Hijab Pin Ingestions - American Academy of Pediatrics
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hijab Pin Ingestions
Dotan Yogev, MD,a Fadi Mahameed, MD,a Alex Gileles-Hillel, MD,b Peri Millman, MD,c Zev Davidovics, MD,c Saar Hashavya, MD,d
David Rekhtman, MD,d Michael Wilschanski, MD,c Yackov Berkun, MD,a Mordechai Slae, MDc
OBJECTIVES: To
characterize the clinical manifestations, outcomes, and complications of hijab pin abstract
ingestion in adolescents and to identify risk factors for a need for intervention.
retrospective review of patients ,25 years of age who presented to our emergency
METHODS: A
department because of hijab pin ingestion between 2007 and 2018. Comparison was
performed between impaled and nonimpaled pins.
RESULTS: We reviewed 1558 foreign-body ingestion cases. Of these, 208 (13.3%) patients
presented because of hijab pin ingestion, with a total of 225 ingested pins. The mean patient
age was 14.7 6 4.1 years, and 88% of patients were girls. Time from ingestion to presentation
was 24 6 49.5 hours. Most pins were located in the stomach (46.6%), and 18.6% of all pins
were impaled. Location in the stomach (odds ratio = 4.3 [95% confidence interval: 1.9–9.2];
P , .001) and abdominal tenderness on examination (odds ratio = 2.7 [95% confidence
interval: 1.3–5.6]; P = .007) were strong independent risk factors for an impaled pin. Time to
intervention was 22.9 hours, and 41 endoscopies were performed. One patient required
laparoscopic surgery. No complications were observed.
CONCLUSIONS: The hijab pin is an increasingly encountered foreign body in pediatric practice. Its
specific clinical features distinguish it from other sharp objects. A delayed interventional
approach in selected patients does not carry a higher risk of complications and results in
significantly fewer interventions compared to existing guidelines. These findings will help
guide pediatric specialists in this prevalent clinical scenario. Management recommendations
are proposed.
b
Pediatric Pulmonology and Sleep Unit and cDivisions of Pediatric Gastroenterology and dPediatric Emergency WHAT’S KNOWN ON THIS SUBJECT: Sharp foreign
Medicine, aDepartment of Pediatrics, Hadassah Hebrew University Medical Center, Mount Scopus Hospital, bodies are common and have been associated with
Jerusalem, Israel significant morbidity. Current guidelines generally
Dr Yogev conceptualized and designed the study, collected data and performed the data analysis, recommend removal of all sharp objects within reach
reviewed the literature, and drafted and revised the manuscript; Dr Mahameed collected data, of the endoscope. The hijab pin is an emerging sharp
performed the initial analysis, and revised the manuscript; Dr Gileles-Hillel contributed to the study foreign body in many Western countries.
design, performed the main data analysis, and revised the manuscript; Drs Millman, Davidovics,
Hashavya, and Rekhtman contributed to the study design, acquisition of data, interpretation of
WHAT THIS STUDY ADDS: Conservative management of
results, and revision of the manuscript; Dr Berkun conceptualized and designed the study, hijab pins reduces the endoscopy rate without
performed the initial data analysis, reviewed the literature, and revised the initial draft; Drs increasing the rate of complications. Abdominal
Wilschanski and Slae contributed to study design and interpretation and analysis of data and to tenderness may be a valuable clinical clue as to which
revision of the initial draft and final manuscript; and all authors approved the final manuscript as patients will benefit from endoscopic intervention.
submitted and agree to be accountable for all aspects of the work. Management recommendations are proposed and
DOI: https://doi.org/10.1542/peds.2019-3472 require future validation.
Accepted for publication Mar 16, 2020
Address correspondence to Mordechai Slae, MD, Division of Pediatric Gastroenterology, Hadassah
Hebrew University Medical Center, Mount Scopus Hospital, Jerusalem, Israel. E-mail: mord@
hadassah.org.il
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). To cite: Yogev D, Mahameed F, Gileles-Hillel A, et al. Hijab
Pin Ingestions. Pediatrics. 2020;145(6):e20193472
Copyright © 2020 by the American Academy of Pediatrics
Downloaded from www.aappublications.org/news by guest on November 8, 2021
PEDIATRICS Volume 145, number 6, June 2020:e20193472 ARTICLE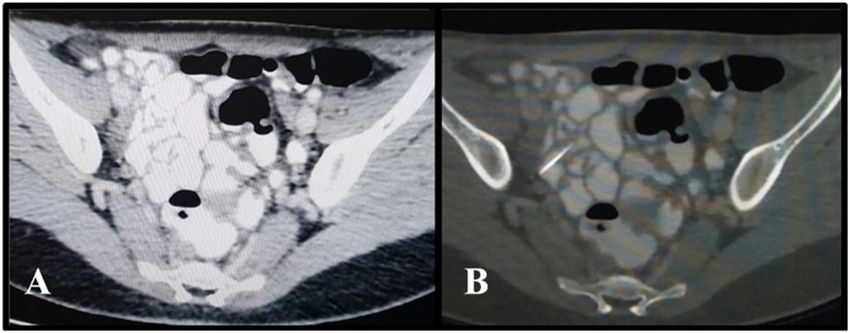
Foreign body ingestion is a common while doing so.7 Ingestion of hijab Pin location was determined by ED
medical problem in pediatric pins is a relatively frequent event, physicians’ notes and was confirmed
emergency departments (EDs) affecting otherwise healthy by reexamining plain films or
worldwide, with a peak incidence adolescent girls, and its prevalence endoscopy pictures. Pin location was
between the ages of 6 months and around the world is rising because of divided into 5 main groups: pharynx,
6 years. The most commonly ingested geopolitical and demographic esophagus, stomach, small bowel,
objects include small toys, coins, changes.8 However, data regarding and colon.
batteries, and magnets.1,2 In older the outcome and appropriate
We collected data regarding
children, this event is rare, occurring management of this specific subtype
management of cases and categorized
mainly in patients with psychiatric of sharp foreign body are limited. We
them according to the following
disorders and suicidal attempts. therefore sought to delineate the
categories: discharge, patient was
Although the majority of ingested clinical manifestations and medical
discharged after ED evaluation was
foreign bodies will pass outcome of children presenting with
completed; observation,
spontaneously, sharp and pointed hijab pin ingestion, to identify risk
patient was admitted for
objects may cause perforation of the factors associated with a need for
medical follow-up and serial
gastrointestinal (GI) tract and were intervention, and, specifically, to
abdominal films; and intervention,
associated with significant morbidity explore whether conservative
any endoscopic or surgical
(35%) and mortality (26%) in the management is associated with
intervention.
preendoscopic era.3 Therefore, complications.
current guidelines favor an urgent Statistical Analysis
interventional approach (,24 hours,
Demographic, clinical, and laboratory
following nil per os guidelines), METHODS variables were summarized by
recommending the removal of all
Participants and Data Collection standard descriptive statistics as
sharp objects within reach of the
means and SDs for continuous
endoscope and emergent (,2 hours We retrospectively reviewed the variables and as proportions for
regardless of nil per os status) Hadassah Hebrew University Medical categorical variables. Student’s t test
removal of sharp objects from Center database, searching for and the Mann–Whitney U test were
patients who are symptomatic.2,4 patients 0 to 25 years old who used to assess differences between
However, previous studies5,6 and presented because of foreign-body the groups for continuous variables.
clinical experience suggest that the ingestion (International Classification Proportional differences were
complication rate may be much lower, of Diseases, Ninth Revision code 938). assessed by using the x2 test,
raising the possibility of a more We selected hijab pin ingestion cases followed by Fisher’s exact test.
conservative, delayed interventional by manually reviewing these files and Correlations were assessed by
approach in selected patients. their abdominal radiographs. Data Pearson’s and Spearman’s coefficients
regarding demographics, signs and as appropriate. Logistic regression
The hijab pin, a 3.5-cm long sharp pin symptoms, anatomic location, medical
with a plastic ball head (Fig 1) used to analyses were used to build a model
management, and time from arrival to best for predicting the finding of an
fasten the hijab (head scarf), is procedure were collected.
frequently held between the lips impaled pin. The statistical analysis
Patients were excluded if no pin was was performed by using SPSS
during the process of wearing and found on chest and abdominal
adjusting the hijab and may be software 20.0 (IBM SPSS Statistics,
radiographs. IBM Corporation).
accidentally swallowed or aspirated
Time span from pin swallowing to The study was approved by the local
arrival (pin to door time) was Institutional Review Board
obtained from the ED files. When an Committee at Hadassah Medical
exact time frame was not Center, Jerusalem, in accordance with
documented, we interpreted the the Declaration of Helsinki (0542–17-
following terms according to our HMO).
estimate on the basis of our
knowledge of arrival times to our ED: Management Recommendations
on the same day, 6 hours; briefly, Over the past years, patients with
1 hour; a few hours earlier, 3 hours; hijab pin ingestion in our center have
FIGURE 1 and the day before, 24 hours. If time been managed according to the
A hijab pin ∼3.5 cm in length with a plastic was stated specifically, we used the clinical judgment of the attending GI
ball head. exact time lapse as mentioned. specialist, with some opting a more
Downloaded from www.aappublications.org/news by guest on November 8, 2021
2 YOGEV et al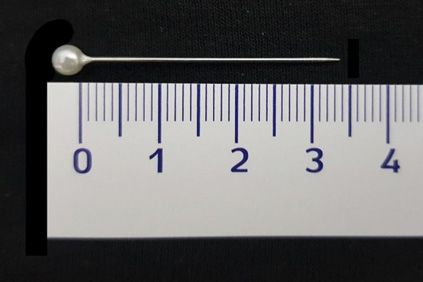
conservative, delayed interventional TABLE 1 Demographic and Clinical Characteristics of Patients With Hijab Pin Ingestion
approach on the basis of their clinical Characteristic Result
experience. To create a center-based Overall, N 208
policy, the data and analysis Age, y, mean 6 SD 14.7 6 4.1
performed for this article were Female sex, % 88
presented to our pediatric GI Pin to door time, h, mean 6 SD 24.0 6 49.5
specialists. They were then asked to Signs and symptoms, %
Abdominal pain without tenderness 12.9
generate specific management Abdominal pain plus tenderness 31.8
recommendations depicting the Asymptomatic 39.4
delayed interventional approach. Other symptoms 15.9
These recommendations were then Location on arrival
compared to previous foreign body Pharynx, impaled/total 1/4
Esophagus, impaled/total 1/3
algorithms2,4 to ensure similar Stomach, impaled/total 31/97
structure and time intervals and were Pin to door time, h, mean 6 SD 29.2 6 64.2
revised accordingly. We searched Endoscopies, n 35
PubMed to address any previous Time to endoscopy, h, mean 6 SD 23.7 6 27.1
publications on hijab pin ingestion Small bowel, impaled/total 7/71
Pin to door time, h, mean 6 SD 12.5 6 26.7
using the phrases hijab pin, turban Endoscopies, n 6
pin, hairpin, scarf pin, and straight Time to endoscopy, h, mean 6 SD 18 6 11.8
pin. All articles were reviewed in the Colon, impaled/total 2/33
process of generating the proposed
recommendations.
Clinical Characteristics impaled in the stomach (Fig 4). No
Ninety-three patients (44.7%) association was found between age,
complained of abdominal pain or sex, or any subjective symptoms and
RESULTS discomfort on presentation. Sixty-six an impaled pin. Location in the
patients (31.7%) had objective stomach (odds ratio = 4.3 [95%
Patients Demographics confidence interval: 1.9–9.2]; P ,
abdominal tenderness on physical
Between January 2007 and examination, and one presented with .001) and abdominal tenderness on
September 2018, ∼630 000 patients abdominal guarding. Eighty-two examination (odds ratio = 2.7 [95%
0 to 25 years of age presented to our patients (39.4%) were asymptomatic. confidence interval: 1.3–5.6]; P =
ED. Foreign-body ingestion accounted Other patients presented with various .007) were strong independent risk
for 1558 (0.2%) visits. Of these, 208 nonspecific symptoms such as throat factors for an impaled pin.
(13.3%) presented because of hijab pain or shortness of breath.
pin ingestion, with a total of 225 hijab Clinical Management and Outcomes
pins (12 patients swallowed multiple All patients underwent plain
Esophageal Pins
pins: a total of 29 pins). The average radiography of the chest and
abdomen. In 15 patients, an Three patients presented with a pin
patient age was 14.7 6 4.1 years, and
abdominal computed tomography in the esophagus. One was removed
88% of patients were girls. Analysis
(CT) scan was performed. In Table 1, endoscopically, and 2 spontaneously
of patients who ingested multiple
we present pin location on arrival to advanced through the GI tract with no
pins was performed according to the
the ED. The most common location complications.
site of the most proximal pin.
Demographic and clinical data are for a pin on arrival was in the
stomach (97 cases, 46.6%). Stomach Pins
shown in Table 1. In Fig 2, we present
the age distribution of the patients. Ninety-seven patients (46.6%)
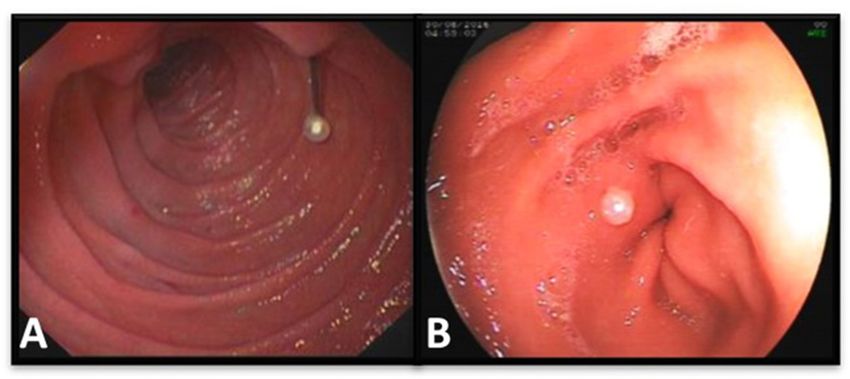
Impaled Hijab Pins presented with 105 pins documented
Extracted Hijab pins were similar to
previously reported pins: a sharp Because impaled pins (Fig 3) are the in the stomach by plain film on
metallic pin ∼3.5 cm in length with ones that have clinical consequence arrival. Three of these patients were
a small plastic ball head. and necessitate endoscopic or found to have an additional 5 pins in
surgical intervention, we examined the small bowel at the time of first
The average pin to door time was the clinical course of this group of imaging. The pin to door time was
24 6 49.5 hours (0.5–336 hours). patients separately. Forty-two of the 29.2 6 64.2 hours. Fourteen (14.4%)
Four patients had an unusually long 225 pins (18.6%) were found to be were discharged directly from the ED
delay to presentation (2–6 months) impaled and penetrating the mucosal and have no documented follow-up.
and were excluded from this analysis. wall, 31 of which (73.8%) were Of the 83 patients who were admitted
Downloaded from www.aappublications.org/news by guest on November 8, 2021
PEDIATRICS Volume 145, number 6, June 2020 3FIGURE 2
Hijab pin ingestion patient age distribution (years).
for observation, 48 were discharged impaled by endoscopy. The mean bowel. Two patients had an
after a follow-up radiograph proved door to endoscopy time was 23.7 6 additional pin in the colon at
propagation of the pin, and 35 27.1 hours (2–120 hours). presentation. The pin to door time
underwent an endoscopy after was 12.5 6 26.7 hours. Forty patients
a follow-up radiograph failed to Small-Bowel Pins were discharged, and 24 were
reveal spontaneous propagation. Seventy-one patients (34.1%) admitted and discharged after
Thirty-one pins were proven to be presented with 73 pins in the small a follow-up radiograph proved
propagation of the pin. Six patients
underwent an endoscopy, and in one
patient, the pin was removed in an
elective surgery. Door to endoscopy
time was 18 6 11.8 hours (6–39
hours).
Colon Pins
Thirty-three patients presented with
34 pins in the colon. The pin to door
time was 34.9 6 33.0 hours. Twenty-
three patients were discharged, and 9
were observed overnight. One patient
FIGURE 3 underwent a colonoscopy, and one
A, A hijab pin impaled in the duodenum. B, A pin impaled in the prepyloric area. The bead head of the patient required manual removal of
pin prevents transluminal migration of the pin and allows easier endoscopic retrieval. the pin under anesthesia.
Downloaded from www.aappublications.org/news by guest on November 8, 2021
4 YOGEV et alFIGURE 4
Impaled pins by location.
Complications and the pin was removed surgically DISCUSSION
Several complications or unique cases from the small bowel with no We present the largest cohort of hijab
were observed. Importantly, no complications. One patient presented pin ingestion cases to date.
complications were observed in with mild abdominal pain shortly Conservative management resulted in
patients while under observation or after ingestion. A CT scan revealed fewer endoscopies, when compared
awaiting an endoscopy. In one the pin penetrating the liver through to current guidelines, without an
previously described case, the duodenum. This pin was removed increase in the rate of complications.
a pharyngeal hijab pin penetrated the endoscopically with no complications. In our study, location of the pin in the
vertebral artery9 and was removed
surgically. In 4 cases, the hijab pin
was originally aspirated into the
airway (as proven by a radiograph)
and was later found in the GI tract.
One patient presented with signs and
symptoms of acute appendicitis but
had a normal appendix visualized on
a CT scan. When reviewing the CT
scan by using bone window, a metal
hijab pin could be differentiated from
the surrounding contrast material in
the proximal ileum (Fig 5). One
FIGURE 5
patient presented 2 months after pin A, A normal abdominal CT scan. B, Using bone window allowed us to differentiate the pin from the
ingestion with mild abdominal pain, surrounding contrast material.
Downloaded from www.aappublications.org/news by guest on November 8, 2021
PEDIATRICS Volume 145, number 6, June 2020 5stomach and abdominal tenderness ingestion cases with an 18% complications while under
on physical examination were strong incidence of hijab pins (32 pins). observation. This important finding
and independent risk factors for an Their approach, as recommended by emphasizes the safety of conservative
impaled pin necessitating endoscopic the guidelines, was that all sharp management of patients with hijab
intervention. On the basis of these objects within reach of the endoscope pin ingestion.
findings, specific management should be removed if possible, and as
According to current guidelines,
recommendations for hijab pin such, all stomach pins were removed
sharp objects beyond the ligament of
ingestion in adolescents are emergently. Therefore, although their
Treitz can be observed by serial
suggested below. study does suggest a low
radiographs, but this should be done
complication rate of hijab pin
Hijab pins were 13.3% of all foreign- in a hospital setting, and surgery is
cases, it does not represent the
body cases in our series, similar to recommended if no passage is
outcome of a conservative
rates reported in Muslim countries7 documented within 3 days.4 In our
management strategy.
but higher than rates reported in study, 50% of cases presented with
Western countries.10,11 A recent case In our study, 97 patients presented the pin already in the small bowel or
series from the United Kingdom with a pin in the stomach and were colon. Most of these patients were
suggests that the prevalence of hijab therefore candidates for emergent discharged, and in the 11-year period
pin ingestion in Western countries is endoscopic retrieval according to of the study, we noted no
changing.8 current guidelines. Adhering to our complications in this group and only
delayed interventional approach one patient who needed surgical
Management of straight pin ingestion reduced the number of endoscopies removal of an impaled pin. Although
is controversial, with to only 35, of which 31 patients did, authors of previous studies on hijab
recommendations spanning from in fact, carry an impaled pin. pins have not proposed specific
conservative follow-up to surgical Managing patients with small- management for small-bowel pins,7,12
intervention.4 Ingested straight pins bowel pins according to these we suggest inpatient observation for
may either pass unnoticeably or recommendations patients with abdominal tenderness
penetrate the mucosa, necessitating resulted in only 6 endoscopies, with and a pin beyond the stomach.
endoscopic or surgical removal and an impaled pin found in 5 of the Outpatient follow-up seems to be
potentially causing damage to patients. a safe option for patients who are
adjacent organs. Because of a cited asymptomatic.
complication rate as high as 35%, Although the signs and symptoms of
current guidelines recommend hijab pin ingestion are nonspecific The hijab pin is typically constructed
removal of any sharp foreign body and vary from anxiety and throat pain of a 3.5-cm long metal body with
within reach of the endoscope.3 to abdominal pain and true a small round plastic head. Accidental
Contrary to this high complication tenderness, they may be a valuable swallowing occurs almost universally
rate, only one patient in our study clue, focusing the clinician on the with the head facing inwards.
(0.048%) required surgery, and only patients who may indeed require Accordingly, Uçan et al15 found that in
one patient had proven intervention, and should not be all 47 pin aspiration cases they
penetration of the liver, yet this did overlooked. We found that abdominal presented, the distal end of the pin
not have any effect on her tenderness was an independent risk found in the lungs was the plastic
clinical status. No other complications factor for an impaled pin, and this has head. This may explain the low
were observed. A similar rate of been incorporated in our number of pins impaled in the upper
surgical interventions for hijab pin management recommendations. In airway and esophagus. However, in
ingestions was presented in a previous large cohort of hijab pin the stomach, the pin may rotate and
a previous study.12 ingestion cases,12 only patients who become impaled. The 29% rate for an
denied abdominal pain and had impaled pin in our study is similar to
Straight pins, and more specifically a normal physical examination were a 27% rate (38 of 137) previously
hijab pins, are clearly conservatively managed. This makes described.12 Once penetrated, the
underrepresented in the literature on their results less applicable to the plastic head acts as a safety
which current guidelines are general population arriving to the ED mechanism, lodging itself
based.10,13,14 Reilly et al13 included in and potentially filters out the more intraluminally on the mucosa and
their cohort various sharp object severe patients. Importantly, even allowing for relatively easy
ingestions but few straight pins. In while including symptomatic endoscopic retrieval (Fig 3B). On the
another study, only 3 of 244 cases patients with abdominal pain and contrary, ingested sewing needles can
were straight pins.10 Aydogdu et al7 tenderness in our study, none of transverse the mucosa into the
presented a cohort of foreign-body these patients suffered any peritoneal cavity.16
Downloaded from www.aappublications.org/news by guest on November 8, 2021
6 YOGEV et alDespite the uneventful clinical course without delaying preparation for hospital is the main referral center in
we described herein, hijab pins in the an endoscopy, because many of Jerusalem for the Muslim community
GI tract carry a small but significant these pins will pass spontaneously. as well as for complicated GI and
risk for serious complications. The 2. Stomach pins: admit patients for surgical pediatric cases. Another
most serious complications occurred observation. Conduct an limitation is that this is not an
in patients with no adequate follow- abdominal radiograph every 6 to interventional study, and the
up who carried an impaled pin for 12 hours. Discharge once the pin management recommendations we
several months. Alkan et al17 has moved beyond the stomach propose have not been validated
presented a patient with right-sided and the patient is asymptomatic. If prospectively.
hydronephrosis due to a hijab pin no progression is observed, plan
ingested 11 months earlier. for an endoscopy within 24 to CONCLUSIONS
Dalrymple et al reported a patient 48 hours.
with a perforation of the duodenum Hijab pin ingestion is a unique clinical
3. Abdominal tenderness: any patient entity. The majority of patients
and liver with a localized pus
with abdominal tenderness and affected are adolescent girls.
collection, who presented with mild
a stomach or bowel pin should be Conservative management reduces
abdominal pain 2 months after pin
admitted for observation. Plan for the rate of endoscopy yet does not
ingestion.18 There has been one
an endoscopy if no movement is increase the rate of complications.
report of death in a patient with hijab
observed within the first 6 to Location of the pin in the stomach
pin ingestion, although the details of
12 hours. and abdominal tenderness on
this case are not clear.19 These cases
reveal the importance of ensuring 4. Delayed presentation: obtain an physical examination were
adequate follow-up for asymptomatic abdominal CT scan of any patient strongly and independently
patients discharged from the hospital arriving with a pin ingestion associated with an impaled pin. In
without proof of passing the pin. dating .2 to 3 weeks. Consider no future guidelines specific
Although a CT scan should not be contrast or use bone window to management recommendations
a routine part of the workup for discriminate the pin from contrast should be considered for adolescents
ingested pins, we suggest considering material. with accidental ingestion of
an abdominal CT scan for any patient hijab pins.
Criteria for discharge from the ED are
arriving with a long-standing impaled as follows: (1) no abdominal
pin to assess for infectious and tenderness on physical examination, ACKNOWLEDGMENT
mechanical complications or if (2) the pin is beyond the pylorus, and We thank Nadav Levinger, MD,
otherwise clinically indicated. (3) adequate follow-up ensured for his assistance in the data
The following recommendations (including a follow-up radiograph collection.
summarize our management of hijab after 2–3 weeks).
pin ingestion in adolescent patients: Our study is limited by its
1. Esophageal pins: manage retrospective nature. There is ABBREVIATIONS
emergently according to current a potential for loss of follow-up of CT: computed tomography
guidelines. Consider an additional patients who later suffered from ED: emergency department
radiograph for patients with complications. However, we believe GI: gastrointestinal
a recent (1 hour) pin ingestion, that this is unlikely because our
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Cheng W, Tam PK. Foreign-body 2. Ikenberry SO, Jue TL, Anderson MA, Gastrointest Endosc. 2011;73(6):
ingestion in children: experience with et al; ASGE Standards of Practice 1085–1091
1,265 cases. J Pediatr Surg. 1999; Committee. Management of ingested 3. Macmanus JE. Perforations of the
34(10):1472–1476 foreign bodies and food impactions. intestine by ingested foreign bodies:
Downloaded from www.aappublications.org/news by guest on November 8, 2021
PEDIATRICS Volume 145, number 6, June 2020 7report of two cases and review of the BMJ Case Rep. 2014;2014: 14. Yuce O, Acikgoz M, Guzel A, et al.
literature. Am J Surg. 1941;53(3): bcr2013202336 Metallic foreign body ingestion during
393–402 9. Ilan O, Weinberger JM, Gomori JM, childhood; the experience of
4. Kramer RE, Lerner DG, Lin T, et al; North Gross M. Extraction of a headscarf pin a university hospital in Turkey. Journal
American Society for Pediatric from the vertebral artery without of Academic Emergency Medicine. 2015;
Gastroenterology, Hepatology, and embolization. Head Neck. 2012;34(4): 14:79–82
Nutrition Endoscopy Committee. 604–606 15. Uçan ES, Tahaoglu K, Mogolkoc N, et al.
Management of ingested foreign bodies 10. Paul RI, Christoffel KK, Binns HJ, Jaffe Turban pin aspiration syndrome: a new
in children: a clinical report of the DM; Pediatric Practice Research Group. form of foreign body aspiration. Respir
NASPGHAN Endoscopy Committee. Foreign body ingestions in children: Med. 1996;90(7):427–428
J Pediatr Gastroenterol Nutr. 2015; risk of complication varies with site of
60(4):562–574 16. Cevizci MN, Demir M, Demir B, Demir I,
initial health care contact. Pediatrics. Kilic O. Migration of ingested sewing
5. Binder L, Anderson WA. Pediatric 1993;91(1):121–127 needle from within sigmoid colon to
gastrointestinal foreign body 11. Orsagh-Yentis D, McAdams RJ, Roberts outside of the lumen. Pak J Med Sci.
ingestions. Ann Emerg Med. 1984;13(2): KJ, McKenzie LB. Foreign-body 2014;30(6):1422–1424
112–117 ingestions of young children treated in
6. Gregori D, Salerni L, Scarinzi C, et al. US emergency departments: 17. Alkan E, Ozkanli O, Balbay D. Right-sided
Foreign bodies in the upper airways 1995–2015. Pediatrics. 2019;143(5): hydronephrosis secondary to
causing complications and requiring e20181988 swallowing a headscarf pin. Urol Int.
hospitalization in children aged 0–14 2013;91(2):242–244
12. Hubara E, Ling G, Pinsk V, et al.
years: results from the ESFBI study. Eur Management of ingested hijab-pin. 18. Dalrymple RA, Berry K, Jester I. A sharp
Arch Otorhinolaryngol. 2008;265(8): J Gastrointest Surg. 2017;21(6): lesson: duodenal perforation 2 months
971–978 1062–1066 after ingestion of a pin. J Indian Assoc
7. Aydogdu S, Arikan C, Çakir M, et al. 13. Reilly BK, Stool D, Chen X, Rider G, Stool
Pediatr Surg. 2017;22(3):179–180
Foreign body ingestion in Turkish SE, Reilly JS. Foreign body injury in 19. Mir SA, Dar HM, Dogra V, Gilkar IA,
children. Turk J Pediatr. 2009;51(2): children in the twentieth century: Ahmad MM. Accidental ingestion of
127–132 a modern comparison to the Jackson hairpins in adolescent Muslim girls
8. Goh J, Patel N, Boulton R. Accidental collection. Int J Pediatr while doing or undoing the headscarf.
hijab pin ingestion in Muslim women: Otorhinolaryngol. 2003;67(suppl 1): International Surgery Journal. 2015;
an emerging endoscopic emergency? S171–S174 2(3):377–380
Downloaded from www.aappublications.org/news by guest on November 8, 2021
8 YOGEV et alHijab Pin Ingestions
Dotan Yogev, Fadi Mahameed, Alex Gileles-Hillel, Peri Millman, Zev Davidovics,
Saar Hashavya, David Rekhtman, Michael Wilschanski, Yackov Berkun and
Mordechai Slae
Pediatrics 2020;145;
DOI: 10.1542/peds.2019-3472 originally published online May 8, 2020;
Updated Information & including high resolution figures, can be found at:
Services http://pediatrics.aappublications.org/content/145/6/e20193472
References This article cites 19 articles, 3 of which you can access for free at:
http://pediatrics.aappublications.org/content/145/6/e20193472#BIBL
Subspecialty Collections This article, along with others on similar topics, appears in the
following collection(s):
Emergency Medicine
http://www.aappublications.org/cgi/collection/emergency_medicine_
sub
Gastroenterology
http://www.aappublications.org/cgi/collection/gastroenterology_sub
Permissions & Licensing Information about reproducing this article in parts (figures, tables) or
in its entirety can be found online at:
http://www.aappublications.org/site/misc/Permissions.xhtml
Reprints Information about ordering reprints can be found online:
http://www.aappublications.org/site/misc/reprints.xhtml
Downloaded from www.aappublications.org/news by guest on November 8, 2021Hijab Pin Ingestions
Dotan Yogev, Fadi Mahameed, Alex Gileles-Hillel, Peri Millman, Zev Davidovics,
Saar Hashavya, David Rekhtman, Michael Wilschanski, Yackov Berkun and
Mordechai Slae
Pediatrics 2020;145;
DOI: 10.1542/peds.2019-3472 originally published online May 8, 2020;
The online version of this article, along with updated information and services, is
located on the World Wide Web at:
http://pediatrics.aappublications.org/content/145/6/e20193472
Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
has been published continuously since 1948. Pediatrics is owned, published, and trademarked by
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2020
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
Downloaded from www.aappublications.org/news by guest on November 8, 2021You can also read

















































