Hereditary Cancer Genetics: What You Need To Know in 2018 - Larry Geier, MD, MBA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hereditary Cancer Genetics:
What You Need To Know in 2018
Larry Geier, MD, MBA
Medical Oncology and Cancer Risk Management
TGW Cancer Genetics
May, 2018
drgeiergenetics@gmail.com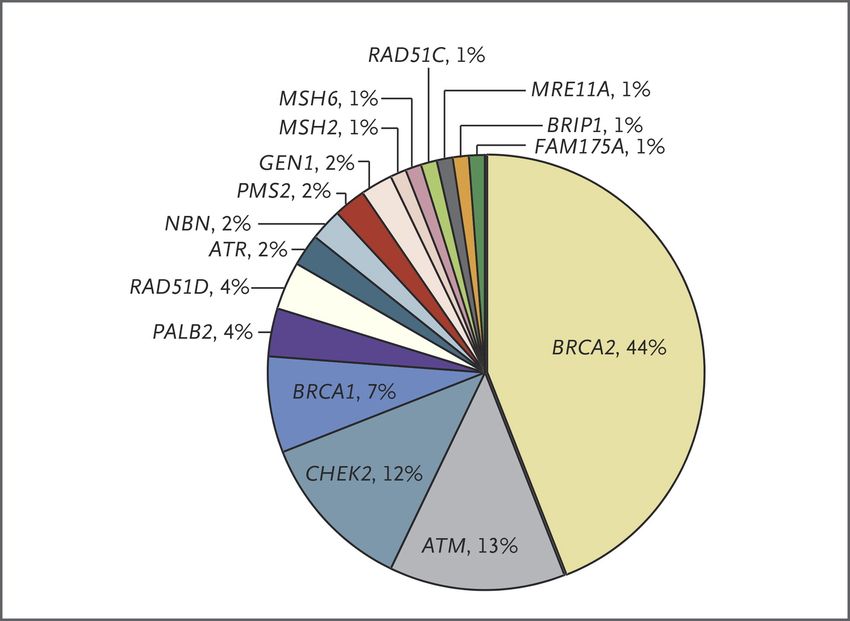
Disclosure Speaker Bureau, Myriad Genetic Labs
Questions For Today • Why should we care about hereditary cancer? • How do we recognize and evaluate suspicious families? • What is PARP, and why (and in whom?) would we want to inhibit it? • What is all the buzz about hereditary prostate cancer? • How can we be more effective at diagnosing Lynch syndrome (and what in the world is a “microsatellite,” and why do we care if it is “unstable?”)
Comprehensive Quality Cancer Care
Elements
Genetics and Diagnostics
Risk Management
Survivorship Surgery
Clinical Radiation
Research
Drug TherapyKansas City Cancer Center*
Genetic Testing Results by Year
*27 Med Onc TOTAL PTS TOTAL PTS
8 Rad Onc
YEAR
TESTED POSITIVE
2004 28 7
2005 69 15
2006 48 10
5Kansas City Cancer Center
(Circa 2006)
• At KCCC, this became a quality of care issue, as we had
been failing our patients and watching them develop
second cancers that could have been prevented
• In 2007, KCCC initiated a new effort to identify and test
patients who met guidelines for genetic testing:
• Better cancer family histories
• More attention to age and cancer phenotype
• Expedited in-house testing at the time of analysis
6Kansas City Cancer Center*
Genetic Testing Results by Year
*27 Med Onc TOTAL PTS TOTAL PTS
8 Rad Onc
YEAR
TESTED POSITIVE
2004 28 7
2005 69 15
New focus on 2006 48 10
cancer genetics
and risk mgmt 2007 296 45
2008 244 40
2009 332 41
2010 380 49
7Our Collective Report Card
• DNA testing for BRCA and Lynch syndrome has now been
clinically available for more than 20 years
• We have comprehensive guidelines on who should be tested
• It is estimated that fewer than 15% of all BRCA mutation
carriers have been found
• Similarly, fewer than 5% of all Lynch carriers have been found
(Cross et al, Clin Med Res 2012; Singh et al, Clin Gastro Hep 2010)My Track Record
• 345 patients with
pathogenic mutations
• Over 30% were either
cancer survivors or
never had cancerRelatively Common
Hereditary Cancer Syndromes
• Hereditary Breast/Ovary Syndrome (BRCA genes)
• Breast, ovary, prostate, melanoma, pancreas
• Lynch Syndrome (“mismatch repair” genes)
• Colon, uterus, ovary, stomach, pancreas, others
• Colon polyposis syndromes (APC, MUTYH genes)
• Colon, upper GI, thyroid, othersBRCA And Lifetime Cancer Risks:
Female (Approximate)
CANCER BRCA1 BRCA2
Breast 80% 80%
Ovarian 40-50% 25%
Prostate NA NA
Pancreas Elevated 4-7%
Melanoma Unknown Elevated
(NCCN 2016)
11BRCA And Lifetime Cancer Risks:
Male (Approximate)
CANCER BRCA1 BRCA2
Breast 1-2% (15X) 7-8% (100X)
Ovarian NA NA
Prostate (Approximate Lifetime Cancer Risks
Associated with Lynch Syndrome*
• Colorectal 50-80%
• Endometrial 25-60%
• Ovary 4-24%
• Stomach 3-13%
• Urothelial 1-7%
• Biliary/Pancreas 1-6%
• Small intestine 3-6%
• CNS (GBM) 1-3%
• Breast, Prostate, Bladder (not yet quantified)
*(NCCN 2016 – risks vary according to the gene affected)Prevalence of Hereditary Cancer:
BRCA vs Lynch Syndrome
• Prevalence of BRCA mutations in U.S. ≈ 1 in 300
• Prevalence of BRCA in Ashkenazi Jews ≈ 1 in 40
• Prevalence also high in other types of Jews
• Prevalence of Lynch syndrome in U.S. ≈ 1 in 300
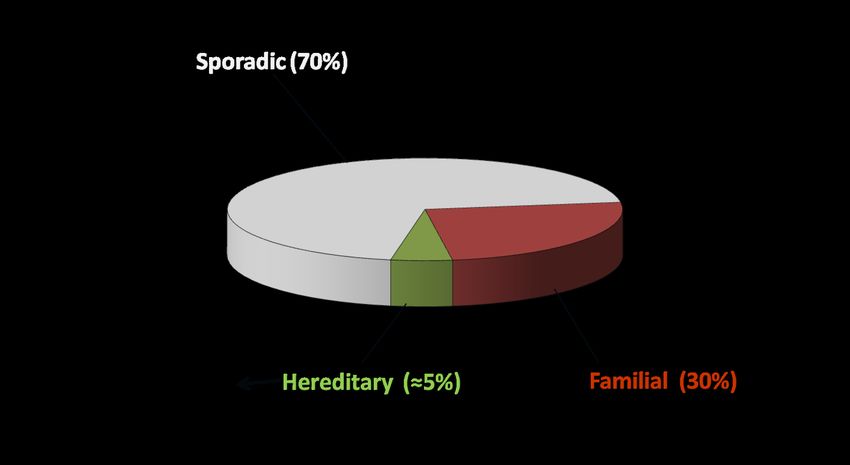
(Narod, et al. 2004; Anglian, et al. 2000; Roa, et al. 1996; Boland, et al. 2010)Familial vs Hereditary Cancer Risk
• Familial patterns are seen in several types of cancer
(e.g., breast, colon, prostate)
• Generally confer a modest increase in risk
• Not attributable to a known defect in a single gene
• Hereditary cancer indicates that cancer risk is attributable
to an inherited mutation that disrupts gene function
• Often a much higher relative risk compared to
average, and a tendency to occur at younger age
• The affected genes are typically DNA repair genes
15Categories of Breast Cancer Risk
70
60
% Risk of Breast Cancer
50
40 BRCA Mutation
30 Familial
Normal
20
10
0
30 40 50 60 70
Age
(Narod, personal communication, 2009)Hereditary Cancer Syndromes
Clinical Implications
• Prevention and high-risk management in carriers of
pathogenic mutations
• Breast Uterus
• Ovary Colorectal
• Others?
• Preventive surgery – eg, breast, uterus, ovary
• Chemoprevention – eg, tamoxifen, OCP, aspirin
• High-risk surveillance – eg, breast MRI, colonoscopy
17Hereditary Cancer Syndromes
Clinical Implications
Optimal management of the newly diagnosed cancer
• Overall prognosis
• Surgery options
• Chemotherapy options:
• PARP inhibitors in BRCA ovarian, breast cancer
• Neoadjuvant platinum in BRCA breast cancer
• Same drugs are promising in hereditary
prostate cancer
18Three Keys To Integrating
Cancer Genetics Into Your Practice
1) Finding the right people to test – more attention to
obtaining better cancer family histories
2) Testing the right genes to maximize the chance of
solving the family puzzle
3) Performing the test using the right lab methodology
to maximize the chance of getting the correct answer
19How Many Cancer Patients
Should Undergo Genetic Testing?
When current NCCN guidelines are applied to large groups of
cancer patients, the following approximate percentages of
patients will be appropriate for genetic testing:
Ovarian 100% NCCN 2008
Breast > 25% NCCN 2017
Colorectal > 25% NCCN 2015
Endometrial > 50% NCCN 2015
Prostate > 20% ? NCCN 2017
Zhang et al. Gynecol Oncol. 2011; Eisenbraun et al. Community Oncology, 2010;
Boland et al. Gastroenterology. 2010; Kerber et al. Familial Cancer, 2005;
Hampel et al. Cancer Res 2006; Lu et al. JCO, 2007; Pritchard et al, NEJM, 2016Hallmarks of Hereditary Cancer
• Family clustering of specific cancers among
siblings or across multiple generations
• Younger age at diagnosis compared to
non-hereditary cases of the same cancer
• Multiple cancers in the same person
• Specific phenotypes in some cancers, eg:
• Triple negative breast cancer (BRCA)
• Proximal mucinous colon cancer (Lynch)
• Higher-grade prostate cancer (BRCA)
21“Automatics” For BRCA Testing
Single indicators for DNA testing:
• Breast cancer by age 45 (invasive or DCIS)
• ANY epithelial ovarian cancer, regardless of age or family hx
• ANY male breast cancer
• Triple negative breast cancer by age 60
• Breast cancer in a Jewish woman
• First degree family members of any of the above
• Family history of BRCA cancers (3 cancers within 3 degrees)
(NCCN, 2017)
22Sherry
• 32 female with invasive ductal cancer, triple negative,
4 cm and rapidly growing
• Father’s side of family unknown
• No response to one cycle neoadjuvant AC
• Genetic testing at dx revealed BRCA1 mutation
• Neoadjuvant cisplatin induced pathologic CR at the
time of bilateral mastectomy
• Remains free of disease 11 years later
23“Automatics” For BRCA Testing
Single indicators for DNA testing:
• Breast cancer by age 45 (invasive or DCIS)
• ANY epithelial ovarian cancer, regardless of age or family hx
• ANY male breast cancer
• Triple negative breast cancer by age 60
• Breast cancer in a Jewish woman
• Metastatic HER2-negative breast cancer
• First degree family members of any of the above
• Family history of BRCA cancers (3 cancers within 3 degrees)
(NCCN, 2018)
24PARP Inhibitors For BRCA+ Cancers
• The BRCA genes are critical to the repair of double-strand DNA
breaks (homologous recombination)
• The cancers that result from germline BRCA mutations are
BRCA-deficient, and therefore can not efficiently repair these
DNA breaks
• These cells are therefore more dependent on alternate
mechanisms of DNA repair to survive
25PARP Inhibitors For BRCA+ Cancers
• The PARP enzymes are integral to one or more of these
“escape” mechanisms for DNA repair
• BRCA-deficient cancer cells are therefore potentially
vulnerable to inhibition of these PARP enzymes
• BRCA+ cancers of the ovary, breast, prostate, and pancreas
have been shown to be sensitive to these PARP inhibitors
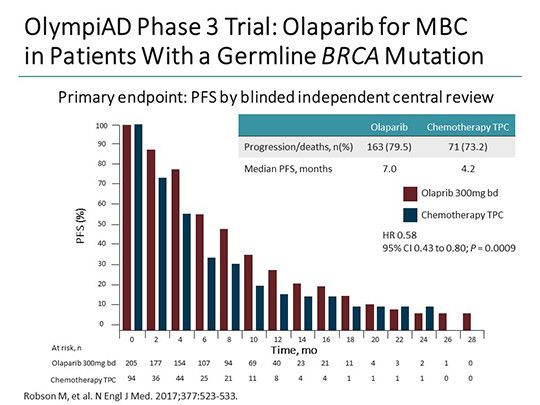
26The OlympiAD Trial
• 302 patients with germline BRCA mutations and metastatic
HER2-neg breast cancer, all previously treated with a taxane
and an anthracycline +/- hormonal therapy
• 2:1 randomization to receive either olaparib or one of 3 single
agent chemo regimens (capecitabine, eribulin, or vinorelbine)
• All patients confirmed BRCA-positive using the Myriad
BRACAnalysis CDx as a companion diagnostic
• Primary endpoint was progression-free survival
(Robson, et al NEJM, 2017)
27The OlympiAD Trial
• Median PFS was 7.0 months with olaparib vs 4.2 months with
single agent chemotx
• Response rate was 60% for olaparib and 29% with chemotx
• Based on this study, NCCN added to the BRCA guidelines that
all patients with HER2-neg metastatic breast cancer are
appropriate for germline BRCA testing
• BRACAnalysis CDX is now FDA-approved for this indication
(Robson, et al NEJM, 2017)
28PARP Inhibitors For BRCA+ Cancers
• PARP inhibitors are now FDA-approved for patients who carry
germline BRCA mutations and have one of the following:
• Ovarian (epithelial)
• Metastatic HER2-negative breast cancer
• Also effective in metastatic prostate cancer related to germline
mutations in BRCA or other DNA repair genes
• Appear to be effective in BRCA+ pancreas cancer
30Hereditary Prostate Cancer
• Hereditary prostate cancer is frequently more aggressive
biologically than sporadic prostate cancer, and this may
need to be factored into medical decision-making
• Some promising drug therapies for advanced prostate
cancer may only be effective in hereditary cases
• The patient may have substantial risk for other cancers,
and these risks must be actively managed
• The family may also be at risk for multiple kinds of cancer
31BRCA And Prostate Cancer Biology
• Retrospective European study of 2019 patients with prostate
cancer (18 BRCA1, 61 BRCA2, and 1940 non-carriers)
• Correlated mutation status with histology, stage, outcome
• BRCA mutations were more frequently associated with:
• Gleason score 8 or higher (p = .00003)
• T3/T4 stage (p = .003)
• Nodal involvement (p = .00005)
• Metastasis at diagnosis (p = .005)
• Cause-specific survival was significantly worse in BRCA
mutation carriers than in non-carriers (8.6 vs 15.7 years)
(Castro et al, JCO, 2013)
32Implications Of Inherited Mutations
On Prostate Cancer Management
• Active surveillance may not be appropriate
• EBRT may be associated with excessive radiotoxicity in
carriers of mutations in certain genes (TP53, ATM)
• EBRT may increase risk of second cancers in the radiated
field (ATM, rectal cancer in Lynch syndrome patients)
• Platinum and PARP inhibitors may be uniquely effective in
hereditary patients with advanced prostate cancer
(Castro et al, JCO, 2013)
33NCCN Guidelines For BRCA Testing
In Prostate Cancer (2017)
• Gleason score of 7 or higher (required)
PLUS
• ANY ONE of the following in the family (among relatives
within 3 degrees on the same side of the family):
• One relative with ovarian cancer (any age)
• One relative with breast cancer by age 50
• Two relatives with any combination of breast,
pancreas, or prostate (Gleason > 7) at any age
• Even more suspicious if Jewish or prostate cancer < 55
(NCCN V2.2017)
34NCCN Guidelines For BRCA Testing
In Prostate Cancer (2017)
Any male with metastatic prostate cancer,
regardless of age, family history, or
Gleason score
(NCCN 2017)
35Other Genes And Prostate Cancer
• Multicenter registry study of men with prostate cancer,
unselected for age, family history, or Gleason score
• Each underwent genetic testing with a panel of 20 genes
involved with DNA repair
• 11.8 % of 692 men with metastatic prostate cancer had
an inherited pathogenic mutation
• 5.3% of all men with metastatic prostate cancer
had a mutation in BRCA2
• ATM, CHEK2, BRCA1, Lynch genes, others
(Pritchard, NEJM, 2016)
36Inherited Pathogenic Mutations
And Metastatic Prostate Cancer
(Pritchard, NEJM, 2016)Other Genes And Prostate Cancer
• Multicenter registry study of men with prostate cancer,
unselected for age, family history, or Gleason score
• Localized prostate cancer – 499 patients
• 4.6% had a pathogenic mutation (P < 0.001)
(Pritchard, NEJM, 2016)
38David
• Prostate cancer (Gleason 3+4=7) diagnosed at age 60
• PSA 4.8, no adverse features
• No family history of prostate cancer
• Active surveillance was undertaken
76
Pancreas
62
No Cancers
68 66 63
Breast 44 Melanoma
45
62 60 56
64 Prostate
39David
• Prostate cancer (Gleason 3+4=7) diagnosed at age 60
• PSA 4.8, no adverse features
• No family history of prostate cancer
• Active surveillance was undertaken
76
Does he meet
NCCN criteria for Pancreas
testing? 62
No Cancers
68 66 63
Breast 44 Melanoma
45
62 60 56
64 Prostate
40David
2 years later:
• PSA was up to 9.5, but David remained asymptomatic
• Radical prostatectomy, now with positive pelvic
nodes (Gleason evolved to 4+4=8)
• PSA dropped to zero appropriately
41David
4 years later:
• PSA remained zero, but he developed low back pain,
and a bone scan was suggestive of metastatic disease
• Exam showed a right breast mass, which biopsy proved
to be invasive ductal cancer
• Mastectomy, spine radiation, and tamoxifen
• Still no consideration of genetic testing
42David – The Sister
Soon thereafter, his sister was diagnosed with
breast cancer, and she underwent genetic testing
76
Pancreas
62
No Cancers
72 70 67
Breast 44 Melanoma
45
66 64 60
68 Prostate 60
Breast 60
Breast 64
43David – The Sister
Genetic testing using a broad 28-gene
panel revealed a mutation in BRCA2
76
Pancreas
62
No Cancers
72 70 67
Breast 44 Melanoma
45
68 66 64
Prostate 60
+ 60
Breast 60
Breast 64
44David – The Rest
76
Pancreas
62
No Cancers
+ 72
+ 70 67
Breast 44 Melanoma
45
68 66 + 64
Prostate 60
+ 60
Breast 60
Breast 64
+ 40 + 36
45Approximate Lifetime Cancer Risks
Associated with Lynch Syndrome*
• Colorectal 50-80%
• Endometrial 25-60%
• Ovary 4-24%
• Stomach 3-13%
• Urothelial 1-7%
• Biliary/Pancreas 1-6%
• Small intestine 3-6%
• CNS (GBM) 1-3%
• Breast, Prostate, Bladder (not yet quantified)
*(NCCN 2016 – risks vary according to the gene affected)s.
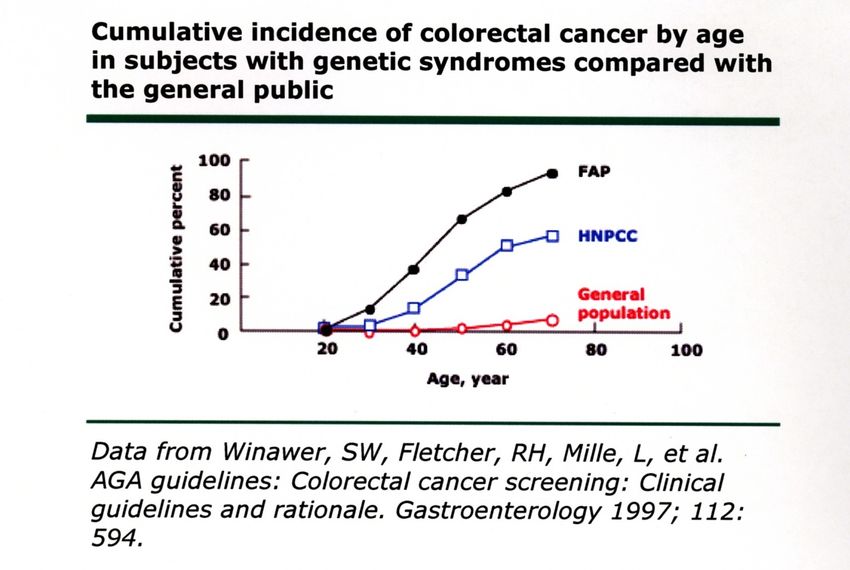
FAP
LYNCH
AVERAGEEpidemiology of Colorectal Cancer Lynch (3%) FAP (< 1%) MAP (< 1%) Others (? %) ≈8000 New Cases/Year
Lynch Syndrome
Accelerated Timeline For CRC
• Genomic instability in Lynch syndrome greatly accelerates
the timeline from colon polyp to CRC
• Instead of the usual 7-10 years, it may be only 1-3 years
• Beware of the colon cancer that seemed to come out of
nowhere, within 2-3 years of a normal colonoscopy
• This is not only the basis for the annual colonoscopy
recommendation, but also an important clue to underlying
Lynch syndromeColorectal Cancer Phenotype:
Sporadic Lynch
• Avg age 60-65 • Avg age 45-55
• 2/3 left-sided • 2/3 right-sided
• Variable histology • Mucinous, signet ring
• Slow evolution from • Rapid evolution from
polyp to cancer polyp to cancer
• Microsatellite • Microsatellite
instability 10-12% instability 90%“Red Flags” For Lynch Syndrome
• F - Any patient with a Lynch cancer and a suspicious family
history of other Lynch cancers (3 cancers within 3 degrees)
• A - ANY pt diagnosed with CRC or uterine cancer by age 50
• M - ANY pt with multiple Lynch cancers, regardless of age
• P - Any colon or uterine cancer with typical Lynch phenotype:
• Right-sided CRC (proximal to splenic flexure)
• Lynch histology features (any one): Mucinous, signet
ring, lymphocytic infiltrate
• Loss of expression of a mismatch repair protein by IHC“Pink Flags” For Lynch Syndrome
• Cancer of the ureter or renal pelvis (transitional)
• Adenocarcinoma of the small intestine
• Development of colorectal cancer less than three
years out from a clean colonoscopy
• Sebaceous skin tumors (adenomas, carcinomas)
• Muir-Torre syndromeDiagnostic Tools For Lynch Syndrome
Tumor Testing:
• Microsatellite Instability (MSI)
• Immunohistochemistry (IHC) for MMR proteins
• Useful for automatic screening of all CRC patients
at the pathology level
Germline DNA Testing:
• Direct DNA analysis of one or more of the five genes
• This is the only way to diagnose LS, and the only way
to track the mutation through the familyMicrosatellite Instability (MSI) • MSI is a functional test • Detects the failure of mismatch repair in the malignant clone compared to the normal tissue • Confusing nomenclature: abnormal reported as “MSI-High” • 10-12% of all CRC tumors are MSI-high • This test is NOT DIAGNOSTIC of Lynch syndrome, and is only 20% specific (ie, 80% have a different underlying cause which is somatic, not hereditary) • 90% sensitive for LS
Immunohistochemistry (IHC) • Performed on the cancer tissue, looking for the presence or absence of the four mismatch repair proteins in the tumor • Theoretically, the defective gene will not produce the corresponding MMR protein • An abnormal test is NOT DIAGNOSTIC of Lynch syndrome, particularly if the missing protein is MLH1 • Similar to MSI, IHC is 20% specific and 90% sensitive for LS, but the 10% it misses is not the same 10% that MSI misses – together the tests are about 97% sensitive • Useful for screening population groups with colon and endometrial cancer
BRAF V600E and MLH1 Inactivation • V600E is a somatic mutation in the BRAF gene that develops in the tumor of some patients with CRC • This mutation can indirectly inactivate the MLH1 gene, and thus lead to the tumor expressing microsatellite instability or loss of the MLH1 protein on IHC • This phenomenon occurs in 10-12% of all CRC’s, and can be associated with improved overall prognosis • If IHC shows loss of MLH1 in the absence of a strong family history of Lynch cancers, the next step is to do BRAF testing on the tumor
Germline DNA Testing • Performed on blood or saliva • Testing for inherited mutations in any of the five Lynch genes that would render that gene defective, and therefore unable to produce the corresponding MMR protein • This is the only way to confirm the diagnosis of LS, and the only way to track a mutation through the family
Screening For Lynch Syndrome:
The Pathology Approach
• If MSI or IHC is abnormal, further evaluation is warranted
depending on family history and the protein that is
missing:
• No family history with absent MLH1 leads to BRAF testing
• No family history with absence of a non-MLH1 protein
leads to DNA testing of the corresponding gene
• Suspicious family history will cause most clinicians to
proceed directly to full Lynch testingLynch Syndrome Algorithm:
The Universal Pathology Approach
ALL CRC And
Endometrial
Automatic
Cancer
Pathology
Patients
Screening:
IHC
LH1
M ) No
sent adic Absent rm
A b po r al
% s MSH2, MSH6,
BRAF (Colon) or (80 or PMS2
Hypermethylation
(Endometrial) Suspicious Family Cancer
History Analysis
Negative OK
DNA Testing
Unlikely to be
Positive
Lynch SyndromeNCCN Guidelines For Lynch Testing
• Personal history of CRC or endometrial cancer:
• by age 50
• at any age, plus a second Lynch cancer at any age
• at any age, plus
– One 1st or 2nd degree relative with any Lynch cancer by 50, or
– Two 1st or 2nd degree relatives with any Lynch cancer at any age
• At any age, with evidence of MMR deficiency by either
MSI or IHC testing of the tumor
• Personal history of any Lynch cancer and a > 5% probability of
having Lynch based on predictive computer model (eg, PREMM)NCCN Guidelines For Lynch Testing In Patients Who Don’t Have Cancer • First degree relative with CRC or endometrial cancer < 50 • First degree relative with CRC or endometrial cancer PLUS a second Lynch cancer, regardless of age • Two 1st or 2nd degree relatives with any Lynch cancer, with at least one cancer prior to age 50 • Three 1st or 2nd degree relatives with any Lynch cancer, regardless of age • > 5% probability of having Lynch syndrome based on one of the predictive computer models (PREMM5, others)
Impact of Broad Multi-Gene Panels • There is much more clinical overlap among the various syndromes than previously realized • Taken as a group, numerous clinical studies show that the traditional syndromic approach will miss more than one third of the pathogenic mutations found using broad multigene panels • Studies have also shown that disease-specific panels still miss 10-20% of clinically actionable mutations
Spectrum of Malignancies In
A Broad 28-Gene Panel
GENES Breast Ovary Colon Panc Prost Uterus Gastric Mel Other
BRCA1, BRCA2 X X X X X
TP53 X X X X X X X X X
PTEN X X X X
STK11 X X X X X X X
PALB2, ATM X X X
CDH1 X X X
CHEK2 X X X
BARD1, NBN X X
RAD51C, BRIP1 ? X
MLH1, MSH2, MSH6, PMS2, EPCAM ? X X X X X X X
APC, SMAD4, BMPR1A X X X X
MUTYH X X
POLD1, POLE, GREM1 X
RAD51D X ?
CDKN2A, CDK4 X X
63A Broad 28-Gene Panel And
Guidelines For Management
GENES Breast Ovary Colon Panc Prost Uterus Gastric Mel Other
BRCA1, BRCA2 X X X X X
TP53 X X X X X X X X X
PTEN X X X X
STK11 X X X X X X X
PALB2, ATM X X X
CDH1 X X X
CHEK2 X X X
BARD1, NBN X X
RAD51C, BRIP1 ? X
MLH1, MSH2, MSH6, PMS2, EPCAM ? X X X X X X X
APC, SMAD4, BMPR1A X X X X
MUTYH X X
POLD1, POLE, GREM1 X
RAD51D X ?
CDKN2A, CDK4 X X
64Janice
• 55-yr-old woman with ER+ invasive ductal cancer, 1.5 cm
• Family history:
• Mother ovarian ca 48
• Maternal aunt breast ca 57, colon ca 68
• Maternal uncle pancreas cancer 70
• Maternal great aunt uterine cancer 49Janice
Uterus 49
76
Ovary 48 Breast 57 Pancreas 70 78
Colon 68
52 59
Breast 55
66Janice
Hereditary syndromes to consider:
• BRCA (2 breast, 1 ovary, 1 pancreas)
• Lynch (1 colon, 1 uterus, 1 ovary, 1 pancreas)
• Cowden (2 breast, 1 uterus)Janice
• Hereditary syndromes to consider:
• BRCA (2 breast, 1 ovary, 1 pancreas)
• Lynch (1 colon, 1 uterus, 1 ovary, 1 pancreas)
• Cowden (2 breast, 1 uterus)
• 28-gene panel revealed a pathogenic mutation in MSH2Janice – The Rest
Uterus 49
Neg
76
Ovary 48 Breast 57 Pancreas 70 78
Colon 68
Neg 59
Neg 52 Breast 55
69Key Takeaway Points • Hereditary syndromes are more common than most realize, and this is now also true for hereditary prostate cancer • Underlying genetic trait affects not only future cancer risk, but also may affect optimal management of the cancer at hand
Key Takeaway Points • Hereditary forms of prostate cancer may be biologically aggressive, and this may be important in medical decision- making • Similar to hereditary breast and ovarian cancers, hereditary prostate cancer may be uniquely sensitive to the effects of PARP inhibitors and other drugs that may not be effective in non-hereditary cases
Key Takeaway Points • Lynch syndrome is terribly under-recognized, yet it is just as common as BRCA, has cancer risks just as high as BRCA, and the cancers are just as preventable as those in BRCA • Universal pathology screening of ALL colorectal and endometrial cancers with IHC for the four Lynch proteins is now considered standard of care, and should also be considered for survivors of these cancers
Key Takeaway Points • Puzzle-solving with a broad multigene panel is simple and straightforward, particularly for providers with little background in genetics. Single syndrome testing leaves too many pathogenic mutations undiagnosed • You should systematically screen your survivor and non- cancer population as well, particularly survivors of breast, colorectal, prostate, and endometrial cancers
Key Takeaway Points • 15% for BRCA and 5% for Lynch after 20 years is a statistic that should be embarrassing to providers, but is also potentially life-threatening to their patients • This is a quality of care issue – genetic evaluation of appropriate patients can no longer be optional • Every doctor, nurse, and other members of the healthcare team has a potential role to play in finding these patients, and helping to prevent the cancers that were destined to occur
Comprehensive Quality Cancer Care
Elements
Genetics and Diagnostics
Risk Management
Survivorship Surgery
Clinical Radiation
Research
Drug TherapyYou can also read