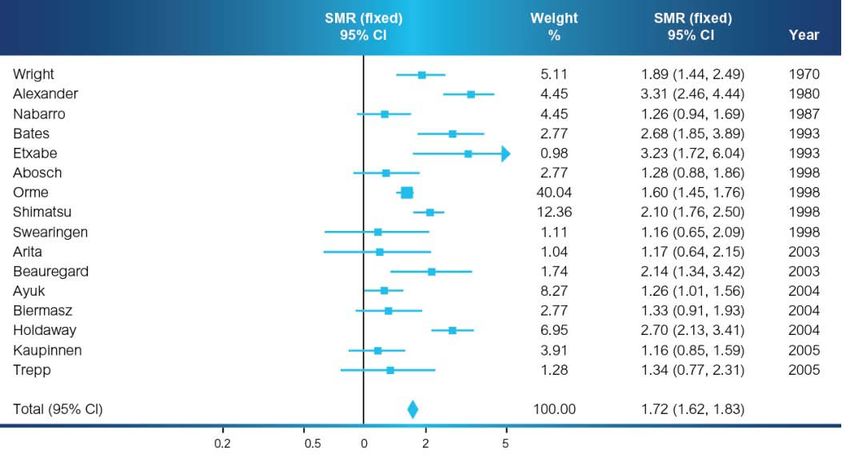
Mortality
• Increased mortality in
uncontrolled acromegaly
• Radiotherapy associated with
increased mortality compared
with other therapies
• More data needed on
stereotactic radiation therapy
• Over-replacement of
hydrocortisone can affect
mortality
• Co-existing adrenal
insufficiency may impact
mortality
Reproduced with kind permission from Dekkers, et al. JCEM, 2008. Copyright The Endocrine Society (2008)You can also read

















































