National Health Cluster Coordination Meeting - November 18th 2020 Sana'a, Yemen
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
National Health Cluster
Coordination
Meeting
November 18th 2020
Sana’a, Yemen
Agenda
• Introduction/Action Point follow up
• Updates from various coordination fora,
• Yemen Humanitarian Senior Official Meeting II SUMMARY
• [
• Epidemiological updates of Communicable Diseases: MOH
❖Cholera, DF and diphtheria, SARI updates
• [
• Updates on
• HCWs payment ongoing discussion for HC Payment policy 2021.
• JIAF- a preparatory step for HPC 2021–HNO 2021,
• 1st Standard Allocation 2020 & progress
• Updates of TWGs
❖MHPSS, Nutrition, EPI/vaccination
• AOB
#
Action Points/ Subjects to Follow Up Responsibility Status
1 There is need to work together to identify the contributory factors to cholera Health Cluster, Cholera
cases decline (agree on type of assessment) Pending
Task force
2 Health Cluster Infographics, Central Level and Hubs, to be shared with partners
on a monthly basis. Health Cluster Ongoing
Yemen Health Cluster Website: www.Yemenhc.org
3 Keep health partners informed on the updates on HNO 2021 Health Cluster Ongoing
4 All selected projects will be recommended to coordinate with MOH for the Ongoing
Health Partners
assessment before they finalize and submit the proposals
5 Health Cluster/ Ongoing/
Health partners are requested to report any utilization decrease - impact
partners Critical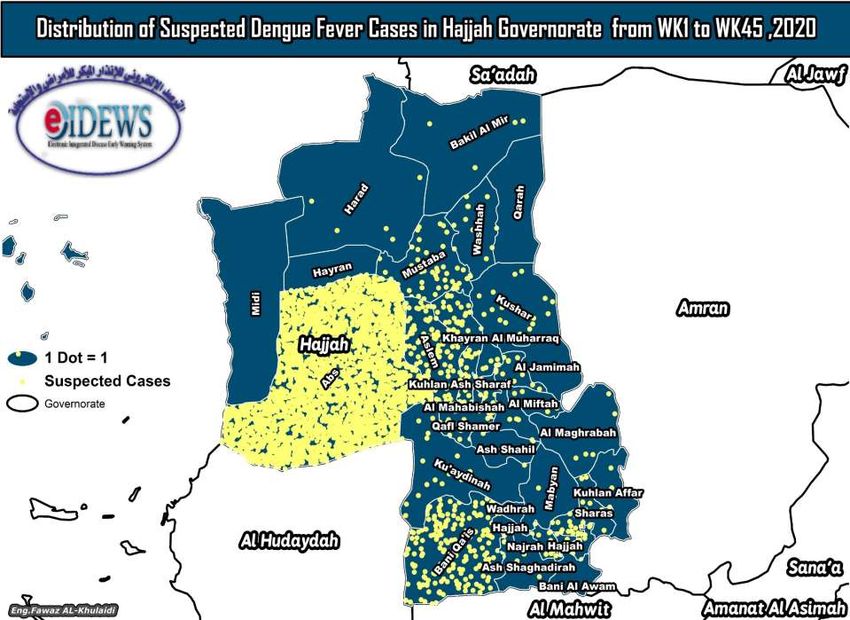
➢Yemen Humanitarian Senior Official Meeting (SOM) II-Summary
• Participation (online) of the main humanitarian actors/donors active in the country.
• SOM- 2 assessed the deteriorating crisis and expressed their commitment to continue acting collectively
along the following lines.
• Yemen shows marked deterioration of the humanitarian crisis, including the imminent risk of famine, due
to increased violence and economic struggles, compounded by shortages of funding, restricted
humanitarian space, politicization of aid and limited imports of basic commodities.
• A spiraling economic collapse, exacerbated by the outbreak of COVID-19 (global) is a realistic prospect
• The humanitarian response in 2020 is severely underfunded and additional resources are urgently required
• Humanitarian actors reiterated their firm commitment to continue providing life-saving support to the
people of Yemen in line with donor accountability regulations and the humanitarian principles of humanity,
neutrality, independence and impartiality.
• Donors reaffirmed the seven areas, which parties to the conflict must respect in Yemen to enable access and
allow accountability, efficient, effective and principled delivery of assistance (Avoid taxation of humanitarian
aid,….,)
• Humanitarian actors agreed that, if and where the operating environment limits or obstructs the flow of
principled and accountable aid, humanitarian programs will continue to be adapted and recalibrated
SOM- 2 SUMMARY 1. Maintain a regular, constructive and consistent dialogue with all parties, assess the situation and its progress in the next months and reconvene before the 2021 pledging conference for Yemen. 2. Increase urgent advocacy, including at the highest level, with the parties for the respect of International Law, including International Humanitarian Law and International Human Rights Law, and the protection of civilians. 3. Intensify engagement with relevant Yemeni parties to facilitate the implementation and monitoring of progress of the seven areas to ensure principled humanitarian delivery. 4. Continue to adapt and recalibrate their programs to adjust to circumstances on the ground in Yemen, whenever the operating environment limits or obstructs the flow of principled and accountable aid. 5. Continue to mobilise and increase much needed funding in Yemen to preserve life-saving assistance – such as food, water, healthcare, nutrition and protection – with focus, on the most pressing and acute needs in the country. With the aim of avoiding a prospect of further downscaling of programmes by humanitarian actors in the coming months due to a lack of funding, substantial additional resources, including development funding, and prompt disbursements are urgently needed before the end of 2020 and in early 2021. 6. Mobilise a support package to prevent the economic collapse, including renewal of proven measures like foreign-exchange injections, as well as identify concrete modalities allowing a more focused developmental and financial support to address the drivers of the crisis in order to keep Yemen from the brink of collapse. 7. Follow up by dispatching high-level missions by the UN, NGOs and donors, where appropriate, to pursue advocacy on humanitarian matters pertaining to the Yemen crisis.
Updates on outbreak
Cholera, DF, SARI and Diphtheria
Current situation
Challenges
Way forward
MoPHP – EOC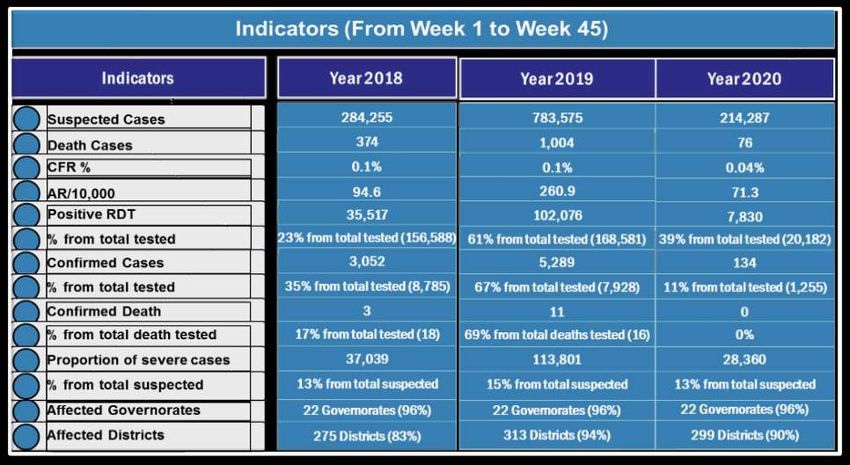
Summary of AWD / Cholera indicators During 2018 ,2019 and 2020

Epidemiological Curve of AWD / Cholera Cases (Cumulative from WK1 ,2019 to WK45 ,2020)
Top Governorates (from WK1 to WK45,2020)
Summary of Cholera indicators During Last 3 Weeks (43,44,45)
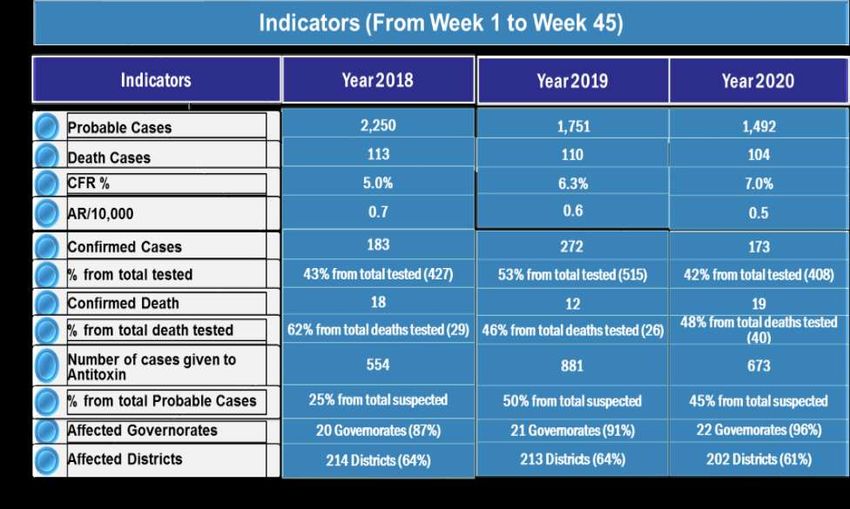
Summary of Diphtheria indicators During
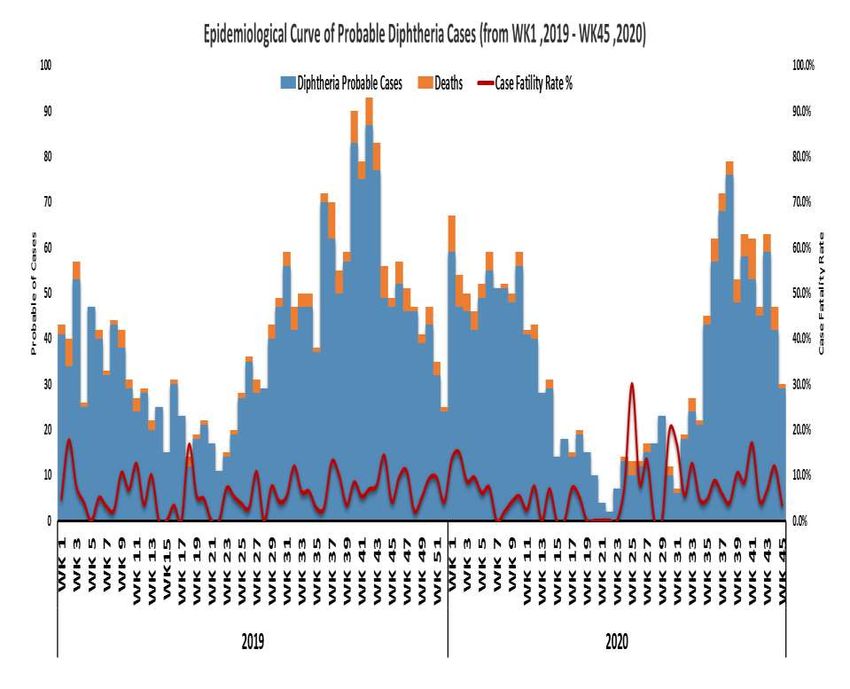
2018 ,2019 and 2020Epidemiological Curve of Probable Diphtheria Cases
(Cumulative from WK1 ,2019 to WK45 ,2020)Summary of Diphtheria indicators During Last 3 Weeks (43,44,45)
Distribution of Probable Diphtheria Cases by Governorates
(From WK42 – WK45 ,2020)Summary of DF indicators During 2018 ,2019 and 2020
EPI-Curve of DF Cases with CFR% (Cumulative from WK1 ,2019 to WK45 ,2020)
Summary of DF indicators During Last 3 Weeks (43,44,45)
Distribution of DF Cases by Governorates
(From WK42 – WK45 ,2020)Summary of SARI indicators During 2018
,2019 and 2020EPI-Curve of SARI Cases with CFR% (Cumulative from WK1 ,2019 to WK45 ,2020)
Summary of SARI indicators During Last 3 Weeks (43,44,45)
Challenges and Recommendations
التحديات والتوصيات
التحديات التي تواجه إدارة الترصد الوبائي
❑قلة الحاالت المؤكدة مخبريا في نظام الترصد الوبائي بسبب عدم توفر
مختبرات خاصة بالترصد الوبائي بالمحافظات ماعد المختبر المركزي
باالمانة باإلضافة الي الحديدة بشكل غير مكتمل
❑شحة اإلمكانيات والموارد الخاصة بنقل العيانات من المديريات الي
المحافظات ثم الي المختبر المركزي للفحص مثل:
❖ عينات الكرونا والحصبة والشلل والكوليرا والدفتيريا والضنك وغيرها
من االمراض في قائمة الترصد الوبائي ( 28مرض)تابع التحديات..
❑ عدم توفر ثالجات لحفظ العينات المخبرية و وعدم توفر نفقات النقل
❑ ضعف االشراف والمتابعة والتقييم الميداني المركزي علي مواقع الترصد
الوبائي ومراكز معالجة الدفتيريا والكوليرا وفرق االستجابة السريعة
بالمديريات بسبب عدم توفر الميزانيات المخصصه لمثل هذه األنشطة
الهامة
❑ عدم اطالع كتلة الصحة بالوزارة بالمخصصات واألنشطة المتوفرة لدى
أعضاء الكتلة ليتم التنسيق معهم لالستفادة من هذه المخصصات والموارد
بالشكل األفضل وفي المناطق ذات األولويةتوصيات إدارة الترصد الوبائي
❑ بناء مختبرات خاصة بالترصد الوبائي بالمحافظات ودعم هذه
المختبرات للقيام بعمل فحص العينات او تخزينها
❑ توفير اإلمكانيات والموارد الخاصة بنقل العيانات من المديريات الي
المحافظات ثم الي المختبر المركزي للفحص مثل عينات الكورونا
والحصبة والشلل والكوليرا والدفتيريا والضنك وغيرها من االمراض
❑ توفير ثالجات لحفظ العينات المخبرية وتوفير نفقات النقلتابع التوصيات..
❑ توفير ميزانيات مخصصه لالشراف والمتابعة والتقييم الميداني
المركزي علي مواقع الترصد الوبائي ومراكز معالجة الدفتيريا
والكوليرا وفرق االستجابة السريعة بالمديريات
❑ إطالع كتلة الصحة بالوزارة بالمخصصات واألنشطة المتوفرة لدى
أعضاء الكتلة ليتم التنسيق معهم لالستفادة من هذه المخصصات
والموارد بالشكل األفضل وفي المناطق ذات األولويةUpdates on the HCWs payment
(incentives/Top-up/Allowances)
Ongoing HC partners’ discussion for HC Payment policy
2021.
&
SurveyModalities of payment support • Incentive: A monetary contribution to encourage one to deliver services. This is not a replacement for the salary rather a reward offered for increased productivity (or to avoid disruption of service and promote lifesaving health services). • Allowance: An amount provided regularly for a defined period for a specified purpose within a set of regulations • Top-up: Addition to an amount to bring it up to a certain level (as a compensation). • Hazard Pay: Means additional pay for performing hazardous duty or work involving physical hardships and risk of exposure to hazardous circumstances. • Per-Diem: The term "per diem" means "daily"; Per diem refers to very short- term temporary employment that consists of just a few days of employment • Extra Duty Allowance: any allowance payable to healthcare staff who are given special assignments or perform additional duties in the evening & night shifts
Background
• Ongoing crisis and deteriorating economic situation
• Devaluation of the Yemeni riyal and Disproportional Inflation
• Constrained access to services and commodities
• Increasing costs of transportation
• Inability of the government to pay salaries to staff (No salaries to staff in the
North while nominal salary in the south, volunteerism OR Non-salaried staff)
• Weak and fragile health system and services due to deficient HR
• Weak monitoring of the health system and services
• Inability to meet the demand of health services
• Difficulty in finding trained HR for projects in remote districts/HTR areas
• Socio-economic hardships of the health workers
• Donors willingness/ fatigue and decreased fundingCurrent Situation and Proposed remedial steps
SOUTH NORTH
Non employed Staff Non employed Staff
Employed MoPHP staff Employed MoPHP staff
(Volunteers) (Volunteers)
Current Situation Current Situation
Nominal Salary in IRG areas No Salary No Salary No Salary
Proposed Proposed
Top-up Allowance Allowance AllowanceHow much and till when (should be paid?)
• According to the level and scale or grade of the health worker
• According to the scope of work
• According to level of difficulty; access; remoteness; risks involved
• Benchmark: Govt. pay scale or Private sector/UN/NGO scale (competitive
scales)
OR
• Previous Health & Nutrition cluster Incentive standardization exercise (2019)
• For the period of HRP 2021 / Standard Allocation project duration
• Current circumstances points toward non-favorable situation will persist in
the year 2021 and even may worsen due to which the govt. inability to pay
salariesIncentives Paid in 2019
Primary Modality of Payment for Incentives Monitoring systems for
incentives
Micro-financing bank (Al Khurami) 22, 52%
Direct payment through local money transfer… 15, 36%
Other modality # of organizations with a monitoring system
5, 12%
Sources of Funding for Incentives No, 21,
40%
# of organizations
0 5 10 15 20 25 Yes, 31,
Yemen Pool Fund 60%
WHO
OFDA
ECHO Frequency of post-distribution monitoring
UNFPA
Organization own reserves
German MOFA (GFFO)
UNICEF Monthly, 19, 61% Quarterly, 9, 29%
King Salman Humanitarian Aid and Relief Centre
Canada (GAC)
SIDA
EKFS
Belgium (DGD)
Other Other,
3, 10%
Other sources specified: DFID, CDCS Centre de crise et de soutien (France Government), OCHA, WFP, Italy,
Kuwait, UAE Aid, USAID, Caritas, SV, Japan, Finland, Alawn Foundation For Development - Selah Foundation.Min, Max and Avg amts (in USD) paid for incentives compared to 2018 harmonized and 2014 MoH scales
2018 Harmonized
Staff Category Oct 2019 Survey 2014 MoH
Scale
Min Max Median
Doctors
General Practitioner (GP) / Doctor 317 1,200 715 650 267
Specialist (Arab Board) 787 2,125 1,527 1,500
Specialist (Master) 417 2,125 1,416 1,200 288
Specialist (Diploma) 209 2,000 1,048 1,000
Paramedics
Nurse (BSc) 108 447 298 350 235
Nurse (technical nurse / Assistant) 137 400 244 200
Pharmacist 108 511 307 400 228
Medical assistant 137 447 312 350 235
Midwife 80 450 296 350 191
Technicians
Technicians (OT, X-ray, Laboratory , Anesthesia ,
160 590 293 250 235
physiotherapy)
Data Registrar 108 286 189 200
Physiotherapist 236 336 286
Vaccinators 80 400 251
Supporting staff
Ambulance driver 78 300 212 200
Driver 100 300 190 150
Cleaner 27 303 149 150
Guard 70 256 147 150
Coordinators/Managers/Supervisors
Central level 108 2,000 924
Governorate level 54 1,500 551
District level 32 1,000 396
Health facility level 90 709 263
Community based workers
Community Health Worker 55 250 110
Community Health Volunteer 18 100 58The need for Sustainable solutions • Govt resume to pay salaries • Govt. negotiate with development partners • Social Security schemes (Insurance….) through developmental partners • Set up Social Fund for Development • Cost recovery/cost sharing
Recommendations and Way Forward • Advocacy document for the CLA and Donors • Kobo survey sharing with HC partners - (Done) • Ongoing discussion • Payments Monitoring • Clear Exit strategy by December 2021 or later.
18 November 2020 Incentive Survey
Organizations that Participated
36Support for Incentives among Organizations
17%
Yes No
83%Reasons for Supporting the Payment of Incentives • Without incentives, Health workers will NOT provide services • Without incentives, Health system will collapse in Yemen • Government pays nominal salary(only in the south) to health workers; therefore, not enough as per the high cost of livings caused by super inflation and the free fall of YER • Incentive is the only motivation for health workers to work in rural and hard to reach areas. • Non employed health workers(Volunteers) are not paid salary by the government. • Projects cannot be implemented in HF without incentives
Reasons for NOT Supporting the Payment of Incentives • Lack of funding • Donors are restricting incentives • It is the duty of government to pay salary to health workers
Impact of Non-Payment of Incentives
3%
Yes No
97%Impact of non-payment of incentives • Quality of Healthcare will deteriorate since health workers will not be committed to their responsibilities, as they will looking for other source of income(no pay, no work) • The Healthcare system will collapse; the number of non-functional health facilities will increase exponentially • Humanitarian aid organization would not be able to implement projects in health facilities without incentives • The gains made in health and nutrition indicators will be lost.
Government Salaries Adequate for health Workers?
8%
14%
Don't Know
No
Yes
78%Who should be paid? • Define Cadres; their scales and their scope of work (Doctors; paramedics; Nurses; Midwives; Auxiliary satff; Volunteers) • Top officials (Central level); GHO/DHO; Managers/coordinators • Standardization, harmonization of scale • Address duplications among staff using Common platform – Emergency Cash Transfer (ECT) • Transparency, Utilization • Top-up for salaried worker • Incentive/allowance for volunteer OR non-salaried • Hazard pay for additional responsibility such as outbreak response by RRTs, Laboratory workers; Cholera/Covid Treatment centre workers
Who should be paid incentives?
Employed Staff NOT receiving salary from
31 5
government(North specific)
Employed Staff receiving salary from government
20 16
(South specific)
Voluntary Staff - NOT on MoPHP payroll list (North
32 4
and South)
Yes No 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%Cadres that are Priority for Incentives
Low Priority High Priority
Priorities 1 2 3 4 5
Specialist 11% 6% 19% 25% 39%
General Practioner (GP) 3% 3% 8% 17% 69%
Medical Assistant 3% 3% 6% 19% 69%
Nurses 3% 0% 5% 14% 78%
Pharmacists 3% 0% 14% 41% 41%
Laboratory Staff 3% 3% 14% 39% 41%
Midwives 3% 0% 3% 11% 83%
Others (cleaners, guards etc..) 3% 3% 16% 25% 53%
GHO/DHOs 33% 11% 33% 17% 6%Support for Revision of Incentive Scale
36%
64%
No - (maintain current harmonized health cluster scale endorsed by MOPHP)
YesQuestions and comments?
Yemen – COVID-19
Main Figures as of 02.11.2020
2067 603 1376
Confirmed Cases Deaths Recovered
29% (11/22) (50%) Last reported cases 0
Governorates affected 0
CFR% Last reported deathsYemen – COVID-19 Activity Update Hazard Pay Program SOUTH: - Initiation of the program is expected to begin in the South within the coming days to cover 21- 34 hospital staff members directly involved with C-19 patient management. Hazard Pay Program North: - list of eligible staff to receive payment expected to be received in the coming days from MoPHP in the North Triage Program of training: - to be available next month - To support non-COVID-19 facilities and provided essential connections to Case Management and IPC
Yemen – COVID-19 Activity Update Global Partnership: - to make available 120 million affordable, COVID-19 rapid diagnostic test for low- and moderate-income countries (Announced Sept 28) - A full access package includes WHO policy guidance on the use of antigen based RDT, manufacturer volume guarantees for low and middle-income countries, catalytic funding to assist governments to deploy the tests and an initial US$50 million procurement fund - The Global Fund commits an initial US$50 million to enable countries to purchase the new tests, with the first orders expected to be placed this week
Yemen – COVID-19 Activity Update COVAX : - A Pillar of the Access to COVID-19 Tools (ACT) Accelerator launched in early April by WHO, Euro Commission, and France to bring together key stakeholders to facilitate the expedited turnaround for access to COVID-19 diagnostics, treatments, and vaccines. - COVAX focus is on the making COVID-19 Vaccines readily available to low resources fragile states. - Recent talks with WB it was proposed that 12 billion will required to fund the COVID-19 vaccines among low income and fragile states, Yemen would be earmarked to receive a share yet to be determined to support it COVID-19 Vaccination campaign.
Yemen – COVID-19
Activity Update
Sero-Prevalence :
- South in high priority governates , pending issue remains the
delivery of reagents ( are planned to be flown into Aden from
Dubai ASAP. Approval from MoPHP to begin has been
granted.
- To measure the sero-prevalence of antibodies to COVID-19 in
the general population by sex and age group, in order to
ascertain the cumulative population immunity.
- To estimate the fraction of asymptomatic, pre-symptomatic or
subclinical infections in the population and by sex and age
group.
- To determine risk factors for infection by comparing the
exposures of infected and non-infected individuals
- To contribute to an improved understanding of antibody
kinetics following COVID-19 infection.
- Total sample size 2000 divvied in 4 districts according to
population size of each districtCOVID-19 Response Needs
Trust
- Rebuild of Public Trust in the Health Services
- Community Acceptance and Awareness of the Risks Posed by C-19
Train
- Develop, Maintain, and Improve Clinical and Technical Expertise
Test
- Extend Testing Capabilities, Capacities, and Targeted Reach
- Access to Data to Drive Response Program Delivery & Monitoring
Treat
- Case management with proven up to date methods based on Global Photo Retivied from: https://www.infomigrants.net/en/post/25129/coronavirus-in-yemen-a-country-on-
Experience and Technology the-brink
- Clinical Care for all C-19 symptomatic levels in addition to existing
medical conditions and emergencies
- Maintain access to specialities, medications, supplies and support
structures
11/21/2020 61Updates on HNO-HRP 2021
HNO 2021
• Cluster specific PIN and Severity • Joint Inter-Sectoral Analysis Framework
Analysis (JIAF)
• Proposed health indicators to • Scoping of the HNO:
➢Context
inform the severity,
➢Shock/ events
➢Impact on exposed population
➢Impact
➢Access Score
➢Risks
➢Health System Capacity:
• JIAf indicators , based on Global clusters
➢Morbidity
• Final List of indicators for all clusters (Below)
• Severity scale is changed 1-
5(instead 0-7)HC JIAF list of Indicators
SEVERITY SCALE Data Status
collection
frequency
Source None/Minimal Stress (2) Severe (3) Extreme (4) Catastrophic
(1) (5)
Coverage of DTC3
(DPT3 / PENTA3) in < 1 EPI data (VCE) >= 95% 90% - < 95% 85% - < 89% 80% - < 84% < = 80% Monthly Available
year old/")
Percentage of children
aged six months to 15
years who have EPI data (VCE) >= 95% 90% - < 95% 85% -< 89% 80% - < 84% < = 80% Monthly Available
received measles
vaccination")
Number of cases or
< 0.25% - >= < 0.75% - >= < 1.0 % - >=
incidence rates (attack eDEWS < = 0.25% >= 1.0% monthly Available
rate) for (cholera) 0.75% 0.50% 0.75 %
Number of health
workers per 10,000 HeRAMS Biannual Available
population ➢ 22 19 - < = 22 15 - < =19 11 - < =15 < = 11
Number of HF with
Basic Emergency
Obstetric Care/ HeRAMS Biannual Available
500,000 population, by
administrative unit")
➢5 4 3 2Updates on the 1st SA 2020
SA Strategy – 2 Priorities
• Priority 1 • Priority 2
• Hardest of the hard to reach (HTR) 2.1- underfunding protection
areas 34 districts programmes
• Based on access analysis 2.2- IDPs response
• Some districts observed remain as 2.3- Pre-Positioning of items for CP
inaccessible - The CCCM and Health Cluster priorities
• Sub-districts need also to be - Health need in districts with Vulnerability
score(4, 5) + IDPs, 33 district
considered
• OCHA approved for 4 districts in Taiz
(Maqbanah, Hayfan, As Selow, Al
Mukha) , as an integrated Response
with other clusters1st SA, 2020 - Health cluster
• P1 = 4 Districts ($3 million TBC) • P2 = 33 Districts ($9.6million TBC)
Total projects =12
Hospital Health centre Health Unit Mobile/ Outreach
Parameter 1 4 13 12 9
Parameter 2 18 37 29 32
Total 22 50 41 4168
List of Health Cluster Activities for 1st SA, 2020: • Provide Minimum Service Package (MSP) including; Basic and Emergency health services , child care & vaccination (Penta/DPT, measles & Polio), Mental Health Services, management of Communicable disease, early diagnosis & management non-communicable disease, through fixed HFs & outreach activities • Provide Minimal Initial Service Package for Reproductive Health through Basic Emergency obstetric care(BEmONC) & Comprehensive Emergency Obstetric Care(CEmONC) in the selected HFs • Support secondary health care provision in the selected supported hospitals • Capacity building of health care workers(Doctor, Nurses, Midwives) , community health workers, community health volunteers • Support IDPs & critical cases referral between health care level • Operationalization / continuation of health services through operational support( HCW payment support (Allowance/Top-Up), water, electricity, and IPC materials, medicines and supplies.
List of Health Cluster Indicators for 1st SA, 2020:
• - # of medical consultations (Out-patient/ communicable disease) for host community and IDPS separately
• -# of children under 18 mo. provided with measles vaccination
• -# of children under 1year provided with Penta/DPT vaccination
• -# health care workers (Doctors, Nurses, Midwife, Lab Tech, Pharmacist) receive top up
• -# of HFs supported with operational support (Water L/mo., fuel L/mo., Solar power support), IPC & waste
management support
• -# of HFs supported with medicines / medical supplies
• - # of women receive ANC ,post-natal care, tetanus vaccine
• - # of deliveries by skilled birth attendants
• -# of assisted delivery (with Caesarian /Section
• -# child Children < 5 Years with SAM & complication supported/referred
• -# of health workers receive training on MSP & other trainings.
• -# of referrals cases (Host community/IDPs)
• -# of people reached with health education sessions
• -# of outreach visitsAssessment tools used by Health Cluster to identify gaps:
In addition to HTR and IDPs sites priorities shared by OCHA and CCCM cluster, Health cluster priorities were
informed/guided by:
❑ Partners presence 4W - gap analysis 2020
❑ Health Cluster severity matrix September 2020,
❑ Current project status (projects that ended in March – October 2020)
❑ Cholera prioritization mapping 2020,
❑ HeRAMS 2019/ 2020 ,
❑ Utilization of health services analysis – impact of COVID-19
❑ Consultation with Sub-National cluster coordinators, partners and GHOs offices
❑ Gaps in health services to the IDPs- Health, Nutrition, WASH, CCCM and Protection cluster partners assessments and
reports
71Steps and timeline Once OCHA launched the SA call, all clusters sent full guidance to partners As usual, the SA is with very tight timeline – • Health Cluster has submitted the cluster priorities based on two priorities with funding estimated • Discussion and mapping with hubs is ongoing 3 -4 Nov • Updated partners 30 Oct & 4th Nov • Inter-Cluster matching done 4th Nov • SAG 5 Nov - OCHA • Submission of dossier on 5th November to YHF Advisory Board • Defense by Cluster 8 Nov and 9 Nov • Based on defense, selected projects notified , Proposals 12 – 27th Nov • Inter-cluster meeting discussing the opportunity of converging to maximize the effect on 16th Nov. • List of activities & indicators share by cluster by 16th Nov. • GSM open on Thursday 19th Nov.
Questions and comments?
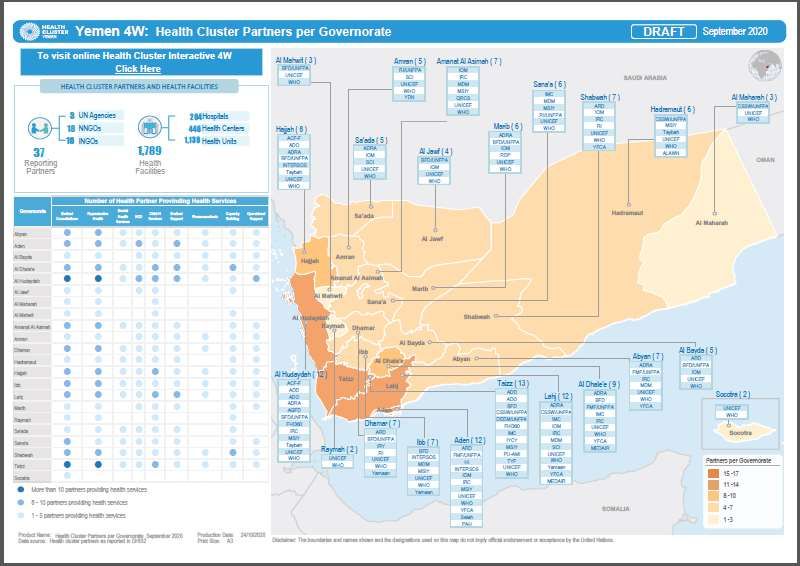
Partner Presence September
2020
Yemen Health Cluster
YEMEN45 Partners reporting status by Months
# of Partners % # of Partners % # of Partners % # of Partners % # of Partners % # of Partners %
Sr.No
(Apr20) (Apr20) (May20) (May20) (Jun20) (Jun20) (Jul20) (Jul20) (Aug20) (Aug20) (Sep20) (Sep20)
1 0 0% 1 2% 1 2% 1 2% 1 2% 0 0%
2 3 7% 3 7% 3 7% 1 2% 1 2% 1 2%
3 11 24% 5 11% 8 18% 7 16% 6 13% 7 16%
4 31 69% 36 80% 33 73% 36 80% 37 82% 37 82%
Legend
100% to 80%
79% to 65%
64% to 50%
Less than 50%Partners Reporting Status
Average of Reporting by Governorate
S Partner Type Status Sep-20 S Partner Type Status Sep-20
1 ACF INGO Active 100% 24 NFDHR NNGO Active 100%(Finished)
2 ADD INGO Active 100% 25 PAC INGO Active 50%
3 ADO NNGO Active 94% 26 PU-AMI INGO Active 96%
4 ADRA INGO Active 94% 27 QRCS INGO Active 92%
5 AGF NNGO Active 100% 28 RDP NNGO Active 100%
6 Alatta NNGO Active 80% 29 RI INGO Active 95%
7 BFD NNGO Active 86% 30 RRD NNGO Active 100%
8 CSSW NNGO Active 89% 31 SAWT NNGO Active 100%
9 DEEM NNGO Active 74% 32 SCI INGO Active 88%
10 FHI360 INGO Active 100% 33 SDF NNGO Active 80%(Finished)
11 FMF NNGO Active 90% 34 SHS NNGO Active 65%(Finished)
12 HA INGO Active 75%(Finished) 35 SOUL NNGO Active 100%
13 HAND NNGO Active 100%(Finished) 36 TFD NNGO Active 100%
14 HI INGO Active 78% 37 TYF NNGO Active 83%
15 IMC INGO Active 85% 38 UNFPA UN Active 85%
16 INTERSOS INGO Active 89% 39 UNICEF UN Active 85%
17 IOM UN Active 76% 40 VHI INGO Active 90%(Finished)
18 IR INGO Active 75% 41 WHO UN Active 100%
19 IRC INGO Active 100% 42 Yamaan NNGO Active 63%
20 IYCY NNGO Active 100% 43 YDN NNGO Active 100%
21 MdM INGO Active 100% 44 YFCA NNGO Active 88%
22 MMF NNGO Active 100%(Finished) 45 ZOA INGO Active 100%
23 MS INGO Active 96% Legend
100% to 80%
79% to 65%
64% to 50%
Less than 50%Services Utilization Jan to Sep 2020 (2019 vs 2020)
Services Utilization Jan to Sep 2020 (2019 vs 2020)
Services Utilization
2020 Vs 2019
Services Difference Services Difference
Medical Consultations -11% NCD -27%
Medical Support 17%
Reproductive Health 13%
Operational Support 59%
Mental Health Services -1%
Capacity Building -51%
Child Health Services -19%Working groups and Taskforce - Updates • Mental Health & Psychosocial Service Support (MHPSS) • WASH in Health Facilities • Nutrition Surveillance System –WHO
MHPSS Technical Working Group
Yemen
October - November 2020
UpdatesOctober-November 2020 Updates
▪ Increasing coordination capacity:
▪ MHPSS TWG coordinator will be travelling to Aden end of this week or beginning
of next week.
▪ UNICEF is considering the possibility to support the MHPSS TWG co-chair in
Sana’a.
▪ Establishment of National Mental Health Programme (NMHP) – Aden: An official
letter was shared regarding the establishment of national mental health
programme. The head of the NMHP was selected and appointed officially in Aden.
▪ Capacity Building: WHO is launching training on mHGAP and PFA to support MoPHP
which will start hopefully during the month of November 2020 in the southern
governorates. For the north it still pending the provision of training participants.
▪ Technical Capacity: WHO YCO is currently working to establish a small technical
group that sits under the TWG to support in addressing some of the gaps related to
the delivery of MHPSS services. Still in consultation phase.EPI/Vaccination Updates
General updates
• 16 governorates implemented the 1st round of Integrated outreach rounds & 7 completed the 2nd round. Third
round integrated outreach to start in governorates that have completed the second round to reach additional
children
• 41 high-risk district implemented MNTE campaign in October.
• Nationwide polio campaign to be conducted through Yemen except Sa’adah in response to the cVDPV1 outbreak
in Sa’adah. Another round will be conducted in Northern governorates with the 3rd in 3 governorates around Sa’adah
– Sa’adah will be conducting multiple fixed site strategy offering bOPV, MR, Diphtheria and all EPI
antigens along with IMCI, Nutrition and WASH interventions. This will be followed by two more
rounds in Sa’adah offering bOPV and routine EPI antigens
• Operational cost, vaccine and non vaccine supplies being arranged with some distributed while other in process
• PPEs (masks, sanitizers & gloves) arranged and being distributed as well all vaccinators and supervisors will be
trained on infection control (IPC) measures in th elight of COVID19 pandemic
• Polio campaign planned for 21 Nov, postponed by the MoPHP to unknown date with 1.3 Million doses already in
Aden and 5.1 million doses of polio vaccine arriving Sanaa on 17 Nov and other preparation ongoing
• Mid Level Management (MLM) : TOT training for central and governorates supervisors completed in Sana’a and
Aden. Training of district supervisors completed in Northern Governorates while it will start in Dec for Southern
governorates.Coverage comparison all antigens for Period Jan - Sep
2019 & 2020
85% 85% 84% 83%
79% 79% 79% 78% 2019 2020
75% 75% 75% 77%
71% 70%
68% 68% 68%
64% 66% 66%
62%
60%
48%
44%
BCG OPV1 OPV3 IPV Penta1 Penta3 PCV1 PCV3 Rota1 Rota2 MR1 MR2
Data of Sep 2020 only from 14 North governoratesCoverage by Months for Period Jan - Sep 2019 & 2020
BCG IPV
81,463 81,406
79,263
77,669
73,217 74,387
68,054
65,575 63,647 63,172 64,872
62,458 60,755 61,166 61,756
57,889 59,235 58,285 57,546 55,595
54,856 63,373 54,052
48,902 62,849
57,517 58,352 56,318 56,835 46,028
52,581 37,602 63,801 55,643
34,876
2019 2020 23,327 2019 2020
Jan Feb Mar Apr May Jun Jul Aug Sep Jan Feb Mar Apr May Jun Jul Aug Sep
Penta 3 MR1
81,406 81,406
74,387 77,692
73,217 71,461
68,054
63,172 64,872
62,849 65,054 62,185
61,166 61,756 59,821 61,369
57,546 55,595 54,713 57,070
54,052 53,772
63,373 50,556
48,885
56,318 56,835 46,028
54,719 41,215 61,140
55,643 58,625
34,876
28,167 29,735
2019 2020 2019 2020
Jan Feb Mar Apr May Jun Jul Aug Sep Jan Feb Mar Apr May Jun Jul Aug Sep
Data of Sep 2020 only from 14 North governoratesMonthly vaccinated children by Penta3 by Fixed activities Jan - Sep
2019 & 2020
52,976
52,171
52,073
51,300
60,000
49,071
51,083 47,860
47,462 45,790
46,398 43,105
52,822
50,000
52,333
48,923
37,035
48,792
45,152
40,000
30,000
27,924
20,000
10,000
-
Jan Feb Mar Apr May Jun Jul Aug Sep
2019 2020AOB • Data Sharing – MoPHP/Partners
THANK YOU Next Health Cluster meeting → 2nd December 2020
You can also read

















































