Elderly Care Break-out session International Visitors Programme 2017
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

@TFHealthcare Break-out session Elderly Care International Visitors Programme 2017

@TFHealthcare
ROOM 7.04
Elderly Care
10:45 Elderly care in the Netherlands
Martin Holling, Ministry of Health, Welfare & Sport
11:00 Q&A
11:20 From PPP to innovation: Fall Prevention Project TOM
Inge Mohede, Nutricia Advanced Medical Nutrition
Ruud van Vessum, Philips
Saskia Kloet, Veiligheid NL
12:00 End
Agenda
@TFHealthcare Elderly care in the Netherlands Martin Holling, Ministry of Health Welfare & Sport

Wet langdurige zorg (Wlz) Long term care act HEALTH (CARE) IN THE NETHERLANDS vno-ncw Martin Holling 27-9-2017
Content
•LTC changes: motives
•Main differences before and after 2015
•Wlz main topics
•Innovation agenda
5
International differences
topics:
• Broad public
• insurance
• Low rate
• informal care
• High rate
• Institutional care
6
7 source: Health at a glance OECD
Reform of Long Term Care: Process •Goals: oDecrease LTC expenditures oImprove balance formal and informal care oImprove quality of care => more person-centred care 8
Measures • Focus on care at home, reduce institutional care • Stimulate informal care • Budget household care (cleaning): -/-40% • The Long-term Care Act (Wlz) has replaced the Exceptional Medical Expenses Act (AWBZ) • Parts of the former ‘AWBZ’ are shifted to: • the Health Care Insurance Act (ZVW) • the renewed Social Support Act (Wmo 2015) and • the Youth Care Act 9

Present system
LTC Expenditures 2015 13%
4%
Social Support Act (Wmo)
Social participation; Municipality 16%
66%
Youth Care Act
Care for young people and their parents, Social participation , Municipality
Health Insurance Act (Zvw)
(mandatory) private healthcare insurance: GP’s / therapists / medication / hospital
care / specialists / ambulance transport / audiovisual and locomotory aids
Long-term Care Act (Wlz)
Replaced the Exceptional Medical Expenses Act (AWBZ). The Wlz is a (mandatory)
public long-term care insurance: nursing homes / homes for the elderly / home care
/ institutional care for disabled people and people with chronic psychiatric disorders
10Wlz structure
Cliënt CIZ
Regional care
offices
Care provider
11Wlz highlights I
Entry barriers
Criteria connected to care:
• Structural care need and
• Clients in need for 24 h surveillance or
• 24 h care nearby
12Wlz highlights II
• Integral package
➢Care in institution or care at home
➢Personal care, guidance and nursing
➢Medical treatment
➢Transport (in combination with care)
• Several clients
➢Older persons
➢Handicapped persons
➢Persons with psychiatric problems (> 3 years care)
13Innovation Agenda
Letter to Parliament: February 2016
“You can live in dignity while receiving care”
(“waardig leven met zorg”).
-Topics:
- More care arrangements for clients: experiment “Personal
care”
- More care innovation (E-Health-Technology)
- More care at home
- Improving quality (new quality framework 2017)
14@TFHealthcare
ROOM 7.04
Elderly Care
10:45 Elderly care in the Netherlands
Martin Holling, Ministry of Health, Welfare & Sport
11:00 Q&A
11:20 From PPP to innovation: Fall Prevention Project TOM
Inge Mohede, Nutricia Advanced Medical Nutrition
Ruud van Vessum, Philips
Saskia Kloet, Veiligheid NL
12:00 End
Agenda@TFHealthcare From PPP to innovation: Fall Prevention Project TOM Inge Mohede, Nutricia Advanced Medical Nutrition Ruud van Vessum, Philips Veiligheid NL
Fall prevention program: A practical multi-partner approach
Content
• WHY: Important • HOW: a coalition • WHAT: a • FIRST impression
facts about falls of multi-partners sustainable and next steps!
and seniors multifactorial
approach-
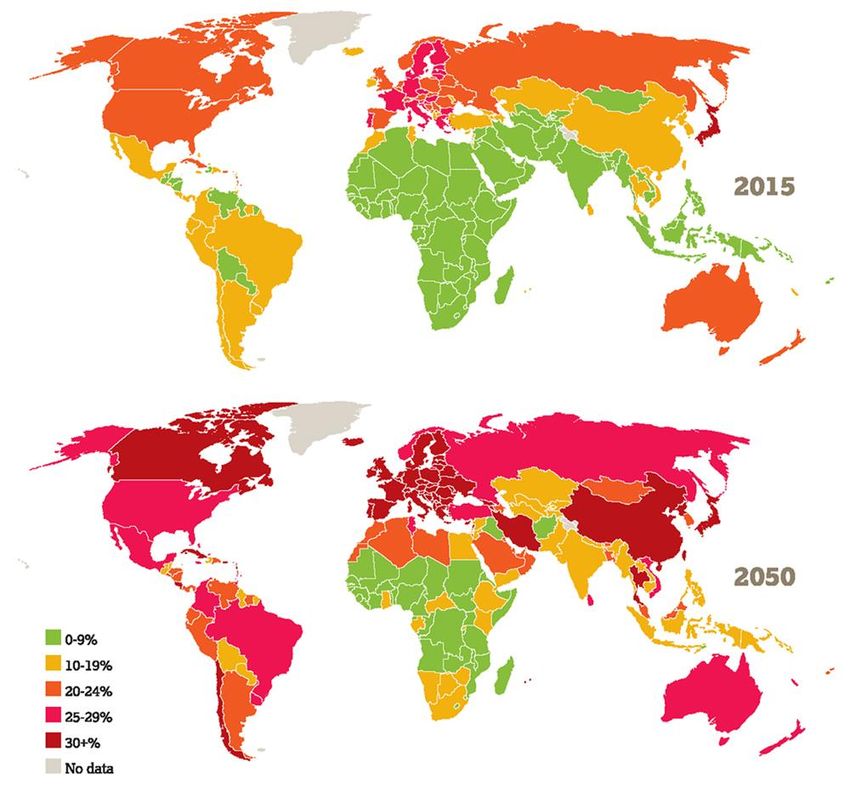
program TOMFacts about ageing
Portion of population aged 60 or over.
Ageing
One of the dominating trends in the world
Ageing
Requires a proactive approach
Ageing
Can create as many opportunities as issues
Ageing
Is only partially a medical topic
Ageing
Is changing society
Source: UNDESA Population division, World population prospects: the 2015 revision, DVD Edition, 2015Definition of health Definition of health 1948: • Health is a state of full physical, mental and social wellbeing (WHO). Definition of health 2011: • The ability to adapt and self manage in the face of social, physical, and emotional challenges • Health is the capacity of people to adapt and orchestrate, in the sense of the physical, emotional and social challenges of life. Being healthy means being able to adapt to disruption, being resilient, being able to maintain or rediscover a balance both physically, mentally and socially (taken from Huber et al., 2011).
Seniors and key areas of concern
Independence
Mobility ( self-reliance)
Loneliness Safety
Source: Indicatie zorgvraag 2030
TNO study on behalf of the Dutch Ministry of healthForecast on functioning of older people in 2030
50-60% of the population above 65 years of
age
Most common
problem Mobility
+/- dementia/
moderate dementia
Source: Indicatie zorgvraag 2030
TNO study on behalf of the Dutch Ministry of healthFalls: threat for seniors’ safety and independence and generate enormous economic and personal costs Key facts: • Falls are the second leading cause of accidental or unintentional injury deaths worldwide. • Each year an estimated 646 000 individuals die from falls globally of which over 80% are in low- and middle-income countries. • Adults older than 65 years of age suffer the greatest number of fatal falls. • 37.3 million falls that are severe enough to require medical attention occur each year.
Urgency • “Ministry encourages regional collaboration in order to live longer at home” (letter to parliament, 2014) • “Seven out of ten 75+ would prefer to live in their own house until death” (WoON, 2010)
NL: Shift of care to the community due to budget pressure
TODAY TOMORROW
Focus: on treatment Focus: early diagnosis /prevention
Care services mainly provided in Care services are increasingly provided in
Budget pressure
formal setting (e.g. hospital) informal setting (e.g. community centers,
home)
Payments of health-care services: Payment shared:
predominantly Health Insurance Health Insurance Companies &
Companies Municipalities
Doctor-centric model Patient-centric model (pro-active self
management becomes key!)
Prof.
care
Professional Informal care
care
Tools + Technology
Informal care
Tools + Technology Self + Network
Self + NetworkContent
• WHY: Important • HOW: a coalition • WHAT: a • FIRST impression
facts about falls of multi-partners sustainable and next steps!
and seniors multifactorial
approach-
program TOMMotivation: Call for action
Our purpose as ONVZ is to create added value for both healthy and unhealthy
insured. A patient centric approach: involve the insured involved, improving
outcomes that matter to them.
PostNL seeks to find smart solutions for societal challenges like ageing and
individualism, by i.e. developing new services that involve personal contact with the
well-known an trusted mailmen at the home address mostly digital world.
At Philips, we strive to make the world healthier and more sustainable through
innovation.
Our goal is to improve the lives of 3 billion people a year by 2025.
An unique opportunity and coalition that combines effective interventions into an
appealing program for seniors, enhances professionals with added skills and prevent
fall related injuries.
At Nutricia Danone, we believe in the power of nutrition at the heart of health and
healthcare. We pioneer new business relationship. One that co-creates and even
co-owns solutions with non for profit organizations, the public sector, local
stakeholders, other companies and academics.Our Mission To support seniors to preserve the highest degree of autonomy in order to longer live independently (at home) by offering an innovative and sustainable care path with prevention solutions reducing number of falls or fall related injuries
What is different
• 4 companies and 1 NGO taking the lead
• Focus on: Focus, Cooperation, Implementation and Continuation
• Working and investing in the cooperation
• We use proven concepts and solutions
• Clear common goals (KPIs) and project plan.
A business like approach
With full attention to the human aspectsOur focus is implementation & continuation Implementation with local relevant partners: Selection based on: • Added value in the project • Drive for real improvement • Ability to scale and maintain
Content
• WHY: • HOW: a coalition • WHAT: a • FIRST impression
Important facts of multi-partners sustainable and next steps!
about falls and multifactorial
seniors approach-
program TOMTOM approach
Nutrition Exercise
Senior
Monitoring Social supportTOM participant • 65 year and older • Increased fall risk • Access to a PC and an email address • No internal electronic equipment
TOM evaluation
We evaluate effect
• Mobility
• Health,
• QOL
We evaluate the proces
• Impact (seniors, health & social carers)
We evaluate the cost-efficiency
We optimize TOM for future implementation
• Execution in 4 Living Labs: Test-Learn-Adapt
• Develop a blueprint4 Living Labs
Living Lab 1 - BEST Living Lab 2 – VITAAL VECHTDAAL
• Recruitment participants: Senior • Recruitment participants: Municipality &
associations local healthcare professionals
• Medical care: Through specially trained
Senior
physiotherapists, dietician
Municipality
• Medical care: Through specially trained
district nurse, physiotherapists and dieticians
• Social care: associations • Social 1 line HCPs
care:
• PostNL • PostNL
• Active involvement specially
trained students
wellbeing/household support .
Living Lab 3 - Houten Living Lab 4 – Den Haag & A’dam
• Recruitment participants: local first line • Recruitment participants: policyholders
healthcare professionals
1 line HCPs
ONVZ (national) HIC
• Medical care:. Through specially trained • Medical care: Combination Face-to-face and
Pharmacies
district nurse, physiotherapists and dieticians videopolicyholders
support; if needed they are referred by
the platform to the relevant Health care
• Social care: e-HCPs
professionals.
• PostNL
• Social care:
• PostNL1st living lab in Best
Start: March 2017
Participants: n=50
Finish: August 2017
First Data: Q1 2018Content
• WHY: Important • HOW: a coalition • WHAT: a • FIRST impression
facts about falls of multi-partners sustainable and next steps!
and seniors multifactorial
approach-
program TOMFirst observations
• Collaboration with local senior association key driver
for attention
• Coalition of big national organizations gives
• Confidence to participants
• Lot of media attention
• Project needs several “local incubators” to learn-
adapt-optimize before expansionSecond impressions
‘Thanks to TOM we get a chance
This chance has been given to us
And now we are in balance
This is an enrichment to our life’
TOM BuddiesFirst learnings and feedback
Majority of participants in 1st Living Lab:
• Gave a high report mark for overall project
• Has more social contacts in local environment
• Improved their level of physical activity
• Felt better
- Availability - Location criteria - Presentation - Contact
- Various timeslots - Personal feedback moments
- UsabilityNext steps…
• Experience and evaluate following Living Lab’s
• Elements of TOM tailored in various local settings and infrastructures
• Develop “TOM tools” 2.0 (e.g. education for PT’s, Nurses and seniors)
• Develop a Blue Print for the TOM approach (learnings of 4 LL’s)
• Public availability of TOM approach (business model)TOM approach
• Optimize TOM for a
sustainable future
implementation in The
Netherlands
• TOM scope with an
international ambition
The “how-to” (form / model /
partnerships/ founding fathers) is
a constantly evolving process with
current partners.THANK YOU! Questions and discussion
@TFHealthcare Thank you! Let’s have some lunch
You can also read