Lincolnshire Primary Care - S
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Lincolnshire Primary Care
S
Pain Management Guidance 2019
LINCOLNSHIRE Clinical Commissioning Groups in association with
Lincolnshire Prescribing and Clinical Effectiveness (PACEF) Forum,
Optum Medicines Management Team and Connect Health Community
Pain Management Services in Lincolnshire.
This guidance is intended for use within primary care and community services
across Lincolnshire by all prescribers (medical and non-medical) and all clinical
staff reviewing patients with chronic/persistent pain.
Version: 1.0
Name of originator/author: James Musk – Clinical Pharmacist, Medicines
Management & Optimisation Team, Optum
Health Services Solutions
Helen Liddell – Consultant Pharmacist, Connect
Health Community Pain Management Services
Name of responsible Prescribing and Clinical Effectiveness Forum
committee/individual: (PACEF)
Date approved by responsible TBC
committee
Date issued: November 2019
Review date: TBC
Target audience: Lincolnshire Clinical Commissioning Groups
(LECCG, LWCCG,SLCCG, SWLCCG) and all
prescribersContents
Patient Assessment ...............................................................................................................3
Pain Intensity .........................................................................................................................4
NHS England recommendations – items not recommended for routine prescribing in primary care
..............................................................................................................................................5
Co-proxamol ......................................................................................................................5
Lidocaine (Versatis®) 5% w/w 700mg medicated plasters .................................................5
Targinact (Oxycodone and Naloxone Combination Product) ..............................................6
Tramacet (Paracetamol and Tramadol Combination Product) ............................................7
Opioid and Gabapentinoid prescribing risks and harms .....................................................8
Opioid Prescribing .................................................................................................................9
General principles of good prescribing practice ..................................................................9
Before initiating opioid therapy...............................................................................................9
Opioid trial ...........................................................................................................................10
Opioid Prescribing ...............................................................................................................10
Opioids and driving ..............................................................................................................10
Opioid Monitoring ................................................................................................................11
Opioid equivalences (read all points below before changing opioids) ..................................11
Approximate equi-analgesic potencies of opioids for oral administration from; .................12
https://www.rcoa.ac.uk/faculty-of-pain-medicine/opioids-aware/structured-approach-to-
prescribing/dose-equivalents-and-changing-opioids .........................................................12
Transdermal preparations ................................................................................................12
Fentanyl .......................................................................................................................12
Buprenorphine – transdermal buprenorphine changed at 7 day (weekly) intervals .....12
Buprenorphine – transdermal buprenorphine changed every three or four days (twice weekly)
.....................................................................................................................................12
Tapering and stopping opioids .............................................................................................13
Stopping opioids in primary care ..........................................................................................13
Stopping opioids in collaboration with specialist services .....................................................13
Points to discuss with patients when de-prescribing ............................................................14
Opioid prescribing contract example ....................................................................................15
Patient Information leaflets .....................................................Error! Bookmark not defined.
Risks of Opioid Medications .............................................................................................17
Opioid side effects............................................................................................................18
Gabapentinoid prescribing risks .......................................................................................20
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 2 of 22
Date: September 2019 - Review date 2021Overview information to support one page summary
The one-page summary ‘Lincolnshire Primary Care— Managing Non-malignant
Chronic/Persistent Pain One-Page Guide’ has been developed to support primary care
prescribers and patients in making the best choices in relation to medicines prescribed to help
ease pain. This summary does not include management of pain in end of life settings or of
disease specific treatments which result in pain reduction (e.g. interventions for angina). This
more detailed ‘Lincolnshire Primary Care Pain Management Guidance 2019’ document aims to
provide guidance to support the one page summary and support conversations and treatment
decisions with patients regarding pain management.
Patient Assessment
The experience of pain is complex and influenced by the degree of tissue injury, current mood,
previous experience of pain and understanding of the cause and significance of pain. Previous
unpleasant thoughts, emotions and experiences can also contribute to the current perception of
pain and if unresolved, can act as a barrier to treatment. A full pain history should therefore
include:
• Description of pain
• Where is the pain?
• Does it radiate elsewhere?
• What does the pain feel like (eg, aching, burning, stabbing)?
• Does it vary in intensity?
• What makes it worse?
• What makes it better?
• What is the effect on sleep?
• What is the effect on mood?
• What is the effect on physical function?
• What is the effect on vocational/social function?
• Current medications and response to drugs (it may be appropriate to continue non-
opioid therapies which have been previously effective)
• Response to previous medications and other interventions including self-management
strategies and alternative therapies (If opioids have previously been ineffective it is
unlikely that offering an alternative opioid preparation will be helpful.)
• Physical health including operations and illnesses. NB some comorbidities such as renal
or hepatic impairment and sleep apnoea, will influence the choice of drug, dose and
safety of therapy
• Mental health including emotional trauma, previous and current mood, contact with
mental health circumstances. Mental health comorbidities and a history of significant
emotional trauma are not a contraindication to opioid therapy but:
– are a risk factor for opioid therapy becoming prolonged and for high doses to be
used
– patients may use opioids to blunt unpleasant thoughts and experiences: this may
make opioids difficult to stop
– are a risk factor for addiction to prescribed opioids
– will be contributory to the current pain experience so need to be identified and
managed separately
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 3 of 22
Date: September 2019 - Review date 2021• Current or previous history of addiction to drugs or alcohol. Patients with a current or
past history of addiction will need careful management and support in collaboration with
specialists with expertise in addiction
• Patient circumstances and context (employment, family responsibilities, sources of
support). Patients with a family/household member with addiction will need additional
support and counselling about risks of diversion of controlled drugs
• Patient’s understanding of pain and expectations of outcome
• Pain assessment tools e.g. VAS, Brief Pain Inventory, Leeds Neuropathic Pain Scale
• Relevant physical examination including observation of patient mobility, distress
• Imaging and other diagnostics (x-rays, scans, blood tests and electrophysiology)
Pain is usually classified depending on duration of symptoms.
• Acute pain is short term pain usually relating to some sort of injury including operation,
fracture or infection. Medicines for acute pain should not be put on repeat prescription
as patients will need to be reassessed regarding changing analgesic requirements.
• Chronic pain (also known as persistent pain) is longer lasting, usually more than three
months and includes lower back pain and arthritis. Sometimes chronic pain can develop
from an acute pain that persists.
• Pain from nerve damage e.g. in diabetes, shingles, multiple sclerosis and following
stroke, is described as neuropathic pain which is a type of chronic pain. (The term
nociceptive pain implies pain associated with a specific definable injury process that is
not neuropathic).
• Visceral pain is pain arising from pelvic, abdominal or thoracic organs. This type of pain
may have neuropathic characteristics but may be particularly complex and always
needs a detailed assessment. Pain symptoms may fall into more than one category.
Pain Intensity
Both acute and chronic pain can range from mild to severe. The intensity of acute pain is largely
(but not completely) related to the degree of tissue injury; put simply, an extensive injury hurts
more than a smaller one. However, there is no similar relationship for chronic pain where the
amount of tissue damage is a small contributor to pain intensity. Anxiety, distress, depression
and concern about causes of pain contribute to the level of pain experienced. Also, unpleasant
thoughts, feelings and memories (even if unrelated to pain) can influence pain severity. This is
not considered a reporting bias; these experiences have been shown to influence pain
perception directly.
On first presentation, simple analgesia should be considered. Self-care may be an option as
paracetamol tablets, ibuprofen tablets and ibuprofen gel are available to buy over the counter.
If further pain relief is needed or if there is obvious severe tissue injury (e.g. major trauma,
postoperative pain) codeine or tramadol may be added. Medications should be an adjunct to
strategies such as addressing common psychological comorbidities (anxiety/depression),
cognitive behavioural strategies, sleep restoration strategies, and physiotherapy. Complete
relief of symptoms is not a goal of therapy as pain provides the body with a protective
mechanism against potential or actual damage to the body’s tissues. Treatment goals should
be patient specific and aim to improve quality of life e.g. improved ability to manage activities of
daily living independently, improved exercise tolerance.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 4 of 22
Date: September 2019 - Review date 2021For details regarding formulary & prescribing recommendations for analgesia prescribing across
Lincolnshire, please see http://www.lincolnshirejointformulary.nhs.uk/
NHS England recommendations – items not recommended for routine
prescribing in primary care
In 2017 NHS England produced guidance on ‘Items which should not routinely be prescribed in
primary care’. Within this was specific guidance relating to four analgesics currently prescribed
within Lincolnshire as of August 2019;
Co-proxamol
Recommendation
NHS England advises CCGs that prescribers in primary care should not initiate co-
proxamol for any new patient.
NHS England advises CCGs to support prescribers in de-prescribing co-proxamol in all
patients and, where appropriate, ensure the availability of relevant services to facilitate
this change (referral to specialist pain service).
Category
Products of low clinical effectiveness, where there is a lack of robust evidence of clinical
effectiveness or there are significant safety concerns.
Annual Spend (nationally as of 2017)
£9,002,824 (NHS Digital)
Background and Rationale
Co-proxamol was a pain-killer which was previously licensed in the UK until being fully
withdrawn from the market in 2007 due to safety concerns. All use in the UK is now on an
unlicensed basis. Since 1985 advice aimed at the reduction of co-proxamol toxicity and fatal
overdose has been provided, but this was not effective and resulted in withdrawal of co-
proxamol by the MHRA. Since the withdrawal, further safety concerns have been raised which
have resulted in co-proxamol being withdrawn in other countries.
Due to the significant safety concerns, the joint clinical working group considered co-proxamol
suitable for inclusion in this guidance.
Patient information leaflets:
https://www.prescqipp.info/items-which-should-not-routinely-be-prescribed-patient-leaflets
Lidocaine (Versatis®) 5% w/w 700mg medicated plasters
Recommendation
NHS England advises CCGs that prescribers in primary care should not initiate lidocaine
plasters for any new patient (apart from exceptions below)
NHS England advises CCGs to support prescribers in deprescribing lidocaine plasters in
all patients and, where appropriate, ensure the availability of relevant services to
facilitate this change.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 5 of 22
Date: September 2019 - Review date 2021 NHS England advises CCGs that if, in exceptional circumstances, there is a clinical
need for lidocaine plasters to be prescribed in primary care, this should be undertaken in
a cooperation arrangement with a multi-disciplinary team and/or other healthcare
professional.
Exceptions and further recommendations
These recommendations do not apply to patients who have been treated in line with NICE
CG173 Neuropathic pain in adults: pharmacological management in non-specialist settings but
are still experiencing neuropathic pain associated with previous herpes zoster infection (post-
herpetic neuralgia).
Category
Item of low clinical effectiveness, where there is a lack of robust evidence of clinical
effectiveness or there are significant safety concerns
Annual Spend (nationally as of 2017)
£19,295,030 (NHS Digital)
Background and Rationale
Lidocaine plasters can be applied for pain relief and are licensed for symptomatic relief of
neuropathic pain associated with previous herpes zoster infection (post-herpetic neuralgia,
PHN) in adults.
NICE CG173 Neuropathic pain in adults: pharmacological management in non-specialist
settings does not recommend lidocaine plasters for treating neuropathic pain.
The joint clinical working group also considered a PrescQIPP CIC review, and during the
consultation more evidence was provided and an up to date evidence summary was deemed
necessary and prepared by the Specialist Pharmacy Service to inform the joint clinical working
group’s recommendations. Based on this review and non-inclusion, the lidocaine plasters are
included with defined exceptions.
Patient information leaflets:
https://www.prescqipp.info/items-which-should-not-routinely-be-prescribed-patient-leaflets
Specialist Pharmacy Service lidocaine plasters evidence review:
https://www.england.nhs.uk/medicines/items-which-should-not-be-routinely-prescribed/
Targinact (Oxycodone and Naloxone Combination Product)
Recommendation
NHS England advises CCGs that prescribers in primary care should not initiate
oxycodone and naloxone combination product for any new patient.
NHS England advises CCGs to support prescribers in deprescribing oxycodone and
naloxone combination product in all patients and, where appropriate, ensure the
availability of relevant services to facilitate this change.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 6 of 22
Date: September 2019 - Review date 2021 NHS England advises CCGs that if, in exceptional circumstances, there is a clinical
need for oxycodone and naloxone combination product to be prescribed in primary care,
this should be undertaken in a cooperation arrangement with a multi-disciplinary team
and/or other healthcare professional.
Category
Items which are clinically effective but where more cost-effective products are available,
including products that have been subject to excessive price inflation.
Annual Spend (nationally as of 2017)
£5,062,928 (NHS Digital)
Background and Rationale
Oxycodone and naloxone combination product is used to treat severe pain and can also be
used second line in restless legs syndrome. The opioid antagonist naloxone is added to
counteract opioid-induced constipation by blocking the action of oxycodone at opioid receptors
locally in the gut.
PrescQIPP CIC have issued a bulletin and did not identify a benefit of oxycodone and naloxone
in a single product over other analgesia (with laxatives if necessary).
Due to the significant cost of the oxycodone and naloxone combination product and the unclear
role of the combination product in therapy compared with individual products, the joint clinical
working group considered oxycodone and naloxone suitable for inclusion in this guidance.
Patient information leaflets:
https://www.prescqipp.info/items-which-should-not-routinely-be-prescribed-patient-leaflets
Tramacet (Paracetamol and Tramadol Combination Product)
Recommendation
NHS England advises CCGs that prescribers in primary care should not initiate
paracetamol and tramadol combination product for any new patient.
NHS England advises CCGs to support prescribers in deprescribing paracetamol and
tramadol combination product in all patients and, where appropriate, ensure the
availability of relevant services to facilitate this change.
Category
Items which are clinically effective but where more cost-effective products are available,
including products that have been subject to excessive price inflation.
Annual Spend (nationally as of 2017)
£1,980,000 (NHS Digital)
Background and Rationale
Paracetamol and tramadol combination products are more expensive than the products with the
individual components (Drug Tariff).
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 7 of 22
Date: September 2019 - Review date 2021PrescQIPP CIC also issued a bulletin which did not identify any significant advantages over
individual products; however it does recognise that some people may prefer to take one product
instead of two. There are also different strengths of tramadol (37.5mg) and paracetamol
(325mg) in the combination product compared to commonly available individual preparations of
tramadol (50mg) and paracetamol (500mg), although the PrescQIPP CIC review found no
evidence that combination product is more effective or safer than the individual preparations.
Due to the significant extra cost of a combination product, the joint clinical working group
considered paracetamol and tramadol combination products suitable for inclusion in this
guidance.
Patient information leaflets: https://www.prescqipp.info/items-which-should-not-routinely-be-
prescribed-patient-leaflets
Opioid and Gabapentinoid prescribing risks and harms
Please refer to patient information leaflets which have been recommended by the specialist
pain service within Lincolnshire and can be found in the appendices of this document; share
with patients wherever appropriate prior to prescribing;
1. ‘Risks of Opioid Medications’
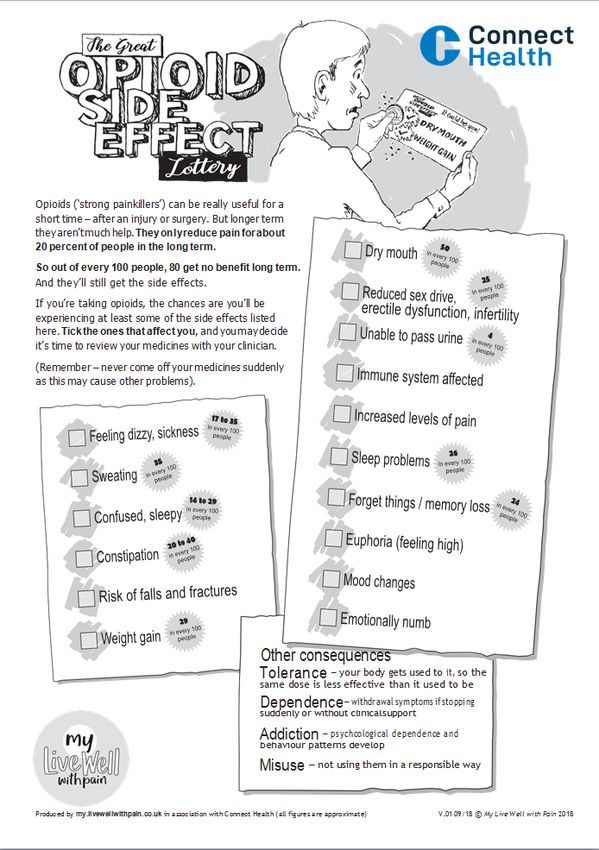
2. ‘The Great Opioid Side Effect Lottery’
3. ‘Are you taking Gabapentin or Pregabalin to help with your pain?’
For further information re opioid prescribing please refer to the following section of this
guideline. When prescribing gabapentin or pregabalin (collectively known as ‘gabapentinoids’)
the following should be considered and discussed with the patient;
5 in 10 people taking a gabapentinoid for nerve pain will not get any benefit at all
Even those who don’t get any benefit will still experience side effects
If you have pain that is not caused by nerve damage or from a change in how the nerve
works, gabapentinoids are very unlikely to be of any help to you
1 in every 3 people taking gabapentinoids will get side effects that stop them using the
medicine
There are lots of possible side effects. The most common, experienced by up to 6 in every 10
people are:
Problems with thinking clearly
Dizziness, problems walking
Tiredness
Tremors (shaking)
Weight gain, water retention or bloating
Changes in mood and emotions, includes depression
Headache or vision changes
Taking gabapentinoids with drugs like codeine and morphine (opioids) also increases the risk of
breathing problems and accidental overdose.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 8 of 22
Date: September 2019 - Review date 2021Opioid Prescribing
The following guidance has been taken from the material produced by the British Pain Society and
Faculty of Pain Medicine amongst other contributors and can be located via
https://www.rcoa.ac.uk/faculty-of-pain-medicine/opioids-aware.
General principles of good prescribing practice
Adherence to general principles of good practice in prescribing underpins pharmacologic
management of pain:
• Be up to date with clinical evidence and relevant legislation
• Prescribe within your own competence
• Prescribing decisions should be supported by best clinical evidence
• Benefits and harms of treatments should be discussed with the patient
Before initiating opioid therapy
The following guidance is taken from the Opioids Aware resource, developed collaboratively by
the British Pain Society and Faculty of Pain Medicine as well as various other contributors;
1. Opioids are very good analgesics for acute pain and for pain at the end of life but there
is little evidence that they are helpful for long term pain
2. A small proportion of people may obtain good pain relief with opioids in the long-term if
the dose can be kept low and especially if their use is intermittent (however it is difficult
to identify these people at the point of opioid initiation).
3. The risk of harm increases substantially at doses above an oral morphine equivalent of
• 120mg/day, but there is no increased benefit: tapering or stopping high dose opioids
• needs careful planning and collaboration.
•
4. If a patient has pain that remains severe despite opioid treatment it means they are not
Opioidsworking and be
should only should
usedbeasstopped,
part of aeven if no
wider other treatment
management is available.
plan that aims to improve
5.
• Chronic pain
physical is very
function, complex
reduce and ifand
disability patients have
improve refractory
quality of life.and disabling symptoms,
• particularly if they are on high dose opioids, a very detailed assessment of the many
Agree individualised treatment goals for each patient and document.
emotional influences on their pain experience is essential.
• Consider utilising an opioid prescribing contract (see opioid prescribing contract
example) between the prescriber and the patient to outline expectations and
responsibilities of both patient and prescriber.
• Opioids should not be used in isolation for the management of chronic/persistent pain -
medications should be an adjunct to strategies such as addressing common
psychological comorbidities (anxiety/depression), cognitive behavioural strategies, sleep
restoration strategies, and physiotherapy. Complete relief of symptoms is not a goal of
therapy as pain provides the body with a protective mechanism against potential or
actual damage to the body’s tissues.
• Treatment success is demonstrated by pain relief and progress towards treatment
goals. Make clear to patients that if a trial is unsuccessful then opioid treatment will be
stopped. Give realistic expectations - opioids are unlikely to give complete pain relief
Some pains do not respond to opioids.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 9 of 22
Date: September 2019 - Review date 2021Opioid trial
• For an initial opioid trial, prescribe a short (1-2 week supply) of morphine immediate
release tablets or liquid. The patient may explore different doses within a specified
range e.g. morphine 5-10mg. If reduction in pain is not achieved following a single dose
of morphine 20mg, opioids are unlikely to be beneficial in the long term.
• Initial positive outcomes do not predict outcomes in the longer term. A small proportion
of patients may do well with opioids in the long term if the dose can be kept low and
particularly if use is intermittent.
• A trial period of FOUR weeks is adequate.
Opioid Prescribing
• Be clear who is responsible for prescribing.
• Discuss alternative strategies for exacerbations of pain such as cognitive behavioural
strategies, sleep restoration strategies, and physiotherapy. ‘Short acting’ opioids e.g.
Oramorph are not appropriate for the majority of patients.
• Ensure that the dosing instructions are clear. The instructions for “as required” opioids
must include a maximum daily dose. “As directed” is not acceptable.
• It is not recommended that any two opioids be prescribed together. If a particular opioid
has failed to achieve treatment goals, it is unlikely that another will work.
• Sedation and cognitive impairment with opioids has important relevance for
concentration-critical activities, particularly driving:
Opioids and driving
• See https://www.gov.uk/drug-safety-update/drugs-and-driving-blood-concentration-
limits-to-be-set-for-certain-controlled-drugs-in-a-new-legal-offence for official DVLA
guidance
• It remains illegal in England and Wales to drive when taking prescription medicines if the
medication impairs a patient’s ability to drive
• The new offence refers to driving with a specified controlled drug in the body, in excess
of a specified limit
• The drugs include licensed medicines, including morphine and methadone but not other
opioids. The specified limits are generally above the normal therapeutic range so most
patients prescribed these drugs are unlikely to be driving with a concentration of a
specified drug in their body above the specified limit.
• The new offence has a statutory “medical defence” to protect patients who may test
positive for certain specified drugs taken in accordance with the advice of a healthcare
professional or the patient information leaflet that accompanies the medicine
• It remains the responsibility of all drivers, including patients, to consider whether they
believe their driving may be impaired on every occasion when they drive
• Drivers who tested positive for morphine were between 8 and 32 times more likely to be
injured or responsible for a road traffic collision compared with those who did not have a
positive test result.
• A patient on high dose morphine (around 200mg/24hours) could be as impaired as
someone with blood alcohol around the level above which it is illegal to drive.
• A patient also drinking or taking other sedative drugs could be impaired at a lower
morphine dose.
• Patients should be aware that during the period following dose adjustment (up or down)
they may be particularly vulnerable to impairment.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 10 of 22
Date: September 2019 - Review date 2021• Prescribers of opioid medicines must be aware of the likely impairing effects of the
drugs and must advise patients accordingly.
• Although this legislation will particularly impact on patients taking morphine, prescribers
should be aware that equi-analgesic doses of other opioids are likely to be equivalently
impairing.
• Prescribers should also advise patients of the potentially distracting effects of pain, and
other co-morbidities such as fatigue and poor sleep in relation to driving
• Discussions in relation to drugs and driving must be clearly documented in the medical
notes and a copy given to the patient.
Opioid Monitoring
Review patients prescribed opioids regularly. Initially review at least monthly, more often if there
are concerns. If the patient is not progressing towards agreed outcomes, taper their opioid dose
and consider alternative strategies.
When the patient achieves their treatment goals on a stable dose, monitor at least biannually.
Opioid equivalences (read all points below before changing opioids)
• When converting from one opioid to another, the initial dose depends on the relative
potency of the two drugs and route of administration.
• An individualised approach is necessary.
• Conversion factors are an approximate guide only because comprehensive data are
lacking and there is significant inter-individual variation.
• In most cases, when switching between different opioids, the calculated dose-equivalent
must be reduced to ensure safety. The starting point for dose reduction from the
calculated equi-analgesic dose is around 25-50%.
• A dose reduction of at least 50% is recommended when switching at high doses (eg,
oral morphine or equivalent doses of 500mg/24 hours or more), in elderly or frail
patients, or because of intolerable undesirable effects.
• The half-life and time to onset of action of the two drugs needs to be considered when
converting so that the patient does not experience breakthrough pain or receive too
much opioid during the conversion period.
• Once the conversion has occurred, the dose of new opioid should be titrated carefully
according to individual response and the patient monitored closely for side effects and
efficacy, especially when switching at high doses.
• Withdrawal symptoms (e.g, sweating, yawning and abdominal cramps, restlessness,
anxiety) occur if an opioid is stopped/dose reduced abruptly.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 11 of 22
Date: September 2019 - Review date 2021Approximate equi-analgesic potencies of opioids for oral
administration from;
(https://www.rcoa.ac.uk/faculty-of-pain-medicine/opioids-aware/structured-approach-to-prescribing/dose-
equivalents-and-changing-opioids)
Potency ratio with oral Equivalent dose to 10mg
morphine oral morphine
Codeine phosphate 0.1 100mg
Dihydrocodeine 0.1 100mg
Hydromorphone 7.5 1.3mg
Methadone * *
Morphine 1 10mg
Oxycodone 2 5mg
Tapentadol 0.4 25mg
Tramadol 0.15 67mg
*The relative potency of methadone depends on the starting dose and the duration of
administration. Conversions to and from methadone should always be undertaken with specialist
advice
Transdermal preparations
Fentanyl – transdermal patches changed at 3 day (72hour) intervals
Fentanyl patch strength (microgram/hr) Oral morphine (mg/day)
12 microgram/hr 45 mg
25 microgram/hr 90 mg
50 microgram/hr 180 mg
75 microgram/hr 270 mg
100 microgram/hr 360 mg
300 microgram/hr 1120 mg
Buprenorphine – transdermal buprenorphine changed at 7 day (weekly) intervals
5 microgram/hr 10 microgram/hr 20 microgram/hr
Codeine 120 240
Tramadol 100 200 400
Morphine 12 24 48
Buprenorphine – transdermal buprenorphine changed every three or four days (twice
weekly)
35 micrograms/hr 52 micrograms/hr 70 micrograms/hr
Morphine 84 126 168
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 12 of 22
Date: September 2019 - Review date 2021Tapering and stopping opioids
It is important to taper or stop the opioid regimen if:
• the medication is not providing useful pain relief. The dose above which harms outweigh
benefits is 120mg oral morphine equivalent/24hours. Increasing opioid load above this dose
is unlikely to yield further benefits but exposes the patient to increased harm
• the underlying painful condition resolves
• the patient receives a definitive pain relieving intervention (eg, joint replacement)
• the patient develops intolerable side effects
• there is strong evidence that the patient is diverting his/her medications to others
Preparation for dose reduction includes:
• explanation of the rationale for stopping opioids including the potential benefits of opioid
reduction (avoidance of long term harms and improvement in ability to engage in self-
management strategies)
• agreeing outcomes of opioid tapering
• deciding which patients may need admission for opioid taper/cessation informed by existing
opioid dose
• physical co-morbidities
• mental health co-morbidities including significant emotional trauma
• monitoring during taper of pain
• symptoms and signs of opioid withdrawal
• choice of opioid reduction scheme
• incremental taper of existing drug
• conversion to methadone or buprenorphine
• defining the role of drug and alcohol services to support dose reduction
• close collaboration between the patient, his or her carers and all members of the patient's
health care team
• arrangements for follow-up including agreed prescribing responsibilities
The dose of drug can be tapered by 10% weekly or two weekly.
Stopping opioids in primary care
The decision to taper/stop an established opioid regimen needs to be discussed carefully with the
patient including:
• explanation of the rationale for stopping opioids including the potential benefits of opioid
reduction (avoidance of long term harms and improvement in ability to engage in self-
management strategies)
• agreeing outcomes of opioid tapering
• arrangements for monitoring and support during opioid taper
• documented agreement of tapering schedule
Stopping opioids in collaboration with specialist services
Patients who are failing to derive benefit from large doses of opioids (greater than oral morphine
equivalent of around 300mg/day) may need support from specialist services in order to reduce
medication.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 13 of 22
Date: September 2019 - Review date 2021This must include detailed exploration of emotional and mental health history (including addiction).
Opioid tapering/cessation when patients are taking high doses is more likely to succeed if patients’
emotional and mental health needs are identified and an appropriate plan for support established.
Points to discuss with patients when de-prescribing
Remain empathic and focus the discussion on medicines only
• Take a full medicines history and ask the patient how well the medicines are working, and
reflect that the patient is describing severe pain despite medicines
• Share that the experience of many patients is that taking medicines results in no
observable benefit for pain
• Explain that we have much better ways of working out how helpful medicines really are and
we know that a lot of things that we thought were helpful in the past have proved to be
disappointing and take responsibility for contributing to where we are now!
• Medicines for pain can be associated with significant harm
• It matters a lot that the patient has confidence that all their medicines are working well
• Usually stopping medicines makes no difference to the pain but can make people feel
better
• If a tapering trial doesn't work we can think again
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 14 of 22
Date: September 2019 - Review date 2021Opioid prescribing contract example
Why do I need to sign a treatment contract?
A treatment contract is used so that your doctor is sure that you understand what is
expected from you whilst you take this type of medicine, and that you consent to the
requirements described in this contract.
Patient name:
Address:
Date of birth:
PLEASE COMPLETE ALL DETAILS
I, ………………………………..understand that …………………. (a strong opioid ) is to be
prescribed to me in an attempt to improve my level of functioning and reduce my pain. My
medical practitioner and I have discussed that strong opioid (morphine-like) medicines may
only be partially helpful in achieving this goal and on occasion will not help at all. I
understand that an opioid medicine is only one part of the management of my chronic pain.
My medical practitioner and I agree to the following conditions regarding my treatment and
the prescribing of an opioid medicine for my pain:
1. My medical practitioner is responsible for prescribing a safe and effective dose of an
opioid medicine. I will not use an opioid medicine other than at the dose prescribed
and I will discuss any changes in my dose with my medical practitioner. Finding the
right dose of opioid will mean having regular appointments with your doctor, to assess
any benefit or problem.
2. Whilst most people do not have any serious problems with this type of medicine when
used as directed, there can be side effects. My medical practitioner has explained the
main ones to me, and I will tell him or her if I experience what could be side effects.
3. Dependence or addiction to prescription pain killers is estimated to occur in 1 in 20
patients.
4. As possible dependence is important in the management of my pain, I have informed
my medical practitioner of any present or past dependence on alcohol or drugs that I
may have had, and of any illegal activity related to any drugs (including prescriptions
medicines) that I may have been involved in.
5. If there are concerns that the medication is not used properly as prescribed and there
are issues of safety to children the prescriber may discuss this case with other non
NHS agencies.
6. My medical practitioner respects my right to participate in decisions about my pain
management and will explain the risks & benefits of any treatment. My medical
practitioner and I will work together to improve my level of functioning and reduce my
pain.
7. I understand that my medical practitioner may stop prescribing my opioid medicine or
change the treatment plan if my level of activity has not improved, if I do not show a
significant reduction in my pain, or if I fail to comply with any of the conditions listed
above.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 15 of 22
Date: September 2019 - Review date 20218. I am responsible for the security of my opioid medicine. Lost or misplaced medicines or
prescriptions for opioid medicines will not be replaced.
9. I will only obtain my opioid medicine from the medical practitioner who signs this
contract, or other doctors in the same practice authorised to prescribe to me. I
understand that no early prescriptions will be provided.
Patient’s signature:
Patient’s name:
Date:
Medical practitioner’s signature:
Medical practitioner’s name:
Please provide a copy of the signed contract to the patient.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 16 of 22
Date: September 2019 - Review date 2021Patient information leaflets Risks of Opioid Medications OPTUM Lincolnshire Primary Care Pain Management Guidance V1.0 Page 17 of 22 Date: September 2019 - Review date 2021
OPTUM Lincolnshire Primary Care Pain Management Guidance V1.0 Page 18 of 22 Date: September 2019 - Review date 2021
Opioid side effects OPTUM Lincolnshire Primary Care Pain Management Guidance V1.0 Page 19 of 22 Date: September 2019 - Review date 2021
Gabapentinoid prescribing risks
If you answered YES to any of these questions,
please turn over...
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 20 of 22
Date: September 2019 - Review date 2021Gabapentin and pregabalin – known as ‘gabapentinoids’ – are used to help with persistent pain (pain that
has lasted longer than three months) caused by damaged or malfunctioning nerves. It is often described as
burning, shooting, electric shocks or pins and needles. If you are experiencing persistent pain and
answered ‘yes’ to any of the questions overleaf, then read on...
How effective are gabapentinoids? Are they the right treatment for me?
• 5 in every 10 people taking a gabapentinoid for • Has your pain reduced since starting or
nerve pain will not get any benefit at all increasing the dose of the gabapentinoid?
• Even those who don’t get any benefit will • Are you doing more or recovering faster from
still experience side effects activity than before you started taking the
• If you have pain that is not caused by nerve medicine?
damage or from a change in how the nerve works, If you do not think the medicines are helping, then you
gabapentinoids are very unlikely to be of any are probably better off trying to slowly reducing them,
help to you with the support of your healthcare team.
• 1 in every 3 people taking gabapentinoids will
Even people who think they might be better using a
get side effects that stop them using the
gabapentinoid should reduce the dose from time to
medicine
time, to see if the medicines really are helping or if they
get the same benefit on a smaller dose.
What about the side effects?
There are lots of possible side effects. So how do I reduce them?
The most common, experienced by up to 6 in
Gabapentinoids should always be reduced slowly and
every 10 people are:
with support. You may need to have different strengths
• Problems with thinking clearly of capsules/tablets to enable you to do this.
• Dizziness, problems walking
• Tiredness Please make an appointment with a member
• Tremors (shaking) of our healthcare team to discuss making
• Weight gain, water retention or bloating changes to your gabapentinoid medicines.
• Changes in mood and emotions, includes
depression
• Headache or vision changes
Taking gabapentinoids with drugs like codeine
and morphine also increases the risk of
breathing problems and accidental overdose.
Are there other ways of managing my pain apart from medicines?
Yes! There are lots of new approaches to pain relief apart from medicines. These
new approaches to pain self-management are helping people regain a better quality
of life. Many of these are things you can do yourself. GPs and pain specialists are
increasingly supporting patients to adopt these new ways to manage their
persistent pain.
To find out more, go to www.my.livewellwithpain.co.uk or www.paintoolkit.org and check out some of the
ideas and techniques. We can help you with these. If you’d like to know more, talk to our healthcare team.
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0 Page 21 of 22
Date: September 2019 - Review date 2021Authors:
James Musk – Clinical Pharmacist, Medicines Management & Optimisation Team,
Optum Health Services Solutions
Helen Liddell – Consultant Pharmacist, Connect Health Community Pain Management
Services
Authorised for use within Primary Care and Community Services across Lincolnshire by
Lincolnshire Prescribing and Clinical Effectiveness Forum (PACEF).
Produced by:
Medicines Management & Optimisation Service
Optum Health Systems Support
November 2019
T 020 7121 0560 l E info@optum.co.uk l optum.co.uk
10th Floor, 5 Merchant Square, Paddington, London, W2 1AS
®
Optum is a registered trademark of Optum, Inc. in the U.S. and other jurisdictions
OPTUM
Lincolnshire Primary Care Pain Management Guidance V1.0
Date: September 2019 - Review date 2021 Page 22 of 22You can also read

















































