Evaluation of Vaccination Coverages in the Health Care Workers of a University Hospital in Southern Italy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Ann Ig 2019; 31 (Suppl 1): 13-24 doi:10.7416/ai.2019.2273
Evaluation of Vaccination Coverages in the Health Care
Workers of a University Hospital in Southern Italy
R. Squeri1, V. La Fauci1, I.A.M. Picerno1, G. Trimarchi2, G. Cannavò3,
G. Egitto3, B. Cosenza4, V. Merlina4, C. Genovese4
Key words: Vaccine hesitancy, healthcare workers, coverage, vaccine
Parole chiave: Esitazione vaccinale, operatori sanitari, copertura, vaccini
Abstract
Introduction. An adequate immunization of the health care workers is essential for infection prevention
and control, to avoid consequences not only for them, but for all patients that the health care workers could
infect causing serious damage and / or death. Unfortunately, to date, despite the presence of international
and national guidelines (Law Decree 119/2017), the vaccination coverage was low, also because of the
“vaccine hesitancy” spread among the same health care workers. In light of the above, the aim of our study
was to investigate the vaccination coverage of healthcare workers of all the operational units present in our
hospital and to evaluate differences between sex, age, professional profile and area of work.
Materials and methods. A study was conducted from March to June 2018 to investigate the vaccination
coverage of healthcare workers at the University hospital “G. Martino” of Messina; data were collected
using a self-completion questionnaire based on Attachment 3 of Ministerial Circular 25233 of 18 August
2017. We verified any possible association between physicians and pediatricians and between age classes
by the chi square method. Also, a logistic regression was used for each vaccination, considering the vac-
cination as the variable and the following covariates: type of operative unit, sex, age and area) in order to
predict the probability of vaccination.
Results. We analyzed a sample of 822 health care workers (324 males and 498 females with an age of 49.5
± 10.5 SD). The sample was made up of physicians (36%), nurses (21%) and other professional categories
(43%). Analyzing the data we obtained vaccination coverages lower than the target required to guarantee
“herd immunity”; higher vaccination coverages were found for females, physicians and the clinical area
and - for influenza vaccination - in the older age groups and - for all the other vaccinations - in the younger
groups.
Conclusions. Data analysis revealed a lax attitude towards vaccinations by health care workers and the
need for measures aimed at increasing vaccination their coverage to prevent them from becoming a source
of dangerous outbreaks.
1
Department of Biomedical Sciences and Morphological and Functional Images, University of Messina, Italy
2
Department of Economics, University of Messina, Italy
3
DMPO AOU “G. Martino”, Messina, Italy
4
Postgraduate Medical School in Hygiene and Preventive Medicine, University of Messina, Italy14 R. Squeri et al.
Introduction of transmission of vaccine preventable
diseases to their patients and relatives,
Despite vaccines have always been and so dangerous outbreak could occur in
considered a successful and cost-effective healthcare environments (8, 9). In light of the
measure to improve health outcomes, in above, the aim of our study was to investigate
recent years there has been a global spread the vaccination coverage of HCWs of all
of a phenomenon known as “vaccine the operational units present in our hospital,
hesitancy”, indicating a delay in receiving AOU “G. Martino” of Messina, and to
vaccination or a refusal to be vaccinated evaluate differences between age classes
despite the availability of vaccination (20-30, 31-40, 41-50, 51-60 and 61-70 years
services (1-3). It involved many factors that of age) and between medical doctors and
could influence the decision to accept some pediatricians. Also, a logistic regression
or all the vaccines in accordance with the was used for each vaccination, considering
recommended schedule, or none at all. In the the vaccination variable and the following
end, this phenomenon resulted in a decrease covariates: type of operative unit, sex, age
of vaccination coverage, with values below and area, in order to predict the probability
the target of 95% coverage required for of vaccination.
“herd immunity”. This decrease was partly
attributable to the disinformation campaigns
implemented not only by the anti-vaccination Materials and methods
groups, but also by some healthcare workers
(HCWs), who should instead represent the The study was conducted from March
main stakeholders (4-6). to June 2018 using a self-completion
HCWs, in fact, do not always agree with questionnaire based on Annex 3. We
vaccinations. The literature ascribed this to the analyzed a sample of 822 HCWs. All the
fear of side effects, to the lack of confidence interviewees filled the questionnaire.
in the effectiveness of vaccinations and Summary statistics were calculated for
to organizational deficiencies in access to all parameters contained in Annex 3 (sex,
vaccination services (6-7). age, professional profile, vaccines carried
In line with the recommendations of the out, etc). The mean and standard deviation
Strategic Advisory Group of Experts (SAGE) was calculated for the sole quantitative
on Immunization of the World Health parameter (age) while absolute and relative
Organization (WHO), it was necessary to frequencies were obtained for qualitative
evaluate vaccine coverage on both a global data (sex, professional profile, vaccinations
and local scale. Few studies have evaluated carried out, etc.).
vaccine coverage of HCWs in healthcare We verified possible statistical differences
settings and the scientific literature was between vaccine coverage of physicians
therefore lacking (7). and pediatricians and between age classes
By Law n. 119 of 31 July 2017, as described above Therefore, 2x2 and
containing “Urgent provisions on vaccination 5x2 contingency tables were built and
prevention” and the connected Ministerial assumptions tested by the chi square method,
Circular 25233 of 16.08.2017, data collection while degrees of freedom were used to
on the vaccination status of teachers, social partition r x k tables.
care workers and HCWs is requested (Annex A multiple step logistic regression with
3). Hence, at present, HCWs are under stepwise model (10) was used for each
no legal obligation to be vaccinated, but vaccination considering the vaccination
they could represent a dangerous source variable (0 = unvaccinated and 1 =Vaccine coverage in HCWs in a University Hospital 15
vaccinated) and the following covariates general surgery, pediatric surgery, plastic
(independent variables x): type of operative surgery, thoracic and vascular surgery,
unit (clinical, surgical and services), sex, maxilla-facial surgery, gynecology and
age and qualification (physicians, nurse obstetrics, neurosurgery, ophthalmology,
and other healthcare workers). This method orthopedic, urology, otolaryngology.
allowed verifying the weight of the single The service area included: Health
covariates in order to predict the probability management, Pathology, Immunological
of vaccination. diagnostics and Virology, Clinical
Using the β parameters for measles, biochemistry, Clinical pharmacology,
chickenpox and mumps vaccination, which Physics, Occupational medicine, Hospital
presented all four globally significant hygiene, Sport medicine, Forensic
depressors (type of operative unit, sex, medicine, Nuclear medicine, Transfusion
age and qualification), we estimated the medicine, Clinical microbiology, Radiology,
probability of vaccination for females and Radiotherapy.
males (the only qualitative repressor) net of The sample included: physicians (30%);
the other variables present in the equation X doctors in training (6%); nurses (21%) and
area X age and X professional category, with other professional categories (43%) such
the following probability estimation model: as biologists, pharmacologists, laboratory
p (X) = e ^ (β_0 + β_1 X_1 + ⋯ β_p X_p) / (1 + e ^ (β_0 + β_1 technicians and administrative staff. The
X_1 + ⋯ β_p X_p)) sample was also stratified by age as follows:
20-30 (5.5%), 31-40 (12.9%), 41-50 (27.8%),
The logistic model provided a smaller 51-60 (36%), 61-70 years (16,8%).
sample size, as the operators who answered In the sample we found the highest
“not remember” or had “natural immunity” vaccination coverage for poliomyelitis
were removed from the dummy variable. (80%), diphtheria (72.4%), tetanus (76,8%)
Significance was set at α = 0.050; therefore and hepatitis B (77,3%); lower coverages
p-values of less than 0.050 for two-tailed emerged for measles, mumps, rubella,
tests were considered statistically significant. varicella and pertussis vaccinations and
The summary and inferential statistics were for some recently introduced vaccinations
analyzed using the software R (11). not specifically recommended for HCWs.
For some diseases the HCWs claimed to
have contracted especially exanthematous
Results diseases, in particular chickenpox. Vaccine
coverage and immunization status of the
Our sample comprised 822 HCWs (324 sample is represented in Table 1.
males and 498 females) with mean age = 49.5 Furthermore, we stratified the sample into
± 10.5 SD. The sample was divided into three three professional categories: physicians,
operational areas: clinical (42%), surgery nurses and other HCWs, evaluating
(28%) and services (30%). The clinical vaccination coverage into three groups as
area included: allergology, cardiology, represented in Table 2. We obtained higher
dermatology, metabolic diseases, geriatric, coverage for physicians for all vaccines
neonatology, hematology, endocrinology, except for hepatitis B, hepatitis A and herpes
infectious diseases, internal medicine, zoster, whose higher coverages were detected
emergency room, nephrology, neurology, in nurses. Higher varicella coverage was also
infantile neuropsychiatry, oncology, found in other HCWs. Statistical differences
pediatrics, pulmonology, psychiatry and were analyzed using a multivariate analysis
rheumatology. The surgical area included: (see table 3).16 R. Squeri et al.
Table 2 - Vaccination coverage reported by different
H.I.: haemophilus influenzae; INF: flu; MEN C: meningococcus C; MEN B; meningococcus B; PNE; pneumococcus; HAV: hepatitis A; HPV: papilloma virus; HZV:
* Legend: POL: poliomyelitis; DIF: diphtheria; TET: tetanus; HBV: hepatitis B; PER: pertussis; MEA: measles; RUB: rubella; CHI: chickenpox; MUM: mumps;
16.8% 21.3% 17.3% 12.5% 31.6% 27.4% 27.3% 28.5% 31.5% 39.8% 29.6% 39.4% 39.7% 39.8% 38.1% 37.3% 40.3%
80.0% 72.4% 76.8% 77.3% 29.5% 30.3% 30.9% 16.4% 23.7% 4.1% 14.0% 7.1% 3.1% 2.7% 7.1% 1.9% 1.1%
0.0% 0.6% 5.0% 14.9% 12.7% 22.4% 8.6% 0.1% 0.1% 0.0% 0.0% 0.1% 0.5% 0.0% 0.6%
MEN MEN PNE HAV HPV HZV categories of HCWs (excluding no respondents).
Physicians Nurses Other HCWs
POL 85.3% 76.6% 73.5%
DIF 77.7% 59.6% 63.8%
TET 76.0% 63.7% 64.1%
HBV 63.7% 73.1% 56.8%
PER 27.7% 18.7% 18.7%
MEA 28.8% 22.2% 27.9%
RUB 30.1% 22.8% 28.1%
CHI 19.2% 17.5% 23.7%
B
MUM 22.9% 16.4% 22.3%
H.I. 4.8% 2.3% 1.7%
C
INF 24.3% 11.1% 12.8%
MEN C 6.2% 3.5% 2.2%
INF
MEN B 3.8% 3.5% 1.1%
PNE 3.1% 1.8% 1.7%
HAV 5.1% 14.0% 6.4%
H.I.
HPV 1.4% 0.0% 1.4%
HZV 1.0% 1.8% 0.8%
MUM
TBC 32.5% 28.7% 25.3%
*For abbreviations see legend of Table 1.
herpes zoster virus; ^Based on the declaration of the HCWs: “I acquired the disease”
CHI
RUB
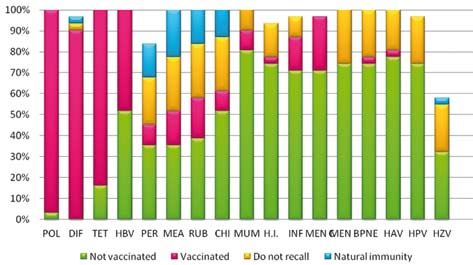
We also decided to evaluate the vaccine
coverage of pediatricians within the clinical
MEA
Table 1 - Vaccine coverage and immunization status of the sample
group as they were the category mainly
involved in childhood vaccine promotion.
We found higher rates of coverage for polio,
PER
diphtheria, tetanus and HBV; while lower
coverage rates were observed for the other
HBV
vaccines studied (Figure 1). Furthermore,
we wanted to search for the presence of
statistical differences of vaccine coverage
TET
between physicians and pediatricians:
we found only differences for measles,
DIF
0%
mumps, rubella, chickenpox (pVaccine coverage in HCWs in a University Hospital 17 Figure 1 - Vaccine coverage in pediatricians *For abbreviations see legend of Table 1. Natural immunity was based on the declaration of the HCWs “I acquired the disease” into Figure 2. The qualitative assessment We performed a multivariate analysis revealed significant differences between the and in Table 3 we represented only the five age groups for: poliomyelitis, hepatitis covariates that presented good explanatory A and tuberculosis (p
18 R. Squeri et al.
Table 3 - Multivariate analysis: covariate that contribute significantly to the predictability of the individual vaccina-
tions
95% CI for OR
β* Pvalue OR
Lower - Upper
Poliomyelitis age 0.041 0.016 1.042 1.008 - 1.078
HBV age -0.096 0.001 0.908 0.886 – 0.931
DT age -0.047 0.001 0.954 0.930 – 0.978
Pertussis sexM -0.600 0.003 0.549 0.368 – 0.818
age -0.035 0.001 0.965 0.948 – 0.983
Measles area -0.290 0.020 0.749 0.586 – 0.956
sexM -0.907 0.001 0.404 0.267 – 0.609
age -0.044 0.001 0.957 0.940 – 0.974
category 0.298 0.011 1.348 1.072 – 1.694
Rubella età -0.055 0.001 0.947 0.930 – 0.964
category 0.249 0.026 1.282 1.030 – 1.597
Chickenpox area -0.284 0.025 0.753 0.588 – 0.964
sexM -0.581 0.006 0.559 0.371 – 0.844
age -0.019 0.045 0.981 0.963 – 1.000
category 0.370 0.002 1.447 1.147 – 1.826
Mumps area -0.281 0.029 0.755 0.587 – 0.971
sexM -0.686 0.001 0.503 0.331 – 0.765
age -0.059 0.001 0.942 0.925 – 0.961
category 0.312 0.009 1.366 1.081 – 1.726
H. influenzae area -0.706 0.030 0.494 0.261 – 0.934
Flu sexM -0.749 0.001 0.473 0.313 – 0.716
age 0.038 0.001 1.039 1.018 – 1.060
category -0.257 0.033 0.773 0.611 – 0.979
Meningococcus C sexM -1.039 0.008 0.354 0.164 – 0.764
age -0.101 0.001 0.904 0.870 – 0.939
Meningococcus B Age -0.083 0.001 0.920 0.881 – 0.961
Pneumococcus SexM -1.135 0.006 0.238 0.086 – 0.656
Age -0.041 0.052 0.959 0.920 – 1.000
HAV sexM -1.396 0.001 0.248 0.140 – 0.437
category 0.412 0.013 1.509 1.091 – 2.088
H. zoster sexM -1.446 0.045 0.235 0.057 – 0.968
*See b value for results interpretation
Age (always with negative β coefficients the variable age increases, the more the
except for polio and influenza) was among probability that the event (vaccination) will
the variables with the greatest weight in occur, decreases.
the choice of vaccination. Therefore, in Sex was the second regressor studied
polio vaccination (positive β), the more the with greater weight in the probability of
variable age increases, the more it is likely vaccination (9/15 vaccinations) and we
that the event will occur (vaccination); obtained a greater tendency to vaccination
on the other hand, in the vaccination by the female sex for each vaccine.
against Hepatitis B (β negative), the more The qualification was also a regressor ofVaccine coverage in HCWs in a University Hospital 19
predicting the vaccination (6/15 vaccinations) the lowest probability to the physicians of
and, finally, the area had its own weight in the service area, first category.
determining the probability of vaccination. In the case of varicella we could establish
It was noted, in particular, that the greatest that for the clinical area, for those starting
compliance was found for the clinical area work in the category of medical managers
and for the physicians. In addition, it was (doctors in training and structured doctors)
noted from Table 6 that the models were we found a chance of getting vaccinated
globally significant (all four regressors) for equal to 66.55% for females and 52.77% for
immunizations of measles, chickenpox and males. In the second category the probability
mumps only. was 74.23% for females and 61.70% for
We obtained from the analysis of the males. For the last qualification examined,
β coefficients of the logistic model, and we found the highest probability of being
using the relative algorithm the vaccination vaccinated at the beginning of the career
probabilities as follows. equal to 80.66% for females and 69.94%
In the case of measles we could establish for males.
that for the clinical area for physicians Moving from the clinical area to the
(doctors in training and structured doctors) surgical area with the same age and
at the beginning of work we obtained qualification characteristics, the likelihood
a chance of getting vaccinated equal to of vaccination decreases, with 59.97%
90.41% for females and 79.20% for males. for females and 45.59% for males for
For nurses the probability was 92.70% for physicians. In the nursing category, on the
females and 83.69% for males. For the last other hand, the probability was equal to
qualification examined we had the highest 68.44% for females and 54.81% for males.
probability of vaccinating at the start of For the last qualification examined we had
the career equal to 94.48% for females and the highest probability of being vaccinated
87.36% for males. at the start of the career equal to 75.84% for
For the surgical area, for the first category females and 63.72% for males.
we found a probability of vaccination of Evaluating the service area, the probability
81.09% for females and 68.35% for males. was - for physicians - 52.99% for females
For nurses, on the other hand, the probability and 38.68% for males. For nurses, on the
was equal to 85.42% for females and other hand, the probability was 62.01%
74.69% for males. For the last qualification for females and 47.72% for males. For the
examined, we had a probability of 91.38% last qualification examined we saw that the
for females and 84.22% for males. chance to get vaccinated at the beginning of
If we considered the service area, the the career is equal to 70.27% for females and
probability in the first category was 76.41% 56.93% for males.
for females and 61.99% for males. For For chickenpox vaccine, we could
nurses, the probability was equal to 81.56% observe that the highest probability of being
for females and 69.02% for males. For the vaccinated is up to the female HCWs of the
last qualification examined we found a third category examined, at the beginning of
chance to get vaccinated equal to 85.80% the working activity belonging to the clinical
for females and 75.27% for males. area; and the lowest probability to the male
So, for measles, we could observe that physicians of the surgical area.
the highest probability of being vaccinated In the case of mumps we could establish
is up to the HCWs of the third category of that for the clinical area for the subjects
females, at the beginning of the working at the beginning of work in the category
activity, belonging to the surgical area; and of medical managers (doctors in training20 R. Squeri et al.
and structured doctors) we found a chance Discussion and conclusions
of getting vaccinated equal to 85.03%
for females and to 74.10% for males. In Analysis of the data revealed vaccination
the nursing category the probability was coverage to fall below the level to ensure
88.59% for females and 79.63% for males. herd immunity. In particular, the rates of
For the last qualification examined we had vaccinated HCWs for polio, hepatitis B,
a probability of vaccinating at the start of tetanus and diphtheria ranged between 60
the career equal to 91.38% for females and and 80%, while for measles, mumps, rubella,
84.22% for males. pertussis, chickenpox and tuberculosis
Moving from the clinical area to the the rate was 20-30%; lower vaccination
surgical area with the same age and coverage was found for some recently
qualification characteristics, the probability introduced vaccinations not specifically
of vaccination decreases for doctors, with recommended yet for HCWs. However,
81.09% for females and 68.35% for males. many HCWs were unable to recall their
In the nursing category, on the other hand, immunization status (Fig. 1), confirming
the probability was equal to 85.42% for national and international data literature (2,
females and 74.69% for males. For the 7, 12). HCWs are at high risk of exposure to
last qualification examined, we had the hazardous biological agents and the WHO
chance to get vaccinated at the career start estimates that approximately 59 million
of 91.38% for females and 84.22% for HCWs are potentially exposed to these on a
males. daily basis worldwide (13). It is well-known
For the service area, the probability that susceptible HCWs were at greater risk
was equal in the first category for females of both acquiring and spreading serious
to 76.41% and for males to 61.99%. For infectious diseases to vulnerable patients,
nurses the probability was equal to 81.56% their colleagues and their family and friends.
for females and 69.02% for males. For the This was of particular concern, given the
last qualification examined we had that the recently reported nosocomial outbreaks
chance to get vaccinated at the beginning of (13-18).
the career is equal to 85.80% for females and In this study, in line with the findings
75.27% for males. of other national and international studies,
For this vaccine we obtained that the vaccination coverage rates were acceptable
highest probability of being vaccinated only for some diseases, but still sub-optimal.
belongs to the health care workers of the Vaccination coverage for influenza fell far
third category of females at the beginning short of the 75% target set for 2015 contained
of the working activity belonging to the in the EU Council recommendation of
surgical area and the lowest probability for December 2009 (2009/1019/EU). Protection
the doctors of the service area. against exanthematous diseases was totally
In conclusion, considering the three inadequate to prevent disease transmission
vaccinations analyzed that have all four among susceptible HCWs and nosocomial
globally representative irritants, we could outbreaks. Our findings revealed that in
observe that the highest probability of the majority of cases physicians have
vaccination belongs to the female health care higher rates of vaccination compared to
workers at the beginning of work belonging other HCWs, especially those working in
to the clinical area for measles vaccination. the clinical area, as also reported in other
We obtained the lowest probability of studies (7, 12, 18, 19). Older workers
vaccination for male physicians of services were found to have a higher uptake for the
area for chickenpox. influenza vaccine, while in younger HCWsVaccine coverage in HCWs in a University Hospital 21
vaccination coverage was higher for hepatitis Protection against infectious diseases
B, measles, mumps, rubella and varicella, in requires both economic and human resources.
line with the literature (7, 12, 18, 19). Investment in training healthcare staff
Higher coverage was observed for was therefore important as the social and
females, confirming the literature: in fact, economic cost of non-protection may be
higher rates are due to prevention of the risks higher.
correlated with some infections in pregnant We must remember that these HCWs
women (for example rubella, HBV, measles, are also potentially able to influence patient
varicella, influenza and pertussis, etc (2). vaccination uptake (1, 19). Despite the
Also, highest coverage rates were found availability of effective vaccines, some
in pediatricians, as reported in international vaccine preventable diseases, such as
literature; in fact, in general, we could measles, had recently spread in Italy
observe in them higher coverage and attitude and the higher number of unvaccinated
towards vaccines; furthermore, pediatricians immigrants might further increase the spread
had higher coverage for measles, mumps, of infectious diseases (20-25).
rubella, chickenpox and meningococcus Vaccines and certain practices, like
C, perhaps because they come into contact handwashing, are fundamental and should be
with children that were more at risk of these considered compulsory to prevent dangerous
infectious diseases (6, 18). outbreaks of infection (23-27).
Another interesting issue from our In this light, novel strategies to address
study is the high percentage of HCWs “vaccine hesitancy” (i.e. promotion of
who declared “do not recall” when asked vaccines via social networks and mass media,
whether they were vaccinated or not, and training for HCWs, provision of vaccines in
this probably reflects a lack of confidence the workplace) should be adopted to improve
in immunization. HCWs should understand vaccination rates among HCWs (28).
that all vaccines are safe and useful; they The recent introduction in Italy of the law
should regard vaccinations as both a right 119/2017 has led to an increase in vaccine
and a duty to protect themselves and their coverage. Nevertheless, the enforce of this
patients. law was still controversial and subject of
A limitations of the study was that the debate. In our opinion, this could cause
HCWs self-report the vaccinations they vaccination coverage to fall down again,
received, so the older age groups may not particularly given the already growing
recall or HCWs might tend to declare that vaccination hesitancy even among expectant
they “do not remember” to avoid incurring mothers (29-31).
legal action; we didn’t investigated the Therefore urgent measures are needed
reason of such a lack of compliance. to achieve satisfactory coverage. However,
Our results confirm that further efforts are in view of the low coverage rates detected
required in Italy both to heighten awareness there is still undoubtedly a long way to go
among HCWs and to guarantee the early (7, 18, 19, 28, 29, 32).
recognition and prompt immunization of Steps have been taken in some regions
susceptible professionals under Healthcare in Italy, which have introduced mandatory
Surveillance Programs. Raising awareness immunization policies to tackle the low
about the importance of vaccination vaccination coverage among HCWs (33-34).
among HCWs and studies on prevalence However, other measures were necessary to
to counteract “vaccine hesitancy” were convince all HCWs (especially physicians)
included in the main goals of the SAGE that vaccination is a duty entailed by their
working group (1). profession. Only in this way they could22 R. Squeri et al.
be the proponents of a real change in the vaccinazione antifluenzale, nelle classi di età avanzate,
general population attitude. Finally, future mentre per tutte le altre vaccinazioni per i giovani.
Conclusioni. Dall’analisi dei dati emerge una mancata
physicians and nurses must be considered attenzione alle vaccinazioni da parte degli operatori sa-
a priority target group for campaigns nitari e la necessità di misure tese all’incremento delle
promoting vaccination, not only due to their coperture vaccinali, onde evitare che gli stessi diventino
work in the hospital, but especially as part of fonte di pericolose epidemie.
a future vision of creating a new generation
of immunized (and immunizing!) HCWs.
References
1. Report of the Sage Working group on vaccine
Riassunto
hesitancy. 2014. Available on: http://www.
Valutazione delle coperture vaccinali negli operatori who.int/immunization/sage/meetings/2014/
sanitari di un ospedale universitario del Sud Italia october/1_Report_WORKING_GROUP_vac-
cine_hesitancy_final.pdf [Last accessed: 2019,
Introduzione. Negli operatori sanitari un adeguato Mar 15].
intervento di immunizzazione è fondamentale per la 2. Karafillakis E, Dinca I, Apfel F, et al. Vaccine
prevenzione e il controllo delle infezioni, con ricadute hesitancy among healthcare workers in Europe:
non soltanto sullo stesso operatore, ma soprattutto nei A qualitative study. Vaccine 2016; 34(41): 5013-
confronti dei pazienti, ai quali potrebbe trasmettere l’in- 20. doi: 10.1016/j.vaccine.2016.08.029. 2016
fezione determinando gravi danni e/o morte. Purtroppo, Aug 26.
a tutt’oggi, nonostante la presenza di linee guida inter- 3. Andre FE, Booy R, Bock HL, et al. Vaccination
nazionali e nazionali (DL 119/2017) le coperture vacci-
greatly reduces disease, disability, death and
nali si mantengono basse, anche a causa del fenomeno
inequity worldwide. Bull World Health Organ
della “vaccine hesitancy” diffuso tra gli stessi operatori
sanitari. Alla luce di quanto sopra, l’obiettivo del nostro
2008; 86(2): 140-6.
studio è stato quello di indagare la copertura vaccinale 4. Dubé E, Laberge C, Guay M, Bramadat P, Roy
degli operatori sanitari di tutte le unità operative presenti R, Bettinger JA. Vaccine hesitancy. An overview.
nel nostro ospedale e di valutare le differenze tra sesso, Hum Vaccin Immunother 2013; 9(8): 1763-73.
età, profilo professionale e area di lavoro. doi: 10.4161/hv.24657.
Materiali e metodi. È stato condotto da Marzo a 5. Signorelli C, Odone A, Cella P, Iannazzo S,
Giugno 2018 uno studio al fine indagare le coperture D’Ancona F, Guerra R. Infant immunization
vaccinali degli operatori sanitari dell’Azienda Ospeda- coverage in Italy (2000-2016). Ann Ist Su-
liera-Universitaria “G. Martino” di Messina; la raccolta per Sanita 2017; 53(3): 231-7. doi: 10.4415/
dati è stata effettuata tramite la somministrazione di un ANN_17_03_09.
questionario cartaceo da autocompilare basato sull’Al- 6. Squeri R, Genovese C, Trimarchi G, Palamara
legato 3 della Circolare 25233 del 18 agosto 2017. È MAR, La Fauci V. An evaluation of attitude
stata indagata la presenza di differenze statisticamente toward vaccines among healthcare workers
significative nelle coperture vaccinali tra medici e pedia- of a University Hospital in Southern Italy.
tri e tra classi decennali di età, attraverso il metodo chi Ann Ig 2017; 29(6): 595-606. doi:10.7416/
quadrato. Inoltre, per ogni vaccinazione, è stata utilizzata ai.2017.2188.
una regressione logistica considerando la variabile vac-
7. Yaqub O, Castle-Clarke S, Sevdalis N, Chataway
cinazione e le seguenti covariate: tipo di unità operativa,
J. Attitudes to vaccination: a critical review.
sesso, età e area, verificando il peso di ognuna al fine di
prevedere la probabilità di vaccinazione.
Social Sci Med 2014; 112: 1-11. https://doi.
org/10.1016/j.socscimed.2014.04.018
Risultati. È stato analizzato un campione di 822
8. Doebbeling BN, Li N, Wenzel RP. An outbreak
operatori sanitari (di cui 324 maschi e 498 femmine
of hepatitis A among health care workers: risk
con età pari a 49,5±10,5 DS). Il campione era composto
da medici (36%) infermieri (21%) e da altre categorie factors for transmission. Am J Public Health
professionali (43%). Dall’analisi dei dati emergono 1993; 83(12):1679-84.
coperture vaccinali al di sotto dell’obiettivo richiesto 9. Hiller U, Mankertz A, Köneke N, Wicker S. Hos-
per garantire la herd immunity, con maggiori coperture pital outbreak of measles - Evaluation and costs
nelle femmine, nei medici e nell’area clinica; e, per la of 10 occupational cases among healthcare work-Vaccine coverage in HCWs in a University Hospital 23
er in Germany, February to March 2017. Vaccine anti-rubella virus antibodies among pregnant
2019 Mar 5. pii: S0264-410X(19)30275-0. doi: women in southern Italy. Int J Gynaecol
10.1016/j.vaccine.2019.02.068. Obstet 2012; 116(3): 211-3. doi: 10.1016/j.
10. Hosmer DW, Lemeshow S, Sturdivant RX. ijgo.2011.10.029.
Applied logistic regression. 3rd ed. New York, 22. Ferrera G, Squeri R, Genovese C. The evolution
USA: John Wiley and Sons, 2013. of vaccines for early childhood: the MMRV.
11. The R Project for Statistical Computing), version Ann Ig 2018; 30(4 Suppl 1): 33-7. doi: 10.7416/
3.5.2. ai.2018.2232.
12. World Health Organization (WHO). Occupa- 23. Sindoni D, La Fauci V, Squeri R, et al. Compari-
tional health. Health workers. Health worker son between a conventional subunit vaccine and
occupational health. Available on: http://www. the MF59-adjuvanted subunit influenza vaccine
who.int/occupational_health/topics/hcworkers/ in the elderly: an evaluation of the safety, toler-
en/. [Last accessed: 2019, Mar 15]. ability and immunogenicity. J Prev Med Hyg
13. American College of Obstetricians and Gy- 2009; 50(2): 121-6.
necologists’ Committee on Gynecological 24. Palamara MA, Visalli G, Picerno I, et al. Measles
Practice. Committee opinion No. 655: Hepatitis outbreak from February to August 2017 in Mes-
B, Hepatitis C, and human immunodeficiency sina, Italy. J Prev Med Hyg 2018; 59(1): E8-E13.
virus infections in obstetrician-gynecologists. doi: 10.15167/2421-4248/jpmh2018.59.1.853.
Obstet Gynecol 2016; 127: e70-4. http://dx.doi. eCollection 2018 Mar.
org/10.1097/AOG.0000000000001315. 25. Weinberg GA, Szilagyi PG. Vaccine Epidemiolo-
14. McCubbin JH, Smith JS. Rubella in a practic- gy: Efficacy, Effectiveness, and the Translational
ing obstetrician: a preventable problem. Am J Research Roadmap. J Infect Dis 2010; 201(11):
Obstet Gynecol 1980; 136: 1087. http://dx.doi. 1607-10. https://doi.org/10.1086/652404.
org/10.1016/0002-9378(80)90655-9. 26. Squeri R, Genovese C, Palamara MA, Trimarchi
15. Tsagris V, Nika A, Kyriakou D, et al. Influenza G, La Fauci V. “Clean care is safer care”: correct
A/H1N1/2009 outbreak in a neonatal intensive handwashing in the prevention of healthcare as-
care unit. J Hosp Infect 2012; 81: 36-40. http:// sociated infections. Ann Ig 2016; 28(6): 409-15.
dx.doi.org/10.1016/j.jhin.2012.02.009. doi: 10.7416/ai.2016.2123.
16. Galanakis E, Jansen A, Lopalco PL, Giese- 27. Squeri R, Riso R, Facciolà A, et al. Management
cke J. Ethics of mandatory vaccination for of two influenza vaccination campaign in health
healthcare workers. Euro Surveill 2013; 18: care workers of a university hospital in the south
20627. http://dx.doi.org/10.2807/1560-7917. Italy. Ann Ig 2017; 29(3): 223-31. doi: 10.7416/
ES2013.18.45.20627. ai.2017.2150.
17. Prato R, Tafuri S, Fortunato F, Martinelli D. 28. Gualano MR, Bert F, Voglino G, et al. Atti-
Vaccination in healthcare workers: an Italian tudes towards compulsory vaccination in Italy:
perspective. Expert Rev Vaccines 2010; 9: 277- Results from the NAVIDAD multicentre study.
83. http://dx.doi.org/10.1586/erv.10.11. Vaccine 2018; 36(23): 3368-74. doi: 10.1016/j.
18. Fortunato F, Tafuri S, Cozza V, Martinelli D, vaccine.2018.04.029.
Prato R. Low vaccination coverage among Ita- 29. Lo Giudice D, Cannavò G, Capua A, et al. Elimi-
lian healthcare workers in 2013. Contributing to nating congenital rubella: a seroepidemiological
the voluntary vs. mandatory vaccination debate. study on women of childbearing age and MMR
Hum Vaccin Immunother 2015; 11(1): 133-9. vaccine coverage in newborns. J Prev Med Hyg
doi: 10.4161/hv.34415. 2009; 50(4): 236-40.
19. EpiCentro. Report n° 37 January 2018. Avaible 30. Gabutti G, Bergamini M, Bonanni P, Guido M,
on: http://www.epicentro.iss.it/problemi/morbil- Fenoglio D, Giammanco A, Sindoni L, Zotti
lo/. [Last accessed: 2018, Oct 29]. C, Boddi V, Bamfi F, Severini R, Bechini A,
20. Castelli F, Sulis G. Review. Migration and Boccalini S, Crovari P; Collaborative Group for
infectious diseases. Clin Microbiol Infect the Study of Pertussis. Assessment of humoral
2017; 23(5): 283-9. https://doi.org/10.1016/j. and cell-mediated immunity against Bordetella
cmi.2017.03.012. pertussis in adolescent, adult, and senior subjects
21. Calimeri S, Capua A, La Fauci V, Squeri R, in Italy. Epidemiol Infect 2008; 136(11): 1576-
Grillo OC, Lo Giudice D. Prevalence of serum 84. doi: 10.1017/S0950268807000192.24 R. Squeri et al.
31. La Fauci V, Riso R, Facciolà A, et al. Response nitario. Linee di indirizzo per la prevenzione
to anti-HBV vaccine and 10-year follow-up of delle principali patologie trasmesse per via
antibody levels in healthcare workers. Public ematica (HBV, HCV, HIV) e per via aerea
Health 2016; 139: 198-202. doi: 10.1016/j. (tubercolosi, morbillo, parotite, rosolia e vari-
puhe.2016.08.007. cella), indicazioni per l’idoneità dell’operatore
32. Legge regionale “Disposizioni per l’esecuzione sanitario.
degli obblighi di vaccinazione degli operatori 34. Determina DG No 613 del 26/10/17. Regione
sanitari”. Available on: https://www.vaccinars- Marche. Le vaccinazioni negli operatori sanitari
inpuglia.org/assets/uploads/files/213/legge- e la prevenzione delle infezioni correlate all’as-
puglia-obbligo-op-san.pdf [Last accessed: 2019, sistenza. Available on: https://www.ospedalesi-
Mar 15]. curo.eu/attachments/article/542/ASUR-Marche-
33. Delibera G.R. Emilia Romagna No 351 del 619DG.pdf [Last accessed: 2019, Mar 15].
12/3/2018. Rischio biologico in ambiente sa-
Corresponding author: Raffaele Squeri, PhD, Department of Biomedical Sciences and Morphological and Functional
Images, University of Messina, Via Consolare Valeria, 98125 Messina, Italy
e-mail: squeri@unime.itYou can also read