Meeting the Challenges of Insomnia in Your Patient Population - Psychiatry ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Meeting the Challenges of Insomnia in
Your Patient Population
Co-Management Strategies, Standards of Care, and
Emerging Pharmacotherapeutic Options
Karl Doghramji, MD
Professor of Psychiatry, Neurology, and Medicine
Medical Director, Jefferson Sleep Disorders Center
Thomas Jefferson University
Philadelphia, Pennsylvania
Educational grant support was provided from Eisai Inc. and Imbrium Therapeutics L.P.
Faculty Disclosure • Dr. Doghramji: Consultant—Eisai, Purdue, Merck, Pfizer; Stock—Merck.
Disclosure
• The faculty have been informed of their responsibility to disclose to the
audience if they will be discussing off-label or investigational use(s) of drugs,
products, and/or devices (any use not approved by the US Food and Drug
Administration).
– Dr. Doghramji will be discussing off-label use of medications in this presentation
and will identify those medications.
• Applicable CME staff have no relationships to disclose relating to the subject
matter of this activity.
• This activity has been independently reviewed for balance.Learning Objectives • Describe the relationship between insomnia and other psychiatric disorders in terms of bidirectional causality and the challenges of co-treatment • Discuss current clinical guidelines for the management of chronic insomnia, recommended standards of care, and limitations of available therapies • Evaluate clinical evidence surrounding emerging insomnia pharmacotherapies, including safety, efficacy, adverse events, and risk-to-benefit ratios
PRE-ACTIVITY QUESTIONS
Question 1 How often do you incorporate insomnia assessment and treatment into management plans for your patients with common psychiatric comorbidities? A. Always B. Often C. Sometimes D. Rarely E. Never
Question 2 How confident are you in your ability to evaluate the strengths, limitations, and indications of current pharmacotherapies for the treatment of insomnia? A. Very confident B. Confident C. Somewhat confident D. Not confident
Question 3 Which of the following best describes the mechanism of action of current and emerging insomnia pharmacotherapies that target orexin signaling? A. Orexin receptor agonists that inhibit arousal B. Orexin receptor agonists that promote sleep C. Orexin receptor antagonists that inhibit arousal D. Orexin receptor antagonists that promote sleep
What proportion of the US adult population suffers
from insomnia on a daily basis?
A. 10%
B. 20%
C. 30%
D. 40%
E. 50%Prevalence of Insomnia
Second Highest Health-Related Complaint Worldwide
Never 2%
Rarely 4.4%
33% Every Night
A Few Nights per Month 25%
21% A Few Nights per Week
National Sleep Foundation. 2005 Adult Sleep Habits and Styles. www.sleepfoundation.org/professionals/sleep-america-polls/2005-adult-
sleep-habits-and-styles. Accessed February 28, 2019. Buscemi N, et al. Manifestations and Management of Chronic Insomnia in Adults:
Summary. Evidence Report/Technology Assessment No. 125. (Prepared by the Alberta Evidence-based Practice Center under Contract
No. C400000021.) AHRQ Publication No. 05-E021-1. Rockville, MD: Agency for Healthcare Research and Quality. 2005. Sleep Report.
www.sleepreviewmag.com. Accessed October 28, 2015.Case
• 71-year-old c/o unrefreshing sleep following retirement
• Onset 4 months ago
• Frequency 4 to 5 nights/week
• Mind “spins” at bedtime
• Feels washed out during day; low energy, moody, irritable
• No medical contributors
• MSE: Psychomotor slowing; mood “fine”. Affect restricted, no h/s
ideation, sensorium clear. Cognitive functions intact71-year-old c/o unrefreshing sleep 4 to 5 nights/week after retirement,
4 months ago; washed out, low energy, moody, irritable, meets MDD criteria.
What additional criterion must be met to satisfy
criteria for DSM-5 insomnia disorder?
A. Duration of insomnia must be > 6 months
B. Difficulty with insomnia must occur nightly
C. Sleep laboratory confirmation of a sleep latency (time to fall
asleep) > 1 hour
D. Must not meet criteria for MDD
E. Meets diagnostic criteria for insomnia disorder
MDD = major depressive disorder.Insomnia Disorder
A. Dissatisfaction with sleep quantity or quality with ≥ 1 of the following:
1. Difficulty initiating sleep (children: w/o caregiver intervention)
2. Difficulty maintaining sleep (children: w/o caregiver intervention)
3. Early morning awakening w/ inability to return to sleep
B. Significant distress or impairment
C. > 3 nights/week
D. > 3 months
E. Adequate opportunity for sleep
Specify if:
– With non-sleep disorder mental comorbidity
– With other medical comorbidity
– With other sleep disorder
Criteria F, G, and H not shown; not all specifiers shown.
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American
Psychiatric Association; 2013.Insomnia and Hyperarousal
Hyperarousal
HPA axis Increased
activation body metabolic
rate
Sympathetic
Cognitive
activation
arousal
Heightened
EEG
brain
arousal
metabolism
EEG = electroencephalogram; HPA = hypothalamic pituitary adrenal.Impairments Associated with Insomnia • Diminished ability to enjoy • Impaired concentration and family and social relationships memory • Decreased quality of life • Increased incidence of pain • Increased absenteeism and • Enhanced risk of present and poor job performance future psychiatric disorders • Motor vehicle crashes • Hypertension • Increased risk of falls • Diabetes • Increased health care costs • Increased mortality
Psychiatric Disorders Comorbid with Insomnia
Point Prevalence
Drug Abuse 4.2
Other Psychiatric Disorders 5.1
Alcohol Abuse 7.0
Dysthymia 8.6
Major Depression 14.0
Anxiety Disorder 23.9
No Psychiatric Disorder 59.5
0 10 20 30 40 50 60
Patients (%)
N=580.
Ford DE, et al. JAMA. 1989;262(11):1479-1484.Complex Relationship between
Insomnia and Mood Disorders
• Insomnia
– Is a common complaint in MDD
– Is more likely to emerge prior to, than during or after, MDD first
episode or recurrence
– Is associated with higher rates of lifetime and current MDD and
suicide
– Its presence and persistence predict future MDD
– Predicts poorer outcome in MDD (persistence, chronicity,
suicidality)
– Predicts the onset of mania in bipolar depression
McCall WV, et al. Curr Psychiatry Rep. 2013;15(9):389. Judd LL, et al. Arch Gen Psychiatry. 2008;65(4):386-394. Cho HJ, et al. Am J
Psychiatry. 2008;165(12):1543-1550. Breslau N, et al. Biol Psychiatry. 1996;39(6):411-418. Ohayon MM, et al. J Psychiatr Res. 2003;37(1):9-
15. Perlis ML, et al. Biol Psychiatry. 1997;42(10):904-913.Sleep Disturbances as Residual Symptoms following
Acute MDD Remission
50
45 Subthreshold
40 Threshold
Participants (%) (n=108)
35
30
25
20
15
10
5
0
Mood Interest Weight Sleep Psycho- Fatigue Guilt Concentration Suicidal
Disturbance motor Ideation
Patients with major depressive disorder (N=215) received fluoxetine 20 mg for 8 weeks. Presence of residual symptoms not predicted by
baseline demographic characteristics or Axis I and Axis II coexisting conditions.
Nierenberg AA, et al. J Clin Psychiatry. 1999;60(4):221-225.Selected Comorbid Conditions and Treatment
Examples
• Obstructive sleep apnea
– CPAP, BIPAP, oral appliances, upper airway surgery
• Restless legs syndrome
– Alpha 2-delta ligands, dopaminergic agents
• MDD
– Antidepressants
• GERD
– Proton pump inhibitors, H2 receptor blocker
• Shift work disorder
– Bedtime melatonin, modafinil/armodafinil prior to shift, bright light therapy
• Medication-induced insomnia
– Dosage or medication change
BIPAP = bilevel positive airway pressure; CPAP = continuous positive airway pressure; GERD = gastroesophageal reflux disease.
Doghramji K, et al. Focus: The Journal of Lifelong Learning in Psychiatry. 2009;7(4):441-445.Insomnia Evaluation and Management Algorithm
Insomnia Disorder Treat NO
Is insomnia No further
comorbid
persistent? treatment needed
condition first
Obtain details about YES YES
course of insomnia
Treat with
Is insomnia behavioral therapy
associated with
comorbid medical Is use of insomnia YES
Is insomnia contributing or psychiatric medication unsafe
condition? in this patient? NO
to decreased daytime YES Treat with behavioral
functioning and quality and/or pharmacologic
of life or worsening NO therapy
of chief complaint?
Does insomnia YES
NO occur
in isolation?
Possible short sleeper;
supportive reassurance
Doghramji Karl, et al. Clinical Management of Insomnia. Second Edition. 2015. Department of Psychiatry and Human Behavior Faculty
Papers. Paper 25.Treatments for Insomnia • Cognitive-behavioral therapy • Alternative nutraceuticals • Nonprescription pharmacologic agents (over-the-counter) • Prescription pharmacologic agents
Psychological and Behavioral Treatments for
Primary Insomnia
Techniques Method
Stimulus control therapy* If unable to fall asleep within 20 minutes, get OOB and repeat as necessary
Relaxation therapies* Biofeedback, progressive muscle relaxation
Restriction of time in bed
Decrease time in bed to equal time actually asleep and increase as sleep efficiency improves
(sleep restriction)
Cognitive therapy Talk therapy to dispel unrealistic and exaggerated notions about sleep
Paradoxic intention Try to stay awake
Sleep hygiene education Promote habits that help sleep; eliminate habits that interfere with sleep
CBT* Combines sleep restriction, stimulus control, and sleep hygiene education with cognitive
therapy
*Standard Treatment according to American Academy of Sleep Medicine.
CBT = cognitive-behavioral therapy; OOB = out of bed.
Morgenthaler T, et al.; American Academy of Sleep Medicine. Sleep. 2006;29(11):1415-1419. Bootzin RR, et al. J Clin Psychiatry. 1992;53
Suppl:37-41.Meta-analytic Support for Efficacy of CBT-i
• 20 RCTs (1162 participants [64% female; mean age, 56 years])
• Approaches to CBT-i incorporated at least 3 of the following:
cognitive therapy, stimulus control, sleep restriction, sleep
hygiene, and relaxation
• At the posttreatment time point
– SOL improved by 19.03 (95% CI, 14.12 to 23.93) minutes,
– WASO improved by 26.00 (CI, 15.48 to 36.52) minutes,
– TST improved by 7.61 (CI, 0.51 to 15.74) minutes, and
– SE% improved by 9.91% (CI, 8.09% to 11.73%)
• Changes seemed to be sustained at later time points. No adverse
outcomes were reported
CBT-i = cognitive-behavioral therapy for insomnia; RCT = randomized controlled trial; SE% = sleep efficiency; SOL = sleep onset latency;
TST = total sleep time; WASO = wake after sleep onset.
Trauer JM, et al. Ann Intern Med. 2015;163(3):191-204.The Dos of Sleep Hygiene
• Get OOB at the same time every morning
• Increase exposure to bright light during the day
• Establish a daily activity routine
• Exercise regularly in the morning and/or afternoon
• Set aside a worry time
• Establish a comfortable sleep environment
• Do something relaxing prior to bedtime
• Try a warm bath
Hauri PJ. In: Hauri PJ, ed. Case Studies in Insomnia; New York, NY: Plenum; 1991:65The Don’ts of Sleep Hygiene
Avoid…
• Alcohol
• Caffeine, nicotine, and other stimulants
• Exposure to bright light during the night
• Exercise within 3 hours of bedtime
• Heavy meals or drinking within 3 hours of bedtime
• Using your bed for things other than sleep (or sex)
• Napping, unless a shift worker
• Watching the clock
• Trying to sleep
• Noise
• Excessive heat/cold in room
Hauri PJ. In: Hauri PJ, ed. Case Studies in Insomnia; New York, NY: Plenum; 1991:65Effect of Blue Light Blocking on Sleep
Factors favoring the initial utilization of CBT over pharmacology in insomnia management include: A. Need for more rapid clinical improvement B. No comorbid medical conditions C. History of, or present, substance use disorder D. Time limitation
Pharmacotherapy vs CBT for Insomnia
Start with Pharmacotherapy Start with CBT
Lack of specific cognitive, or behavioral factors Need for sustained clinical improvement
Need for rapid improvement History of, or present, substance use/abuse
Time limitations Multiple comorbid medical conditions
Limited finances Hypnotic discontinuation
Shortage of trained therapists
Doghramji K, et al. Integrating psychotherapy and pharmacology in insomnia. In: de Oliveira, et al (Eds). Integrating Psychotherapy and
Psychopharmacology (Clinical Topics in Psychology and Psychiatry). First Edition. New York, NY: Routledge; 2014.Dietary Supplements
• Utilized by more than 50% of the US adult population
• Dietary substance
– Supplements existing diet
– Contains
• Vitamin
• Mineral
• Herb or other botanical
• Amino acid
• Others
– Taken orally
Bailey RL, et al. J Nutr. 2011;141(2):261-266. National Institutes of Health. Dietary Supplement Health and Education Act of 1994. Public
Law 103-417. 103rd Congress. https://ods.od.nih.gov/about/dshea_wording.aspx. Accessed February 28, 2019.Nonprescription Agents for Insomnia:
Limited Evidence for Hypnotic Efficacy
Product Latin Name (or Generic Name) Adverse Effects
Valerian root V. officinalis L. Restless sleep, gastrointestinal upset, headache,
contact allergies, mydriasis, possible carcinogen,
possible hepatotoxicity
First-generation histamine-1- Diphenhydramine hydrochloride, Vomiting, depression, malaise, drowsiness, impaired
receptor antagonists diphenhydramine citrate, doxylamine mentation, extrapyramidal reactions, rhabdomyolysis,
succinate dry mouth, weakness, gastrointestinal upset,
headache, impotence, urinary retention, increased
intraocular pressure
Meolie AL, et al.; Clinical Practice Review Committee; American Academy of Sleep Medicine. J Clin Sleep Med. 2005;1(2):173-187.Nonprescription Agents for Insomnia:
Insufficient Evidence for Hypnotic Efficacy
Product Latin Name Adverse Effects
Hops Humulus lupulus Unknown
Chamomile Matricaria recutita Vomiting, allergic reactions
Lemon balm Melissa officinalis Unknown
Fatigue, gastrointestinal upset, dizziness, anxiety,
St. John’s wort Hypericum perforatum
headache, photosensitivity, phototoxicity
Patrinia root Patrinia Scabiosaefolia Fisch Nausea
Niacin Niacin, niacinamide, vitamin B3 None known at recommended daily allowances
Magnesium Magnesium None known at recommended daily allowances
Vitamin B12, cyanocobalamin, None known at recommended hydroxocobalamin, daily
Vitamin B12
hydroxocobalamin, methylcobalamin allowances
Dietary changes Unknown
Yoku-kan-san-ka chimpi-hange Unknown
Meolie AL, et al.; Clinical Practice Review Committee; American Academy of Sleep Medicine. J Clin Sleep Med. 2005;1(2):173-187.Nonprescription Agents for Insomnia:
No Evidence of Hypnotic Efficacy or Significant Safety Concerns
Product Latin or Scientific Name Adverse Effects
Passionflower Passiflora incarnata Dizziness, confusion, ataxia, possible prolonged QT
Californian poppy Eschscholzia californica Unknown
Wild lettuce Lactuca virosa Possible hallucinogenic
Scullcap Seizures, possible hepatotoxicity
Calcium None known at recommended daily allowances
Vitamin A None known at recommended daily allowances
5-hydroxytryptophan Unknown
Natrum muriaticum Unknown
Jamaican dogwood Piscidia piscipula Toxicity to humans
Alcohol Dependence, neurotoxicity, cardiotoxicity, myelosuppression,
hepatotoxicity, respiratory depression, sedation, depression
L-tryptophan L-2-amino-3-(indole-3-yl) propionic acid Eosinophilia myalgia syndrome
Kava kava Piper methysticum Hepatotoxicity
Meolie AL, et al.; Clinical Practice Review Committee; American Academy of Sleep Medicine. J Clin Sleep Med. 2005;1(2):173-187.Melatonin Meta-analysis in Primary Sleep Disorders
• 19 placebo-controlled studies, 1683 participants
• Melatonin demonstrated efficacy in
– Reducing sleep latency (WMD = 7.06 minutes)
– Increasing total sleep time (WMD = 8.25 minutes)
• Effects magnified with longer duration and higher doses
– Improved sleep quality (standardized mean difference = 0.22)
• No significant effects of trial duration and melatonin dose
WMD = weighted mean difference.
Ferracioli-Oda E, et al. PLoS One. 2013;8(5):e63773.Melatonin Impairs Glucose Tolerance
Morning Evening
9 9 *
AUC120: P=.0002 * AUC120: P=.0002
Glucose (mmol/L)
Glucose (mmol/L)
8 ANOVArm: P=.002 8 *
ANOVArm: P=.001
*
7 * * 7
6 * 6
*
*
5 5
4 4
3 3
TF T30 T60 T90 T120 T180 TF T30 T60 T90 T120 T180
80 AUC120: P=.771 80 * AUC120: P=.007
*
70 70
Insulin (µU/mL)
Insulin (µU/mL)
ANOVArm: P=.992 ANOVArm: P=.004
60 60
50 50
40 40 Placebo
30 30 *
20 20
Melatonin
10 10
0 0
TF T30 T60 T90 T120 T180 TF T30 T60 T90 T120 T180
Time (min) Time (min)
Comparison between the effects of placebo and melatonin administrations on plasma glucose and insulin concentrations in response to
an oral load of glucose (75 g) performed in the morning (09:00) and evening (21:00). TF = time fasting; T30, 60, 90, 120, and 180, time after
OGTT (min); AUC120, paired t-test for AUC (melatonin and placebo) calculated with 120 min; ANOVArm, two-way ANOVA for time and
treatment effects with repeated measurements. When ANOVA was significant, paired t-test was used to evaluate times in which variations
were different. *Different from placebo at that time, PPrescription Agents for Insomnia
• FDA-non-approved for insomnia
– Sedating antidepressants
– Antipsychotics
– Anticonvulsants
• FDA-approved hypnotics
– Benzodiazepine receptor agonists
• Benzodiazepines
• Nonbenzodiazepines
– Melatonin receptor agonist
– H1 receptor antagonist
– Orexin receptor antagonistLow Dose Sedating Antidepressants for Insomnia
• Trazodone, doxepin, mirtazapine, paroxetine
• Advantages
– Sedating side effects
– Low abuse risk
– Large dose range
• Disadvantages
– Efficacy not well established for insomnia
– Side effects include daytime sedation, anticholinergic effects,
weight gain, drug-drug interactions
These agents are not FDA approved for insomnia.
Kupfer DJ, et al. N Engl J Med. 1997;336(5):341-346. Sharpley AL, et al. Biol Psychiatry. 2000;47(5):468-470. Karam-Hage M, et al.
Psychiatry Clin Neurosci. 2003;57(5):542-544. National Institutes of Health. Sleep. 2005;28(9):1049-1057.Low Dose Atypical Antipsychotics for Insomnia
• Quetiapine, olanzapine
• Advantages
– At appropriate doses, effective for psychotic disorders
– Low abuse potential
– Sedation
• Disadvantages
– Not well investigated in insomnia disorder
– Daytime sedation, anticholinergic effects, weight gain
– Risk of extrapyramidal symptoms, possible tardive dyskinesia
– Glucose and lipid abnormalities
These agents are not FDA approved for insomnia.
Kupfer DJ, et al. N Engl J Med. 1997;336(5):341-346. Sharpley AL, et al. Biol Psychiatry. 2000;47(5):468-470. Karam-Hage M, et al.
Psychiatry Clin Neurosci. 2003;57(5):542-544. National Institutes of Health. Sleep. 2005;28(9):1049-1057.Which of the following brain neurotransmitters is
involved in sleep generation?
A. Histamine
B. GABA
C. Serotonin
D. Norepinephrine
E. EpinephrineArousal and Sleep-Promoting Systems
Arousal Sleep
Posterior
lateral
hypothalamus
(orexin)
5-HT = serotonin; Ach = acetylcholine; BF = basal forebrain; DA = dopamine; DR = dorsal raphe nucleus; GABA = gamma-aminobutyric
acid; Gal = galanin; LC = locus coeruleus; LH = lateral hypothalamic; MCH = melanin-concentrating hormone; NE = norepinephrine; ORX =
orexin; PPT/LDT = pedunculopontine and laterodorsal tegmental; TMN = tuberomammillary nucleus; VLPO = ventrolateral preoptic
nucleus; vPAG = ventral periaqueductal gray matter.
Modified from Fuller PM, et al. J Biol Rhythms. 2006;21(6):482-493. Silber MH, et al. Neurology. 2001;56(12):1616-1618.Orexins/Hypocretins
• Hypothalamic peptides
– Localized in the dorsolateral hypothalamus
– Wide projections throughout the brain
– Projections found in the spinal column
• Peptide neurotransmitters
– Arousal
– Locomotion
– Metabolism
– Increase blood pressure/heart rate
Peyron C, et al. J Neurosci. 1998;18(23):9996-10015. Moore RY, et al. Arch Ital Biol. 2001;139(3):195-205. Silber MH, et al. Neurology.
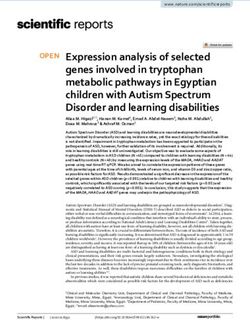
2001;56(12):1616-1618.Elevated Plasma Orexin-A Levels in Insomnia Disorder
120
*
100
Orexin-A Level (pg/mL)
80
60
40
20
0
Normal Sleepers Insomnia Patients
228 patients with insomnia disorder vs 282 normal sleepers.
Tang S, et al. Peptides. 2017;88:55-61.Benzodiazepine Receptor Agonists:
Benzodiazepines
Dosage Range† Half-life Short-term
Medication Onset of Action
(mg) (h) Limitation?
Estazolam 0.5–2 Rapid 10–24 Yes
Flurazepam 15–30 Rapid 47–100 Yes
Quazepam 7.5–15 Rapid 39–100 Yes
Slow–
Temazepam 7.5–15 9.5–12.4 Yes
Intermediate
Triazolam 0.25–0.50 Rapid 1.5–5.5 Yes
†Normal
adult dose. Dosage may require individualization.
MICROMEDEX. www.micromedex.com. PDR. www.PDR.net.A 60-year-old man complains of insomnia; he falls asleep rapidly after going to
bed, but wakes up repeatedly starting at 1 AM, feeling fatigued the next day.
What is the least appropriate medication?
A. Zolpidem ER
B. Ramelteon
C. Eszopiclone
D. Doxepin low dose
E. SuvorexantSelective Benzodiazepine Receptor Agonists
Zaleplon Zolpidem Zolpidem ER Eszopiclone
Dose (mg) [elderly] 5, 10, 20 [5] 5, 10 [5] 6.25, 12.5 [6.25] 1, 2, 3 [1]
Tmax (hours) 1 1.6 1.5 1
Half-life (hours) [elderly] 1 2.5 [2.9] 2.8 [2.9] 6 [9]
Sleep Latency ↓ ↓ ↓ ↓
Wake after Sleep Onset -- -- ↓ ↓
↑
Total Sleep Time ↑ ↑ ↑
(20 mg)
Schedule IV IV IV IV
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/.Newer Hypnotics
Ramelteon Doxepin Suvorexant
Melatonin receptor Dual orexin receptor
Mechanism H1 receptor antagonist
agonist antagonist
Dose (mg) [elderly] 8 3, 6 [3] 10–20
Tmax (hours) 0.75 3.5 2
Half-life (hours)
1–2.6 15.3 12
[elderly]
Sleep Latency ↓ -- ↓
Wake after Sleep Onset -- ↓ ↓
Total Sleep Time -- -- ↑
Schedule None None IV
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/.Zolpidem Variants
Zolpidem Zolpidem SL Zolpidem SL Zolpidem Oral Spray
Men: 3.5; Women: 1.75
[1.75]
Dose (mg) [elderly] 5,10 [5] 5,10 [5] 5,10 [5]
MOTN, 4 hours remaining
until AM awakening
Tmax (hours) 1.6 1.4 1.3 0.9
Half-life (hours) [elderly] 2.5 [2.9] 2.9 2.5 2.7
MOTN = middle-of-the-night; SL = sublingual.
US Food and Drug Administration. Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/.Adverse Effects of Hypnotics
• Benzodiazepine receptor agonists • H1 receptor antagonist
– Daytime sedation, psychomotor and – Somnolence/sedation
cognitive impairment (depending on – Nausea
dose and half-life)
– Upper respiratory tract infection
– Rebound insomnia • Orexin receptor antagonist
– Respiratory depression in vulnerable
– Somnolence
populations
– Risk of impaired alertness and motor
– DEA Schedule IV coordination, including impaired
• Melatonin receptor agonist driving; increases with dose
– Headache, somnolence, fatigue, – Contraindicated in narcolepsy
dizziness – DEA Schedule IV
– Not recommended for use with
fluvoxamine due to CYP 1A2
interaction
Mitler MM. Sleep. 2000;23 Suppl 1:S39-S47. Holbrook AM, et al. CMAJ. 2000;162(2):225-233. Charney DS, et al. In: Hardman JG, et al (Eds). Goodman
and Gilman’s The Pharmacological Basis of Therapeutics. Tenth Edition. McGraw Hill; 2001:399-427. US Food and Drug Administration.
Drugs@FDA: FDA Approved Drug Products. www.accessdata.fda.gov/scripts/cder/daf/. MICROMEDEX. www.micromedex.com.Driving Safety:
MOTN Low-Dose Zolpidem SL
7.5
SDLP Change from Placebo (cm)
5.0
+2.5 cm threshold
2.5
for impairment
0
-2.5 cm threshold
-2.5
for impairment
-5.0
M F M F M F
ZST 4h ZST 3h ZOP
SDLP = standard deviation of lateral position; SL = sublingual; ZOP = zopiclone; ZST = zolpidem sublingual tablet.
Vermeeren A, et al. Sleep. 2014;37(3):489-496.The risk of parasomnias
during hypnotic use is enhanced by:
A. Co-administration with sedating agents
B. MDD
C. Younger age
D. Female gender
E. Lower socioeconomic statusZolpidem-Induced Parasomnias
• Spontaneous reports
• Sleep-driving; preparing and eating food, making phone calls, or having sex
• Amnesia for events
• Risk factors
– Co-use of alcohol or sedatives
– Use at doses exceeding the maximum recommended dose
– Sleep disorder: OSA or PLMS
– H/O parasomnia
– Ingestion at unusual bedtime
– Ingestion while agitated or not typically asleep
– Ingestion when sleep deprived
– Poor management of pill bottles
– Living alone
PLMS = periodic limb movements of sleep; OSA = obstructive sleep apnea.
Poceta JS. J Clin Sleep Med. 2011;7(6):632-638.Selected Considerations in Choosing a Hypnotic Agent
• Initiation or maintenance insomnia
– Initiation: Zaleplon, zolpidem, ramelteon
– Maintenance: Doxepin low dose, zolpidem SL MOTN
– Initiation and maintenance: Zolpidem ER, eszopiclone, suvorexant
• Respiratory compromise; safety in mild to moderate OSA/COPD
– Ramelteon, suvorexant
• Abuse potential
– Lowest: Ramelteon, doxepin
• Prior failure of selected medication
• Patient preference
COPD = chronic obstructive pulmonary disease.
PDR. www.PDR.net. Sun H, et al. J Clin Sleep Med. 2016;12(1):9-17. Kryger M, et al. Sleep Breath. 2007;11(3):159-164.Insomnia Complaints in MDD
• 80% inpatients
• 40% outpatients
• Reduced quantity
– Initial
– Middle
– Early morning awakening
• Reduced quality
• Unrefreshing sleep
Reynolds CF 3rd, et al. Sleep. 1987;10(3):199-215.RCTs of Hypnotic Agents in
Conjunction with SSRI in MDD
• Zolpidem 10 mg vs PBO for persistent insomnia following SSRI (fluoxetine, sertraline,
paroxetine) Rx for MDD or dysthymia
– Improvement in subjective sleep measures
• Zolpidem ER 12.5 mg plus escitalopram vs PBO plus escitalopram in MDD patients with
insomnia
– Improvement in subjective sleep measures
– Improvement in next day functioning
• Eszopiclone 3 mg plus fluoxetine vs PBO plus fluoxetine in MDD patients with insomnia
– Improved subjective sleep measures
– Improved quality of life
– Higher overall MDD remission rates
• Suvorexant 10 to 20 mg vs PBO for persistent insomnia following stable antidepressant
management for MDD
– Study in progress at 3 sites
Hypnotics are not FDA indicated for treatment of MDD.
PBO = placebo; SSRI = selective serotonin reuptake inhibitor.
Asnis GM, et al. J Clin Psychiatry. 1999;60(10):668-676. Fava M, et al. Biol Psychiatry. 2006;59(11):1052-1060. Fava M, et al. J Clin Psychiatry. 2011;72(7):914-928.
McCall WV, et al. J Clin Sleep Med. 2010;6(4):322-329. ClinicalTrials.gov Identifier: NCT02669030.Hypnotics Under Development
• Dual and single orexin receptor • Melatonin receptor agonists
antagonists – Controlled release melatonin for
– Lemborexant elderly (Circadin®)
– TCS-OX2-29 – Piromelatine
– Seltorexant – Others
• Benzodiazepine receptor agonists • Beta-blockers
– Controlled release zaleplon • Histamine H1 antagonists
– Inhaled zaleplon • 5-HT2A receptor antagonists
– Lorediplon • Adenosine receptor agonists
– EVT-201 • Angiotensin II receptor 1 antagonist
• Cannabinoid agonistLemborexant
• Dual orexin receptor antagonist; is thought to regulate sleep and wake by dampening
wakefulness without hindering the ability to awaken to external stimuli
• Controlled study in insomnia disorder demonstrated improvement in sleep latency and
continuity
• Phase 2 study under way for irregular sleep-wake rhythm disorder and mild to moderate
Alzheimer’s dementia
• New drug application (NDA) submitted to FDA for insomnia disorder January 15, 2019
– SUNRISE 1 and SUNRISE 2; N=~2000
– SUNRISE 1: 1-month, double-blind, placebo-controlled study; Phase 3 head-to-head
comparison vs zolpidem ER; objectively assessed sleep parameters (time to sleep
onset, sleep efficiency, and wake after sleep onset)
– SUNRISE 2: 12-month study; subjectively assessed for ability to fall asleep and stay
asleep based on patient self reports (sleep diaries)
• Adverse effects: Somnolence, headache, sleep paralysis, rapid eye movements
abnormal sleep, nightmare, abnormal dreams, dizziness, back pain, hypnagogic
hallucinations, myalgia, feeling drunk
Murphy P, et al. J Clin Sleep Med. 2017;13(11):1289-1299. Study of the Efficacy and Safety of Lemborexant in Subjects 55 Years and Older
With Insomnia Disorder (SUNRISE 1). ClinicalTrials.gov Identifier: NCT02783729. Long-term Study of Lemborexant in Insomnia Disorder
(SUNRISE 2). ClinicalTrials.gov Identifier: NCT02952820.Lemborexant Morning Driving Performance and
MOTN Body Sway
Means with 95% CI Lemborexant 2.5 mg
10 Zopiclone 7.5 mg Lemborexant 5 mg
8 Lemborexant 10 mg
Individual SDLP Difference
from Placebo Value (cm)
6
4
2.4
2
30
Change from Baseline
0
in Body Sway (units*)
Placebo (N=56)
LS Mean (95% CI)
-2 -2.4 20
-4 Zolpidem 6.25 mg (N=56)
-6 10
Lemborexant 5 mg (N=56)
-8 Lemborexant 10 mg (N=56)
-10 0
ZOP LEM 2.5 LEM 5 LEM 10 ZOP LEM 2.5 LEM 5 LEM 10
(N=48) (N=32) (N=32) (N=32) (N=48) (N=32) (N=32) (N=32) -10
Day 2 Day 9 Middle of the Night
*A unit of body sway is defined as 1/3 degree angle of arc movement of the ataxiameter. Dashed horizontal line indicates threshold for
clinically meaningful change from baseline.
Vermeeren A, et al. Sleep. 2018 Dec 31;[Epub ahead of print]. Murphy P, et al. Auditory awakening threshold to evaluate ability to awaken
after administration of lemborexant versus zolpidem. Sleep. 2018;41(Suppl 1):A156- A157.The Future in Insomnia Treatments
• Refining pharmacotherapy
– Higher efficacy, remission (cure?)
– Fewer side effects
– Novel mechanisms
– Selection of hypnotic based on receptor profile or comorbid
conditions
• Development of hypnotic devices
– Mobile electronics to stratify and treat insomnia
– Thermal devices
• Online CBT
• Improving health outcomes through insomnia treatmentConclusions • Insomnia is highly prevalent in psychiatric patients • It is associated with psychological and physical impairments and enhances the risk of psychiatric conditions • Management begins with a systematic evaluation followed by treatment of comorbidities • Whenever possible, treat the comorbid disorder • Insomnia can be directly managed by CBT and pharmacologic agents
POST-ACTIVITY QUESTIONS
Question 1 How often will you incorporate insomnia assessment and treatment into management plans for your patients with common psychiatric comorbidities? A. Always B. Often C. Sometimes D. Rarely E. Never
Question 2 How confident are you in your ability to evaluate the strengths, limitations, and indications of current pharmacotherapies for the treatment of insomnia? A. Very confident B. Confident C. Somewhat confident D. Not confident
Question 3 Which of the following best describes the mechanism of action of current and emerging insomnia pharmacotherapies that target orexin signaling? A. Orexin receptor agonists that inhibit arousal B. Orexin receptor agonists that promote sleep C. Orexin receptor antagonists that inhibit arousal D. Orexin receptor antagonists that promote sleep
Q&A
You can also read