Does Treatment of Paradoxical Vocal Fold Movement Disorder Decrease Asthma Medication Use? - sbccp
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Laryngoscope
C 2016 The American Laryngological,
V
Rhinological and Otological Society, Inc.
Does Treatment of Paradoxical Vocal Fold Movement Disorder
Decrease Asthma Medication Use?
Scott Kramer, MD; Brad deSilva, MD; L. Arick Forrest, MD; Laura Matrka, MD
Objectives/Hypothesis: To determine whether diagnosis and treatment of paradoxical vocal fold movement disorder
(PVFMD) leads to decreased asthma medication use. Secondary objectives include determining initial rate of asthma medica-
tion use, characterizing symptom improvement, and correlating with pulmonary function testing (PFT).
Study Design: Prospective observational study.
Methods: Patients newly diagnosed with PVFMD at a single institution were recruited to participate. Medication ques-
tionnaires were completed at the initial visit, at the first return visit for therapy, and at 6 months. PFTs were reviewed when
available.
Results: Sixty-six patients were recruited; the study was closed early because findings reached significance. Fifty-six
patients (85%) were taking asthma medication at presentation. Forty-four patients presented with PFTs, and two-thirds were
normal. Forty-two patients completed follow-up questionnaires; 79% decreased asthma medication use (P < .001), and 82%
reported symptom improvement. Seventy-seven percent of patients participated in therapy and 23% did not, with equal rates
of decrease in asthma medication use between these groups. Outcomes did not vary based on PFT pattern (i.e., obstructive
vs. nonobstructive, P 5 .75).
Conclusions: Diagnosis and treatment of PVFMD lead to a decline in asthma medication use. This decrease occurred
alongside symptom improvement and irrespective of PFT findings. Use of asthma medication in this patient population is
high, at 85%.
Key Words: Paradoxical vocal fold movement, vocal cord dysfunction, asthma.
Level of Evidence: 4.
Laryngoscope, 127:1531–1537, 2017
INTRODUCTION effect on their dyspnea, and the inhaled medication
Paradoxic vocal fold movement disorder (PVFMD) causes laryngeal irritation that worsens their symptoms
is a disease characterized by intermittent episodes of and prompts further inhaler usage, propagating the
dyspnea, cough, and stridor. This clinical constellation is cycle. No studies have previously determined the effect
nonspecific, and many patients with PVFMD are initial- of diagnosis and treatment of PVFMD on asthma medi-
ly tested and treated for asthma before a proper diagno- cation use.
sis is reached.1–3 Early diagnosis and treatment is It can be difficult to distinguish PVFMD from asth-
critical, because undiagnosed PVFMD has been linked ma; furthermore, asthma and PVFMD frequently coex-
with very high healthcare costs, and efficacious therapy ist, with varying symptomatic contributions from each
is available.4,5 Asthma is one of the most common mis- entity.9 Patients who are referred for PVFMD evaluation
diagnoses, and patients referred to the otolaryngologist by pulmonologists have often been told they have a
for PVFMD evaluation may already be taking asthma degree of asthma, but with symptoms out of proportion
medication.6–8 Patients with PVFMD who use asthma to asthma alone. It can be unclear what proportion of
medications may in fact worsen their dyspnea, second- their symptoms is due to asthma versus PVFMD. Some
ary to a vicious chemical-physiologic cycle. In this cycle, patients undergo pulmonary function testing (PFT) and
patients use asthma medication without significant are prescribed asthma medications, but are still not
definitively given the diagnosis of asthma.
The primary objective of this study was to deter-
From the James Care Voice and Swallowing Disorders Clinic, The
Ohio State University, Wexner Medical Center, Columbus, Ohio, U.S.A. mine if the treatment of PVFMD leads to decreased use
Editor’s Note: This Manuscript was accepted for publication of asthma medication. A secondary objective is to deter-
September 27, 2016. mine if diagnosis and education alone (absent the com-
A portion of this research was presented at the American
Broncho-Esophageal Association Annual Meeting, Las Vegas, Nevada,
pletion of any formal therapy) has any effect on
U.S.A., May 14, 2014. medication use. Tertiary objectives are to determine 1)
The authors have no funding, financial relationships, or conflicts symptomatic response to diagnosis and treatment of
of interest to disclose.
Send correspondence to Laura Matrka, MD, Ohio State University, PVFMD, 2) the percentage of patients presenting for
Wexner Medical Center, Eye and Ear Institute, Suite 4000, 915 Olentangy PVFMD evaluation who are already using asthma medi-
River Road, Columbus, OH 43212. E-mail: laura.matrka@osumc.edu
cation, 3) any differences in the above outcomes based
DOI: 10.1002/lary.26416 on PFT patterns.
Laryngoscope 127: July 2017 Kramer et al.: Treatment of PVFMD and Asthma Medication
1531MATERIALS AND METHODS data collection, the Ohio State University Institutional Review
Board approved the study protocol. Patients newly diagnosed
Study Design with PVFMD ages 13 to 80 years were recruited to participate
This is a prospective observational cohort study of 66 in a consecutive manner. Diagnosis of PVFMD was made based
patients conducted at the JamesCare Voice and Swallowing Dis- upon previously described guidelines.10 All patients diagnosed
orders Clinic at The Ohio State University, Wexner Medical with PVFMD underwent flexible transnasal laryngoscopy and
Center from July 1, 2013 to July 1, 2014. Prior to beginning demonstrated evidence of all of the following: 1) inappropriate
Fig. 1. Initial medication questionnaire completed at the time of diagnosis.
Laryngoscope 127: July 2017 Kramer et al.: Treatment of PVFMD and Asthma Medication
1532Fig. 2. The follow-up questionnaire shown is completed at first postdiagnosis visit and at 6 months.
adduction of vocal folds during quiet respiration, breath hold- Data Collection
ing, counting tasks, or after physical exertion or odor presenta- Upon diagnosis and subsequent consent to participate in
tion as described by Forrest et al.10; 2) full abduction at some the study, patients completed a medication questionnaire (Fig. 1)
point during the exam, ruling out paresis or paralysis; 3) no evi- examining their use of short-acting and long-acting b-agonists,
dence of another cause of airway obstruction. If evidence of inhaled or oral corticosteroids, inhaled corticosteroid/b-agonist
inappropriate movement was not observed at rest or with the combinations, leukotriene inhibitors, and inhaled anticholinergic
provocative respiratory tasks, patients were challenged with medications. Patients were then educated on the features of
either exercise or odor presentation, if either was noted as a PVFMD, using the video of their laryngoscopy to illustrate key
symptom trigger for the patient. aspects, and they were offered a course of laryngeal control ther-
Exclusion criteria for study participation included: 1) sys- apy. Laryngeal control therapy was performed by a licensed
temic corticosteroid use for another disease besides asthma or speech language pathologist (SLP) with specialized training in
chronic obstructive pulmonary disease, 2) evidence of other the treatment of PVFMD. A second medication questionnaire
laryngeal pathology affecting vocal fold mobility, 3) previous (Fig. 2) was completed at the start of the first return visit for
treatment or diagnosis of PVFMD, and 4) inability to partici- laryngeal control therapy to capture any effect from the initial
pate in laryngeal control therapy for cognitive reasons. Whether visit and its associated education alone. The same follow-up
a patient was definitively diagnosed with asthma in addition to questionnaire was completed at approximately 6 months follow-
PVFMD did not affect eligibility, for reasons noted above. When ing diagnosis, whether or not therapy had been completed.
available, PFT results were reviewed for evidence of an obstruc- Patients were also questioned on subjective symptom improve-
tive pattern; PFT results had no bearing on diagnosis or eligibil- ment and the number of completed laryngeal control therapy ses-
ity to participate. The study was initially designed to recruit sions. PFT results were collected and tabulated when available.
200 patients. However, due to the significance of results at an Diagnosis of obstructive airway disease was based on the forced
interval analysis time point, the decision was made to report expiratory volume in 1 second (FEV1), forced vital capacity
results early and close the study. (FVC), FEV1/FVC ratio, and the pulmonologist’s interpretation.
Laryngoscope 127: July 2017 Kramer et al.: Treatment of PVFMD and Asthma Medication
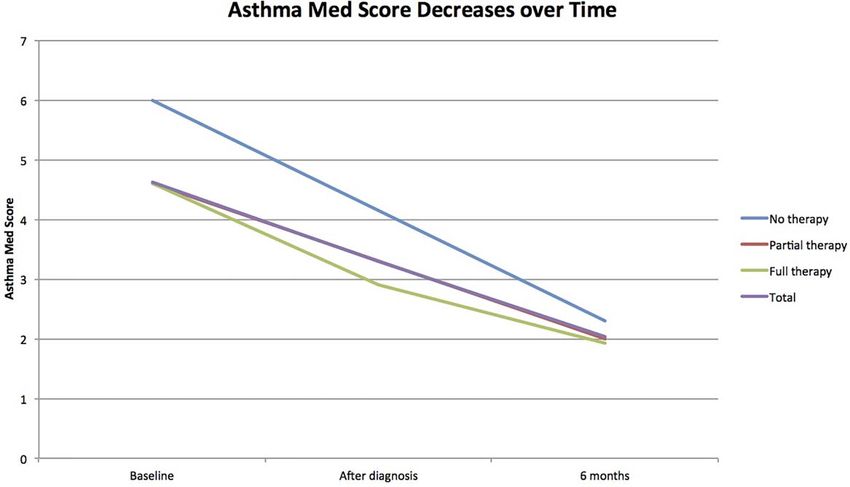
1533Fig. 3. The asthma medication score decreases after diagnosis alone and after therapy, regardless of how much therapy is completed.
Data included are only from time points with at least two responses. “Partial therapy” and “Full therapy” lines are closely overlapping.
Statistical Analysis Seventy-two percent (18 of 25) of those completing a full
Patients were assigned a numerical score based on the fre- course of therapy (two or more sessions, as determined by
quency with which they used medications. The frequency inter- the therapist) demonstrated a decrease in asthma medica-
vals are detailed in Figures 2 and 3. Subjects were assigned tion use, compared with 100% (five of five) of those com-
values of 1, 2, 3, or 4 for each increasing frequency interval. pleting a partial course; the decrease in medication use
For example, a patient using a short-acting b-agonist less than was significant, but the difference between the two groups
2 days per week received one point, whereas a patient using the
was not. Nine patients completed no laryngeal control
same medication more than two days per week received two
points. Once numerical values were assigned, the values from
therapy, and eight of those (89%) showed decreased asth-
each category were added together to form an aggregate score ma medication use. The mean decrease in asthma medica-
(asthma medication score). The asthma medication scores for tion score was 2.68 for patients completing a full therapy
each subject were compared at each time point for which data course, 2.60 for patients completing a partial therapy
were available. Asthma medication scores were compared using course, and 3.44 for patients completing no therapy (P 5
the paired-samples t test or one-way analysis of variance. Nomi- .71; Fig. 3). The mean asthma medication score decreased
nal variables were compared using v2 analysis. Data were from 4.62 to 3.29 after patients received a diagnosis alone,
analyzed using SPSS software (IBM, Armonk, NY). before any treatment (P 5 .03).
RESULTS
Asthma Medication Use at Presentation and
Patient Characteristics Symptom Improvement
Sixty-eight patients were identified as eligible to Fifty-six patients (84.8%) were using asthma medi-
participate during the study period. Two were excluded cation at the time of presentation. Fifty-four patients
because of chronic systemic corticosteroid use for dis- (82%) reported symptomatic improvement of their symp-
eases besides asthma or chronic obstructive pulmonary toms after diagnosis and/or treatment of their PVFMD.
disease. Eighty-five percent were female, and the medi- Ninety-two percent of patients completing a full therapy
an age was 42 years. Forty-two patients completed course reported improved symptoms, compared with 60%
follow-up questionnaires, 40 of whom completed ques- of patients completing a partial course and 66.7% of
tionnaires at least 6 months out from diagnosis (Table patients completing no therapy (P 5 .09). Baseline asth-
I). The remaining two completed follow-up question- ma medication score was not significantly different
naires at the initial therapy visit but not thereafter. between these groups.
Diagnosis and Treatment of PVFMD Decreased PFT Data Did Not Impact Asthma Medication
Asthma Medication Use Use or Symptoms
Overall, the mean asthma medication score decreased Forty-four patients (66%) had PFT data available;
from 4.85 at diagnosis to 2.40 at last follow-up (P < .001). 57% of these demonstrated no evidence of asthma,
Laryngoscope 127: July 2017 Kramer et al.: Treatment of PVFMD and Asthma Medication
1534TABLE I.
Follow-up Data.
Asthma Medication Score Symptoms (%)
Baseline After Diagnosis 6 Months P Value Improved Unchanged P Value
Therapy completed
None (n 5 9) 6 NA 2.3 .71 66.7 33.3 .09
Partial, 1 session (n 5 5) 4.6 NA* 2 60 40
Complete, 2 or more (n 5 25) 4.6 3.17 1.92 92 8
PFT result
No obstructive pattern (n 5 25) 5.08 3.17 2.29 .75 70.6 29.4 .43
Obstructive disease (n 5 19) 5.53 5 2.85 83.3 16.7
Total 4.62 3.29 2.03session. Of course, even if symptom severity was initially symptomatic improvement may be under- or over-
less for this subgroup, they did not have less pathologic reported by this study. However, by reaching out to all
PFT results; the incidence of an obstructive pattern on patients at the 6-month point, whether they had been
PFT was the same (P 5 .24). Finally, it is possible that lost to follow-up or not, we attempted to avoid this bias.
poor compliance explains the lack of difference among
these groups; many of those participating in therapy
may have been noncompliant with the daily laryngeal Implications and Future Directions
control exercises outside of therapy appointments, and This study highlights the importance of diagnosing
therefore gained little additional benefit beyond that of and treating PVFMD. Patients properly diagnosed and
the education and instruction given at the initial visit. treated use less asthma medication and have improved
Eighty-five percent of patients referred to us were symptoms, avoiding the hassle, cost, and side effects of
being treated with asthma medication, 43% of those taking superfluous medication. Although we do not specif-
with PFT performed had an obstructive pattern, and the ically counsel patients regarding asthma medication use,
majority was female. These characteristics are compara- results of this study have led many in our practice to rou-
ble with other series of PVFMD patients.3,4 The median tinely recommend that the patient revisit his or her asth-
age of 42 years is also on par with the subjects of the ma medication regimen with the pulmonologist once
aforementioned studies (42.6 and 45, respectively). symptoms are improving. Future directions include an
Although PVFMD has been described specifically in expansion of this study to our pediatric population, which
young athletic persons, it is clearly not restricted to this is currently underway. Other studies might include a
demographic. cost-analysis of diagnosis and treatment of PVFMD ver-
Although many patients had previously undergone sus the cost of a missed diagnosis; the cost of the initial
PFT, our subjects were not initially stratified based on visit, flexible laryngoscopy procedure, and speech therapy
PFT results or a preexisting diagnosis of asthma. There is likely much less than the cost of inappropriate medica-
are several reasons for this. First of all, a diagnosis of tion usage, missed work, emergency service utilization,
asthma does not exclude the possibility of PVFMD. Sug- and multiple medical visits. Further research might focus
gestive PFT results, and even a positive methacholine on PVFMD in patients with chronic obstructive pulmo-
challenge test, cannot rule out PVFMD. Additionally, nary disease, laryngopharyngeal reflux, or allergic rhini-
some patients referred by a pulmonologist have PFT tis and their use of disease-specific medication. We
suggestive of obstructive disease but do not have a clear encourage otolaryngology and nonotolaryngology practi-
diagnosis of asthma. They may have symptoms incom- tioners to have a high suspicion for this disorder in
pletely controlled by inhaled b-agonists, or their symp- patients with otherwise unexplained dyspnea.
tom severity is out of proportion to PFT findings.
Additionally, patients with asthma undergoing PFT who CONCLUSION
are already controlled on proper medication may have Diagnosis and treatment of PVFMD leads to a
nondiagnostic results. The authors felt that if a referring decline in use of asthma medication. This decrease in
pulmonologist was not able to give a definitive diagnosis medication use occurs even as symptoms improve.
of asthma based on the available information, it would Decreased use of asthma medications is seen immediate-
be inappropriate for us to do so. Thus, PFT data do not ly after the initial diagnostic visit for many patients,
impact patient eligibility. Results were compared
typically with further decrease in medication use and
between the group of patients with obstructive pattern
symptomatic improvement as therapy proceeds.
on PFT and those without an obstructive pattern, but it
This is the first study, prospective or otherwise, to
should be clear that this is not the same as a comparison
demonstrate a decrease in asthma medication use with
between patients with coexisting asthma and those with-
diagnosis and treatment of PVFMD. Future endeavors
out. PFT results did not impact asthma medication use.
should examine the overall expense of misdiagnosed
In other words, both patients with PFT evidence of
PVFMD, including the cost of asthma medication and
obstruction and those without evidence of obstruction
emergency care, and compare this with the cost of diag-
significantly decreased their asthma medication scores.
nosing and treating PVFMD.
Study Limitations BIBLIOGRAPHY
A potential point of bias is that compliance with 1. Seear M, Wensley D, West N. How accurate is the diagnosis of exercise
home therapy exercises was not measured. Another is induced asthma among Vancouver schoolchildren? Arch Dis Child 2005;
the relatively low rate of patients completing follow-up 90:898–902.
2. Newman KB, Dubester SN. Vocal cord dysfunction: masquerader of asth-
questionnaires (64%). There are several possible reasons ma. Sem Respir Crit Care Med 1994;15:161–167.
for this. Importantly, speech therapy (and particularly 3. Newman KB, Mason UG, Schmaling KB. Clinical features of vocal cord
dysfunction. Am J Respir Crit Care Med 1995;152(4 pt 1):1382–1386.
laryngeal control therapy) is not covered by certain 4. Chiang T, Marcinow AM, deSilva BW, Ence NB, Lindsey SE, Forrest AL.
insurance carriers. Patients may become lost to follow- Exercise induced paradoxical vocal fold motion disorder. Laryngoscope
2013;123:727–731.
up if they seek less expensive care elsewhere or deter- 5. Sullivan MD, Heywood BM. A treatment for vocal cord dysfunction in
mine that laryngeal control therapy is not worth the female athletes: an outcome study. Laryngoscope 2001;111:1751–1755.
6. Christopher KL, Wood RP, Eckert RC, Blager FB, Raney RA, Souhrada JF.
cost at all. Symptom severity or resolution may also lead Vocal-cord dysfunction presenting as asthma. N Engl J Med 1983;308:
to the choice not to follow up. Thus, the true rate of 1566–1570.
Laryngoscope 127: July 2017 Kramer et al.: Treatment of PVFMD and Asthma Medication
15367. Traister RS, Fajt ML, Petrov AA. The morbidity and cost of vocal cord 11. Mikita J, Parker J. High levels of medical utilization by ambulatory
dysfunction misdiagnosed as asthma. Allergy Asthma Proc 2016;37: patients with vocal cord dysfunction as compared to age- and gender-
25–31. matched asthmatics. Chest 2006;129:905–908.
8. Traister RS, Fajt ML, Whitman-Purves E, Anderson WC, Petrov AA. A 12. Doshi DR, Weinberger MM. Long-term outcome of vocal cord dysfunction.
retrospective analysis comparing subjects with isolated and coexistent Ann Allergy 2006;96:794–799.
vocal cord dysfunction and asthma. Allergy Asthma Proc 2013;34: 13. Marcinow AM, Thompson J, Chiang T. Paradoxical vocal fold motion disor-
349–355. der in the elite athlete: Experience at a large division I university.
9. Yelken K, Yilmaz A, Guven M, Eyibilen A, Aladag I. Paradoxical vocal fold Laryngoscope 2014;124:1425–1430.
motion dysfunction in asthma patients. Respirology 2009;14:729–733. 14. Han JJ, Lee JH, Oh SH, Chang SO. Assessing the effects of tinnitus
10. Forrest LA, Husein T, Husein O. Paradoxical vocal cord motion: classifica- retraining therapy in patients lost to follow-up: a telephone survey. Otol
tion and treatment. Laryngoscope 2012;122:844–853. Neurotol 2015;36:581–587.
Laryngoscope 127: July 2017 Kramer et al.: Treatment of PVFMD and Asthma Medication
1537You can also read