Hyperreflective foci in predicting the treatment outcomes of diabetic macular oedema after anti vascular endothelial growth factor therapy
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
www.nature.com/scientificreports
OPEN Hyperreflective foci in predicting
the treatment outcomes of diabetic
macular oedema after anti‑vascular
endothelial growth factor therapy
Chu‑Hsuan Huang1, Chang‑Hao Yang2,3, Yi‑Ting Hsieh2, Chung‑May Yang2,3,
Tzyy‑Chang Ho2 & Tso‑Ting Lai2,4*
This retrospective study evaluated the association of hyperreflective foci (HRF) with treatment
response in diabetic macular oedema (DME) after anti-vascular endothelial growth factor (VEGF)
therapy. The medical records, including of ophthalmologic examinations and optical coherence
tomography (OCT) images, of 106 patients with DME treated with either intravitreal ranibizumab
or aflibercept were reviewed. The correlations between best-corrected visual acuity (BCVA) changes
and HRF along with other OCT biomarkers were analysed. The mean logMAR BCVA improved from
0.696 to 0.461 after an average of 6.2 injections in 1 year under real-world conditions. Greater
visual-acuity gain was noted in patients with a greater number of HRF in the outer retina at baseline
(p = 0.037), along with other factors such as poor baseline vision (p < 0.001), absence of epiretinal
membrane (p = 0.048), and presence of subretinal fluid at baseline (p = 0.001). The number of HRF after
treatment was correlated with the presence of hard exudate (p < 0.001) and baseline haemoglobin A1C
(p = 0.001). Patients with proliferative diabetic retinopathy had greater HRF reduction after treatment
(p = 0.018). The number of HRF in the outer retina, in addition to other baseline OCT biomarkers, could
be used to predict the treatment response in DME after anti-VEGF treatment.
Diabetic macular oedema (DME), occurring in 3–9% of patients with diabetes, is a sight-threatening condition
arising in cases of diabetic r etinopathy1–4. Among the different treatments for DME, anti-vascular endothelial
growth factor (anti-VEGF) therapy, compared with laser photocoagulation and steroid treatment, has been
shown to lead to superior visual outcomes5. Furthermore, intravitreal injection (IVI) of anti-VEGF agents such as
ranibizumab and aflibercept has been shown to significantly improve the vision and macular anatomy of patients
with DME in clinical trials, especially when injections were administered under strict loading and re-treatment
protocols6–8. However, the frequency of re-treatment in the real world was often lower than that recommended,
therefore resulting in relatively inferior outcomes compared with those of the clinical t rials9,10.
The treatment response of DME after anti-VEGF injection differs between clinical trial and real-world studies
and varies among patients. To better understand the prognosis of DME after anti-VEGF therapy, several clinical
biomarkers have been correlated with treatment outcomes, including central foveal thickness (CFT), external
limiting membrane disruption, ellipsoid zone disruption, subretinal fluid (SRF), and presence of hyperreflective
foci (HRF)11–13. Bolz et al. firstly reported the presence of HRF and their characteristics on optical coherence
tomography (OCT) in patients with D ME14, but their nature remained unclear despite several possible origins
having been proposed, including lipid extravasation from a compromised vasculature, microglia proliferation, or
retinal pigmented epithelium (RPE) m igration14,15. In addition, previous studies have also reported controversial
results regarding the correlation between HRF and visual acuity, especially that the presence of HRF in different
retinal layers at baseline might impact visual improvement after anti-VEGF therapy differently16–20. Therefore,
unlike other OCT biomarkers such as SRF, which have been determined to predict the treatment response of
DME12,21, the role of HRF as a predicting factor for DME has not been determined.
1
Department of Ophthalmology, Cathay General Hospital, Taipei, Taiwan. 2Department of Ophthalmology,
National Taiwan University Hospital, No 7, Chung‑Shan S. Rd., Taipei 100, Taiwan. 3Department of Ophthalmology,
College of Medicine, National Taiwan University, Taipei, Taiwan. 4Graduate Institute of Clinical Medicine, College
of Medicine, National Taiwan University, No 7, Chung‑Shan S. Rd., Taipei 100, Taiwan. *email: b91401005@
ntu.edu.tw
Scientific Reports | (2021) 11:5103 | https://doi.org/10.1038/s41598-021-84553-7 1
Vol.:(0123456789)www.nature.com/scientificreports/
Baseline characteristics (N = 106)
Age (y/o) 62.68 ± 9.21
Sex (male) 45.28%
HbA1C 7.63 ± 1.13%
Hypertension 62.22%
Pseudophakic 29.24%
Previous treatment 30.19%
PDR 31.43%
Hard exudate 45.28%
Baseline VA (LogMAR) 0.696 ± 0.317
Baseline CFT (μm) 410.86 ± 115.33
Epiretinal membrane 31.13%
Intraretinal cyst 86.79%
Subretinal fluid 31.13%
Table 1. Demographic data at the baseline of the patients who received anti-vascular endothelial growth
factor treatment for diabetic macular oedema. HbA1C haemoglobin A1C, PDR proliferative diabetic
retinopathy, VA visual acuity, CFT central foveal thickness.
Figure 1. The average BCVA and CFT at the baseline and 3, 6, 12 months after anti-VEGF treatment for
diabetic macular oedema. Both BCVA and CFT significantly improved compared with baseline at 3, 6, and
12 months after initial anti-VEGF treatment. BCVA best-corrected visual acuity, CFT central foveal thickness,
VEGF vascular endothelial growth factor. *p < 0.001 (compared with baseline).
The purpose of this study was to investigate the treatment response of DME and its correlation with OCT
biomarkers, especially the presence of HRF in different retinal layers.
Results
Visual and anatomical outcomes. The demographic data of the 106 patients with diabetic macular
oedema who were enrolled are summarised in Table 1. Overall, the average age was 62.7 ± 9.2 years, and 45.3%
of the patients were male. Proliferative diabetic retinopathy (PDR) was confirmed by fluorescein angiography
in 31.4% of patients. There were 69.8% treatment-naïve patients in our cohort. The mean logarithm of the mini-
mum angle of resolution (logMAR) best-corrected visual acuity (BCVA) at baseline was 0.696 ± 0.317. Factors
associated with poor baseline vision included thicker CFT, presence of SRF, and a greater number of HRF in the
inner retina (p < 0.001, p = 0.005, p = 0.014, respectively). The average BCVA at 3, 6, and 12 months after the first
injection was 0.525 ± 0.323, 0.516 ± 0.330, and 0.461 ± 0.351, respectively (Fig. 1), and significant visual improve-
ments were found at every time point compared with baseline (all p < 0.001). The mean injection numbers were
4.2 ± 1.0 in the first 6 months and 6.2 ± 2.1 in 1 year.
Association of hyperreflective foci with visual and anatomical improvements at 1 year. A
greater number of HRF in the outer retina at baseline was correlated with better BCVA improvement at the
12-month follow-up (p = 0.037). However, the number of HRF in the inner retina was not associated with BCVA
improvement. Other factors correlated with BCVA improvement are listed in Table 2. Patients with history of
hypertension, previous treatment for DME, and presence of epiretinal membrane (ERM) at baseline had lesser
visual improvement after treatment (p = 0.001, 0.031, and 0.048, respectively). In contrast, worse baseline vision
and the presence of SRF at baseline were correlated with better BCVA improvement (p < 0.001 and p = 0.001,
respectively). As for the treatment response of CFT, a greater number of HRF in both the inner and outer ret-
Scientific Reports | (2021) 11:5103 | https://doi.org/10.1038/s41598-021-84553-7 2
Vol:.(1234567890)www.nature.com/scientificreports/
VA change at the 12th
month
P-value Coefficient
Hypertension 0.001 0.209
Previous treatment 0.031 0.136
Baseline VA (LogMAR) < 0.001 − 0.337
Baseline epiretinal membrane 0.048 0.123
Baseline subretinal fluid 0.001 − 0.209
Baseline HRF in the outer retina 0.037 − 0.007
Table 2. Baseline factors associated with best-corrected visual acuity improvement at 1 year in patients
with diabetic macular oedema under anti-vascular endothelial growth factor therapy. VA visual acuity, HRF
hyperreflective foci.
Study Design N Treatment F/u (m) Assessment Layering VA implications
Associated with better VA outcome
Amounts of HRF in the outer retina associated
Current study Retro 106 Ranibizumab/Aflibercept 12 Quantitative Inner/outer/SRF
with greater VA improvement
Amounts of HRF associated with greater VA
Schreur et al.19, 2018 Retro 54 Bevacizumab 3 Quantitative Inner/outer
improvement
Presence of HRF in the outer retina associated
Yoshitake et al.29, 2020 Retro 77 Ranibizumab 12 Qualitative Inner/outer
with greater VA improvement
No association with VA outcome
Framme et al.16, 2012 Retro 51 Ranibizumab Bevacizumab 1 Quantitative Whole retina Amounts of HRF not associated with final VA
Vujosevic et al.27, 2016 Pro 20 Ranibizumab 6 Quantitative 3 layers Amounts of HRF not associated with final VA
Dexa implant Amounts of HRF within IRC not associated with
Ahn et al.22, 2020 Retro 45 1 Quantitative Within IRC
Anti-VEGF VA improvement
Associated with worse VA outcome—poor VA improvement
Presence of HRF associated with poor VA
Zur et al.30, 2018 Retro 299 Dexa implant 4 Quantitative Inner/outer
improvement
Presence of HRF in IRC associated with poor VA
Murakami et al.25, 2018 Retro 23 Ranibizumab 3 Qualitative Within IRC
improvement
Associated with worse VA outcome—poor final VA
Presence of HRF in the outer retina associated
Nishijima et al.26, 2014 Retro 32 Vitrectomy Mean: 15.3 Qualitative Outer
with poor final VA
Amounts of HRF in the outer retina associated
Kang et al.17, 2016 Retro 97 Bevacizumab Mean: 6.71 Quantitative Inner/outer
with poor final VA
Chatziralli et al.24, 2016a Retro 92 Ranibizumab Dexa implant 9 Quantitative Whole retina Amounts of HRF associated with poor final VA
Chatziralli et al.23, 2017b Pro 54 Dexa implant 12 Qualitative Whole retina Presence of HRF associated with poor final VA
Presence of HRF cluster associated with poor
Weingessel et al.28, 2018 Pro 50 Ranibizumab + laser PRN 60 Qualitative Whole retina
final VA
Liu et al.18, 2019 Retro 26 Conbercept 3 Quantitative Inner/outer/sub-RPE Amounts of HRF associated with poor final VA
Table 3. Studies evaluating the role of baseline hyperreflective foci in predicting visual outcomes after
treatment for diabetic macula oedema. N case number, F/u follow-up interval (months), VA visual acuity,
Retro retrospective, Pro prospective, IRC intraretinal cyst, Dexa implant dexamethasone implant, HRF
hyperreflective foci, SRF subretinal fluid, VEGF vascular endothelial growth factor, RPE retinal pigment
epithelium, PRN pro re nata. a This study included macula oedema resulted from diabetic retinopathy and
retinal vein occlusion. b This study included diabetic macular oedema patients refractory to anti-VEGF
treatment.
ina at baseline was correlated with greater CFT improvement at the 12-month follow-up (see Supplementary
Table S1 online).
Literature review regarding the role of hyperreflective foci in predicting visual outcomes. We
identified 13 studies that reported on the association between HRF and final visual acuities or visual
improvements16–19,22–30. The differences in study designs and their results are summarised in Table 3. Two stud-
ies reported greater VA improvement in the presence of HRF; one of them found that the correlation was limited
to HRF in the outer retina, and the other found a correlation between VA gain and HRF in both the inner and
outer retina. Three studies reported no association between HRF and final VA or VA improvement, and the other
8 studies reported less VA improvement or inferior final VA in the presence of baseline HRF.
Scientific Reports | (2021) 11:5103 | https://doi.org/10.1038/s41598-021-84553-7 3
Vol.:(0123456789)www.nature.com/scientificreports/
Figure 2. The average number of HRF in different retinal layers at the baseline and 3, 6, 12 months after anti-
vascular endothelial growth factor treatment for diabetic macular oedema. The number of HRF in every retinal
layer significantly decreased in all follow up time points compared with baseline. HRF hyperreflective foci, SRF
subretinal fluid. *p = 0.001 (compared with baseline). #p = 0.002 (compared with baseline). **p < 0.001 (compared
with baseline).
HRF in the inner retina, P-value (coefficient) HRF in the outer retina, P-value (coefficient)
Baseline 6th month 12th month Baseline 6th month 12th month
Age 0.896 0.517 0.886 0.157 0.027 (0.086) 0.037 (0.087)
Sex 0.217 0.157 0.394 0.682 0.146 0.187
HbA1c 0.984 0.024 (0.198) 0.002 (0.280) 0.632 0.001 (1.053) 0.001 (1.108)
HTN 0.545 0.451 0.363 0.883 0.325 0.362
Naïve 0.26 0.739 0.793 0.132 0.447 0.384
PDR 0.862 0.989 0.057 0.579 0.010 (− 2.014) 0.018 (− 2.047)
HE < 0.001 (1.665) < 0.001 (0.588) < 0.001 (0.744) < 0.001 (9.794) < 0.001 (5.374) < 0.001 (5.851)
Table 4. The coefficient and P-value in the linear regression model for possible associated baseline
characteristics of the number of HRF in the inner and outer retina at different time points. The coefficient of
significant factors (p-value < 0.05) is shown within the brackets. HbA1C haemoglobin A1C, HTN hypertension,
PDR proliferative diabetic retinopathy, HE hard exudate.
Factors associated with the amount of hyperreflective foci. The number of HRF at different ana-
tomical locations and different time points (Fig. 2) was correlated with baseline HRF amounts and other demo-
graphic data (Table 4). The presence of hard exudate correlated with the number of HRF at every time point and
every layer of the retina (p < 0.001 for all). The number of HRF in the inner and outer retina after treatment was
positively correlated with haemoglobin A1C (HbA1c) (p = 0.002 and 0.001, respectively). The number of HRF
in the outer retina was more greatly reduced after treatment in younger patients (p = 0.037) and in patients with
PDR (p = 0.018).
Comparison of the treatment outcomes of different anti‑VEGF agents. Among all 106 cases
enrolled, 65 eyes received IVI treatment with ranibizumab and 41 eyes with aflibercept. There was no difference
between the groups at baseline except for more ERM in the aflibercept group (15 [23%] vs. 18 [44%], p = 0.024)
and a higher incidence of SRF in the ranibizumab group (25 [39%] vs. 8 [20%], p = 0.04). The two groups had
comparable visual improvements at every time point. There were slightly fewer total injections in the aflibercept
group than in the ranibizumab group (6.5 ± 2.1 vs. 5.7 ± 1.9) with borderline significance (p = 0.080). There was
no interaction between the amounts of HRF in the outer retina and the drug type used in the regression model
in predicting VA improvement (p = 0.207).
Discussion
In this present study, we demonstrated the efficacy of anti-VEGF therapy in treating DME, both anatomically
and functionally, under real-world conditions. The treatment effect was sustained during the 1-year follow-up
with an average of six injections. In addition, a greater number of HRF in the outer retina at baseline predicted
better visual improvement, as did other OCT biomarkers such as absence of ERM and presence of SRF.
Bolz et al. first introduced the characteristics and localisation of HRF found on OCT among patients with
DME14. These HRF were commonly distributed through the retinal layers, including the subretinal space. In
addition to their presence in DME and advanced DR, HRF were also found in the early stage of DR with inad-
equate glucose and blood pressure control31. The different origins of HRF, including extravasated lipids from
Scientific Reports | (2021) 11:5103 | https://doi.org/10.1038/s41598-021-84553-7 4
Vol:.(1234567890)www.nature.com/scientificreports/
compromised microvessels in diabetic r etinopathy14, microglia activated by i nflammation32, and migrating RPE
cells33, might contribute to the wide distribution of HRF observed in our study.
Despite their undetermined nature, HRF have been linked to visual outcome, yet the results varied among
different studies (Table 3). Uji et al. found that the presence of HRF in the outer retina was related to poor baseline
vision and disrupted anatomical structure in DME before treatment20. In the present study, we found that patients
with a higher number of HRF in the outer retina had enhanced visual improvement at the 1-year follow-up,
which was in accordance with the findings of two recent r eports19,29. Other studies have reported inferior visual
outcome or limited improvement after anti-VEGF therapy with the presence of HRF at b aseline17,18,23–26,28,30. The
inconsistency might have resulted from the wide range of HRF present at baseline across studies. Furthermore,
the HRF in different studies may have had different origins, thus showing different predictive values. In addition,
not every study separately evaluated HRF in different retinal layers. In our study, we evaluated HRF according
to their presence in different retinal layers; hence, the exact role of HRF in outcome prediction could be better
appreciated.
To date, there is limited literature focusing on the relationship between other baseline biomarkers and the
presence of HRF before and after treatment. In the current study, we noted a strong correlation between the
presence of hard exudate at baseline and the presence of HRF in every layer before and after treatment. This
finding supported the hypothesis that HRF represents lipid extravasation as subclinical hard exudate. Further-
more, patients with PDR at baseline exhibited fewer residual HRF in the outer layer after treatment. The high
concentration of VEGF in patients with PDR possibly caused increased vascular permeability and leakage, which
further formed HRF. As a result, the HRF in these eyes had a better response under adequate anti-VEGF therapy,
and thus fewer HRF after treatment. The level of HbA1c, representing the average status of blood glucose con-
trol, was reported to be independent of the prognosis of DME treatment in a large clinical t rial34. However, in
a real-world retrospective study, better HbA1c was correlated with superior visual and anatomical outcomes35.
Framme et al. also showed that a greater number of HRF was found in patients with higher HbA1c16. In this study,
higher HbA1C at the time of diagnosing DME, possibly representing a more ischaemic retinal environment, was
related with a greater number of HRF in the inner and outer retina after anti-VEGF therapy. This effect lasted
for 12 months after first injection.
A previous study linked the presence of HRF to a higher grade of inflammation, which might contribute to
poor response to anti-VEGF t herapy32. Nevertheless, Chatziralli et al. demonstrated that both intravitreal anti-
VEGF and steroid therapy could result in a similar degree of HRF reduction in retinal vascular disease, along with
comparable visual o utcomes24. Our study also found significantly decreased HRF after anti-VEGF therapy, and
the reduction of HRF was similar among eyes treated with different anti-VEGF agents. The efficacy of different
anti-VEGF agents in treating DME has been evaluated in previous studies and showed conflicting results. While
one study with a small number of cases reported similar efficacy between aflibercept and r anibizumab36, other
studies showed superior efficacy of aflibercept37,38. Moreover, in DRCR.net protocol T, they reported a better
visual gain with aflibercept compared to ranibizumab at 1 year, especially in patient with worse baseline vision
(worse than 20/50)39–41. However, the difference was not significant at the 2-year follow-up40. In our study, which
only included patients with baseline vision worse than 20/50, the visual improvements were comparable in both
groups in a clinical practice setting, with a 12.5-letter gain in the ranibizumab group and a 10-letter gain in the
aflibercept group, which were both inferior to the results of the clinical trial. In addition, different anti-VEGF
agents did not affect the predictive value of HRF in our study.
Other biomarkers were also reported to be associated with VA outcomes. The presence of SRF was correlated
with better visual acuity improvement and CFT reduction in our study, which were in accordance with previ-
ous findings42,43, especially when the patients had been treated a ggressively21. Conversely, the presence of ERM
contributed to inferior functional and anatomical o utcomes44. In addition to those baseline OCT biomarkers, the
BCVA response at 3 months also independently predicted the visual outcome at 12 months (see Supplementary
Table S1 online) as described in a previous s tudy45.
The major limitation of this study was its retrospective nature and the relatively small number of patients. Fur-
thermore, the decision and timing for re-injection were also based on variable clinical conditions and decided by
the patient and physician. However, our results constitute evidence derived from a real-world setting and provide
additional information, complementing the findings of clinical trials, to help guide physicians in their routine
clinical practice. Another limitation was the possibility of selection bias, especially when comparing the treatment
outcomes between different anti-VEGF agents. Although most baseline factors were balanced, the prevalence
of ERM and SRF was slightly different at baseline between the aflibercept group and the ranibizumab group.
In conclusion, we reported our real-world experience with the 1-year outcome of anti-VEGF treatment for
DME, showing significant visual and anatomical improvements with both aflibercept and ranibizumab. In addi-
tion, we demonstrated that OCT biomarkers including SRF, ERM, and HRF in the outer retinal layer could help
predict the treatment outcomes in patients with DME after anti-VEGF therapy. Furthermore, the number of
HRF was associated with the presence of hard exudates at baseline, the status of diabetic retinopathy, and blood
glucose control. Our results could help predict the treatment response in patients with DME and might further
facilitate individualised treatment.
Methods
Study population and intervention. We retrospectively reviewed the records of patients who had been
diagnosed with DME and treated with 0.5 mg of ranibizumab or 2 mg of aflibercept in National Taiwan Uni-
versity Hospital from January 2016 to December 2017. The study has been approved by the Institutional Review
Board of National Taiwan University Hospital and was performed in accordance with the guidelines and regula-
tions of the Institutional Review Board; the study also adhered to the tenets of the Declaration of Helsinki. The
Scientific Reports | (2021) 11:5103 | https://doi.org/10.1038/s41598-021-84553-7 5
Vol.:(0123456789)www.nature.com/scientificreports/
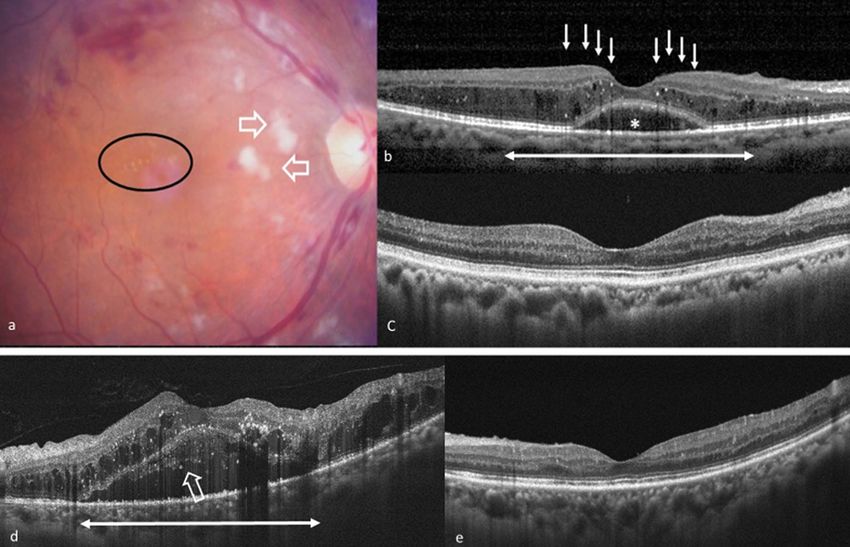
Figure 3. Two representative cases of patients who had DME and underwent anti-vascular endothelial
growth factor treatment. (a–c) A 67-year-old female patient without previous treatment for DME. (a) The
fundus photography at the baseline revealed severe non-proliferative diabetic retinopathy with diffuse retinal
haemorrhage and cotton wool spots (empty arrows). There was a limited amount of hard exudate in the macular
area (circle). (b) The OCT at baseline exhibited DME and the presence of SRF (asterisk). Large numbers of
HRF, mostly located in the outer retina (white arrows), were found within 3 mm of the central macula (double
arrow). The baseline visual acuity was 20/100, and CFT was 406 μm. (c) The patient received three injections
in 1 year, and the final OCT revealed total resolution of DME and disappearance of HRF in every retinal layer
in the central macula. The visual acuity was 20/30, and the CFT was 188 μm at the final visit. (d,e) A 49-year-
old male patient without previous treatment for DME. (d) The OCT at baseline exhibited DME with SRF and
the presence of HRF in all three retinal layers. The presence of HRF in SRF is highlighted (empty arrow). The
baseline visual acuity was 20/100, and the CFT was 859 μm. (e) After eight injections in 1 year, the final OCT
revealed total resolution of DME and significantly decreased HRF in every retinal layer. The visual acuity was
20/25, and the CFT was 213 μm at the final visit. CFT central foveal thickness, DME diabetic macular oedema,
HRF hyperreflective foci, OCT optical coherence tomography, SRF subretinal fluid.
necessary informed consent was obtained from all patients. Patients with OCT- and fluorescein angiography-
evident central involving DME and a baseline BCVA between 20/400 and 20/40 (Snellen) were included in this
study. All patients were treated with two or three monthly loading injections, followed by as needed injections
according to the BCVA change and OCT findings at each follow-up visit. Each patient visited the clinic every
4–8 weeks for at least 1 year. The choice between ranibizumab and aflibercept was based on the physician’s pref-
erence. The exclusion criteria included a serum haemoglobin A1c (HbA1c) level greater than 10% at baseline, a
history of receiving vitrectomy, glaucoma, previous treatments for DME (e.g. macular laser, intravitreal steroid,
and anti-VEGF agents) within 6 months prior to the first IVI in our hospital, presence of macular scar, less than
two loading injections of anti-VEGF, and presence of coexisting retinal vascular disease.
Data collection. We collected baseline data including of age, sex, HbA1c at the time of first anti-VEGF
treatment, hypertension, lens status, previous treatment (PRP, IVI, steroid, or laser), BCVA in logMAR, fun-
dus photography, fluorescein angiography, and OCT images. The OCT was performed using the RTVue XR
Avanti with AngioVue OCTA system (Optovue Inc., Fremont, CA, USA), and fluorescein angiography using
Heidelberg retina angiography HRA 2 (Heidelberg Engineering Inc., Germany). The presence of hard exudate
on fundus photography, the presence of PDR on fluorescein angiography, CFT, the presence of ERM, intraretinal
cysts (IRCs), SRF, and the number of HRF on OCT were recorded. The following data were also collected at 3,
6, and 12 months after first injection: BCVA in logMAR, CFT, number of injections, presence of ERM, IRCs,
and SRF, and the number of HRF. HRF were defined as discrete, circumscribed, hyperreflective dots on OCT,
with size ranging from 20 to 40 μm (Fig. 3). The location of HRF was classified into three layers, modified from
Scientific Reports | (2021) 11:5103 | https://doi.org/10.1038/s41598-021-84553-7 6
Vol:.(1234567890)www.nature.com/scientificreports/
the study by Zur et al.30, including inner (from the internal limiting membrane to the inner nuclear layer), outer
(from the outer plexiform layer to the ellipsoid zone), and SRF (within the SRF) layers. The amounts of HRF
within the central 3 mm of the macula were manually counted by two retinal specialists (TTL and CHH), and
the central 3 mm of the macula was defined as 1500 μm on both sides from the foveal centre using the built-in
software calliper.
Literature review. To better understand the role of HRF in predicting the treatment outcomes of DME,
we conducted a systematic search using the PubMed database for studies written in any language and published
before June 28, 2020. We used the following keywords: (hyperreflective foci) AND (diabetic macular edema).
In addition, we reviewed the reference lists of all selected articles to identify other potentially relevant studies.
The eligibility criteria were: (1) recruited patients with DME who received any type of treatment; (2) evaluated
the presence of HRF, either qualitatively or quantitatively, using OCT; (3) reported on the association of HRF
with treatment response of DME, as either final BCVA or BCVA improvement. Two retinal specialists (TTL and
CHH) independently reviewed the titles and abstracts of all identified studies and extracted the data from all
eligible studies.
Statistical analysis. For the analysis of BCVA, CFT, and the amount of HRF, the comparisons of meas-
urements between baseline and follow-up visits were performed with paired Student’s t-tests. Linear regres-
sion analyses were performed to evaluate the predictive factors for visual outcome and CFT at the 12-month
follow-up. The candidate predictive factors included demographic data, OCT biomarkers, drug type, interaction
between drug type and HRF, and injection numbers. Age, sex, and pre-treatment logMAR BCVA (for visual
improvement) or CFT (for CFT reduction) were adjusted in all models. Linear regression analyses were also
performed to evaluate the factors associated with the number of HRF. The candidate predictive factors included
age, sex, HbA1c, presence of HTN, treatment history, and presence of PDR or hard exudate. The statistical analy-
sis was performed using SPSS (V.21; IBM Corp., Armonk, NY, USA). A P value lower than 0.05 was considered
statistically significant.
Data availability
The database of current study will be available on request after the evaluation and approval of the request by the
Institutional Review Board of National Taiwan University Hospital.
Received: 20 May 2020; Accepted: 18 February 2021
References
1. Wong, T. Y. et al. Diabetic retinopathy in a multi-ethnic cohort in the United States. Am. J. Ophthalmol 141, 446–455. https://doi.
org/10.1016/j.ajo.2005.08.063 (2006).
2. Wong, T. Y. et al. Guidelines on diabetic eye care: The international council of ophthalmology recommendations for screening,
follow-up, referral, and treatment based on resource settings. Ophthalmology 125, 1608–1622. https://doi.org/10.1016/j.ophth
a.2018.04.007 (2018).
3. Yau, J. W. et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 35, 556–564. https: //doi.org/10.2337/
dc11-1909 (2012).
4. Zhang, X. et al. Prevalence of diabetic retinopathy in the United States, 2005–2008. JAMA 304, 649–656. https://doi.org/10.1001/
jama.2010.1111 (2010).
5. Kim, E. J. et al. Treatment of diabetic macular edema. Curr. Diab. Rep. 19, 68. https://doi.org/10.1007/s11892-019-1188-4 (2019).
6. Brown, D. M. et al. Intravitreal aflibercept for diabetic macular edema: 100-week results from the VISTA and VIVID Studies.
Ophthalmology 122, 2044–2052. https://doi.org/10.1016/j.ophtha.2015.06.017 (2015).
7. Fouda, S. M. & Bahgat, A. M. Intravitreal aflibercept versus intravitreal ranibizumab for the treatment of diabetic macular edema.
Clin. Ophthalmol. 11, 567–571. https://doi.org/10.2147/OPTH.S131381 (2017).
8. Nguyen, Q. D. et al. Ranibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Oph-
thalmology 119, 789–801. https://doi.org/10.1016/j.ophtha.2011.12.039 (2012).
9. Holekamp, N. M. et al. Vision outcomes following anti-vascular endothelial growth factor treatment of diabetic macular edema
in clinical practice. Am. J. Ophthalmol. 191, 83–91. https://doi.org/10.1016/j.ajo.2018.04.010 (2018).
10. Patrao, N. V. et al. Real-world outcomes of ranibizumab treatment for diabetic macular edema in a United Kingdom National
Health Service Setting. Am. J. Ophthalmol. 172, 51–57. https://doi.org/10.1016/j.ajo.2016.09.002 (2016).
11. Choi, M. Y., Jee, D. & Kwon, J. W. Characteristics of diabetic macular edema patients refractory to anti-VEGF treatments and a
dexamethasone implant. PLoS ONE 14, e0222364. https://doi.org/10.1371/journal.pone.0222364 (2019).
12. Lai, T. T., Yang, C. M., Yang, C. H., Ho, T. C. & Hsieh, Y. T. Treatment outcomes and predicting factors for diabetic macular edema
treated with ranibizumab: One-year real-life results in Taiwan. J. Formos. Med. Assoc. 118, 194–202. https://doi.org/10.1016/j.
jfma.2018.03.009 (2019).
13. Kwan, C. C. & Fawzi, A. A. Imaging and biomarkers in diabetic macular edema and diabetic retinopathy. Curr. Diab. Rep. 19, 95.
https://doi.org/10.1007/s11892-019-1226-2 (2019).
14. Bolz, M. et al. Optical coherence tomographic hyperreflective foci: A morphologic sign of lipid extravasation in diabetic macular
edema. Ophthalmology 116, 914–920. https://doi.org/10.1016/j.ophtha.2008.12.039 (2009).
15. Framme, C., Wolf, S. & Wolf-Schnurrbusch, U. Small dense particles in the retina observable by spectral-domain optical coherence
tomography in age-related macular degeneration. Invest. Ophthalmol. Vis. Sci. 51, 5965–5969. https: //doi.org/10.1167/iovs.10-5779
(2010).
16. Framme, C., Schweizer, P., Imesch, M., Wolf, S. & Wolf-Schnurrbusch, U. Behavior of SD-OCT-detected hyperreflective foci in
the retina of anti-VEGF-treated patients with diabetic macular edema. Invest. Ophthalmol. Vis. Sci. 53, 5814–5818. https://doi.
org/10.1167/iovs.12-9950 (2012).
17. Kang, J. W., Chung, H. & Chan Kim, H. Correlation of optical coherence tomographic hyperreflective foci with visual outcomes
in different patterns of diabetic macular edema. Retina 36, 1630–1639. https://doi.org/10.1097/IAE.0000000000000995 (2016).
18. Liu, S., Wang, D., Chen, F. & Zhang, X. Hyperreflective foci in OCT image as a biomarker of poor prognosis in diabetic macular
edema patients treating with Conbercept in China. BMC Ophthalmol. 19, 157. https://doi.org/10.1186/s12886-019-1168-0 (2019).
Scientific Reports | (2021) 11:5103 | https://doi.org/10.1038/s41598-021-84553-7 7
Vol.:(0123456789)www.nature.com/scientificreports/
19. Schreur, V. et al. Hyperreflective foci on optical coherence tomography associate with treatment outcome for anti-VEGF in patients
with diabetic macular edema. PLoS ONE 13, e0206482. https://doi.org/10.1371/journal.pone.0206482 (2018).
20. Uji, A. et al. Association between hyperreflective foci in the outer retina, status of photoreceptor layer, and visual acuity in diabetic
macular edema. Am. J. Ophthalmol. 153, 710–717. https://doi.org/10.1016/j.ajo.2011.08.041 (2012).
21. Lai, T. T., Hsieh, Y. T., Yang, C. M., Ho, T. C. & Yang, C. H. Effect of reimbursement policy on visual outcomes in patients with
diabetic macular edema treated with ranibizumab. Retina https://doi.org/10.1097/IAE.0000000000002716 (2019).
22. Ahn, J., Han, S., Ahn, S. M., Kim, S. W. & Oh, J. Clinical implications of suspended scattering particles in motion observed by
optical coherence tomography angiography. Sci. Rep. 10, 15. https://doi.org/10.1038/s41598-019-55606-9 (2020).
23. Chatziralli, I. et al. Identification of time point to best define “sub-optimal response” following intravitreal ranibizumab therapy
for diabetic macular edema based on real-life data. Eye (Lond) 31, 1594–1599. https://doi.org/10.1038/eye.2017.111 (2017).
24. Chatziralli, I. P., Sergentanis, T. N. & Sivaprasad, S. Hyperreflective foci as an independent visual outcome predictor in macular
edema due to retinal vascular diseases treated with intravitreal dexamethasone or ranibizumab. Retina 36, 2319–2328. https://doi.
org/10.1097/IAE.0000000000001070 (2016).
25. Murakami, T. et al. Association between characteristics of foveal cystoid spaces and short-term responsiveness to ranibizumab for
diabetic macular edema. Jpn J. Ophthalmol. 62, 292–301. https://doi.org/10.1007/s10384-018-0575-8 (2018).
26. Nishijima, K. et al. Hyperreflective foci in outer retina predictive of photoreceptor damage and poor vision after vitrectomy for
diabetic macular edema. Retina 34, 732–740. https://doi.org/10.1097/IAE.0000000000000005 (2014).
27. Vujosevic, S. et al. Hyperreflective retinal spots and visual function after anti-vascular endothelial growth factor treatment in
center-involving diabetic macular edema. Retina 36, 1298–1308. https://doi.org/10.1097/IAE.0000000000000912 (2016).
28. Weingessel, B. et al. Treatment of diabetic macular edema with intravitreal antivascular endothelial growth factor and prompt versus
deferred focal laser during long-term follow-up and identification of prognostic retinal markers. J. Ophthalmol. 2018, 3082560.
https://doi.org/10.1155/2018/3082560 (2018).
29. Yoshitake, T. et al. Hyperreflective foci in the outer retinal layers as a predictor of the functional efficacy of ranibizumab for diabetic
macular edema. Sci. Rep. 10, 873. https://doi.org/10.1038/s41598-020-57646-y (2020).
30. Zur, D. et al. OCT biomarkers as functional outcome predictors in diabetic macular edema treated with dexamethasone implant.
Ophthalmology 125, 267–275. https://doi.org/10.1016/j.ophtha.2017.08.031 (2018).
31. De Benedetto, U., Sacconi, R., Pierro, L., Lattanzio, R. & Bandello, F. Optical coherence tomographic hyperreflective foci in early
stages of diabetic retinopathy. Retina 35, 449–453. https://doi.org/10.1097/IAE.0000000000000336 (2015).
32. Lee, H., Jang, H., Choi, Y. A., Kim, H. C. & Chung, H. Association between soluble CD14 in the aqueous humor and hyperreflective
foci on optical coherence tomography in patients with diabetic macular edema. Invest. Ophthalmol. Vis. Sci. 59, 715–721. https://
doi.org/10.1167/iovs.17-23042(2018).
33. Chen, K. C. et al. Intraretinal hyperreflective foci in acquired vitelliform lesions of the Macula: Clinical and histologic study. Am.
J. Ophthalmol. 164, 89–98. https://doi.org/10.1016/j.ajo.2016.02.002 (2016).
34. Singh, R. P. et al. The impact of systemic factors on clinical response to ranibizumab for diabetic macular edema. Ophthalmology
123, 1581–1587. https://doi.org/10.1016/j.ophtha.2016.03.038 (2016).
35. Matsuda, S. et al. The impact of metabolic parameters on clinical response to VEGF inhibitors for diabetic macular edema. J.
Diabetes Complications 28, 166–170. https://doi.org/10.1016/j.jdiacomp.2013.11.009 (2014).
36. Shimizu, N. et al. Comparisons of efficacy of intravitreal aflibercept and ranibizumab in eyes with diabetic macular edema. Biomed
Res. Int. 2017, 1747108. https://doi.org/10.1155/2017/1747108 (2017).
37. Babiuch, A. S. et al. Diabetic macular edema treated with intravitreal aflibercept injection after treatment with other anti-VEGF
agents (SWAP-TWO study): 6-month interim analysis. Int. J. Retina Vitreous 5, 17. https://doi.org/10.1186/s40942-019-0167-x
(2019).
38. Herbaut, A. et al. Switching to aflibercept in diabetic macular edema not responding to ranibizumab and/or intravitreal dexa-
methasone implant. J. Ophthalmol. 2017, 8035013. https://doi.org/10.1155/2017/8035013 (2017).
39. Cai, S. & Bressler, N. M. Aflibercept, bevacizumab or ranibizumab for diabetic macular oedema: recent clinically relevant findings
from DRCR.net Protocol T. Curr. Opin. Ophthalmol. 28, 636–643. https://doi.org/10.1097/ICU.0000000000000424 (2017).
40. Wells, J. A. et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema: Two-year results from a comparative
effectiveness randomized clinical trial. Ophthalmology 123, 1351–1359. https://doi.org/10.1016/j.ophtha.2016.02.022 (2016).
41. Diabetic Retinopathy Clinical Research, N. et al. Aflibercept, bevacizumab, or ranibizumab for diabetic macular edema. N. Engl.
J. Med. 372, 1193–1203. https://doi.org/10.1056/NEJMoa1414264 (2015).
42. Schwarzer, P., Ebneter, A., Munk, M., Wolf, S. & Zinkernagel, M. S. One-year results of using a treat-and-extend regimen without
a loading phase with anti-VEGF agents in patients with treatment-naive diabetic macular edema. Ophthalmologica 241, 220–225.
https://doi.org/10.1159/000495623 (2019).
43. Sophie, R., Lu, N. & Campochiaro, P. A. Predictors of functional and anatomic outcomes in patients with diabetic macular edema
treated with ranibizumab. Ophthalmology 122, 1395–1401. https://doi.org/10.1016/j.ophtha.2015.02.036 (2015).
44. Wong, Y. et al. Vitreoretinal interface abnormalities in patients treatedwith ranibizumab for diabetic macular oedema. Graefes
Arch. Clin. Exp. Ophthalmol. 255, 733–742. https://doi.org/10.1007/s00417-016-3562-0 (2017).
45. Dugel, P. U. et al. Baseline visual acuity strongly predicts visual acuity gain in patients with diabetic macular edema following
anti-vascular endothelial growth factor treatment across trials. Clin. Ophthalmol. 10, 1103–1110. https://doi.org/10.2147/OPTH.
S100764 (2016).
Author contributions
C.H.Y. and T.T.L. designed the study. C.H.H. prepared the manuscript. C.H.Y., Y.T.H., T.C.H., C.M.Y., and
T.T.L. collected the clinical data. C.H.H., Y.T.H., and T.T.L. performed the statistical analysis. C.H.Y. and T.T.L.
supervised the research. All authors reviewed, revised, and agreed with the manuscript.
Competing interests
The authors declare no competing interests.
Additional information
Supplementary Information The online version contains supplementary material available at https://doi.
org/10.1038/s41598-021-84553-7.
Correspondence and requests for materials should be addressed to T.-T.L.
Reprints and permissions information is available at www.nature.com/reprints.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and
institutional affiliations.
Scientific Reports | (2021) 11:5103 | https://doi.org/10.1038/s41598-021-84553-7 8
Vol:.(1234567890)www.nature.com/scientificreports/
Open Access This article is licensed under a Creative Commons Attribution 4.0 International
License, which permits use, sharing, adaptation, distribution and reproduction in any medium or
format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the
Creative Commons licence, and indicate if changes were made. The images or other third party material in this
article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the
material. If material is not included in the article’s Creative Commons licence and your intended use is not
permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from
the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
© The Author(s) 2021
Scientific Reports | (2021) 11:5103 | https://doi.org/10.1038/s41598-021-84553-7 9
Vol.:(0123456789)You can also read