Liver trauma: WSES 2020 guidelines
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Coccolini et al. World Journal of Emergency Surgery (2020) 15:24
https://doi.org/10.1186/s13017-020-00302-7
REVIEW Open Access
Liver trauma: WSES 2020 guidelines
Federico Coccolini1*, Raul Coimbra2, Carlos Ordonez3, Yoram Kluger4, Felipe Vega5, Ernest E. Moore6, Walt Biffl7,
Andrew Peitzman8, Tal Horer9,36, Fikri M. Abu-Zidan10, Massimo Sartelli11, Gustavo P. Fraga12, Enrico Cicuttin1,
Luca Ansaloni13, Michael W. Parra14, Mauricio Millán3, Nicola DeAngelis15, Kenji Inaba16, George Velmahos17,
Ron Maier18, Vladimir Khokha19, Boris Sakakushev20, Goran Augustin21, Salomone di Saverio22, Emanuil Pikoulis23,
Mircea Chirica24, Viktor Reva25, Ari Leppaniemi26, Vassil Manchev27, Massimo Chiarugi1, Dimitrios Damaskos28,
Dieter Weber29, Neil Parry30, Zaza Demetrashvili31, Ian Civil32, Lena Napolitano33, Davide Corbella34,
Fausto Catena35 and the WSES expert panel
Abstract
Liver injuries represent one of the most frequent life-threatening injuries in trauma patients. In determining the
optimal management strategy, the anatomic injury, the hemodynamic status, and the associated injuries should be
taken into consideration. Liver trauma approach may require non-operative or operative management with the
intent to restore the homeostasis and the normal physiology. The management of liver trauma should be
multidisciplinary including trauma surgeons, interventional radiologists, and emergency and ICU physicians. The aim
of this paper is to present the World Society of Emergency Surgery (WSES) liver trauma management guidelines.
Keywords: Liver trauma, Adult, Pediatric, Minor, Moderate, Severe, Classification, Guidelines, Surgery, Hemorrhage,
Operative management, Non-operative management, Interventional, Radiology, Intensive care
Background trauma centers. This advanced strategy necessitates a
Liver trauma is one of the most common abdominal le- multidisciplinary approach to deal with the complexity
sions in severely injured trauma patients [1]. Diagnosis of moderate and severe liver injury. The majority of pa-
and treatment of hepatic trauma has evolved with the tients admitted with liver injuries have minor or moder-
use of modern diagnostic and therapeutic tools [2–4]. ate injuries (WSES I, II, III) (AAST-OIS I, II, or III) and
Until two to three decades ago, most cases with blunt are successfully treated by NOM. In contrast, one third
abdominal trauma and possible injury in parenchymat- of severe injuries (WSES IV, V) (AAST-OIS IV, V) allow
ous organs were managed by exploratory laparotomy [5]. for NOM [6]. In pediatric patients, NOM should be con-
Several innovative multimodal approaches as EVTM sidered the optimal management approach. In determin-
(endovascular trauma and bleeding management) have ing the optimal treatment strategy, the anatomical
allowed to greatly increase the likelihood of non- description of liver lesions is fundamental but not suffi-
operative management (NOM) for selected patients. cient. In fact, the decision whether patients need to be
Nowadays, even borderline patients or transient re- managed operatively or undergo NOM is based mainly
sponder, without other indications for laparotomy, may on the hemodynamic status, associated injuries, and on
be considered for NOM in selected and well-developed the anatomical liver injury grade.
The aim of this manuscript is to present the updated
World Society of Emergency Surgery (WSES) liver
* Correspondence: federico.coccolini@gmail.com
1 trauma management guidelines.
General, Emergency and Trauma Surgery Department, Pisa University
Hospital, Via Paradisia 1, 56100 Pisa, Italy
Full list of author information is available at the end of the article
© The Author(s). 2020 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.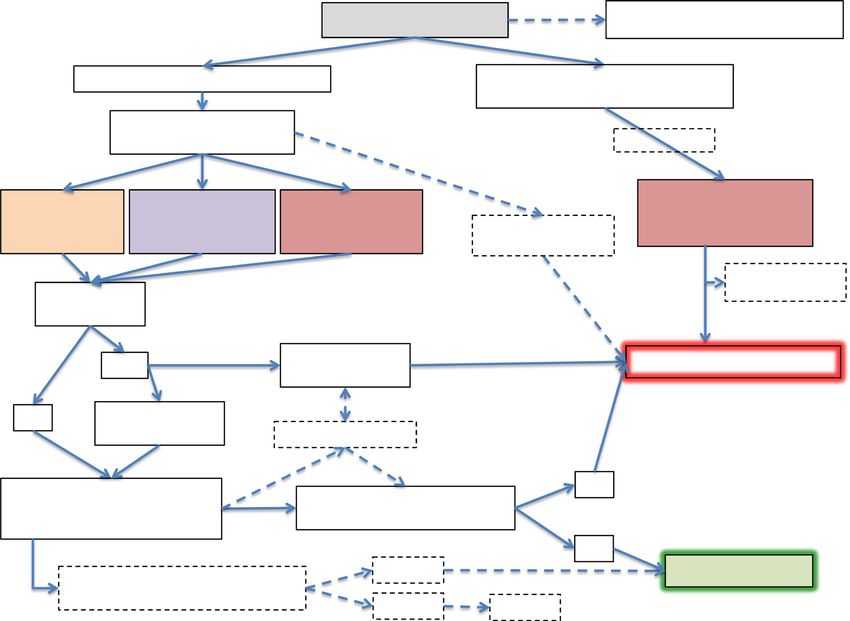
Coccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 2 of 15
Notes on the use of the guidelines Definitions
The guidelines are evidence-based, with the grade of rec- In adult patients, hemodynamic instability is considered
ommendation based on the evidence. The guidelines the condition in which admission systolic blood pressure
present the diagnostic and therapeutic methods for opti- is < 90 mmHg with clinical evidence of hemorrhagic
mal management of liver trauma. The practice guide- shock with skin vasoconstriction (cool, clammy, de-
lines promulgated in this work do not represent a creased capillary refill), altered level of consciousness
standard of practice. These are suggested plans of care, and/or shortness of breath, or > 90 mmHg but requiring
based on best available evidence and the consensus of bolus infusions/transfusions and/or vasopressor drugs
experts, but they do not exclude other approaches as be- and/or admission base excess (BE) > -5 mmol/l or trans-
ing within the standard of practice. For example, they fusion requirement of at least > 4 units of packed red
should not be used to compel adherence to a given blood cells within the first 8 h. Transient responder pa-
method of medical management, which method should tients (adult and pediatric) are those showing an initial
be finally determined after taking account of the condi- response to adequate fluid resuscitation, but then subse-
tions at the relevant medical institution (staff levels, ex- quent signs of ongoing blood loss and perfusion deficits.
perience, equipment, etc.), and the characteristics of the These patients have an initial response to therapy but do
individual patient. However, responsibility for the results not reach sufficient stabilization to undergo endovascu-
of treatment rests with those who are directly engaged lar procedures or NOM.
therein, and not with the consensus group. In pediatric patients, hemodynamic stability is consid-
ered a systolic blood pressure of 70 mmHg plus twice
Methods the child’s age in years. An acceptable hemodynamic sta-
A computerized search was done by the bibliographer in tus in children is considered a positive response to fluid
different databanks (MEDLINE, Scopus, EMBASE). resuscitation: 2 boluses of 20 mL/kg of crystalloid re-
Citations were included for the period between January placement should be administered before blood replace-
1990 and October 2019 using the primary search strat- ment leading to heart rate reduction, cleared sensorium,
egy: liver, injuries, trauma, hepatic, adult, pediatric, return of peripheral pulses, normal skin color, increase
hemodynamic instability/stability, angioembolization, in blood pressure and urinary output, and an increase in
management, nonoperative, conservative, operative, sur- warmth of the skin in the extremities. Clinical judgment
gery, diagnosis, and follow-up, combined with AND/OR. however is fundamental in evaluating pediatric patients.
No search restrictions were imposed. The dates were se-
lected to allow comprehensive published abstracts of WSES classification
clinical trials, consensus conference, comparative studies, The WSES classification (Table 2) divides liver injuries
congresses, guidelines, government publication, multi- into four classes considering the AAST-OIS classifica-
center studies, systematic reviews, meta-analysis, large tion (Table 3) and the hemodynamic status (Table 4):
case series, original articles, and randomized controlled
trials. Case reports and small case series were excluded. Minor (WSES grade I)
Narrative review articles were also analyzed to determine Moderate (WSES grade II)
if other cited studies should be included. Severe (WSES grade III and IV)
The level of evidence (LE) was evaluated using the
GRADE system [7] (Table 1). Minor hepatic injuries:
A group of experts in the field coordinated by a cen-
tral coordinator was contacted to express their evidence- WSES grade I includes AAST-OIS grade I–II
based opinion on several issues about the pediatric (< hemodynamically stable lesions.
16 years old) and adult liver trauma [8, 9]. Hepatic
trauma was assessed by the anatomy of the injury, type Moderate hepatic injuries:
of injury (blunt and penetrating injury), management
(conservative and operative management), and type of WSES grade II includes AAST-OIS grade III
patient (adults, pediatrics). Through the Delphi process, hemodynamically stable lesions.
different issues were discussed in subsequent rounds.
The central coordinator assembled the different answers Severe hepatic injuries:
derived from each round. Each version was then revised
and improved. An expert group discussed the definitive WSES grade III includes AAST-OIS grade IV–V
version. The final version about on agreement was hemodynamically stable lesions.
reached resulted in the present manuscript. Statements WSES grade IV includes AAST-OIS grade I–VI
are summarized in Table 4. hemodynamically unstable lesions.Table 1 GRADE system to evaluate the level of evidence and recommendation
Grade of recommendation Clarity of risk/benefit Quality of supporting evidence Implications
1A
Strong recommendation, high-quality Benefits clearly outweigh risk and burdens, RCTs without important limitations or overwhelming Strong recommendation, applies to most
evidence or vice versa evidence from observational studies patients in most circumstances without
reservation
1B
Coccolini et al. World Journal of Emergency Surgery
Strong recommendation, moderate-quality Benefits clearly outweigh risk and burdens, RCTs with important limitations (inconsistent results, Strong recommendation, applies to most
evidence or vice versa methodological flaws, indirect analyses, or imprecise patients in most circumstances without
conclusions) or exceptionally strong evidence from reservation
observational studies
1C
(2020) 15:24
Strong recommendation, low-quality or very Benefits clearly outweigh risk and burdens, Observational studies or case series Strong recommendation but subject to
low-quality evidence or vice versa change when higher quality evidence
becomes available
2A
Weak recommendation, high-quality evidence Benefits closely balanced with risks and RCTs without important limitations or overwhelming Weak recommendation, best action may
burden evidence from observational studies differ depending on the patient, treatment
circumstances, or social values
2B
Weak recommendation, moderate-quality Benefits closely balanced with risks and RCTs with important limitations (inconsistent results, Weak recommendation, best action may
evidence burden methodological flaws, indirect, or imprecise) or differ depending on the patient, treatment
exceptionally strong evidence from observational studies circumstances, or social values
2C
Weak recommendation, low-quality or very Uncertainty in the estimates of benefits, risks, Observational studies or case series Very weak recommendation; alternative
low-quality evidence and burden; benefits, risk, and burden may be treatments may be equally reasonable
closely balanced and merit consideration
Page 3 of 15Coccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 4 of 15
Table 2 WSES liver trauma classification falsely negative due to clotted blood or suboptimal qual-
WSES grade AAST Hemodynamic ity views [11–13]. In the pediatric population, reported
Minor WSES grade I I–II Stable sensitivity and specificity ranges from 42 to 52% and 96
Moderate WSES grade II III Stable
to 98%, with a negative predicting value for intra-
abdominal fluid of 93–96% [8, 9, 14–16]. The low sensi-
Severe WSES grade III IV–V Stable
tivity of E-FAST in hemodynamically stable pediatric pa-
WSES grade IV I–VI Unstable tients may warrant further investigation, specifically
contrast-enhanced ultrasound (US) or abdomen/pelvis
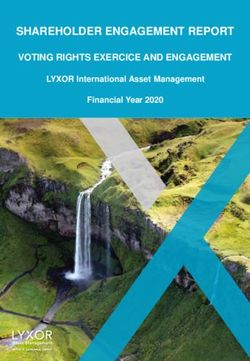
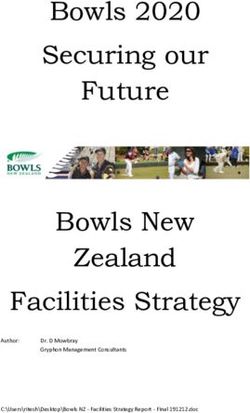
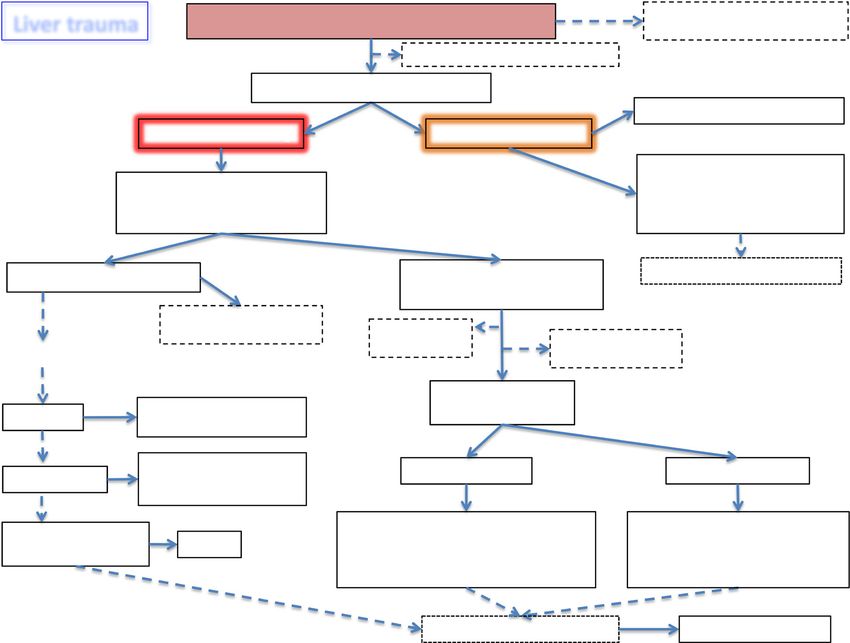
Based on the present classification, we suggest two CT scan or magnetic resonance, in hemodynamically
management algorithms: one general (Fig. 1) and one stable pediatric patients with a high degree of suspicion
specifically dedicated to hemodynamically unstable pa- for intra-abdominal injury (abnormal physical examin-
tients (Fig. 2). ation, abnormal laboratory values, or other radiologic
studies).
Diagnosis Computed tomography (CT) scan is considered the
gold standard in trauma imaging assessment with a sen-
The diagnostic methods on admission are sitivity and specificity approaching 96–100% [17–19].
determined by the hemodynamic status (GoR 1A). CT must be immediately available and performed only
Extended-focused abdominal sonography for trauma in hemodynamically stable or stabilized patients or in
(E-FAST) is rapid in detecting intra-abdominal free those who transiently responded to fluid resuscitation in
fluid (GoR 1A). special circumstances and under the supervision of the
CT scan with intravenous contrast is the gold trauma team [20, 21]. Delayed-phase CT helps in differ-
standard in hemodynamically stable trauma patients entiating patients with active bleeding from those with
(GoR 1A). contained vascular injuries [22]. This data is important
to reduce the risk of discrepancy between CT scan im-
Careful physical examination is of paramount import- ages and angiographic images (only 47% of patients have
ance in determining the need for exploratory laparotomy a confirmation of the CT findings at angiography) [22].
[10]. E-FAST is useful and generally reliable in trauma Active contrast extravasation is a sign of active
in general. However, abdominal ultrasound may be hemorrhage [23]. CT scan may help in subsequent
Table 3 AAST liver trauma classificationCoccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 5 of 15
Table 4 Statements summary
Statements
Diagnostic procedures - The diagnostic methods on admission are determined by the hemodynamic status (GoR 1A).
- E-FAST is rapid in detecting intra-abdominal free fluid (GoR 1A).
- CT scan with intravenous contrast is the gold standard in hemodynamically stable trauma patients (GoR 1A).
Non-operative management - NOM should be the treatment of choice for all hemodynamically stable minor (WSES I) (AAST I–II), moderate
(NOM) (WSES II) (AAST III), and severe (WSES III) (AAST IV–V) injuries in the absence of other internal injuries requiring
surgery (GoR 2A).
- In patients considered transient responders with moderate (WSES II) (AAST III) and severe (WSES III) (AAST IV–V)
injuries, NOM should be considered only in selected settings provided the immediate availability of trained
surgeons, operating room, continuous monitoring ideally in an ICU or ER setting, access to angiography,
angioembolization, blood and blood products, and in locations where a system exists to quickly transfer such
patients to higher level of care facilities (GoR 2B).
- A CT scan with intravenous contrast should always be performed in patients being considered for NOM (GoR 2A).
- AG/AE may be considered as a first-line intervention in hemodynamically stable patients with arterial blush on CT
scan (GoR 2B).
- In hemodynamically stable children, the presence of contrast blush on CT scan is not an absolute indication for
AG/AE (GoR 2B).
- Serial clinical evaluations (physical exams and laboratory testing) must be performed to detect a change in clinical
status during NOM (GoR 2A).
- NOM should be attempted in the setting of concomitant head trauma and/or spinal cord injuries with reliable
clinical exam, unless the patient could not achieve specific hemodynamic goals for the neurotrauma and the
instability might be due to intra-abdominal bleeding (GoR 2B).
- Intensive care unit admission in isolated liver injury may be required only for moderate (WSES II) (AAST III) and
severe (WSES III) (AAST IV–V) lesions (GoR 2B).
- In selected cases where an intra-abdominal injury is suspected in the days after the initial trauma, interval
laparoscopic exploration may be considered as an extension of NOM and a means to plan patient management
in a step-up treatment strategy (GoR 2C).
- In low-resource settings, NOM could be considered in patients with hemodynamic stability without evidence of
associated injuries, with negative serial physical examinations and negative imaging and blood tests (GoR 2C).
Operative management (OM) - Hemodynamically unstable and non-responder patients (WSES IV) should undergo OM (GoR 2A).
- Primary surgical intention should be to control the hemorrhage and bile leak and initiation of damage control
resuscitation as soon as possible (GoR 2A).
- Major hepatic resections should be avoided at first and only considered in subsequent operations, in a resectional
debridement fashion in cases of large areas of devitalized liver tissue done by experienced surgeons (GoR 2B).
- Angioembolization is a useful tool in case of persistent arterial bleeding after non-hemostatic or damage control
procedures (GoR 2A).
- Resuscitative endovascular balloon occlusion of the aorta (i.e., REBOA) may be used in hemodynamically unstable
patients as a bridge to other more definitive procedures for hemorrhage control (GoR 2B).
Short- and long-term - Intrahepatic abscesses may be successfully treated with percutaneous drainage (GoR 2A).
follow-up - Delayed hemorrhage without severe hemodynamic compromise may be managed at first with AG/AE (GoR 2A).
- Hepatic artery pseudoaneurysm should be managed with AG/AE to prevent rupture (GoR 2A).
- Symptomatic or infected bilomas should be managed with percutaneous drainage (GoR 2A).
- Combination of percutaneous drainage and endoscopic techniques may be considered in managing post-traumatic
biliary complications not suitable for percutaneous management alone (GoR 2B).
- lavage/drainage and endoscopic stenting may be considered as the first approach in delayed post-traumatic biliary
fistula without any other indication for laparotomy (GoR 2B).
- Laparoscopy as initial approach should be considered in cases of delayed surgery, so as to minimize the invasiveness
of surgical intervention and to tailor the procedure to the lesion (GoR 2B).
Thrombo-prophylaxis, feeding, - Mechanical prophylaxis is safe and should be considered in all patients with no absolute contraindication (GoR 2A).
and mobilization - LMWH-based prophylaxis should be started as soon as possible following trauma and may be safe in selected
patients with liver injury treated with NOM (GoR 2B).
- In those patients taking anticoagulants, individualization of the risk-benefit balance of anticoagulant reversal is
suggested (GoR 1C).
- Early mobilization should be achieved in stable patients (GoR 2A).
- In the absence of contraindications, enteral feeding should be started as soon as possible (GoR 2A).
surgical procedures and angiography/angioembolization fluid without solid organ injury in a hemodynamically
(AG/AE) [24–32]. stable patient. The possibility of DPL-related complica-
Diagnostic peritoneal lavage (DPL) should be consid- tions (up to 2%) should be considered [33].
ered diagnostic modality in low-resource settings, where
CT scan or US is not promptly available [33]. It should Non-operative management
be considered in the presence of massive subcutaneous
emphysema in a shocked patient in whom ultrasound NOM should be the treatment of choice for all
cannot be done and/or in the presence of free peritoneal hemodynamically stable minor (WSES I) (AAST I–Coccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 6 of 15
Fig. 1 Liver trauma management algorithm (SW: stab wound. Number sign indicates wound exploration near the inferior costal margin should
be avoided if not strictly necessary. Asterisk indicates angioembolization should be always considered for adults, only in selected patients and in
selected centers for pediatrics)
II), moderate (WSES II) (AAST III), and severe In hemodynamically stable children, the presence of
(WSES III) (AAST IV–V) injuries in the absence of contrast blush on CT scan is not an absolute
other internal injuries requiring surgery (GoR 2A). indication for AG/AE (GoR 2B).
In patients considered transient responders with Serial clinical evaluations (physical exams and
moderate (WSES II) (AAST III) and severe (WSES laboratory testing) must be performed to detect a
III) (AAST IV–V) injuries, NOM should be change in clinical status during NOM (GoR 2A).
considered only in selected settings provided the NOM should be attempted in the setting of
immediate availability of trained surgeons, operating concomitant head trauma and/or spinal cord
room, continuous monitoring ideally in an ICU or injuries with reliable clinical exam, unless the patient
ER setting, access to angiography, could not achieve specific hemodynamic goals for
angioembolization, blood, and blood products, and the neurotrauma and the instability might be due to
in locations where a system exists to quickly transfer intra-abdominal bleeding (GoR 2B).
such patients to higher level of care facilities (GoR Intensive care unit admission in isolated liver injury
2B). may be required only for moderate (WSES II)
A CT scan with intravenous contrast should always (AAST III) and severe (WSES III) (AAST IV–V)
be performed in patients being considered for NOM lesions (GoR 2B).
(GoR 2A). In selected cases where an intra-abdominal injury
AG/AE may be considered as a first-line interven- is suspected in the days after the initial trauma,
tion in hemodynamically stable patients with arterial interval laparoscopic exploration may be consid-
blush on CT scan (GoR 2B). ered as an extension of NOM and a means toCoccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 7 of 15
Fig. 2 Hemodynamically unstable liver trauma management algorithm (DCS: damage control surgery, ICU: intensive care unit,
REBOA-C: REBOA-cava)
plan patient management in a step-up treatment surgeons, CT scanning, angiography, OR, and blood and
strategy (GoR 2C). blood products) [16, 40–44].
In low-resource settings, NOM could be considered As a general consideration, great attention should be
in patients with hemodynamic stability without evi- paid in selecting PT for NOM especially in the case of
dence of associated injuries, with negative serial gunshot wound (GSW) and even more if thoraco-
physical examinations and negative imaging and abdominal. They should be considered for NOM only in
blood tests (GoR 2C). centers with experience in dealing with PT. Even in pa-
tients presenting with stable conditions and with no evi-
Absolute requirements for NOM are hemodynamic dence of other intra-abdominal/internal injuries, interval
stability and absence of other lesions requiring surgery laparoscopy should be always considered in order to
[9, 15, 34–39]. In hemodynamically stable patients with- confirm the absence of other injuries requiring surgical
out other associated injuries requiring OM, NOM is repair.
considered the standard of care [8, 14, 15]. The concept In PT, NOM feasibility has been reported [35–37, 45–
is valid for both: blunt (BT) and penetrating trauma 49] with 50% and 85% success rate of NOM for stab
(PT). Attempting NOM in moderate (WSES II) (AAST- wounds (SW) in anterior and posterior abdomen re-
OIS III) and severe (WSES III) (AAST-OIS IV–V) blunt spectively [34, 50]. Similar managing strategy can be ap-
or penetrating injuries requires the ability to diagnose all plied to GSWs [35, 45]. Necessary distinction between
associated injuries and to provide intensive management low- and high-energy penetrating trauma however is
(continuous clinical monitoring, serial hemoglobin mon- mandatory when deciding for OM or NOM. Low-energy
itoring, and around-the-clock availability of trained PT (SW and low-energy GSW) may be safely treatedCoccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 8 of 15 with NOM at first, provided the patient is In children, the use of primary hepatic AE has been re- hemodynamically stable and no other injuries require ported rarely and is debated even in the presence of ar- surgery. In considering NOM, interval laparoscopy terial blush where it seems to increase NOM failure should be considered to rule out missed intra-abdominal rates [55], or according to some studies, it does not cor- injuries. High-energy GSW and other ballistic injuries relate with decrease odds of laparotomy [30]. In the are less amenable to NOM, and in 90% of cases, OM is pediatric population, AE use is associated with older age required [34, 36, 51]. In abdominal GSWs, up to 25% of and is not completely defined in terms of efficacy and non-therapeutic laparotomy has been reported [51], con- cost-effectiveness, especially in low-resource settings [30, firming the need to have strict selection criteria for OM 55–61]. Some authors, however, identify the presence of or NOM even in the GSW cohort. Associated head and active contrast extravasation as an independent predictor spinal cord injuries (that preclude affordable clinical for pseudoaneurysm (PSA) formation in children, re- examination) and significant reduction in hemoglobin gardless of injury grade. This suggests a thorough requiring > 4 units of blood transfusion in the first 8 h follow-up during NOM of these patients, so to obtain an [34, 45] have been suggested as predictive criteria of early identification and angiographic treatment of PSA NOM failure in abdominal GSWs. [62]. Patient selection is influenced by the diagnostic cap- The biggest risk of NOM in penetrating trauma is a ability and accuracy. In fact, the accuracy of CT scan missed abdominal injury, especially hollow viscus perfor- in SWs has been questioned [37, 50]. Even in the ation [34, 46]. However, no increase in mortality rates presence of a negative CT scan, exploratory laparos- with missed hollow viscus perforation has been reported copy/laparotomy may be necessary [37]. Interval in patients without peritonitis on admission [63]. As a laparoscopy is a useful tool to be considered in obese counterpart, non-therapeutic laparotomy leads to an in- patients or in the presence a long and tangential crease in morbidity [63]. Moreover, OM in penetrating wound tract or when the trajectory is difficult to de- liver injuries has a higher liver-related complication rate termine on CT scan [34, 37]. In anterior abdominal (50–52%) compared to blunt injuries [34, 46]. SW, local wound exploration (LWE) is generally ac- During NOM for liver injuries, no standard early curate in evaluating penetration depth; small external follow-up and monitoring protocols exist in adult or in wounds may be enlarged for precise LWE and deter- children [34]. Serial clinical evaluation and hemoglobin mination of anterior fascia violation [34, 35]. LWE, measurement represent the cornerstone in evaluating however, may be misleading, and patients should be NOM patients [14]. Bedsides, US may represent an af- admitted for observation if equivocal. Wounds close fordable tool during early follow-up. Presence of large to the inferior costal margin should be evaluated by subcapsular hematomas is not a strict indication for LWE with caution and only if strictly necessary. OM, but a higher risk of NOM failure exists. In any case, GSWs undergoing NOM may warrant a CT scan to these patients should undergo serial blood test: increas- determine the trajectory [45, 51]. CT scan specificity and ing levels of transaminases could indicate the presence sensitivity of 96% and 90.5% respectively for GSWs re- of intrahepatic parenchymal ischemia or rare cases of quiring laparotomy have been reported [52]. The gold torsion of suprahepatic veins [64]. ICU admission may standard to decide for OM or NOM remains the clinical be indicated for moderate (WSES II) (AAST III) and se- examination [34, 51] associated with laboratory and vere (WSES III–IV) (AAST IV–V) liver trauma in order radiological evaluation. Strict clinical and hemoglobin to reduce the mortality risk [26]. evaluation should be done (every 6 h for at least 24 h); If available, interval laparoscopy during NOM provides after index CT scan allowing for NOM, serial ecoghra- important information about the evolution of the injury. phical evaluation may be utilized to help in defining pa- Laparoscopy should be considered an important tool in tient clinical evolution. Once stabilized, patients are the NOM of liver injuries, and it could be used as a usually transferred from ICU to the ward [35, 45, 50]. bridge strategy to plan an immediate or subsequent lap- NOM is contraindicated if free intra- or retro- aroscopic/laparotomy intervention [65]. peritoneal air, free intra-peritoneal fluid in the absence Particular attention should be paid in managing of solid organ injury, localized bowel wall thickening, hemodynamically stable patients with liver trauma as- bullet tract close to hollow viscus with surrounding sociated with spinal trauma (ST) and severe traumatic hematoma [46], and in high-energy penetrating trauma brain injury (STBI). In blunt trauma, NOM should are detected at CT scan. apply to all patients with no other indication to lapar- In selected centers, AE is considered as an “extension” otomy. However, the optimal management of con- of NOM in patients with liver injuries presenting with comitant STBI and/or ST and penetrating liver ongoing resuscitative needs [9, 53, 54]. If required, AE injuries is debated and OM in general could be sug- can be safely repeated. gested as safer [45, 48, 66].
Coccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 9 of 15
Patients affected by neurotrauma (i.e., spinal cord exclusion may be used [64, 74]. Of paramount import-
or moderate-severe traumatic brain injury) in fact, for ance is to provide simultaneous intraoperative intensive
several instances, differ from the others because they resuscitation with early institution of a massive transfu-
need a higher perfusion pressure to adequately supply sion protocol (MTP) aiming to maintain organ perfusion
oxygen to the brain and to the spinal cord to reduce and ultimately reverse all trauma-induced physiological
the subsequent burden of disability and mortality. A derangements [34, 71, 73, 75].
disruption of the normal blood flow regulation in the In case of evident injury to the proper hepatic artery,
central nervous system (CNS) characterizes the an attempt to control and repair it should be made. If
trauma and eventually leads to a blood flow not effective or not possible, selective hepatic artery
dependent on perfusion pressure in ischemic tissue ligation should be considered as a viable option. If the
[67]. Specific hemodynamic goals for ST and STBI injury is on the right or left branches of the proper hep-
are defined as SBP > 110 mmHg and/or a CPP be- atic artery, selective ligation is advisable. If the right or
tween 60 and 70 mmHg in the case of moderate/se- common hepatic artery must be ligated, cholecystectomy
vere TBI and an MBP > 80 mmHg in case of ST [68, should be performed to avoid gallbladder necrosis [2,
69]. To date, no study specifically addressed the 76]. If the patient’s condition allows for it, post-operative
NOM of abdominal solid organ injuries in the neuro- AE represents a viable alternative allowing hemorrhage
trauma patient, and several authors have considered it control while reducing complications [34, 66, 71, 77].
an exclusion criterion from NOM [45, 48, 70]. How- Hepatic artery ligation increases the risk of hepatic ne-
ever, since the first goal is to have a stable patient crosis, abscesses, and biloma formation [34].
with adequate perfusion pressure, there is no rationale Portal vein injuries should be repaired primarily. Portal
in denying NOM to these patients, as long as the vein main branch ligation should not be considered and
specific hemodynamic goals are met. should be avoided because of the high risk of liver ne-
crosis or massive bowel edema. If no other option exists,
Operative management ligation can be used, but only in patients with an intact
hepatic artery. Liver packing or liver resection should be
Hemodynamically unstable and non-responder pa- preferred to ligation in case of lobar or segmental/sub-
tients (WSES IV) should undergo OM (GoR 2A). segmental portal venous branch injuries [34, 76].
Primary surgical intention should be to control the Whenever Pringle maneuver or arterial control fails
hemorrhage and bile leak and initiation of damage and bleeding persists, the presence of an aberrant hep-
control resuscitation as soon as possible (GoR 2A). atic artery should be considered. If the bleeding comes
Major hepatic resections should be avoided at first from behind the liver, retro-hepatic caval or hepatic vein
and only considered in subsequent operations, in a injury should be highly suspected [34, 77]. Three viable
resectional debridement fashion in cases of large options exist for the management of retrohepatic caval/
areas of devitalized liver tissue done by experienced suprahepatic venous injuries: (1) tamponade with hepatic
surgeons (GoR 2B). packing, (2) direct repair (with or without vascular isola-
Angioembolization is a useful tool in case of tion), and (3) lobar resection [38, 78–80]. Liver packing
persistent arterial bleeding after non-hemostatic or is the least risky method to temporarily deal with severe
damage control procedures (GoR 2A). venous injuries [34, 66, 81–83]. Direct venous repair is
Resuscitative endovascular balloon occlusion of the difficult especially in non-experienced hands, with high
aorta (i.e., REBOA) may be used in mortality rates [34, 66].
hemodynamically unstable patients as a bridge to Different techniques of hepatic vascular exclusion with
other more definitive procedures for hemorrhage shunting procedures have been described, most of them
control (GoR 2B). anecdotally. The veno-veno bypass (femoral vein and in-
ferior mesenteric vein to axillary or jugular vein by pass)
At laparotomy, if no major bleeding is present, com- and the use of fenestrated stent grafts are the most fre-
pression alone or electrocautery, bipolar devices, argon quently used [66, 71, 76, 84]. The atrio-caval shunt by-
beam coagulation, topical hemostatic agents, simple su- passes the retro-hepatic cava blood through the right
ture of the hepatic parenchyma, or omental patching atrium using a chest tube put into the inferior vena cava.
may be sufficient to stop the bleeding [34, 66, 71–73]. Mortality rates in such a complicated situations are very
In case of major hemorrhage, more aggressive proce- high and usually related to the fact that the decision to
dures including manual compression and hepatic pack- perform the shunt is made late in the case [71].
ing, ligation of vessels in the wound, hepatic Complete vascular exclusion of the liver is generally
debridement and finger fracture, balloon tamponade, poorly tolerated in the unstable patient with major blood
shunting procedures, or hepatic vascular isolation and loss [34].Coccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 10 of 15
Resuscitative endovascular balloon occlusion of the Combination of percutaneous drainage and
aorta (REBOA) catheter in zone I should be considered endoscopic techniques may be considered in
if despite all damage control procedures, there is still ac- managing post-traumatic biliary complications not
tive surgical bleeding. Simultaneously, the large high suitable for percutaneous management alone (GoR
flow femoral venous catheter should be exchanged over 2B).
a guide wire to an introducer with the aim of floating up Laparoscopic lavage/drainage and endoscopic
and inflating a resuscitative endovascular balloon occlu- stenting may be considered as the first approach in
sion of the vena cava (REBOVC) at the level of the delayed post-traumatic biliary fistula without any
retro-hepatic vena cava. The goal is to achieve proximal other indication for laparotomy (GoR 2B).
and distal vascular control of a possible retro-hepatic/ Laparoscopy as initial approach should be
supra-hepatic vessel injury with the REBOVC and ultim- considered in cases of delayed surgery, so as to
ately obtaining complete combined endovascular/open minimize the invasiveness of surgical intervention
liver isolation with the Pringle maneuver. A supra- and to tailor the procedure to the lesion (GoR 2B).
diaphragmatic central venous access must be obtained
prior to inflating the REBOA/REBOVC [85–91]. In blunt hepatic trauma, particularly after high-grade
In cases of liver avulsion or total crush injury, when a injury, complications occur in 12–14% of patients [9,
total hepatic resection is indicated, hepatic transplant- 66]. Diagnostic tools for complications after NOM in-
ation has been described [76]. A retrospective study clude clinical examination, blood tests, ultrasound, and
based on the European Liver Transplant Registry identi- CT scan. Routine follow-up with CT scan is not neces-
fies an ISS score less than 33 for recipient selection, so sary unless there is clinical suspicion of a complication
to avoid futile procedures [92]. [6, 9, 66]. In the presence of abnormal inflammatory re-
Anatomic hepatic resection may seldom be considered sponse, abdominal pain, fever, jaundice, or drop of
as a surgical option [6, 93, 94]. In unstable patients and hemoglobin level, repeated CT scan is recommended
during damage control surgery, it should be avoided, but [9]. Bleeding, abdominal compartment syndrome, infec-
in case of need, a non-anatomic resection is safer and tions (abscesses and other infections), biliary complica-
easier [34, 66, 71, 76]. For staged liver procedures, either tions (bile leak, hemobilia, biloma, biliary peritonitis,
anatomic or non-anatomic resections may be safely per- biliary fistula), and liver necrosis are the most frequent
formed by experienced surgeons [76]. complications associated with NOM [16, 66]. Ultrasound
Temporary abdominal closure may be indicated if the is useful in the assessment of bile leak/biloma in grade
risk of abdominal compartment syndrome is high or in IV–V injuries, especially with a central laceration.
those situation where a “second look” operation is Re-bleeding or secondary hemorrhage is the most fre-
needed [71–73]. quently reported complications after NOM as in subcap-
Two principal indications for post-operative sular hematoma or pseudo-aneurysm (PSA) rupture
angiography-embolization (AG-AE) have been proposed: (range 1.7–5.9%) with a mortality rate up to 18% [9, 66,
(1) after initial operative hemostasis, in stable or stabi- 101, 102]. In the majority of cases (69%), “late” bleeding
lized patients with contrast blush at completion CT can be treated non-operatively [9, 66].
scan; and (2) as adjunctive hemostatic tool in patients Hepatic artery PSA is a rare complication with a
with uncontrolled suspected arterial bleeding despite prevalence of 1% [103]. Asymptomatic PSA should be
emergency laparotomy and hemostasis attempt [34, 54, treated as early as possible with AE because of the high
95–99]. Recent evidence suggests that routine use of im- risk of rupture and the associated high morbidity [34,
mediate post-damage control hepatic angiography re- 104, 105]. In patients with melena or hematemesis fol-
duces mortality in grade IV/V hepatic injuries [100]. lowing liver trauma, bleeding from the ampulla of Vater
(hemobilia) is highly suggestive of ruptured intrahepatic
Complications PSA [106, 107]. AE is the treatment of choice [6, 34, 66].
In the presence of intrahepatic bilio-venous fistula (fre-
Intrahepatic abscesses may be successfully treated quently associated with bilemia), endoscopic retrograde
with percutaneous drainage (GoR 2A). cholangiopancreatography (ERCP) represents an effect-
Delayed hemorrhage without severe hemodynamic ive tool [108].
compromise may be managed at first with AG/AE Biliary complications include biloma, biliary fistula, bil-
(GoR 2A). hemia, and bile peritonitis (incidence 2.8–30%) [8, 40].
Hepatic artery pseudoaneurysm should be managed Most traumatic bilomas regress spontaneously. Enlar-
with AG/AE to prevent rupture (GoR 2A). ging, symptomatic or infected bilomas can be success-
Symptomatic or infected bilomas should be fully managed with percutaneous drainage. Percutaneous
managed with percutaneous drainage (GoR 2A). drainage may be combined with therapeutic ERCP withCoccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 11 of 15
eventual endobiliary stent placement [9, 101, 109–111]. to balance the risk of bleeding against the benefit of pre-
Bile peritonitis has been usually treated with laparotomy. venting thrombotic complications. Poor outcomes derive
Combination of laparoscopic irrigation/drainage and from the failure to restore the anticoagulation as soon as
endoscopic bile duct stent placement may represent a possible [127].
valid alternative [101, 102, 112, 113]. Early enteral feeding is associated with improved clin-
Abscesses are rare after NOM and usually happen in ical outcomes when administered within the first 72 h
severe lesions (prevalence 0.6–7%) [9, 66, 114–117]. CT from admission in ICU [128], and it should be delayed
scan or ultrasound-guided percutaneous drainage is the only in cases of uncontrolled shock, use of vasopressor
treatment of choice with high success rate and no re- therapy, uncontrolled hypoxaemia and acidosis, uncon-
ported mortality [106]. In the presence of necrosis and trolled upper GI bleeding, gastric aspirate > 500 ml/6 h,
devascularization of hepatic segments, surgical manage- bowel ischemia, bowel obstruction, abdominal compart-
ment may be indicated whenever affecting patient condi- ment syndrome, and high-output fistula without distal
tion [34, 66]. feeding access [129]. Oral intake, when possible, should
Generally, once stabilization of traumatized patient is be initiated after 24–48 h from the traumatic event.
obtained, late complications should be managed prefer-
entially by minimally invasive procedures. Laparoscopy Follow-up
and endoscopy are part of this approach, which became Mandatory late follow-up imaging is not indicated, and
possible in a delayed surgery setting [64, 65, 118, 119]. it should be used only if the patient’s clinical condition
and/or symptoms indicating a complication require it
Thromboprophylaxis, feeding, and mobilization for diagnosis. The majority of liver lesions heal in about
4 months [14, 66]. After moderate and severe liver injur-
Mechanical prophylaxis is safe and should be ies, patients may usually resume normal physical activ-
considered in all patients with no absolute ities after 3–4 months.
contraindication (GoR 2A). During the recovery phase, patients should be encour-
LMWH-based prophylaxis should be started as soon aged to not remain alone for long periods and to return
as possible following trauma and may be safe in immediately to the hospital in case of increasing abdom-
selected patients with liver injury treated with NOM inal pain, lightheadedness, nausea, or vomiting [14, 34].
(GoR 2B).
In those patients taking anticoagulants, Conclusions
individualization of the risk-benefit balance of anti- Management of liver trauma is multidisciplinary. When
coagulant reversal is suggested (GoR 1C). feasible, non-operative management should always be
Early mobilization should be achieved in stable considered as the first option in adult and in the
patients (GoR 2A). pediatric populations. For this reason, clinical condition,
In the absence of contraindications, enteral feeding anatomical injury grade, and associated injuries should
should be started as soon as possible (GoR 2A). be considered together in deciding the best treatment
option.
Venous thromboembolism (VTE) is one of the great
Abbreviations
risks of trauma victims, because patients enter a hyper- NOM: Non-operative management; OM: Operative management;
coagulation state within 48 h from injury [120–122]. AAST: American Association for Surgery for Trauma; WSES: World Society of
More than 50% of patients without thrombo-prophylaxis Emergency Surgery; PTS: Panamerican Trauma Society; ATLS: Advanced
trauma life support; ERCP: Endoscopic retrograde cholangiopancreatography;
may develop deep vein thrombosis (DVT) and subse- BLT: Blunt liver trauma; SW: Stab wounds; GSW: Gunshot wound;
quent pulmonary embolism (PE) which carries a moral- DCS: Damage control surgery; OR: Operating room; AG: Angiography;
ity rate up to 50% [120, 121]. PE is the third leading AE: Angioembolization; EVTM: Endovascular bleeding and trauma
management; STBI: Severe traumatic brain injury; ST: Spine trauma;
cause of death in trauma patients. CNS: Central nervous system; PSA: Pseudoaneurysm; REBOA: Resuscitative
No differences in complication, mortality, and NOM endovascular balloon occlusion of the aorta; MTP: Massive transfusion
failure rate were demonstrated when thrombo- protocol
prophylaxis was administered within and after 48 and Acknowledgements
72 h from the initial injury in patients without STBI and None
BST [123–125]. Early mobilization is not related to (1) General and Trauma Surgery, Rambam Medical Centre, Tel Aviv, Israel
(2) General Surgery Dept., Mehilati Hospital, Helsinki, Finland
NOM failure and secondary bleeding [126]. However, (3) General Emergency and Trauma Surgery, Bufalini Hospital, Cesena, Italy
VTE rates seem to be over fourfold when LMWH is ad- (4) Fundación Valle del Lili, Division of Trauma and Acute Care Surgery, Cali,
ministered > 72 h from admission [120]. Colombia
(5) Division of Trauma and Acute Care Surgery, Universidad del Valle –
In patients taking anticoagulants, it is important to Hospital Universitario del Valle, Cali-Colombia
evaluate the eventual need for reversal therapy in order (6) Fundacion Valle del Lili, Clinical Research Center, Cali, ColombiaCoccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 12 of 15
(7) Trauma/Acute Care Surgery & Surgical Critical Care, University of Mexico. 6Trauma Surgery, Denver Health, Denver, CO, USA. 7Trauma Surgery
Campinas, Campinas, Brazil Department, Scripps Memorial Hospital La Jolla, San Diego, CA, USA.
8
(8) General, Acute Care, Abdominal Wall Reconstruction, and Trauma Surgery Surgery Department, University of Pittsburgh, Pittsburgh, PA, USA.
9
Foothills Medical Centre, Calgary, Alberta, Canada Department of Cardiothoracic and Vascular Surgery, Örebro University
(9) Department of Surgery and Obstetrics and Gynecology, University of Hospital, Örebro University, Örebro, Sweden. 10Department of Surgery,
Buea, Buea, Cameroon College of Medicine and Health Sciences, UAE University, Al-Ain, United Arab
(10) Emergency Surgery Dept., Parma University Hospital, Parma, Italy Emirates. 11General and Emergency Surgery, Macerata Hospital, Macerata,
(11) Emergency and Trauma Surgery Dept., Niguarda Hospital, Milano, Italy Italy. 12Trauma/Acute Care Surgery & Surgical Critical Care, University of
(12) Hospital Universitário Terezinha De Jesus, Faculdade De Ciências Campinas, Campinas, Brazil. 13General, Emergency and Trauma Surgery
Médicas E Da Saúde De Juiz De Fora (Suprema) Brazil Department, Bufalini Hospital, Cesena, Italy. 14Department of Trauma Critical
(13) Trauma and Acute Care Surgery and Surgical Critical Care Trauma, Care, Broward General Level I Trauma Center, Fort Lauderdale, FL, USA. 15Unit
Department of Surgery University of California, Davis, USA of Digestive Surgery, HPB Surgery and Liver Transplant, Henri Mondor
(14) General Surgery Dept., Hadassah Medical Centre, Jerusalem, Israel Hospital, Créteil, France. 16General and Trauma Surgery, LAC+USC Medical
(15) Emergency Medicine Dept., Verona Hospital, Verona, Italy Center, Los Angeles, CA, USA. 17General and Emergency Surgery,
(20) General and Emergency Surgery Dept., Montevideo Hospital, Massachusetts General Hospital, Boston, MA, USA. 18Department of Surgery,
Montevideo, Paraguay Harborview Medical Centre, Seattle, USA. 19General Surgery Department,
(21) Trauma and Surgical Critical Care, University of Michigan Health System, Mozir City Hospital, Mozir, Belarus. 20General Surgery Department, Medical
East Medical Center Drive, Ann Arbor, MI, USA University, University Hospital St George, Plovdiv, Bulgaria. 21Department of
(22) Papa Giovanni XXIII Hospital, Bergamo, Italy Surgery, Zagreb University Hospital Centre and School of Medicine,
(23) Emergency medicine dept., Pisa University Hospital, Pisa, Italy University of Zagreb, Zagreb, Croatia. 22General and Trauma Surgery
(24) Intensive Care Dept., Pisa University Hospital, Pisa, Italy Addenbrooke’s Hospital, Cambridge University Hospitals NHS Foundation
(25) General, Emergency and Trauma Surgery Dept., Pisa University Hospital, Trust, Cambridge, UK. 233rd Department of Surgery, Attiko Hospital, National
Pisa, Italy & Kapodistrian University of Athens, Athens, Greece. 24Chirurgie Digestive,
(26) General, Emergency and Trauma Surgery Dept., Monza University CHUGA-CHU Grenoble Alpes, Grenoble, France. 25General and Emergency
Hospital, Monza, Italy Surgery, Sergei Kirov Military Academy, Saint Petersburg, Russia. 26General
(27) Chirurgie D’Urgence et Digestive, CHUGA-CHU Grenoble Alpes, Gre- Surgery Department, Mehilati Hospital, Helsinki, Finland. 27General and
noble, France Trauma Surgery Department, Pietermaritzburg Hospital, Pietermaritzburg,
(28) Interventional Radiology Dept., Mozir City Hospital, Mozir, Belarus South Africa. 28General and Emergency Surgery, NHS Lothian, Edinburgh, UK.
29
(29) Department of Surgery, Stanford University, Stanford, CA, USA Department of General Surgery, Royal Perth Hospital, Perth, Australia.
30
(30) Erzincan University Faculty Of Medicine Mengucek Gazi Training General and Trauma Surgery Department, London Health Sciences Centre,
Research Hospital Erzincan, Turkey Victoria Hospital, London, ON, Canada. 31General Surgery, Tbilisi State
Members of WSES Expert Panel: Hany Bahouth (1), Matti Tolonen (2), Paola Medical University, Tbilisi, Georgia. 32Trauma Surgery, Auckland University
Fugazzola (3), Jose Julian Serna (4), Fernando Rodriguez (4), Alberto F. García Hospital, Auckland, New Zealand. 33Division of Acute Care Surgery, University
(4), Adolfo Gonzalez (5), Luis Fernando Pino (5), Mónica Guzmán-Rodríguez of Michigan Health System, Ann Arbor, MI, USA. 34ICU Department, Papa
(6), Bruno M Pereira (7), Andrew Kirkpatrick (8), Alain Chichom Mefire (9), Giovanni XXII Hospital, Bergamo, Italy. 35Emergency and Trauma Surgery,
Antonio Tarasconi (10), Osvaldo Chiara (11), Carlos Augusto Gomes (12), Maggiore Hospital, Parma, Italy. 36Department of Surgery, Örebro University
Joseph Galante (13), Miklosh Bala (14), Paola Perfetti (19), Fernando Machado Hospital, Örebro University, Örebro, Sweden.
(20), Oreste Romeo (21), Francesco Salvetti (22), Lorenzo Ghiadoni (23),
Francesco Forfori (24), Paolo Malacarne (24), Silvia Pini (24), Marsia Pucciarelli Received: 17 January 2020 Accepted: 6 March 2020
(25), Marco Ceresoli (26), Catherine Arvieux (27), Denis Khokha (28), David A.
Spain (29) and Arda Isik (30).
References
Authors’ contributions
1. Brillantino A, Iacobellis F, Festa P, Mottola A, Acampora C, Corvino F, Del
FC, RC, CA, YK, FV, EM, WB, AP, TH, FAZ, MS, GPF, EC, LA, MWP, MM, NDA, KI,
Giudice S, Lanza M, Armellino M, Niola R, Romano L, Castriconi M, De Palma
GV, RM, VK, BS, GA, SDS, MP, MC, VR, AL, VM, MC, DD, DW, NP, ZD, IC, LN, DC,
M, Noschese G. Non-operative management of blunt liver trauma: safety,
and FCa contributed to the manuscript conception and draft, critically
efficacy and complications of a standardized treatment protocol. Bull Emerg
revised the manuscript, contributed important scientific knowledge, and
trauma. 2019;7(1):49–54.
approved the final manuscript.
2. David Richardson J, Franklin GA, Lukan JK, Carrillo EH, Spain DA, Miller FB,
Wilson MA, Polk HC, Flint LM. Evolution in the management of hepatic
Funding
trauma: a 25-year perspective. Ann Surg. 2000;232(3):324–30.
None
3. Badger SA, Barclay R, Campbell P, Mole DJ, Diamond T. Management of
liver trauma. World J Surg. 2009;33(12):2522–37.
Availability of data and materials 4. Peitzman AB, Richardson JD. Surgical treatment of injuries to the solid
Not applicable abdominal organs: a 50-year perspective from the Journal of Trauma. J
Trauma. 2010;69(5):1011–21.
Ethics approval and consent to participate 5. Morrison JJ, Bramley KE, Rizzo AG. Liver trauma--operative management. J R
Not applicable Army Med Corps. 2011;157(2):136–44.
6. Piper GL, Peitzman AB. Current management of hepatic trauma. Surg Clin
Consent for publication North Am. 2010;90(4):775–85.
Not applicable 7. Oxford Centre for Evidence-based Medicine - Levels of Evidence (March
2009) - CEBM [Internet]. Available from: http://www.cebm.net/oxford-centre-
Competing interests evidence-based-medicine-levels-evidence-march-2009/.
The authors declare that they have no competing interests. 8. Boese CK, Hackl M, Müller LP, Ruchholtz S, Frink M, Lechler P. Nonoperative
management of blunt hepatic trauma: a systematic review. J Trauma Acute
Author details Care Surg. 2015;79(4):654–60.
1
General, Emergency and Trauma Surgery Department, Pisa University 9. Kozar RA, Moore FA, Moore EE, West M, Cocanour CS, Davis J, Biffl WL,
Hospital, Via Paradisia 1, 56100 Pisa, Italy. 2Riverside University Health System, McIntyre RC. Western Trauma Association critical decisions in trauma:
CECORC Research Center, Loma Linda University, Loma Linda, USA. 3Division nonoperative management of adult blunt hepatic trauma. J Trauma. 2009;
of Trauma and Acute Care Surgery, Fundación Valle del Lili, Cali, Colombia. 67(6):1144–8 discussion 1148-9.
4
Division of General Surgery, Rambam Health Care Campus Haifa, Haifa, 10. Fodor M, Primavesi F, Morell-Hofert D, Haselbacher M, Braunwarth E, Cardini
Israel. 5Department of Surgery, Hospital Angeles Lomas, Huixquilucan, B, Gassner E, Öfner D, Stättner S. Non-operative management of bluntCoccolini et al. World Journal of Emergency Surgery (2020) 15:24 Page 13 of 15
hepatic and splenic injuries-practical aspects and value of radiological 31. Carver D, Kirkpatrick AW, D’Amours S, Hameed SM, Beveridge J, Ball CG. A
scoring systems. Eur Surg. 2018;50(6):285–98. prospective evaluation of the utility of a hybrid operating suite for severely
11. Becker A, Lin G, McKenney MG, Marttos A, Schulman CI. Is the FAST exam injured patients. Ann Surg. 2018;20:1.
reliable in severely injured patients? Injury. 2010 May;41(5). 32. Gaski IA, Skattum J, Brooks A, Koyama T, Eken T, Naess PA, Gaarder C.
12. Kirkpatrick AW, Sirois M, Laupland KB, Liu D, Rowan K, Ball CG, Hameed SM, Decreased mortality, laparotomy, and embolization rates for liver injuries
Brown R, Simons R, Dulchavsky SA, Hamiilton DR, Nicolaou S. Hand-held during a 13-year period in a major Scandinavian trauma center. Trauma
thoracic sonography for detecting post-traumatic pneumothoraces: the Surg acute care open. 2018;3(1):e000205.
Extended Focused Assessment with Sonography for Trauma (EFAST). J 33. Buci S, Torba M, Gjata A, Kajo I, Bushi G, Kagjini K. The rate of success of the
Trauma. 2004;57(2):288–95. conservative management of liver trauma in a developing country. World J
13. Kirkpatrick AW, Sirois M, Ball CG, Laupland KB, Goldstein L, Hameed M, Emerg Surg. 2017;12:24.
Brown DR, Simons RK, Kortbeek J, Dulchavsky S, Boulanger BB. The hand- 34. Coccolini F, Montori G, Catena F, Di Saverio S, Biffl W, Moore EE, Peitzman
held ultrasound examination for penetrating abdominal trauma. Am J Surg. AB, Rizoli S, Tugnoli G, Sartelli M, Manfredi R, Ansaloni L. Liver trauma: WSES
2004;187(5):660–5. position paper. World J Emerg Surg. 2015;10:39.
14. Parks NA, Davis JW, Forman D, Lemaster D. Observation for nonoperative 35. Biffl WL, Leppaniemi A. Management guidelines for penetrating abdominal
management of blunt liver injuries: how long is long enough? J Trauma. trauma. World J Surg. 2015;39(6):1373–80.
2011;70(3):626–9. 36. Biffl WL, Moore EE. Management guidelines for penetrating abdominal
15. Hommes M, Navsaria PH, Schipper IB, Krige JEJ, Kahn D, Nicol AJ. trauma. Curr Opin Crit Care. 2010;16(6):609–17.
Management of blunt liver trauma in 134 severely injured patients. Injury. 37. Biffl WL, Kaups KL, Pham TN, Rowell SE, Jurkovich GJ, Burlew CC, Elterman J,
2015;46(5):837–42. Moore EE. Validating the Western Trauma Association algorithm for
16. Stassen NA, Bhullar I, Cheng JD, Crandall ML, Friese RS, Guillamondegui OD, managing patients with anterior abdominal stab wounds: a Western
Jawa RS, Maung AA, Rohs TJ, Sangosanya A, Schuster KM, Seamon MJ, Trauma Association multicenter trial. J Trauma. 2011;71(6):1494–502.
Tchorz KM, Zarzuar BL, Kerwin AJ, Eastern Association for the Surgery of 38. Croce MA, Fabian TC, Menke PG, Waddle-Smith L, Minard G, Kudsk KA,
Trauma, Rohs TJ Jr, Sangosanya A, Schuster KM, Seamon MJ, Tchorz KM, Patton JH, Schurr MJ, Pritchard FE. Nonoperative management of blunt
Zarzuar BL, Kerwin AJ. Nonoperative management of blunt hepatic injury: hepatic trauma is the treatment of choice for hemodynamically stable
an Eastern Association for the Surgery of Trauma practice management patients. Results of a prospective trial. Ann Surg. 1995;221(6):744–53
guideline. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S288–93. discussion 753-5.
17. Carr JA, Roiter C, Alzuhaili A. Correlation of operative and pathological injury 39. Cimbanassi S, Chiara O, Leppaniemi A, Henry S, Scalea TM,
grade with computed tomographic grade in the failed nonoperative Shanmuganathan K, Biffl W, Catena F, Ansaloni L, Tugnoli G, De Blasio E,
management of blunt splenic trauma. Eur J Trauma Emerg Surg. 2012;38(4): Chieregato A, Gordini G, Ribaldi S, Castriconi M, Festa P, Coccolini F, di
433–8. Saverio S, Galfano A, Massi M, Celano M, Mutignani M, Rausei S, Pantalone
18. Bee TK, Croce MA, Miller PR, Pritchard FE, Fabian TC. Failures of splenic D, Rampoldi A, Fattori L, Miniello S, Sgardello S, Bindi F, Renzi F,
nonoperative management: is the glass half empty or half full? J Trauma. Sammartano F. Nonoperative management of abdominal solid-organ
2001;50(2):230–6. injuries following blunt trauma in adults: results from an International
19. Clark R, Hird K, Misur P, Ramsay D, Mendelson R. CT grading scales for Consensus Conference. J Trauma Acute Care Surg. 2018;84(3):517–31.
splenic injury: why can’t we agree? J Med Imaging Radiat Oncol. 2011;55(2): 40. Velmahos GC, Toutouzas KG, Radin R, Chan L, Demetriades D. Nonoperative
163–9. treatment of blunt injury to solid abdominal organs: a prospective study.
20. Becker CD, Mentha G, Terrier F. Blunt abdominal trauma in adults: role of CT Arch Surg. 2003;138(8):844–51.
in the diagnosis and management of visceral injuries. Part 1: liver and 41. Yanar H, Ertekin C, Taviloglu K, Kabay B, Bakkaloglu H, Guloglu R.
spleen. Eur Radiol. 1998;8(4):553–62. Nonoperative treatment of multiple intra-abdominal solid organ injury after
21. Shapiro MJ, Krausz C, Durham RM, Mazuski JE. Overuse of splenic scoring blunt abdominal trauma. J Trauma. 2008;64(4):943–8.
and computed tomographic scans. J Trauma. 1999;47(4):651–8. 42. JF F, YC W, BC L, YP H, MF C. The CT risk factors for the need of operative
22. Anderson SW, Varghese JC, Lucey BC, Burke PA, Hirsch EF, Soto JA. Blunt treatment in initially hemodynamically stable patients after blunt hepatic
splenic trauma: delayed-phase CT for differentiation of active hemorrhage trauma. J Trauma. 2006;61(3).
from contained vascular injury in patients. Radiology. 2007;243(1):88–95. 43. Fang JF, Chen RJ, Wong YC, Lin BC, Hsu YB, Kao JL, Kao YC. Pooling of
23. Jeffrey RB, Olcott EW. Imaging of blunt hepatic trauma. Radiol Clin N Am. contrast material on computed tomography mandates aggressive
1991;29(6):1299–310. management of blunt hepatic injury. Am J Surg. 1998;176(4):315–9.
24. Marmery H, Shanmuganathan K, Mirvis SE, Richard H, Sliker C, Miller LA, 44. Poletti PA, Mirvis SE, Shanmuganathan K, Takada T, Killeen KL, Perlmutter D,
Haan JM, Witlus D, Scalea TM. Correlation of multidetector CT findings with Hahn J, Mermillod B. Blunt abdominal trauma patients: can organ injury be
splenic arteriography and surgery: prospective study in 392 patients. J Am excluded without performing computed tomography? J Trauma. 2004;57(5):
Coll Surg. 2008;206(4):685–93. 1072–81.
25. Boscak AR, Shanmuganathan K, Mirvis SE, Fleiter TR, Miller LA, Sliker CW, 45. Navsaria PH, Nicol AJ, Krige JE, Edu S. Selective nonoperative management
Steenburg SD, Alexander M. Optimizing trauma multidetector CT protocol of liver gunshot injuries. Ann Surg. 2009;249(4):653–6.
for blunt splenic injury: need for arterial and portal venous phase scans. 46. Demetriades D, Hadjizacharia P, Constantinou C, Brown C, Inaba K, Rhee P,
Radiology. 2013;268(1):79–88. Salim A. Selective nonoperative management of penetrating abdominal
26. Tignanelli CJ, Joseph B, Jakubus JL, Iskander GA, Napolitano LM, Hemmila solid organ injuries. Ann Surg. 2006;244(4):620–8.
MR. Variability in management of blunt liver trauma and contribution of 47. Demetriades D, Rabinowitz B. Indications for operation in abdominal stab
level of American College of Surgeons Committee on Trauma verification wounds. A prospective study of 651 patients. Ann Surg. 1987;205(2):129–32.
status on mortality. J Trauma Acute Care Surg. 2018;84(2):273–9. 48. Navsaria PH, Nicol AJ, Edu S, Gandhi R, Ball CG. Selective nonoperative
27. Osterballe L, Helgstrand F, Hillingsø J, Henriksen B, Svendsen LB. Management management in 1106 patients with abdominal gunshot wounds:
of patients with liver traumas. Ugeskr Laeger. 2014 Sep 15;176:38. conclusions on safety, efficacy, and the role of selective CT imaging in a
28. Roudsari BS, Psoter KJ, Padia SA, Kogut MJ, Kwan SW. Utilization of prospective single-center study. Ann Surg. 2015;261(4):760–4.
angiography and embolization for abdominopelvic trauma: 14 years’ 49. Omoshoro-Jones JAO, Nicol AJ, Navsaria PH, Zellweger R, Krige JEJ, Kahn
experience at a level I trauma center. AJR Am J Roentgenol. 2014;202(6): DH. Selective non-operative management of liver gunshot injuries. Br J
W580–5. Surg. 2005;92(7):890–5.
29. Samuels JM, Urban S, Peltz E, Schroeppel T, Heise H, Dorlac WC, Britton LJ, 50. Biffl WL, Kaups KL, Cothren CC, Brasel KJ, Dicker RA, Bullard MK, Haan JM,
Burlew CC, Robinson C, Swope ML, McIntyre RC. A modern, multicenter Jurkovich GJ, Harrison P, Moore FO, Schreiber M, Knudson MM, Moore EE.
evaluation of hepatic angioembolization - complications and readmissions Management of patients with anterior abdominal stab wounds: a Western
persist. Am J Surg. 2020;219(1):117–22. Trauma Association multicenter trial. J Trauma. 2009;66(5):1294–301.
30. Swendiman RA, Goldshore MA, Fenton SJ, Nance ML. Defining the role of 51. Lamb CM, Garner JP. Selective non-operative management of civilian
angioembolization in pediatric isolated blunt solid organ injury. J Pediatr gunshot wounds to the abdomen: a systematic review of the evidence.
Surg. 2019 May 11;. Injury. 2014;45(4):659–66.You can also read