Massachusetts Board of Registration in Medicine 2018 Update - Carol A.M. Purmort Acting Director of Licensing - namss
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Massachusetts Board of
Registration in Medicine
2018 Update
Carol A.M. Purmort
Acting Director of Licensing
Structure of Talk History of Physician Licensing in Massachusetts Current Board and its Committees 2017/2018 Updates at the Board of Medicine
A Brief History of Physician Licensing in Massachusetts
Medical Training in the United States
(1700’s)
MA Legislature Concerns “And whereas it is clearly of Importance, that a just Discrimination should be made between such as are duly educated and properly qualified for the Duties of their Profession and those who may ignorantly and wickedly administer medicine, whereby the Health and License of many valuable Individuals are endangered, or perhaps lost to the Community.”
Chapter 15, of the Acts of 1781, established
the Massachusetts Medical Society (MMS).
MMS was granted the power to examine all
candidates and, if found skilled and qualified,
to grant a medical license to the physician.
1781-1850
Pathway for licensure, rarely followed
Unlicensed physicians continued to practice
medicine;
For profit medical schools proliferated and
graduated a number of uneducated and ill-
trained physicians.
1850 Massachusetts legislature revoked all statutes regarding the licensure of physicians
1850 -1894
Many different attempts were made to
establish a licensing requirement for
physicians.Professor James C. White, circa 1890 Harvard Medical School In the mid-1860’s, Professor White called for higher standards with regard to: admission to medical school; greater emphasis on science; and enhancement in training (to match European Medical Schools).
1894
Chapter 458, of the acts of 1894, the Massachusetts
legislature established the Board of Registration of
Physicians and Surgeons. (The Board has been in
continuous operation since 1894)
Effective January 1, 1895, the Board was required to
examine applicants and issue licenses to physicians
who successfully passed the examination and
complied with the other provisions of Chapter 458.1910 – The Creation of Modern Medical
Education
• AMA and Carnegie Foundation
approached Abraham Flexner, an
educator, to survey medical education
with an end to restructuring medical
education
• Visited all 155 medical schools in the
United States and Canada
• Only 2 medical schools were considered
excellent in both clinical and laboratory
facilities: Johns Hopkins and Western
Reserve.The Flexner Report Recommendations
• Establish preliminary educational requirements prior
to entering medical school;
• Deny licensure to graduates of schools that fail to
provide adequate medical education;
• Develop a strong state board made up of the best of
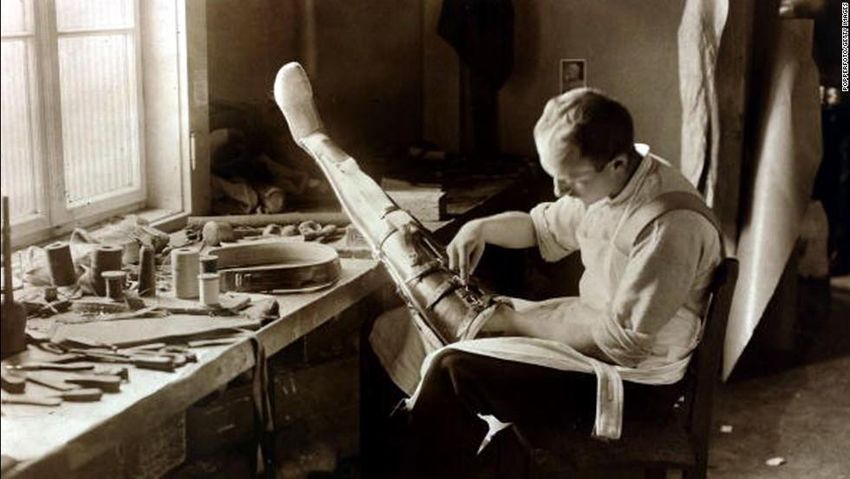
the medical profession.WWI
Post - WWI
Medical knowledge and techniques grew to an
extent that there was too much to teach, even
during a four year course. Internships were
developed.
By the mid-1920’s all US graduates were
required to complete an internship
Gradually, longer training programs, specialty
programs and fellowships began to develop.Present Day 2018
Mission of the Board The mission of the Board is to ensure that only qualified and competent physicians of good moral character are licensed to practice in the Commonwealth of Massachusetts and that those physicians and health care institutions in which they practice provide to their patients a high standard of care, and support an environment that maximizes the high quality of health care in Massachusetts.
Structure of the Board of Registration in Medicine
The Board consists of seven members who are appointed by
the Governor to three-year terms. There are two public
members and five physicians members.
A member may serve only two full consecutive terms.
Members sometimes serve beyond the end of their terms
before a replacement is appointed.
Members may serve on one or more of the Board’s
committees.
Board members are volunteers.Committees of the Board
Complaint Committee. Reviews and makes recommendations
on evidence gathered by the Enforcement Division.
Licensing Committee. Reviews license applications and makes
recommendations to the Board in situations where issues are
raised regarding a physician’s ability to meet the Board’s
statutory and/or regulatory requirements for licensure.
Quality and Patient Safety Committee. Works with health care
facilities to improve patient safety processes, and strengthens
medical quality assurance programs.
Committee on Acupuncture. Works with the Board to regulate
the practice of acupuncture.The Licensing Division The Licensing Division’s work is essential to ensuring that only qualified physicians are licensed to practice medicine in Massachusetts. The Licensing Division accomplishes this crucial function by collecting and verifying the credentials of physicians applying for licensure in Massachusetts.
2017 Initial Full License Application Metrics
Median Processing time for an Initial Full License Application:
73 Days
Average Processing time for an Initial Full License
Application: 75 days
Processing time for applications is dependent on:
1) submission of all required documentation;
2) the current volume of applications being processed by the
Licensing Division Staff; and
3) the need for additional review by the Licensing Committee or the
Board.2017 Initial Limited License Application Metrics
The Licensing Division’s goal for 2017 was to have 80% of qualified limited
license applicants approved more than 15 days in advance of the training
program start date.
1,797 initial limited license applicants were approved by the Board.
82% of initial limited license applicants were approved more than 15 days
in advance of the training program start date.
91% of all initial limited license applicants were approved 7 days in
advance of the training program start date.
98% of all initial limited license applicants were approved one day in
advance of the training program start date.Enforcement
The Enforcement Division’s work is also essential to ensuring
that only qualified physicians are licensed to practice medicine in
Massachusetts.
The Enforcement Division was created by law to:
Investigate complaints relating to the proper practice of
medicine by the Board’s licensees; and
Prosecute disciplinary actions against licensees when the
Board deems it necessary and appropriate.BOARD OF REGISTRATION IN MEDICINE UPDATES
Online Initial Licensure Project
BORIM is in the beginning stages of developing an online
licensure project. This project is for both initial full and initial
limited license applications.
This program will allow BORIM staff more time to devote to
reviewing applications with the goal of shortening the time
frame for processing initial full and limited license
applications.MassHealth Section 22, Chapter 10 of the Acts of 2015, requires applicants to submit an application to MassHealth. The Board’s role in this process is to ensure that a physician attests to submitting that application as a condition of licensure.
Policy on Lapsed License Applications
Beginning in 2003, the application of a physician seeking to
revive a license lapsed for over two years, was required to be
considered by the Licensing Committee. Effective, January
2018, this type of application does not need to be considered by
Licensing Committee if :
The physician has not responded affirmatively to any adverse
questions on the lapsed license application; and
The physician has been in the continuous practice of medicine.Supervisory Board Evaluation
In September 2017, the Board adopted a policy on
Supervisory Evaluations. This policy clarifies the
type of information that the Board is looking for:
Honest and impartial assessment of the applicant by a
physician who has supervised the applicant’s clinical
practice of medicine;
Evaluator should have no conflict of interest, either
personally, professionally or financially, in the
applicant’s licensure in Massachusetts.Policy on Withdrawing License Applications In October 2017, the Board adopted a policy that states, in relevant part, “once the application has been placed on the agenda of the Licensing Committee, an applicant generally may not withdraw his or her license application. In extraordinary circumstances, an applicant may ask the full Board for permission to withdraw. Only the full Board will hear requests to withdraw.” Approval to withdraw a license application requires a unanimous vote of the Board.
CORI In July 2014, the Board began requiring initial full license applicants to undergo a CORI check as part of a general background check for licensing purposes. Required 2 Access: All adult/youthful offender convictions, non- convictions and pending offenses. CORI available through the iCORI service is limited to Massachusetts criminal court appearances. BORIM has expressed an interest in expanding access to out-of- state criminal history through the FBI national criminal history database.
Expansion of CORI
Fall/Winter 2018
CORI checks will be expanded to include:
Lapsed License Applicants;
Temporary License Applicants; and
Limited License Applicants.Continuing Medical Education (CME) Pilot
Program
Pilot program in effect from January 1, 2018 until
December 31, 2020
50 CMEs required (either Category 1 or 2)
Licensees may claim 1.00 credit for every hour of
reading a journal or point of care resource accessed in
the process of delivering patient care or updating
clinical knowledge.
Licensees must maintain a log of credits earned.CME Pilot Program (cont’d)
2 credits per Chapter for reading the Board’s
Regulations (243 CMR 1.00 – 3.00) for a total of 6
credits
10 Risk Management Credits (either Category 1 or 2)
End of Life Credits (One time event)CME Pilot Program (cont’d)
3 Credits in Opioid Education and Pain management,
if the physician prescribes controlled substances.
Required (but already completed for licensure):
• Demonstration of EHR Proficiency*;
• Recognition and Reporting of Child Abuse and Neglect
Training*;
• Domestic Violence and Sexual Violence Training*.
* Means that this is a one-time only requirement.Thank you Questions?
You can also read