Minnesota e-Health Advisory Committee Meeting - Co-Chairs: Alan Abramson | Sonja Short February 15, 2019 - Minnesota ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Minnesota e-Health Advisory Committee Meeting
Co-Chairs: Alan Abramson | Sonja Short
February 15, 2019
Topics on Today’s Agenda
Legislative Update
HIE Task Force
E-Prescribing Workgroup
Minnesota e-Health Summit
MN e-Health Interoperability Steering Committee
Consumer Engagement
21st Century Cures Act and Other e-Health Initiative
Updates
Wrap-up and Next Steps
2
Minnesota e-Health Initiative Charge – Vision
A public-private collaboration established in 2004
Legislatively chartered
Coordinates and recommends statewide policy
on e-Health
Develops and acts on statewide e-health
priorities
Reflects the health community’s strong
commitment to act in a coordinated, systematic
and focused way
Vision: “All communities and individuals benefit from and are
empowered by information and technology which advances
health equity and supports health and wellbeing.”
3
Legislative Update from MDH
Diane Rydrych & Jennifer Fritz
February 15, 2019
Minnesota e-Health HIE Task Force Update
Task Force Co Chairs: Peter Schuna & George Klauser
Outline for Today
• Updates
• Progress on deliverables
• Timeline for remaining meetings
• Summary of agreements and accomplishments
• Discuss and provide input on critical success factors
• Request for Advisory Committee endorsement
6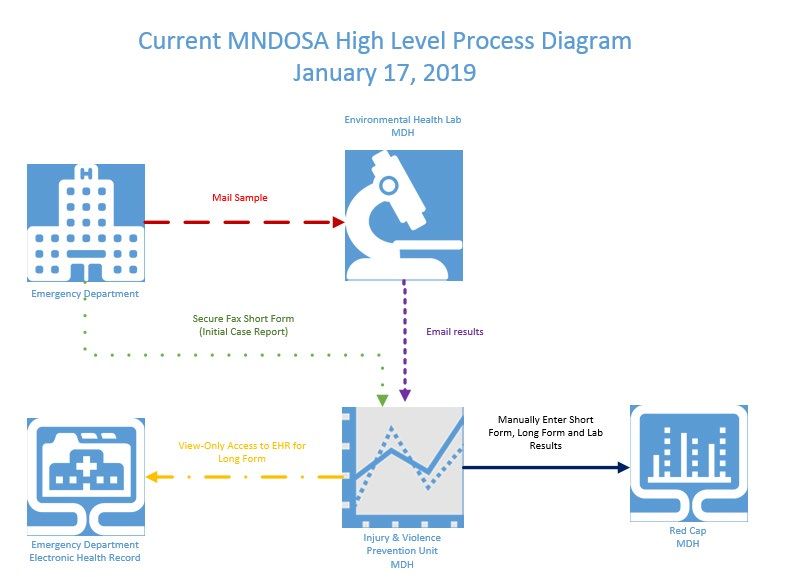
Progress on HIE Task Force Deliverables
Deliverable 1: Action steps for 2018-2019 to implement connected networks by
building upon existing HIO and national network connections
• Recommendation 1 endorsed by e-Health Advisory Committee on 9/28
Deliverable 2: An implementation plan for 2018-2019 with measureable targets
• Implementation Plan subgroup for recommendation 1 established and has met four
times, draft plan for review by Task Force soon
Deliverable 3: A plan for five-year interim governance, authority, and financing
with the goal of optimal HIE
• Governance discussion started in September, essential elements identified in
November, continues today with focus on critical success factors and expectations
Deliverable 4: Recommended policy updates to Minnesota’s HIE Oversight Law
• HIE Review Panel had initial discussion; further action as needed in concert with
Deliverable 3
7
Timeline for completing HIE Task Force deliverables
February 28 Make preliminary recommendations to address critical success
factors of alignment and financial commitment as well as authority
and financing (focus on essential elements for defining services and
determining governance). Deliverable 3
March 21 Review preliminary recommendations for Advisory Committee
consideration at April meeting (continue Deliverable 3)
April 18 Review Advisory Committee modifications and make final
recommendations for Deliverable 3. Make suggestions for initial
changes to HIE oversight law & related laws (Deliverable 4) for
Advisory Committee consideration at May meeting
May 30 Review Advisory Committee modifications to recommendations and
develop plan for public comment in June.
August Restart HIE Workgroup - meet to review and revise recommendations
September Final Recommendations for Advisory Committee consideration; move
forward on implementation
8
Minnesota Connected Networks Approach and
Governance Framework (all the gold)
Nodes of the Other Stakeholders of
Connected Networks the Connected Networks
Preferred Centralized
Services of the Federal initiatives
Connected Networks (e.g., TEFCA)
healthcare Payers
directory
DHS
patient
directory
MDH
routing
mechanism Quality Reporting
Other state
agencies/programs
Other state or
national initiatives
9
Summary of Accomplishments and Future Focus Areas
Refer to handout- Summary of HIE Task Force Accomplishments …
Purpose:
To acknowledge and highlight the work of the HIE Task Force, including
activities, discussion and consensus toward a Minnesota connected
networks approach.
HIE Task Force promoting incremental approach (focus) to ensure the most
value and/or return on investment.
Questions or comments?
10Identified Critical Success Factors (Key Issues)
Deliverable 3- Plan for five-year interim governance, authority, and financing
1) Full participation is needed to achieve the most value for all
• Dependent on commitment by large health systems- key data contributors
2) One or more HIO(s) is needed to fill HIE connectivity gaps (e.g., smaller,
independent providers, LTPAC, BH, social services)
• Dependent on ensuring sustainability for one or more HIO as “safety-net”
3) Financial commitment by all participants (nodes and other
stakeholders) is needed to ensure long-term sustainability
• Dependent on participant fee structure (e.g., fees for centralized services)
4) Alignment with other HIE activities (national, federal and state) is
needed to achieve an efficient and effective network (e.g., minimize
connections, reduce/eliminate duplicate services)
• Dependent on flexible governance process that can evolve to meet HIE needs
11Discussion
Critical Success Factors
• To what extent do you agree that these are critical success
factors for Minnesota Connected Networks overall? Why?
• Are there others?
• Do you have suggested strategies for any of the critical
success factors?
12Critical Success Factor - Full Participation
Common strategies
Full participation is needed to achieve the most value for all
• Dependent on commitment by large health systems- key data
contributors
Summary of common strategies discussion at January 31 meeting
• support for payer incentives, payer requirements, state government
incentives or requirements, and stand up one or more centralized
services incrementally (patient directory, healthcare directory and/or
routing services)
• strongest support was behind “stand up one or more centralized services,
incrementally” to help demonstrate multi-stakeholder value and/or
return on investment
• strongest support for patient directory to improve patient matching
13Incremental Approach Strategy
• Using a centralized patient directory or other patient
matching service, the HIE Task Force will:
• Discuss governance needs (e.g., essential elements)
• Make recommendations for governance, financing
and authority
• Apply these recommendations to other centralized
services or connected networks services as needed.
14Discussion
Incremental Approach Strategy
What are your initial thoughts on this strategy?
To what extent do you agree with this strategy?
Are there other priority strategies that should be
considered?
15Request for Advisory Committee Action
Endorse:
• Move forward, using an incremental approach, to
discuss governance needs using a centralized
patient directory or other patient matching service.
• General direction for next three months, plan for
public comment period and final recommendations
in September
16e-Prescribing Workgroup Update
Karen Soderberg, MDH
Laura Topor, Granada HealthOverview
• Purpose: Advance comprehensive implementation of e-prescribing standard
transactions and procedures by Minnesota’s stakeholders.
• The work will address two key issues:
• Increasing adoption of electronic prescribing of controlled substance by Minnesota’s
prescribers.
• Documenting and developing stakeholder consensus on addressing barriers to full
implementation of the NCPDP SCRIPT standard and e-prescribing processes.
Stakeholders include prescribers, dispensers, payers, and pharmacy benefit managers.
• Co-chairs:
• Steve Simenson, Goodrich Pharmacy
• Lee Mork, Allina Health
• Meetings held 11/14/18, 1/8/19 and 2/13/19
18Matrix of issues
• Prescriber-Pharmacist communication
• There is not an efficient and fast way for prescriber and pharmacist to
communicate (except by phone).
• Cancel messages
• There is slow uptake of the RxCancel function on both prescriber and pharmacy
sides.
• Workflow and technical challenges need to be addressed.
• Indication and/or diagnosis information on script and label
• Allows pharmacists to better counsel patients and identify issues.
• Patients are more likely to adhere if they know why they are taking meds.
• Pharmacy systems are enabled to receive; need to have prescriber send it.
• Could help in obtaining prior auth from payer if diagnosis code is included on
claim.
19Issues, continue
• Formulary and benefit information
• Often out of date or inaccurate.
• Information on alternatives, if sent, is sorted alphabetically rather than using a logic model to
identify preferred alternatives at point of care.
• Real-time benefit checks will help; proprietary solutions are in use but no industry standards.
• e-Prior Authorization
• Some are still doing this retrospectively (i.e., pharmacy-directed) due to inaccurate formulary
and benefit data.
• MN requirements (from AUC) don’t align.
• MME (morphine milligram equivalent) decision support
• Several MME calculators exist but formulas appear to be inconsistent and don’t include
liquid and patches. Pediatric calculator in Epic is not safe.
• Medication lists and reconciliation
• Real-time information is needed for a single source of truth for medications.
• Need to think not just about opioids, but also future information needs. Be prepared to
manage the next crisis.
20Next steps
• Road show outreach
• Continue to flesh out issues and opportunities
• Potentially identify an “eUC” use case to develop
• Next meeting on March 14 (2-4pm; location TBD) – Join us!
• Questions? Contact Karen.Soderberg@state.mn.us
21Minnesota e-Health Summit Planning
Sue Severson| Jennifer Fritz
February 15, 2019Minnesota e-Health Summit
15th Anniversary Summit: Information that Works
Thursday, June 13, 2019
Keynote Speaker
Dr. Vindell Washington
Executive Vice President and Chief Medical Officer
Blue Cross and Blue Shield of Louisiana
2315th Anniversary Minnesota e-Health Summit
New Venue: Minnesota Landscape Arboretum
2415th Anniversary e-Health Summit
Current Opportunities
New Sponsorship Levels (see handout)
Refer Potential Sponsors/Exhibitors
Sign-up today
Share ideas on program format:
Plenary session topics/panels/learning labs
25Minnesota e-Health Interoperability Steering Committee
Jennifer Fritz
February 15, 2019E-Health MDH Interoperability Advisory Group
Membership
• Cathy Gagne, PHN, St. Paul-Ramsey Department of • Emily Emerson, Assistant Division Director, Infectious
Public Health Disease Epidemiology, Prevention, and Control,
Minnesota Department of Health
• Nancy Garrett, Chief Analytics Officer and Senior Vice
President for Information Technology, Hennepin • Myra Kunas, Assistant Division Director, Public Health
HealthCare Laboratory, Minnesota Department of Health
• Jonathan Shoemaker, SVP and Chief Information and • Chuck Stroebel, Assistant Division Director, Health
Improvement Officer, Allina Health Promotion and Chronic Disease, Minnesota
Department of Health
• Meyrick Vaz, Vice President, Strategic Market
Partnerships, UnitedHealthcare Office of the CIO • Jennifer Fritz, Director, Office of Health IT, Minnesota
Department of Health
• Shawn Kammerud, Chief Information Security
Officer\Director Service Management, Minnesota IT • Karen Welle, Director, Office of Data Strategy and
Services, Partnering with Minnesota Department of Interoperability, Minnesota Department of Health
Health
• Tony Steyermark, Supervisor of MDH Interoperability,
• Heather Petermann, Division Director, Health Care Office of Health IT, Minnesota Department of Health
Research & Quality, Minnesota Department of Human
Services
27E-Health MDH Interoperability Advisory Group
February 6 Meeting Update – Summary of Discussion
• Reviewed charter
• Provided an overview of MDH interoperability scope of work, roles and
responsibilities within MDH
• Discussed current barriers and opportunities related to interoperability
with MDH
• Today’s work is built on the groundwork laid by the e-Health Advisory
Committee starting in 2009 on Interoperability, Standards, and Meaningful
Use.
• Develop list of MDH Interoperability projects (in process)
• Develop a State Agency Community of Interest for Interoperability
• Need for plain language and common understanding of the data security
architecture is important for building trust and relationships
• Next Meeting: April 2019
28Promoting Interoperability Progress to date (Examples)
• Electronic Laboratory Reporting (ELR)
• Working with hospitals to onboard, developing HL7 2.5.1 message importing capability,
application system improvements
• Infectious Disease Laboratory
• New application development with full HL7 messaging capacity, developing plan to identify
pilot sites and piloting process
• Immunizations
• Working with clinics and hospitals to onboard, application system improvements, updating
documentation for meaningful use reporting to identify opportunities for standardization
and efficiencies, working to pilot onboarding through a Health Information Organization
• Newborn Screening Program
• Developing requirements for electronic lab ordering
• Blood Lead Program
• Developing requirements for improved electronic data exchange
29MDH Coordination Progress to date
• Interviewing for Director of Office of Data Strategy and Interoperability
• Drafting and implementation of MDH interoperability roadmap
• Enhancements to MDH internal exchange infrastructure (MDH Data Exchange /
Orion Rhapsody) to meet program and stakeholder needs
• Funding to incentivize connectivity through a Health Information Organization
for Promoting Interoperability program (Meaningful Use)
• Continued work on MDH Interoperability Data Inventory
• Development of MDH Interoperability Communication Plan
• Planning for submitting application for 90/10 funding for Federal Fiscal Years 2020
and 2021
30Remember,
Don't forget!
Consumers
How to engage
with e-Health
Initiative
Activities?Terms Ending – June 30, 2019
• Dentists (1 yr) • Pharmacists (1 yr)
• Long Term Care (2 yr) • Large Hospitals (2 yr)
• Expert in HIT (2 yr) • Vendors (2 yr)
• Consumer (2 yr) • Health Care Purchasers & Employers
(2 yr)
• Research (2 yr)
Next Steps:
• Incumbents will receive an email with instructions for re-applying
• A public call for applicants will be issued by the Minnesota Secretary of State
• Expand / assist recruitment to seek more diverse participation &
membership
Optional Tagline Goes Here | mn.gov/websiteurl 32Co-Chair Nomination and Selection Process
Appointing Authority
• Commissioner appoints Co-Chairs from amongst Advisory Committee members
Nominating Co-Chairs
• Nominations taken from Committee members including co-chairs and alternates
Term Cycle
• Two-year staggered term cycle to ensure continuity in leadership
Process:
• Members will receive email with request to nominate candidates for Co-Chair
vacancy. Respond in 10 days by email to Bob Johnson at
bob.b.Johnson@state.mn.us
3321st Century Cures Act Proposed Rule
Kari Guida | Senior Health InformationProvider Burden Coordinated Response
Kari Guida | Senior Health InformationStrategy on Reducing Regulatory and Administrative Burden
Relating to the Use of Health IT and EHRs Report
• Released in November 2018, Submitted January 2019
• Three primary goals for reducing health care provider burden:
• Reduce the effort and time required to record information in EHRs for health care
providers during care delivery.
• Reduce the effort and time required to meet regulatory reporting requirements for
clinicians, hospitals, and health care organizations.
• Improve the functionality and intuitiveness (ease of use) of EHRs.
• https://www.healthit.gov/sites/default/files/page/2018-
11/Draft%20Strategy%20on%20Reducing%20Regulatory%20and%20Administ
rative%20Burden%20Relating.pdf
36Coordinated Response
Prioritized Recommendations
• Continue to reduce overall regulatory burden around documentation of patient encounters.
(Clinical Documentation, Strategy 1, Recommendation 1)
• Leverage data already present in the EHR to reduce re-documentation in the clinical note. (Clinical
Documentation, Strategy 1, Recommendation 2 )
• Evaluate and address the other process and clinical factors contributing to burden associated
with prior authorization. (Clinical Documentation, Strategy 3, Recommendation 1)
• Continue to promote nationwide strategies that further the exchange of electronic health
information to improve interoperability, usability, and reduce burden. (Health IT Usability and the User
Experience, Strategy 4, Recommendation 4)
• Federal agencies, in partnership with states, should improve interoperability between health IT
and PDMPs through the adoption of common industry standards consistent with ONC and CMS
policies and the HIPAA Privacy and Security Rules. (Public Health Reporting, Strategy 1, Recommendation 1)
• HHS should increase adoption of electronic prescribing of controlled substances with access to
medication history to better inform appropriate prescribing of controlled substances. (Public Health
Reporting, Strategy 1, Recommendation 2)
37e-MNDOSA Project Kari Guida & Company
Minnesota Drug Overdose and Substance Use Pilot
Surveillance System (MNDOSA)
MNDOSA is a surveillance system to track emergency department visits and
hospitalizations attributable to the recreational use of drugs and other
substances, excluding alcohol alone.
Surveillance of suspected overdose or substance use will allow us to:
• determine the burden of substance use/overdoses seen in select emergency
departments and hospitals in Minnesota
• identify clusters of ED visits/hospital treatment for drug overdoses
• identify substances causing clusters, unusual or atypical clinical presentation, and severe
illnesses in order to inform approaches to treatment and prevention
• describe the populations most affected to help focus and guide prevention efforts
39Current MNDOSA High Level Process Diagram
40e-MNDOSA Project
Overview
e-MNDOSA Project: assessing options for electronic standards-based
exchange of information from emergency departments to MDH for drug
overdose events
• CDC “Surge” funding was awarded in the fall of 2018 to combat the opioid crisis
(Sept 2018 – Aug 2019)
• Injury and Violence Prevention Section (IVPS) and the Office of Health Information
Technology (OHIT) are collaborating on e-MNDOSA Project and its objectives:
• Train IVPS staff in informatics, e-health, the Minnesota and public health reporting e-health
ecosystems, standards-based exchange, etc.
• Engage local, state and federal partners to provide guidance and recommendations to
implement and pilot e-MNDOSA.
• Identify robust requirements for standards-based exchange for drug overdose surveillance
through e-MNDOSA.
• Develop recommendations and next steps for standards-based exchange for e-MNDOSA.
41Methods and Approach
• Using a collaborative team model
• IVPS and OHIT
• Leveraging stakeholder engagement
• Advisory Group, Interested Individuals, MN e-Health Initiative, and more
• Applying a multi-prong approach
• Assess Information, Workflow, and Requirements
• Develop and Validate Models (current and future)
• Discover Opportunities for Improvement
42Initial Advisory Group Discussion
Identifying patients that meet the case definition is difficult. The following are
considerations when thinking about identifying patients:
• There is not one ICD-10 code that meets the MNDOSA case definition. There are 1)
numerous codes for drug overdoses; 2) various ways the codes are implemented both within
a facility and across facilities; and 3) gaps in the codes (not all types of drugs individuals
overdose on are in the code set).
• When figuring out this issue, need to consider implications of over reporting and
underreporting.
• Providers are looking at symptoms and do not know about drug use until the labs come back
which can be the first time drug use is noted in the medical record.
• Altered mental state is used to assure the encounter gets billed. This includes for alcohol and
other drug overdoses.
43Connected to Minnesota e-Health Initiative
• Crossover between participants
• Provide updates and seek input at Advisory Committee meetings
• Interested in more detail, contact kari.guida@state.mn.us
44Operationalizing Value Based Health Care in a
Fee for Service world
Brief Update: CAQH/CORE Value Based Purchasing Advisory Group
Minnesota e-Health Advisory Committee
February 15, 2019
PROTECTING, MAINTAINING AND IMPROVING THE HEALTH OF ALL MINNESOTANSPurpose – create awareness, seek input
• MDH is part of a national CAQH/CORE Advisory Group advising on “operating
rule” development/updates to address the needs of the payment continuum
from FFS to VBP.
• MDH is seeking input and feedback to provide as part of its advisory role.
2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 46Overview • CORE background • CORE study and findings • Next steps 2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 47
CAQH/CORE
• More than 130 organizations – providers, health plans, vendors, government
agencies, and standard-setting bodies – developing operating rules to simplify
healthcare administrative transactions
• Designated the Secretary of the Department of Health and Human Services
(HHS) as the author for federally mandated operating rules per Section 1104 of
the ACA.
• Operating rules: (per ACA) “the necessary business rules and guidelines for the
electronic exchange of information that are not defined by a standard or its
implementation specifications.”
2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 48CORE 18 Month Study and Report
• “The success of value-based payment is … dependent upon smooth and
reliable business interactions between all stakeholders … especially between
healthcare providers and health plans.”
• CAQH CORE conducted an 18-month study to examine value-based payment
operational processes
• Identify opportunity areas that, if improved, would streamline implementation of
value-based payment.
All Together Now: Applying the Lessons of Fee-for-Service to Streamline Adoption of Value-Based Payments. CAQH-CORE.
https://www.caqh.org/sites/default/files/core/value-based%20payments/core-value-based-payments-report.pdf
2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 49How well does the existing model work? 2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 50
Findings and challenges
• VBP models require certain information to be deployed earlier in the workflow
and/or exchanged more often.
• New data unique to VBP models are also needed at various stages of the
revenue cycle
• As the types of VBP models continue to grow and vary, providers and health
plans will need consistent and uniform methods to exchange this information
in a timely, cost- effective manner.
2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 51Non-uniformity is currently the norm in value-based
payment implementation
More standardization is needed
•… especially for “data quality and
standardization, interoperability, patient risk
stratification, provider attribution and quality
measurement.”
Don’t let history repeat itself!
All Together Now: Applying the Lessons of Fee-for-Service to Streamline Adoption of Value-Based Payments. CAQH-CORE.
https://www.caqh.org/sites/default/files/core/value-based%20payments/core-value-based-payments-report.pdf
2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 52CORE Advisory group
• Review “challenges and opportunities”
• Translate to possible priorities for operating rules, other standardization
efforts
• Meeting over next several months
2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 532/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 54
More information • Contact: David Haugen MDH Administrative Simplification Program David.Haugen@state.mn.us Thank you. (See additional following “outtake” slides for additional information) 2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 55
“Outtake #1”-- Value Based Health Care
• “… a healthcare delivery model in which providers, including hospitals and
physicians, are paid based on patient health outcomes.”
• “Value-based care differs from a fee-for-service or capitated approach, in
which providers are paid based on the amount of healthcare services they
deliver. The “value” in value-based healthcare is derived from measuring
health outcomes against the cost of delivering the outcomes.”
What Is Value-Based Healthcare? NEJM Catalyst, January 1, 2017 https://catalyst.nejm.org/what-is-value-
based-healthcare/
2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 56“Outtake #2” -- VBP brings new demands, challenges
• Much more data needed
• Quality
• Attribution of patients to providers
• “Apples to apples comparisons” -- Risk assessment, risk adjustment
• Differing, siloed systems
• Claims vs. EHRs
• Separate data warehouses and reporting
• Differing terminology, language
2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 57“Outtake #3” -- Don’t let history repeat itself • Many features of value-based payment do not align with the current fee-for-service operational system. • …. proprietary systems and processes for implementing value-based payment have already begun to introduce operational variations. • Without collaboration to minimize variations, the current environment is ripe for repeating a scenario that cost stakeholders billions of dollars and slowed and complicated adoption of fee-for-service transactions. • … by applying lessons learned…, CAQH CORE hopes to energize an effort to ease value-based payment operational inefficiencies. 2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 58
“Outtake #4” 2/14/2019 P RO TECTIN G, MAIN TAIN IN G AN D IMP RO VIN G THE HEAL TH O F AL L MIN N ESO TAN S 59
Meeting Wrap-up
Next Steps
Upcoming Workgroup/Task Force Meetings
Consumer Engagement - Patient Journey Mapping: Monday, February 25 12:00 -2:00
p.m. Normandale Community College
HIE Task Force: Thursday, February 28 9:00 a.m. – 12:00 p.m. | Wellstone Center
Next Advisory Committee Meeting
Monday, April 22, 2019, 1:00 p.m. – 4:00 p.m. | Medtronic, Fridley
2019 Minnesota e-Health Summit: Information that Works.
Save the Date: June 13, 2019 | Minnesota Landscape Arboretum, Chaska
60You can also read