"Doctors Do Too Little Technology": A Longitudinal Field Study of an Electronic Healthcare System Implementation
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Information Systems Research
Vol. 22, No. 3, September 2011, pp. 523–546
issn 1047-7047 eissn 1526-5536 11 2203 0523 http://dx.doi.org/10.1287/isre.1110.0383
© 2011 INFORMS
“Doctors Do Too Little Technology”: A Longitudinal
Field Study of an Electronic Healthcare System
Implementation
Viswanath Venkatesh
Information Systems, Walton College of Business, University of Arkansas, Fayetteville, Arkansas 72701,
vvenkatesh@vvenkatesh.us
Xiaojun Zhang
Department of Information Systems, Business Statistics and Operations Management, School of Business and Management,
Hong Kong University of Science and Technology, Clear Water Bay, Kowloon, Hong Kong, xiaojunzhang@ust.hk
Tracy A. Sykes
Information Systems, Walton College of Business, University of Arkansas, Fayetteville, Arkansas 72701,
tracy@tracyannsykes.com
W ith the strong ongoing push toward investment in and deployment of electronic healthcare (e-healthcare)
systems, understanding the factors that drive the use of such systems and the consequences of using
such systems is of scientific and practical significance. Elaborate training in new e-healthcare systems is not a
luxury that is typically available to healthcare professionals—i.e., doctors, paraprofessionals (e.g., nurses) and
administrative personnel—because of the 24 × 7 nature and criticality of operations of healthcare organizations,
especially hospitals, thus making peer interactions and support a key driver of or barrier to such e-healthcare
system use. Against this backdrop, using social networks as a theoretical lens, this paper presents a nomological
network related to e-healthcare system use. A longitudinal study of an e-healthcare system implementation, with
data gathered from doctors, paraprofessionals, administrative personnel, patients, and usage logs lent support
to the hypotheses that: (1) ingroup and outgroup ties to doctors negatively affect use in all user groups; (2)
ingroup and outgroup ties to paraprofessionals and administrative personnel positively affect use in both those
groups, but have no effect on doctors’ use; and (3) use contributes positively to patient satisfaction mediated by
healthcare quality variables—i.e., technical quality, communication, interpersonal interactions, and time spent.
This work contributes to the theory and practice related to the success of e-healthcare system use in particular,
and information systems in general.
Key words: IT diffusion and adoption; healthcare and IT
History: Robert Fichman, Rajiv Kohli, and Ranjani Krishnan, Senior Editors. This paper was received on
February 16, 2009, and was with the authors 16 months for 3 revisions.
Introduction care industry—ranging from hospitals to suppliers
“We perform assessments on all new residents when to patients (PricewaterhouseCoopers 1999, 2005). The
they enter the facility. Although we will get their implementation of e-healthcare systems is expected
hospital orders at that time, currently, it takes 24 to reduce costs and errors and seamlessly integrate
to 48 hours to get the patient’s 6complete7 records. patient data, thus providing better health care at
This is a fragile, medically compromised patient pop- a lower cost (PricewaterhouseCoopers 1999, 2005).
ulation that would benefit most from electronically The U.S. government, for instance, aims to make
linked information networks,” said Patricia Kolling,
all medical records electronic and standardized by
chief compliance officer at BEI, one of the largest nurs-
2014, thus creating enormous pressure to implement
ing home chains in the U.S.
e-healthcare systems rapidly. In the United States, $77
The cost of health care is about a fifth of the billion could be saved annually by properly imple-
U.S. GDP and close to that for OECD countries menting and adopting e-healthcare systems (Hillestad
(PricewaterhouseCoopers 2005) and is on the rise. et al. 2005). A key barrier to success of such sys-
Electronic healthcare (e-healthcare) systems have tems is the availability of adequate training and
been touted as a key solution to several prob- support (PricewaterhouseCoopers 1999). Typically, e-
lems that plague the healthcare industry, with enor- healthcare systems are inflicted on healthcare profes-
mous benefits expected for all parties in the health- sionals with little or no training or process change
523Venkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation 524 Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS support, thus resulting in adoption taking much We use social network theory as the lens to fur- longer than expected and benefits not being realized ther our understanding of e-healthcare system use for a long time (PricewaterhouseCoopers 1999, 2005). and its impacts. Social network theory is particu- In light of this, it is estimated that only between a larly appropriate for reasons largely related to its fourth or a third of all doctors use technology solu- focus on interpersonal interactions and their rela- tions available to them, and less than 5% use all tionships to behaviors and outcomes (Borgatti and the powerful features available in these solutions. Foster 2003, Brass and Labianca 1999, Labianca and Most physicians often rely on paper records that Brass 2006). First, given the critical and 24 × 7 nature are frequently incorrect or outdated (e.g., O’Brien of operations in healthcare organizations, especially 2008). Even in healthcare organizations that have suc- hospitals, there is little or no time for traditional cessfully deployed healthcare systems, it is often the training (PricewaterhouseCoopers 1999, 2005), thus case that caregivers and administrative personnel fre- making interactions with peers and colleagues and quently do not use the system as intended—i.e., at the learning on the job important in these organizations. time of interaction with the patient—instead, data are Second, in most cases, the knowledge necessary to entered into the system at a later time. This greatly complete work activities is specialized and spread undermines the benefits of the system at the point across many individuals. Third, healthcare profession- of care and major touchpoints with patients. In sum, als rely on each other to learn not only about medical there is an underutilization and/or abandonment of practices, but also about technology (Davidson and e-healthcare systems. Thus, understanding the factors Chiasson 2005). Finally, because communication is at influencing success of e-healthcare systems is of great the heart of health care, there is a need for research practical significance. to examine how interactions among various groups IS researchers have long studied technology in of healthcare professionals and the consequences of health care, with much of the emphasis being at the such interactions (see Kaplan et al. 2007) influence macrolevel, ranging from policy issues and challenges outcomes of interest. (e.g., Currie and Guah 2007) to challenges in small Among the different types of networks, e.g., advice, physician practices (e.g., Reardon and Davidson 2007) friendship, and information (Borgatti 2005), we focus to firm-level outcomes, such as profitability (e.g., on advice networks, particularly advice seeking, Devaraj and Kohli 2000) and compliance to standards because during the implementation of a new e- (e.g., Davidson and Chiasson 2005), to quality of care healthcare system, healthcare professionals are more at the level of the hospital (e.g., Devaraj and Kohli likely to seek knowledge related to the system in 2000) and the group (e.g., Kane and Alavi 2008). Some order to use it for work activities. The advice pro- research at the individual level has found that doctors vided by healthcare professionals is bound by their have typically not embraced e-healthcare systems and educational backgrounds and professional cultures. preferred to use paper records (e.g., Anderson 1997, Such acculturation is likely to contribute to the devel- O’Brien 2008). This is important because firm-level opment of healthcare professionals’ cognitive schema, benefits are ultimately garnered when individuals in which would play a significant role in affecting indi- critical roles in healthcare organizations embrace and viduals’ decision-making (see Labianca et al. 2000). use implemented systems and, if such individual use Likewise, healthcare professionals who receive advice occurs, contributes to positive outcomes. More recent will interpret and apply such advice based on their work has focused on the design of healthcare sys- educational backgrounds and professional cultures. tems (e.g., Johnson et al. 2008) and their impacts Thus, we incorporate advice seeking and accultura- on various aspects of quality of care (e.g., Matheny tion into our theorizing in order to better understand et al. 2007). There has also been work on user accep- e-healthcare system use and its impacts. tance and usability (e.g., Klein 2007), a topic that In the quest for the ultimate dependent variable has been researched extensively in the broader IS of interest, we turned to the broad literature on IS context as well (see Venkatesh et al. 2007). Despite success and work on e-healthcare systems. The IS suc- the great interest in e-healthcare system implementa- cess model of DeLone and McLean (2003) has identi- tions, a recent review suggests that the work in this fied examples of critical metrics of success. System use area is largely atheoretical and based on retrospec- is one such metric, and has been the focus of much tive accounts and data from the same source for all work at the individual level studying technology aspects of the model, thus rendering prior work to be implementations (see Venkatesh et al. 2003). Beyond somewhat limited in terms of richness and scientific system use, the IS success model calls for a study of rigor (see Overtveit et al. 2007). Against the backdrop net benefits and/or broader personal and organiza- of these gaps, there is a need for more theory-driven tional outcomes of interest. In the context of health investigations of the underlying phenomenon of use care, one such metric is patient satisfaction—in fact, and impacts of e-healthcare systems. recent work has suggested that patient satisfaction
Venkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation
Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS 525
is key because it is not only an important metric to an individual has access to the information they
healthcare providers in its own right but also is key need to resolve work-related problems (see Burkhardt
to insurance companies as a consequence of quality and Brass 1990). Network centrality can drive the
of care (Kohli and Piontek 2007). Therefore, research performance of the “appropriate” behaviors guided
explaining patient satisfaction is particularly impor- by access to resources, such as advice, information
tant in the domain of health care and technology. and knowledge, and the performance of behaviors
Given the important role of system use in driving can have positive performance impacts (Borgatti and
implementation outcomes, the objectives of this work Foster 2003, Lin 2001; for examples, see Bolino et al.
are to: 2002). Network centrality also yields benefits sim-
(i) develop a nomological network around e-health- ply by virtue of position and topology of the net-
care system use by doctors, paraprofessionals, and work without a focal individual necessarily having
administrative personnel—specifically, we develop a to perform any behaviors (see Borgatti and Foster
model that draws from social network theory and 2003 for a discussion). Prior research indicates that
identify predictors of e-healthcare system use, and link employee network centrality plays an important role
such system use to patient satisfaction; and in influencing access to important resources, such as
(ii) empirically validate the model in a longitudinal advice, information, and knowledge, and applying
field study conducted in a hospital, with data gath- such resources in completing one’s job may greatly
ered from healthcare professionals and patients. improve one’s job performance (Brass 1984, Sparrowe
et al. 2001). Taken together, the core idea is that
This work is expected to contribute to research in
centrality contributes positively to performance both
several ways. First, it enriches our understanding of
directly and by leading to the performance of a key
e-healthcare system success by linking the network
behavior or set of behaviors that in turn drive perfor-
position to patient satisfaction mediated by use and
mance outcomes.
the proximal impacts of use, thus adding not only to
When seeking advice, they will be exposed to var-
individual-level work on e-healthcare system success
ious ideas, concepts, knowledge, and views of other
(e.g., Klein 2007) but also complementing macrolevel people that may in turn shape their own views
work on this topic (e.g., Devaraj and Kohli 2000). Sec- toward, and knowledge of, the new system, making
ond, this work complements research on e-healthcare them react to the system in different ways. Thus, the
system success by leveraging acculturation of differ- extent to which they are connected to others in an
ent groups of healthcare professionals and linking advice network will play an important role in driving
advice networks to key outcomes in the context of system-related behaviors, such as system use. Practi-
e-healthcare systems. Finally, this work adds to the tioner literature suggests that the use of e-healthcare
body of knowledge related to IS success (DeLone systems should result in performance benefits. Draw-
and McLean 2003, Rai et al. 2002). Specifically, this ing from social networks research, we would expect
work responds to continuing calls in prior research to network position of users to result in direct perfor-
extend the nomological network related to IS imple- mance benefits.
mentation beyond the technocentric outcomes that
are typically studied in IS research (see Venkatesh Model Development
et al. 2007). The baseline model builds on prior social networks
research that network position will foster behavior—
Background: Social Networks here, e-healthcare system use—and performance—
Prior social networks research suggests that network here, quality of care and patient satisfaction. Our
position influences behavior and performance out- proposed model expands on the baseline model by
theorizing that ingroup ties and outgroup ties will
comes (e.g., Borgatti and Foster 2003, Lin 2001). Lin
have positive or negative effects, depending on pro-
(2001), citing four reasons grounded in social capi-
fessional group—i.e., doctors versus paraprofession-
tal, namely information, influence, social credentials,
als versus administrative personnel. With regard to
and reinforcement, suggest that individuals who are
consequences of e-healthcare system use, we will
more embedded in social networks are more likely to
make the case that e-healthcare system use will
perform particular target behaviors. An individual’s
positively influence various quality of care metrics
network position is typically conceptualized as net- that will in turn positively influence overall patient
work centrality, which describes how well connected satisfaction.
an individual is within the network (Borgatti 2005).
We adopt an egocentric conceptualization of advice Construct Definitions
network centrality, referring to an individual’s inter- In the healthcare context, the distinctions across dif-
action with others in an organizational unit to get ferent professional groups are critical in the understand-
advice. The greater the centrality, the more likely ing of the impacts of centrality on e-healthcare systemVenkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation 526 Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS use. We organize the professionals into three cate- questionnaire III (e.g., Hays et al. 1987; Ware et al. gories: doctors, paraprofessionals (e.g., nurses, doc- 1976a, b, Ware et al. 1983), which is widely deployed tor’s assistants) and administrative personnel. The in practice, is based on extensive field work. They first category—i.e., doctors—comprises those who employed a grounded theory approach to identify the have MD degrees and are the primary healthcare core elements of quality of health care that drive over- providers making decisions regarding patient care. all patient satisfaction. They identify six determinants Such a categorization based on possessing a med- of patient satisfaction: technical quality, communica- ical degree is consistent with much prior work on tion, interpersonal interactions, time spent, financial this topic (e.g., Kane and Alavi 2008, Pratt et al. aspects, and access/availability/convenience, whose 2006). The second category—i.e., paraprofessionals— definitions are adapted from Ware et al. (1976a, b, primarily consists of nurses, doctors’ assistants, and 1983) and Hays et al. (1987). Technical quality is the technicians, and are those who are in direct or indi- patient’s assessment of each healthcare professional’s rect care-giving support roles to doctors and hold a competence in handling specific aspects of care and professional certificate/license endorsing their abil- administrative handling; communication is defined ity to play a support role in caregiving. The third as the extent to which the patient perceives that he category—i.e., administrative personnel—comprises or she has received sufficient information about the those not involved in caregiving but who provide care in the hospital, care after they leave the hos- support activities related to care, such as billing, pital, and administrative matters from each health- credit, and insurance. care professional; interpersonal interactions is defined We argue that individuals’ centralities in different as a patient’s perceptions of empathy and friend- professional groups and the extent to which those liness of each healthcare professional; time spent individuals’ networks cut across the different profes- is defined as the extent to which the patient per- sional groups are related to e-healthcare system use ceives that each healthcare professional has spent suf- and performance. Building on the definition of cen- ficient time with the patient; financial aspects are trality, an ingroup tie is a connection to an individ- defined as the patient’s assessment of the hospi- ual who is in the same professional group, and an tal’s handling of various money-related matters; and outgroup tie is a connection to an individual who access/availability/convenience is the patient percep- is in a different professional group. Consequently, tions about various logistical aspects related to the ingroup centrality is how well connected an individual hospital, its location, and organization. As we dis- is in his or her own professional group, and outgroup cuss later, we use the first four metrics as being direct centrality is how well connected an individual is in consequences of e-healthcare system use and use the each of the other professional groups. For instance, other two as control variables in predicting patient a doctor’s connectedness to other doctors represents satisfaction. ingroup centrality, and a doctor’s connectedness to paraprofessionals represents outgroup centrality (to Baseline Model paraprofessionals). Based on the earlier discussion about social networks, The study of system use has a rich history in we present a baseline model. An employee who is IS research at the individual level (see DeLone and more central in a network is likely to have access McLean 2003, Venkatesh et al. 2003). E-healthcare sys- to more resources (e.g., Ahuja et al. 2003, Cross and tem use is defined as the interaction a user has with Cummings 2004), such as information about a new the newly installed technological system. We concep- system. Such ties will help users deal with ques- tualize use as duration, frequency, and/or intensity of tions and challenges related to using the new sys- use (e.g., Venkatesh et al. 2008). tem (e.g., Jensen and Aanestad 2007). To resolve such Patient satisfaction is defined as the extent to which a problems, they are likely to seek advice from their patient, or the patient’s authorized decision maker, is coworkers. Also, connections to different groups of pleased with the overall medical care received (Hays users, i.e., doctors, paraprofessionals, and adminis- et al. 1987, Zeithaml et al. 1990). While patient sat- trative personnel, may expose central individuals to isfaction is an important ultimate dependent vari- a variety of views and knowledge related to the able, research in health care has noted that quality is new system. By reflecting the connectedness of an a key determinant of satisfaction (Hays et al. 1987; individual, in this context, network centrality is the Ware et al. 1976a, b, 1983; Ware and Snyder 1975). extent to which an individual can obtain information Research on quality of care has varied greatly and has about system features, procedural details, and activ- primarily been driven by a variety of instruments that ities in the new process; knowledge, such as tips and are available in practice (see American Physical Ther- tricks, shortcuts, and details related to the integra- apy Association 1995 for a collection of instruments tion of the process and software; and other tangi- used in a variety of hospitals). The patient satisfaction ble resources, such as training resources, manuals, and
Venkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation
Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS 527
tutorials, that can greatly help with using the system records, and requires doctors to fundamentally alter
(Sykes et al. 2009). Beyond the instrumental support the way they organize their thought processes about
described above, those who provide advice often pro- patient care (Anderson 1997). Moreover, the intro-
vide social support. Advisors are frequently listeners duction of any new technology, e.g., an e-healthcare
who can empathize and/or sympathize with a focal system, can change the original power structure that
individual. Such empathy and sympathy can drive traditionally favors central doctors through the redis-
behavior—here, e-healthcare system use (Loewenstein tribution of information that confers power on their
and Small 2007). possessors (see Burkhardt and Brass 1990, Doolin
Beyond the well-established general behavior to 2004), the disruption of occupational roles (Black et al.
performance relationship, prior work, mostly based 2004), and power transfer in the forms of hospital
on anecdotal evidence, has suggested that e-health- management possibly being able to usurp doctors’
care system use can contribute positively to over- power and integrate the power into administrative
all patient satisfaction (see Kohli and Piontek 2007). personnel (Doolin 2004). For fear of losing their
Several mechanisms are cited in the trade press for autonomy and power, central doctors in an advice
such an effect—e.g., e-healthcare systems reduce costs network can be expected to develop negative views
and errors (e.g., Anderson 1997, Jensen and Aanestad towards a new e-healthcare system.
2007). As noted earlier, despite limited systematic
empirical evidence, patient satisfaction is emerging Supporting Roles of Paraprofessionals and Ad-
as a critical metric that reflects quality and value ministrative Personnel. The main task of para-
of care (Kohli and Piontek 2007). Beyond the use- professionals is to assist doctors. The training of
performance relationship, network centrality itself can paraprofessionals thus centers around supporting
yield direct performance benefits given that central doctors and delivering secondary care. Considering
individuals are more likely to gain access to resources, the supporting role they play, they typically under-
such as advice and social support unrelated to the sys- stand their relative power and autonomy. In contrast
tem, that contribute positively to their performance to doctors, paraprofessionals will have more positive
(Sparrowe et al. 2001). Thus, in keeping with prior views towards the implementation of a new system
social network theory, our baseline model suggests and are more likely to use it. For example, stud-
that the relationship between network position and ies indicate that the strength of a new e-healthcare
performance will be partially mediated by behavior. system is in its ability to help create and store
well-documented nursing notes (Jensen and Aanestad
Doctor, Paraprofessionals, and Administrative 2007) that create a better overview of each patient
Personnel: Roles and Acculturation and ease the work processes for paraprofessionals
Acculturation of Doctors. Doctors, paraprofession- such that they could spend more time on patient
als, and administrative personnel) have different edu- care instead of on administrative tasks (e.g., Jensen
cational backgrounds and professional cultures that and Aanestad 2007). Whereas doctors are generally
play a key role in shaping their predispositions unwilling to change their traditional practice and use
toward technologies in the workplace. Doctors have a new e-healthcare system, paraprofessionals tend to
a strong sense of professional identity that revolves more readily accept and use a new e-healthcare sys-
around their education and medical practices. This tem (Anderson 1997). Another reason paraprofession-
identity is formed early in their career (Freidson als develop more favorable views toward a new sys-
1988, Pratt et al. 2006). Doctors also tend to have a tem than doctors do is that whereas doctors do not
high level of professional commitment tied to treating consider the implementation of a new system as a
patients and clinical practices even as they progress way to improve patient treatment, paraprofessionals
through their career and evolve into other roles, such are likely to perceive such a system as an effective
as a physician executive (e.g., Hoff 2001). The doctor- tool for facilitating coordination with other healthcare
patient relationship is one of the most special and groups, another important role of paraprofessionals in
hinges on a strong sense of mutual trust and loyalty addition to their bedside responsibilities (Jensen and
(Vaughan and Higgs 1995) and practices related to Aanestad 2007). Finally, whereas the introduction of
interacting with patients are ingrained into doctors’ a new e-healthcare system may jeopardize the unique
professional identity from the earliest days of their power of doctors (Bhattacherjee and Hikmet 2007,
training (Pratt et al. 2006). Furthermore, doctors view Doolin 2004, Frideson 1985, Malvey 1981), paraprofes-
autonomy and power as a cornerstone of their pro- sionals will be less affected because they do not pos-
fession (e.g., Blumenthal 1994). The implementation sess such unique power before the implementation of
of e-healthcare systems has been seen as something a new e-healthcare system and, therefore, they do not
that changes traditional medical practice, lowers the have as much to lose. Instead, the implementation of
autonomy that doctors have in constructing patient a new system might empower paraprofessionals dueVenkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation
528 Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS
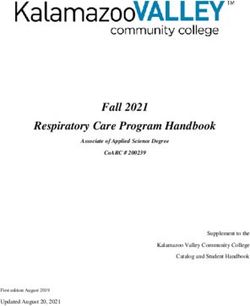
Figure 1 Research Model
H5
Quality of care
Network
position Technical
quality
Centrality among
doctors
Communication
H1–H3* Electronic H4 H6
Centrality among healthcare Patient
paraprofessionals system use satisfaction
Interpersonal
interactions
Centrality among
admin personnel
Time spent
∗
Moderated by group membership.
to other groups’ increased reliance on paraprofession- the hierarchy, are likely to obey policies and deci-
als (Pisano et al. 2001). sions made by top management, and thus are likely
The last group of e-healthcare systems’ users is to actively use, and influence others to use, the new
administrative personnel. This group not only sup- system.
ports doctors so that they can deliver better-quality
health care, but also coordinates external and internal Proposed Model
activities to optimize hospital management. For exam- Figure 1 shows the proposed model. The model
ple, if doctors require specific medical equipment, relates network position in different professional
they need to coordinate with the doctors and the groups to quality of care via e-healthcare system
suppliers of the equipment. They need to coordinate use. Quality of care in turn predicts patient satisfac-
and manage doctors’ and paraprofessionals’ sched- tion. The model further presents that the relationship
ules to optimize healthcare operation. In order to do between network position and system use will be
so, they must monitor and/or administer the work moderated by group membership, with the interac-
of doctors and paraprofessionals. They generally have tions proposed being shown in Table 1.
a favorable view toward adoption and use of a new Impact of Ties to Doctors on E-Healthcare Sys-
e-healthcare system because such systems can help tem Use. Contrary to much prior social networks
them monitor and administer the work of doctors and research, in the context of doctors, we argue that both
paraprofessionals (Doolin 2004). Furthermore, much ingroup ties within doctors and outgroup ties to doc-
monitoring and administration helps administrative tors will have a negative effect on e-healthcare system
personnel better control doctors and make them more use. We have discussed the benefits associated with
responsible for their own actions (Doolin 2004). Prior centrality as being able to access different resources.
research has suggested that computerized physician In this context, central doctors are those who inter-
order entry (CPOE) systems could support clinical act a great deal with doctors for advice, information,
management practices in coping with institutionally and knowledge related to performing their work. As
triggered change in the organizational environment noted earlier, doctors are likely to develop negative
(Davidson and Chismar 2007). To respond to insti- views towards the new system because it could pose
tutional changes in markets or regulatory pressures a threat to their autonomy and power (Bhattacherjee
in the organizational environment, such as the pres- and Hikmet 2007, Jensen and Aanestad 2007), which
sure exerted by regulatory agencies, insurers, and have been viewed as the cornerstone of their profes-
large firms (Bodenheimer 1999), administrative per- sion (e.g., Blumenthal 1994). Such negative views are
sonnel, especially those at the top of the hierarchy, likely to prevent central doctors from actively seeking
would be more likely to adopt and use new systems knowledge to resolve system-related problems, result-
(Greenwood and Hinings 1996, Scott 2001). Other ing in less or ineffective use of the system. Even when
administrative personnel, i.e., those not at the top of central doctors seek advice from other doctors aboutVenkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation
Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS 529
Table 1 Effects of Ties on System Use
Ties to:
Ties from: Doctors Paraprofessionals Admin personnel
Doctors H1A: Negative effect on use H2A: No effect on use H3A: No effect on use
Paraprofessionals H1B: Negative effect on use H2B: Positive effect on use H3B: Positive effect on use
Admin personnel H1C: Negative effect on use H2C: Positive effect on use H3C: Positive effect on use
the new system, they are likely to get negative com- dependence on doctors for their workflow and activ-
ments about the system, thus reinforcing their original ities. In contrast, paraprofessionals and administra-
negative views towards the system. We thus expect tive personnel with fewer outgroup ties to doctors are
doctors who are better connected to other doctors to likely to explore and use the new system. Thus, we
resist using the system and to continue to engage in hypothesize as follows.
traditional practices. Although social capital gener- Hypothesis 1B (H1B). Outgroup ties to doctors will
ally tends to foster new behavior through information negatively influence system use among paraprofessionals.
and resource access, there is evidence that it can cre-
ate maladaptive situations, foster undesirable behav- Hypothesis 1C (H1C). Outgroup ties to doctors will
iors, and inhibit behaviors (see Gargiulo and Benassi negatively influence system use among administrative
1999, Portes and Landolt 1996, Portes 1998). We expect personnel.
that to be the case here, where there is a desire for Impact of Ties to Paraprofessionals and Adminis-
and commitment to the status quo, such that more trative Personnel on E-Healthcare System Use. Doc-
ingroup ties within doctors will negatively influence tors’ ties to outgroup members—i.e., paraprofession-
e-healthcare system use. In contrast, noncentral doc- als and administrative personnel—are not expected
tors, i.e., doctors who are on the periphery of the net- to have an effect on their own system use. This is
work, will be less influenced by other doctors because an important null effect to recognize. Doctors, as pre-
of their limited interactions with other doctors. They viously discussed, due to their commitment to tra-
are thus less likely to be submerged in a sea of nega- ditional medical practices and professional identity,
tive views towards the new system. Consequently, at are not likely to be open to input and influence from
least to some extent, they are more likely to explore other groups, particularly those groups over whom
and use the new system. Also, noncentral doctors they preside in the clinical hierarchy and view as sup-
could see the new system as a way to acquire power porting to their role. The acculturation of doctors pre-
and status within the network, a benefit that using the vents them from seeking and acting upon advice from
new system potentially confers (Burkhardt and Brass paraprofessionals and administrative personnel. Even
1990). Thus, we hypothesize as follows. though doctors can be well connected to paraprofes-
sionals who could be the sources of knowledge about
Hypothesis 1A (H1A). Ingroup ties will negatively the new system, they are less likely to seek knowl-
influence doctors’ e-healthcare system use. edge from paraprofessionals because seeking knowl-
edge reveals their ignorance (see Borgatti and Cross
The negative effects observed in the case of ingroup 2003, Lee 1997). Admitting their ignorance to peo-
ties to doctors are also expected to apply in the case ple of lower status could tarnish their reputation or
of outgroup ties that paraprofessionals and adminis- image, which could pose a threat to doctors’ authority,
trative personnel have to doctors. When being asked which they are strongly motivated to protect (Ferris
by paraprofessionals or administrative personnel for et al. 1994, Lee 1997). Furthermore, studies have indi-
advice related to how to better use the system, doc- cated that doctors have to rely more on information
tors are less likely to provide useful advice due to provided by paraprofessionals after the implementa-
their limited use and knowledge about the system. tion of a new e-healthcare system (Pisano et al. 2001).
They could even persuade those paraprofessionals To minimize seeking knowledge from people of lower
and administrative personnel not to use the system. status, they are likely to act against a change that
Those with many outgroup ties to doctors are more could subvert such authority (e.g., Black et al. 2004).
likely to be influenced by doctors and develop similar Doctors value their autonomy and are not likely
negative views towards the new system via negative to depend on administrative personnel for system-
comments about the system and how it interrupts tra- related advice. The reason is that doctors are likely
ditional medical practices. Doctors are at the top of to perceive the implementation of a new system as
the clinical hierarchy (Kaplan et al. 2007, Melia 1987), empowering to administrative personnel while reduc-
and those lower down the hierarchy have greater ing their own autonomy (Jensen and Aanestad 2007).Venkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation
530 Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS
As noted earlier, e-healthcare systems can be used get help to resolve problems in using the new system,
to help monitor and scrutinize doctors’ activities in such individuals are more likely to use it.
hospitals (Doolin 2004). By implementing a new sys- In both cases, because of the complexity and inter-
tem, hospital management can reduce doctors’ power dependence that is created by a new e-healthcare sys-
and integrate power into the organizational decision- tem, there will be benefits to being well connected
making process. Thus, a new system poses a direct to both groups. Paraprofessionals who are better con-
threat to both doctors’ autonomous roles, such as nected within the group are more likely to be able to
being the only entity that can determine modes of resolve problems, get assistance on features applica-
treatment (Bhattacherjee and Hikmet 2007, Frideson ble to them, and learn how to adapt their old work
1985), and strong economic bargaining position in practices to the new system context. Furthermore,
the hospital, such as having direct access to the paraprofessionals who are better connected to admin-
policy-making governing board without having to istrative personnel will be able to work on aspects of
go through the chief executive officer in the hospital the system that will be at the nexus of patient care and
(Malvey 1981). Doctors are more likely to form nega- administration. By having stronger ties to administra-
tive perceptions of a system when they perceive it as tive personnel, paraprofessionals are likely to better
a control mechanism and a threat to their autonomy understand their own new workflows as well as the
(Bhattacherjee and Hikmet 2007, Jensen and Aanestad jobs of administrative personnel and how the system
2007). Consequently, doctors are less likely to seek fits into their (administrative personnel) workflow.
advice from administrative personnel who assume Taken together, both ingroup ties to other paraprofes-
the role of deploying the control mechanism, i.e., the sionals and outgroup ties to administrative person-
new system. Prior research suggests that such politi- nel will contribute positively to system use among
cal barriers between doctors and administrators must paraprofessionals. Likewise, from the perspective of
be resolved in order for effective knowledge exchange administrative personnel, ties within the group and
between these two groups of users that could lead outside the group to paraprofessionals will be pos-
to the strategic application and use of the new sys- itively related to system use because they will help
tem (Kim and Michelman 1990). We thus suggest that administrators to more easily solve problems related
there will be little or no effect of outgroup ties on to the system. Thus, we hypothesize as follows.
doctors’ e-healthcare system use.
In contrast to our discussion thus far, we expect Hypothesis 2A (H2A). Outgroup ties to paraprofes-
both ingroup and outgroup ties will have a favorable sionals will not influence e-healthcare system use among
effect in the context of paraprofessionals and admin- doctors.
istrative personnel. As noted earlier, the acculturation Hypothesis 2B (H2B). Ingroup ties will positively
of paraprofessionals and administrative personnel influence e-healthcare system use among paraprofessionals.
makes them more likely to view the new system
favorably because the new system is likely to bene- Hypothesis 2C (H2C). Outgroup ties to paraprofes-
fit them. Paraprofessionals or administrative person- sionals will positively influence e-healthcare system use
nel who have high ingroup centrality are those who among administrative personnel.
are well connected to paraprofessionals or administra- Hypothesis 3A (H3A). Outgroup ties to administra-
tive personnel, respectively, and hence are more likely tive personnel will not influence e-healthcare system use
to be affected by others’ positive views toward the among doctors.
system, which will be further reinforced when seek-
ing knowledge from others within these groups. In Hypothesis 3B (H3B). Outgroup ties to administra-
addition, such individuals enjoy a broad array of ben- tive personnel will positively influence e-healthcare system
efits and opportunities unavailable to those on the use among paraprofessionals.
periphery of the network (Sykes et al. 2009), such as Hypothesis 3C (H3C). Ingroup ties will positively
a better access to knowledge. This could be critical
influence e-healthcare system use among administrative
in an e-healthcare system implementation where the
personnel.
formal training sessions are not effective in provid-
ing the knowledge necessary, but rather much of the Impacts of System Use on Quality of Care.
learning occurs in the community of practice, such as There have been extensive discussions in the trade
the advice network (Jensen and Aanestad 2007). Being press about the various positive impacts that e-
central within the ingroup advice network of para- healthcare systems can provide (e.g., Anderson 1997,
professionals or administrative personnel will result PricewaterhouseCoopers 2005). Much of this has cen-
in more assistance from peers and the super-users tered around improved quality of care, with a particu-
(Jensen and Aanestad 2007). Given that ingroup para- lar emphasis on reducing errors (e.g., Anderson 1997).
professionals or administrative personnel are likely to Based on the documented empirical evidence and theVenkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation
Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS 531
reason that using e-healthcare systems will allow doc- Impacts of Network Centrality on Quality of Care.
tors and paraprofessionals to provide better care, we The effect of network centrality on quality of care
expect a positive relationship between use and quality will be partially mediated by system use. Prior work
of care. The primary reasons why e-healthcare sys- argues that an employee’s network centrality plays
tems will be helpful in improving technical quality is an important role in affecting access to key resources,
that there will be better and more complete access to i.e., information, knowledge, or work-related advice,
patient information. This will allow doctors and para- which in turn serves as a key mechanism contributing
professionals to provide the most relevant care (e.g., positively to job performance (Brass 1984, Sparrowe
tests and advice) rather than engaging in exploratory et al. 2001). In this context, central individuals can be
testing and creating redundancy in tests. In terms of doctors, paraprofessionals, or administrative person-
administration, the availability of accurate and com- nel who have a large number of ties to other doctors,
plete information with the e-healthcare system will paraprofessionals, or administrative personnel in an
allow for greater accuracy in billing and other admin- advice network. The more ties they have, the more
istrative formalities. Thus, we hypothesize as follows. sources from which they could seek knowledge or
Hypothesis 4A (H4A). Electronic healthcare system advice to improve quality of care. For example, cen-
use will positively influence technical quality. tral doctors in a doctors’ advice network are likely
to obtain more advice or knowledge from other doc-
Communication, interpersonal interactions, and
time spent with patients will all be favorably affected tors about how to deal with a difficult medical case,
as a result of e-healthcare system use. For doctors and including treatment plans, similar cases, and ongo-
paraprofessionals, the availability of more accurate ing medical trials. When they get advice from other
and complete patient case information will mean that doctors, they can compare cases handled by others
they will be able to provide the relevant information with their own and synthesize and evaluate differ-
about their thought process and treatment plans to ent sources of advice to make a better decision. Like-
patients. It will require them to spend less time study- wise, central paraprofessionals can get advice from
ing this information after talking with the patient in doctors or paraprofessionals such that they would
order to arrive at treatment plans. With more accurate have knowledge about how to deliver better service
and complete information available prior to and at the to patients. Finally, administrative personnel can get
point of care, care givers will be less subject to piece- advice from doctors and paraprofessionals to remove
meal information that can typically result in altering ineffective procedures, resulting in better care. Con-
the course of treatment plans. Given the availability sequently, such central individuals are likely to per-
of better information about a patient at the point of form better than less-central individuals. Thus, we
care and more efficient assessment of each case, doc- hypothesize as follows.
tors and paraprofessionals can spend more time and Hypothesis 5 (H5). Network centrality will positively
be friendlier in their interactions with patients as the
influence quality-of-care metrics—i.e., technical quality,
time pressures (per patient) can be expected to reduce
communication, interpersonal interactions, and time spent.
somewhat. Recall that communication relates to infor-
mation provided to the patient and interpersonal Impact of Quality of Care on Patient Satisfaction.
aspects relate to concern and friendliness toward the There is evidence that quality and the proximal deter-
patient. We note that the effectiveness benefits of the minants of satisfaction hinge upon context. Specific
e-healthcare system will essentially allow for both attributes of quality related to the service context have
types of benefits to be garnered. Likewise, for admin- been related to customer satisfaction in a variety of
istrative personnel, the accurate and timely informa- industries (see Ostrom and Iacobucci 1995, Zeithaml
tion available from an e-healthcare system will free et al. 1990). In the healthcare context, building on
up time they would otherwise have to use to collate prior research on quality of care and patient satisfac-
all records and discern various billing and follow-up tion, four key metrics of quality of care—i.e., tech-
matters. This will make available more time to bet- nical quality, communication, interpersonal aspects,
ter interact with patients and/or authorized decision and time spent—that are expected to be influenced by
makers. Thus, we hypothesize as follows. e-healthcare system use will in turn positively influ-
Hypothesis 4B (H4B). Electronic healthcare system ence patient satisfaction. The general rationale, albeit
use will positively influence communication with patients. at the level of the hospital, for the effects of each of
these metrics on overall patient satisfaction has been
Hypothesis 4C (H4C). Electronic healthcare system
developed in prior work (e.g., American Physical
use will positively influence interpersonal interactions with
Therapy Association 1995; Hays et al. 1987; Marquis
patients.
et al. 1983; Ware et al. 1976a, b, 1983). The rationale
Hypothesis 4D (H4D). Electronic healthcare system at the level of each patient and at the level of each
use will positively influence time spent with patients. individual caregiver or administrative staff memberVenkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation
532 Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS
is that receiving the right treatment at an affordable who received care at the hospital (and/or closest
price will be important in driving satisfaction. This relative or friend authorized to make decisions on
is akin to the effects of accuracy of product or ser- behalf of the patients—hereinafter, “authorized deci-
vice delivery on customer satisfaction (see Zeithaml sion maker”). Overall, of the 1,348 possible respon-
et al. 1990). The healthcare context, even more so than dents (244 doctors, 894 paraprofessionals, and 210
many other service situations, requires intensive inter- administrative personnel), 1,120 respondents pro-
actions between the client and service personnel and vided responses, which was above the threshold of
hinges on the empathy and sympathy of these person- 80% that is recommended for primary social net-
nel. Communication, interpersonal aspects, and time work studies (Wasserman and Faust 1994). Within
spent are key to patient perceptions of such interac- the different user groups, we found the response rate
tions. For instance, communication, which incorpo- to be highest among administrative personnel (n =
rates patient education, will be seen by patients as 190), followed by paraprofessionals (n = 770), and
being key to their care when they are at the hospi- lowest among doctors (n = 160). To assess nonre-
tal and even when they leave the hospital (e.g., home sponse bias, we compared the respondent and non-
care). When doctors, paraprofessionals, and adminis- respondent demographic profiles. We found that the
trative personnel are rated highly on each of those profiles were comparable and statistically equivalent,
three components, it contributes to a greater level of with one exception—i.e., among doctors, more of the
satisfaction. Thus, we hypothesize as follows. nonrespondents were contracted doctors who were
Hypothesis 6 (H6). Quality-of-care metrics—i.e., tech- only at the hospital part time, which was not seen as a
nical quality, communication, interpersonal interactions, major threat because their expected use of the solution
and time spent—will positively influence and role in the advice network was expected to be
more minimal compared to those doctors employed
full time at the hospital. We used only the usable
Method responses to construct the advice network matrices
Context and System (e.g., 160 × 160 in the sample of doctors; 11120 × 11120
Our study was conducted in the context of an imple- in the entire sample) and in the all data analyses.
mentation of an IT-based enterprise-wide healthcare All patients received a survey to assess their satis-
solution, which we term E-HealthSys to maintain con- faction with the care and administration at the hos-
fidentiality, in a private hospital. The hospital pro- pital. Although the exact number of surveys mailed
vided a complete range of healthcare services to was not shared with us, a total of 8,440 patient
patients. The hospital had about 800 beds and boasted and/or authorized decision-maker responses were
a medium-sized emergency care operation. The hospi- received. Each doctor and paraprofessional had, on
tal had on its staff just under 250 doctors, with about average, about 40 and 60 responses, respectively. Each
20% of them being contracted on an as-needed basis. administrative staff member had, on average, about
These contracted doctors were typically at the hospi- 65 responses.
tal on one or two days of the week, depending on
the workload. There were about three times as many Procedure
paraprofessionals working at the hospital across vari- The study was conducted in conjunction with the
ous shifts. Finally, a little over 200 administrative staff implementation of E-HealthSys at the hospital. The
members were involved in the running the hospital. timeline for the major activities and data collected
E-HealthSys was designed to support all aspects is shown in Table 2. There was strong support for
of patient care, including patient health informa- E-HealthSys from the top management, and this was
tion, health records, treatment plans, billing, and reflected in their interest in collecting data from their
follow-up. In that sense, this system is typical of those employees. The researchers provided input into the
that hospitals are currently implementing in an effort questionnaire that was being administered by the hos-
to modernize operations and become more effective pital. The hospital retained a market research firm
and efficient. The system was developed by a leading to assist with the data collection to ensure that the
vendor and was customized to fit the needs of the employees were comfortable with sharing informa-
specific hospital over a six-month period before the tion honestly and also to ensure the privacy and con-
training. Some doctors, paraprofessionals, and admin- fidentiality of employee responses.
istrative personnel were interviewed by the vendor in As can be seen in Figure 1 (model diagram shown
the process of customizing the system. earlier), one of the key aspects of our research design
is the three distinct sources used in the data col-
Participants lection: (1) individual-level and social network data
The participants were doctors, paraprofessionals, and from employees; (2) use data from system logs; and
administrative personnel at the hospital and patients (3) patient satisfaction and related data from patientsVenkatesh et al.: A Longitudinal Field Study of an Electronic Healthcare System Implementation
Information Systems Research 22(3), pp. 523–546, © 2011 INFORMS 533
Table 2 Data Collection Timeline
T0: Pretraining T1: Month 1 T2: Months 2–3 T3: Months 4–12
Archival measures of Training takes place over a E-HealthSys is installed and Change management support
preimplementation quality 1-month period, with available on all computers. is measured at the end of
of care from patient several sessions available. month 6.
surveys.
Survey to collect Use is averaged over this
individual-level variables period.
and social network data.
Archival measures of
post-implementation
quality of care from patient
surveys.
and/or authorized decision makers. Several training essary to access data. Approximately two months was
sessions were offered over the month before the avail- deemed the learning phase by the management. Dur-
ability of the system. Management mandated that ing this period, the vendor and upper management
within a month all employees had to attend one ses- held three weekly town hall meetings to get feedback
sion tailored to their user group, and consistent with from users. Fixes and changes were effected during
this, almost everyone attended a session, although this period. The next nine months to the end of the
some of the contracted doctors could not fit this into first year of deployment was considered the period of
their schedule. The training sessions were tailored evaluation by management, at the end of which they
to the needs of the specific user groups—i.e., doc- were to take stock of the system and decide on possi-
tors, paraprofessionals, and administrative personnel. ble course corrections. During this nine-month period,
Anyone was welcome to attend any session or multi- no major changes were made to the system. Also, dur-
ple sessions. Each training session spanned approxi- ing this period, on-call problems (bugs reported and
mately 4 hours, and employees could attend as many time taken to fix the bugs) were tracked. It was esti-
sessions as they desired. The number of participants mated that approximately 80 man hours were dedi-
in any session was capped at 25 to facilitate small cated to addressing problems in the first month and
class sizes. Several sessions were run in parallel, and that number was down to fewer than 40 hours in the
given the around-the-clock nature of a hospital, ses- second month and fewer than 5 hours by the third
sions were offered 16 hours a day. In order to accom- month, thus suggesting that the technical aspects of
modate this hectic training schedule, at times during the implementation were reasonably well executed.
the month the hospital ran at less than 100% capac- We gathered use data from e-healthcare system logs
ity and postponed some nonemergency hospitaliza- over this nine-month period. Although we continued
tion visits or referred them to their sister hospital to gather use data, we sought to explain use dur-
about 30 miles away. Given the sheer number of train-
ing this phase of the implementation—i.e., termed the
ing sessions, especially in parallel, it was impossible
shakedown phase—because it can make or break a
to eliminate trainer variability, but because the train-
system (see Morris and Venkatesh 2010). During this
ers followed a specific script, biases were minimized.
period, the system was available to provide patient
Also, trainer dummy variables were not significant,
care and handle follow-up administrative care. About
thus further minimizing potential biases. Pertinent to
a week following each patient’s hospital visit, a sur-
our study, as can be seen from Table 2, we gath-
vey was mailed to them to collect data on the care
ered pretraining data about patient satisfaction, which
they received. One follow-up survey was sent two
was a control variable. Immediately following the
training, in conjunction with the organization’s sur- weeks after the initial survey, and one follow-up
vey, individual-level and social network data were phone call was made another two weeks later in order
gathered. Immediately after completion of their train- to enhance the response rate. In cases where patients
ing session, doctors, paraprofessionals, and adminis- were unable to participate, authorized decision mak-
trative personnel filled out a survey that was used ers were sought to fill out the survey.
to gather individual-level variables and social net-
Measures
work data.
The appendix lists the items from the survey that
After the training sessions were completed,
were used in this paper.
E-HealthSys was made available on desktop com-
puters, laptop computers, and handheld tablet com- Survey of Health-Care Professionals. Various
puters throughout the hospital. Internet access was individual-level variables were measured primarily
available throughout the hospital and was often nec- for use as control variables. The social network data,You can also read