Miti, presunzioni ed evidenze in obesità pediatrica - FBK per la Salute
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Gestione multidisciplinare e integrata tra ospedale e
territorio del paziente sovrappeso-obeso in età pediatrica
Trento, sabato 16 maggio 2015
Miti, presunzioni ed evidenze in obesità pediatrica
Claudio Maffeis
UOC Pediatria ad Indirizzo Diabetologico e Malattie del Metabolismo
Centro Regionale Specializzato in Diabetologia Pediatrica
AOUI e Università di Verona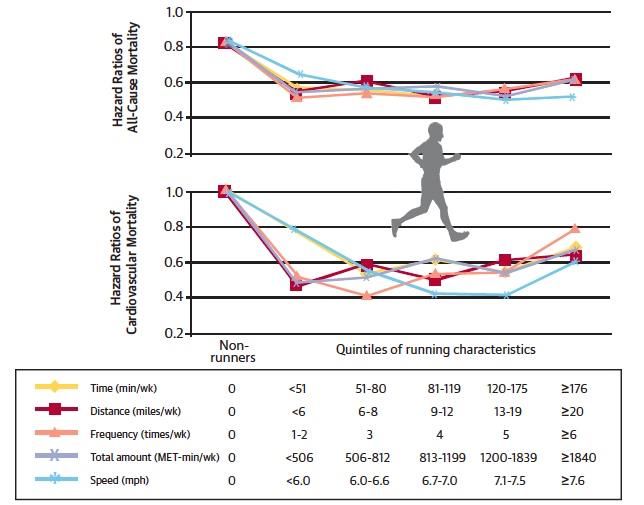
Prevalenza di sovrappeso ed obesità
nei bambini di 8-9 anni in Italia
Okkio alla Salute 2014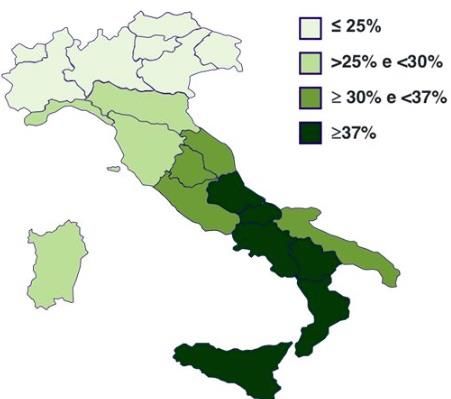
Prevalenza di sovrappeso e obesità
in Italia tra I 2 ed I 6 anni
Overweight
25,0%
20,0%
15,0% males
females
10,0% totale
5,0%
0,0%
National reference I.O.T.F. C.D.C.
Obesity
18,0%
16,0%
14,0%
12,0%
males
10,0%
females
8,0%
totale
6,0%
4,0%
2,0%
0,0%
National reference I.O.T.F. C.D.C
Maffeis C et al. Obes Res, 2006
Il bambino obeso “brucia” meno calorie rispetto al bambino normopeso: Ingrassa perché ha un difetto termogenetico!
total energy expenditure in normal weight
and obese prepubertal children
2500 P
components of the total daily energy expenditure of a 10-year-old boy kcal/day 2,000 EEGrowth
basal energy expenditure of 9-year-old children
obese post-obese never-obese
1,300
energy p < 0.05
expenditure
(kcal/day)
1,000
energy 1,300
expenditure
adjusted for FFM
p = ns
(kcal/day)
1,000
Maffeis C, et al. Int J Obes ‘92meal-induced thermogenesis
obese post-obese never-obese
% 6 p = ns
meal
energy
3
0
Molnar D et al. Eur J Pediatr ‘85
Maffeis C et al. Eur J Clin Nutr ‘92Il bambino ha bisogno di tanta energia per crescere
Spesa energetica per l’accrescimento
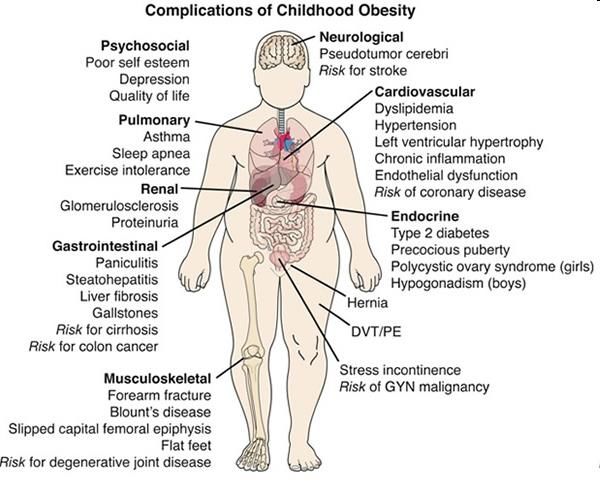
Il bambino obeso non ha un vero problema di salute: ha solo qualche chilo di troppo!
OBESITÀ
ACCUMULO
INFIAMMAZIONE
ECTOPICO DI GRASSO d d
d
d
a
INSULINO
INSULIN d
RESISTENZA
RESISTANCE
m
*
*
a *
Ipertensione
Sbarbati M, Maffeis C, et al.
dislipidemia Pediatrics 2006
IGT – T2D
Franzese A, Vajro P, et al.
Dig Dis Sci 1997 SINDROME
METABOLICABasta un po’ di volontà e il peso in più si perde facilmente!
primary care surveillance and intervention for overweight or obese 5-
10-year-old children: the LEAP 2 randomised controlled trial
INTERVENTION
4 standard consultations over 12 weeks targeting change
in nutrition, physical activity, & sedentary behaviour,
supported by purpose designed family materials
25
P = ns
BMI
(kg/m2)
20 baseline
6 months
12 months
15
intervention control
primary care screening followed by brief counselling is not effective In overweight
or mildly obese children and it would be very costly if universally implemented
Wake M, et al BMJ 2009Two-year Follow-up in 21,784 Overweight Children
and Adolescents With Lifestyle Intervention
129 treatment centers 5 centers with the highest success rate
SDS BMI SDS BMI SDS BMI SDS BMI
lost of reduction reduction lost of reduction reduction
follow-up 0.5 follow-up 0.5
100 100
(%) (%)
80 80
60 60
40 40
20 20
0 0
6 12 24 6 12 24 6 12 24 6 12 24 6 12 24 6 12 24
time (months) time (months)
Reinehr T, et al Obesity 2009Se un bambino nasce con basso peso bisogna alimentarlo con abbondanza per fargli recuperare presto il peso….. in difetto!
Fattori di rischio di obesità
Peso alla nascita
Peso a termine (kg)
2.5 4.5Odds ratio for childhood obesity by infant weight gain
between 0 and 1 year adjusted for sex, age, a weight
Lakshman R, et al. Circulation 2012;126:1770-9.Velocità di crescita primo anno
12
Peso (kg)
8
4
0
45 55 65 75
Lunghezza (cm)Se il latte della mamma scarseggia, diamo il latte di vacca che è buono e fa crescere bene!
FORMULA PROTEIN CONTENT AND WEIGHT GAIN
A RANDOMIZED CLINICAL TRIAL
1.0
*
Weight/
Lenght 0.5 * High protein formula
(z score) Human Milk
0 Low protein formula
-0.5
-1.0
1 3 6 12 24 Age(months)
Socha P, et al. Am J Clin Nutr. 2011;94(6 Suppl):1776S-1784SSe il bambino viene allattato al seno non diventerà mai obeso!
2013;368:446-54.
BREAST-FEEDING AND OBESITY
“…. Although existing data indicate that breast-feeding does not
have important antiobesity effects in children, it has other
important potential benefits for the infant and mother and should
therefore be encouraged. “Se il piccolo ha tanta fame e cresce bene posso introdurre gli alimenti solidi anche presto, dopo i primissimi mesi di vita
Timing of Solid Food Introduction and
Risk of Obesity in Preschool-Aged Children
Huh SY, et al. Pediatrics 2011;127:e544Una caloria è una caloria: poco importa se è da proteine, grassi o carboidrati
nutrient requirements
350 carbohydrate
g/day
250
150 protein
50
lipid
0
0 6 12 18
Age (years)fatty food
more palatable
high energy density
50
less satiating
fat
mass
(%)
25
r = 0.28 P< 0.01
0
10 30 50
Klesges RC et al. AJCN ‘94
lipid intake (% of energy intake)
Gazzaniga JM, et al.AJCN ‘93
Maffeis C et al. Int J Obes ‘96covert manipulation of dietary fat and energy density: effect on
substrate flux and food intake in men eating ad libitum
fat balance MJ energy balance
MJ
20 20 high fat
medium fat
15 15
low fat
10 10
5 5
0 0
- 5 - 5
- 10 - 10
0 1 2 3 4 5 6 7 0 1 2 3 4 5 6 7
time (days) time (days)
Stubb RJ, et al. AJCN 1995; 62:316-29.dietary pattern prospectively associated with increased adiposity
during childhood and adolescence
High Risk
Dietary Pattern
Energy-dense
High-fat
Low-fiber
Ambrosini GL, et al. Int J Obes 2012;36:1299-1305high-fibre, low-fat diet predicts long-term weight loss and decreased
type 2 diabetes risk: the Finnish Diabetes Prevention Study
6
low-fat/ low-fat/ high-fat/ high-fat/
high fibre low fibre high fibre low fibre
5
Hazard
ratio
for 4
Diabetes *
3
2
1
0
•Adjusted for: group assignment, age, sex, baseline BW, fat & fibre intake,
baseline 2-h glucose, baseline and follow-up period physical activity, weight change
Lindstrom J, et al. Diabetologia 2006Joint classification of whole- and refined-grain intake
on visceral adipose tissue (VAT) volume
McKeown N M et al. Am J Clin Nutr 2010;92:1165-1171Blood glucose and triacylglycerol postprandial profile
MIXED
MEAL
Plasma 150
glucose &
TAG triacylglycerol
120
(mg/dl)
90
glucose
60
-30 0 60 120 180 240
Time (min)Postprandial triacylglycerol profile after two isocaloric, isoproteic
meals with different fat and carboidrate content in obese children
LF meal
Fat/Carbohydrate
140
140
Fat/Carbohydrate
HF meal
TAG 130
120
(mg/dl) 120
110
100
100
90 p< 0.05
80
80
70
60
60
0'0 60' 100
90' 120' 150'200180' 240' 300'
300
Time (min)
Maffeis C, et al. Obesity 2010POSTPRANDIAL PRO-ATEROGENIC PROFILE: change of oxidized lipoprotein concentration in obese children after two isocaloric, isoproteic meals with a different fat and carbohydrate content ox-LDL P
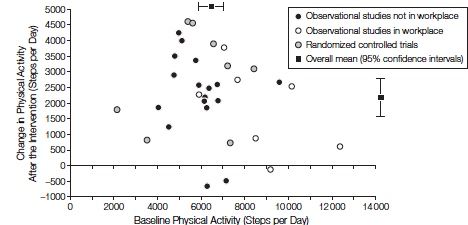
Per calare si deve fare attività fisica ad elevata intensità!
Using pedometers to increase physical activity and improve health
Bravata DM, et al. JAMA 2007;298:2296-304.Efficacy of a 12 Weeks Exercise Program without
Diet in Reducing Obesity in Men
Exercise: brisk walking/light jogging, 80% max HR, 700 kcal/day.
0 -2 -4 -6 -8 - 10
Body weight (kg)
Waist circumference (cm)
Body fat (kg)
Subcutaneous abdominal fat (kg)
Visceral abdominal fat (kg)
VO2max (L/min)
Ross R, et al. Ann Intern Med. 2OOO;133:92-1O3.energy expenditure during walking and running in obese
and nonobese prepubertal children
10
METs
7.5
OBESE
5
Pthe role of free-living daily walking in human weight gain and obesity
Levine JA et al. Diabetes 2008Nutrient oxidation measured during walking at speeds of 4, 5,
and 6 km/h, respectively, in a group of obese prepubertal children
Maffeis, C. et al. JCEM 2005;90:231-236Leisure-Time Running Reduces All-Cause and Cardiovascular
Mortality Risk In a 15-year follow-up
Lee D, et al. J Am Coll Cardiol 2014;64:472-81Leisure-Time Running Reduces All-Cause and Cardiovascular
Mortality Risk In a 15-year follow-up
Running, even 5 to 10 min/day and at
slow speedsNon preoccupiamoci: se la “dieta” fallisce ci sono farmaci e chirurgia
Expert Committee Recommendations Regarding the Prevention,
Assessment, and Treatment of Child and Adolescent
Overweight & Obesity: Summary Report
Barlow SE & the Expert Committee Pediatrics 2007 (suppl.) (modified)
Obiettivi comportamentali della terapia
Allattamento al seno
Colazione
Pasti consumati in famiglia (vs Fast Food)
Alimentazione bilanciata in nutrienti (RDA)
Frutta e vegetali, Fibra
Densità energetica dei cibi e dei pasti
Porzioni
Bevande zuccherate
(Calcio)
Video-esposizione
Attività fisicaTake home message L’obesità è una malattia, che va prevenuta e curata con attenzione. Gli obiettivi per l’intervento sono chiari. Gli strumenti: accanto all’alimentazione, l’attività fisica svolge un ruolo di assoluto rilievo. Il risultato potrà essere favorevole nel medio-lungo termine solamente se famiglia, pediatra, scuola (e società) collaboreranno attivamente e con pazienza allo scopo.
SAVE THE DATE
VIII° CONGRESSO NAZIONALE:
NUTRIZIONE, METABOLISMO E DIABETE NEL
BAMBINO E NELL’ADOLESCENTE
La pediatria dà i… “numeri”?
Hotel CTC Best Western
Verona, 25-26 settembre 2014You can also read