Obesity as an Independent Risk Factor for Cardiovascular Disease: A 26-year Follow-up of Participants in the Framingham Heart Study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Obesity as an Independent Risk Factor
for Cardiovascular Disease: A 26-year Follow-up
of Participants in the Framingham Heart Study
HELEN B. HUBERT, M. P. H., PH.D., MANNING FEINLEIB, M. D ., DR. P.H.,
PATRICIA M. MCNAMARA, AND WILLIAM P. CASTELLI, M.D.
SUMMARY The relationship between the degree of obesity and the incidence of cardiovascular disease
(CVD) was reexamined in the 5209 men and women of the original Framingham cohort. Recent observa-
tions of disease occurrence over 26 years indicate that obesity, measured by Metropolitan Relative Weight,
was a significant independent predictor of CVD, particularly among women. Multiple logistic regression
analyses showed that Metropolitan Relative Weight, or percentage of desirable weight, on initial examina-
tion predicted 26-year incidence of coronary disease (both angina and coronary disease other than angina),
coronary death and congestive heart failure in men independent of age, cholesterol, systolic blood pressure,
cigarettes, left ventricular hypertrophy and glucose intolerance. Relative weight in women was also posi-
tively and independently associated with coronary disease, stroke, congestive failure, and coronary and
CVD death. These data further show that weight gain after the young adult years conveyed an increased
risk of CVD in both sexes that could not be attributed either to the initial weight or the levels of the risk
factors that may have resulted from weight gain. Intervention in obesity, in addition to the well established
risk factors, appears to be an advisable goal in the primary prevention of CVD.
THE IMPORTANCE of body weight, body mass and surance Company desirable weight tables. 16 These
other measures of adiposity in the prediction of cardio- desirable weights, derived from the mortality experi-
vascular disease (CVD) has been the subject of long- ences of subscribers, have been revised upward be-
standing debate. Many studies have shown that the cause new data on insured lives'7 suggest that it is
incidence of certain types of CVD, particularly coro- healthier to be heavier than once thought. Recent anal-
nary heart disease and stroke, is greater in heavier yses of long-term mortality in Framingham indicate,
persons,'` but only a few suggest that any obesity however, that this may not be so; minimal mortality
index makes an additional contribution to risk once the occurs at previously published levels of desirable
levels of coexisting risk factors are taken into ac- weight.'8 Although recent statistics indicate that the
count. '. 2'4 Obesity is associated with elevated blood general U.S. population, particularly men, has been
pressure, blood lipids and blood glucose,7 1 and getting heavier over the last few decades, 19 20 consider-
changes in body weight are coincident with changes in ably more data are needed to evaluate the implications
these risk factors for disease.", 113 Thus, the consensus of this trend. Likewise, revisions to the desirable
has been that the increased risk among heavier persons weight tables seem premature, because the complex
is due primarily to the influence of the associated risk relationships between body weight and health or dis-
factor profile and not to the degree of obesity per se. ease are so poorly understood. This reappraisal of the
The existing data have also been interpreted to suggest impact of relative weight on cardiovascular morbidity
that obesity is benign when it exists without other in Framingham further emphasizes the need for cau-
major risk factors for CVD. tion, because health-related issues. other than total
In this report, we reexamine the obesity question mortality should be considered in arriving at accept-
and describe the influence of relative weight on the 26- able levels of desirable weight.
year incidence of CVD in Framingham men and wom- Methods
en. Earlier results from this study suggested that the
degree of obesity is not a potent independent risk factor The Framingham Heart Study population has been
for CVD in general, particularly among women. 14, 15 examined and followed biennially for the development
However, these conclusions were based on analyses of of CVD since 1948.21 In this report we present the
the influence of relative weight over shorter periods of morbidity experience of 2252 men and 2818 women,
follow-up and may not have conveyed the true impact ages 28-62 years, who were free of clinically recog-
of disease risk. nizable CVD at the first study examination, which took
Such a reevaluation appears timely in view of the place between 1949 and 1950. Manifestations of CVD
current revisions to the original Metropolitan Life In- included coronary heart disease, congestive heart fail-
ure, stroke and intermittent claudication.
From the Epidemiology and Biometry Program, National Heart, For the purposes of this report, the subjects were
Lung, and Blood Institute, Bethesda, Maryland, and the Framingham classified by weight and other risk attributes at the
Heart Study, Framingham, Massachusetts. initial examination only and observed over 26 years for
Presented in part at the 22nd Annual Conference on Cardiovascular the development of CVD. The obesity index chosen to
Disease Epidemiology, San Antonio, Texas, March 1982. characterize the population was Metropolitan Relative
Address for correspondence: Helen Hubert, Ph.D., NHLBI, Federal
Building, Room 300, Bethesda, Maryland 20205. Weight (MRW), or percentage of desirable weight (the
Received July 29, 1982; revision accepted December 20, 1982. ratio of actual weight to desirable weight x 100).
Circulation 67, No. 5, 1983. Desirable weight for each sex was derived from the
968
Downloaded from http://circ.ahajournals.org/ by guest on March 16, 2015OBESITY AND CARDIOVASCULAR DISEASE/Hubert et al. 969
1959 Metropolitan Life Insurance Company tables'6 by less than 1 hour) or nonsudden coronary death. Con-
taking the midpoint of the weight range for the medium gestive heart failure was indicated when at least two
build at a specified height. Since desirable weights major or one major and two minor diagnostic condi-
were reported for subjects wearing both clothes and tions existed concurrently upon examination.23 The
shoes, these figures were adjusted in order to apply major stroke end point of interest was atherothrom-
them to Framingham subjects, who were weighed botic brain infarction, defined as the sudden onset of a
and measured in a dressing gown and without shoes localizing neurologic deficit lasting over 24 hours
(table 1). without evidence of embolism or hemorrhage. Inter-
Other characteristics of interest at the initial ex- mittent claudication was diagnosed from subjective
amination were systolic blood pressure, measured in responses to questions on calf cramping during ex-
the left arm of the seated subjects with a mercury ertion.
sphygmomanometer and a 14-cm cuff long enough Preliminary analyses of the data consisted of calcu-
to fit the most obese arm; serum cholesterol concen- lating crude incidence rates of disease by level of
tration, determined by the method of Sperry;22 the MRW. More formal statistical methods used to assess
number of cigarettes smoked per day, assessed by a the influence of MRW independently of the coexisting
physician-administered medical history questionnaire; levels of the major cardiovascular risk factors relied
glucose intolerance, defined by a casual blood glucose upon multivariate logistic regression procedures24 in
level of at least 120 mg%, the presence of glycosuria or which the probability of an event was described as a
a definite history of diabetes; and left ventricular hy- function of several attributes measured at entry to the
pertrophy on a 13-lead ECG. Framingham Study. Regression coefficients generated
Criteria for each cardiovascular outcome during fol- by the logistic model measured the strength of the
low-up were standardized,23 and decisions regarding association between adiposity and the probability of
diagnosis were made by a panel of Framingham inves- disease after adjustment for age and the other risk
tigators. Coronary heart disease included diagnoses of factors. The coefficients divided by their standard er-
(1) angina pectoris, evidenced by a typical history of rors provided tests of significance to indicate whether
chest pain on a physician-administered questionnaire; these relationships were significantly different from
(2) myocardial infarction, determined by specified zero (p 0.05 when z ¢ 1.96). Standardized coeffi-
-
electrocardiographic changes, diagnostic elevation of cients that adjust for differences in measurement units
serum enzymes with prolonged ischemic chest pain, or between variables were also calculated to show the
autopsy; (3) coronary insufficiency, defined as pro- impact of weight relative to the other risk factors for
longed ischemic chest pain accompanied by transient disease.
ischemic abnormalities on the ECG; and (4) sudden (in
Results
TABLE 1. Adjusted Desirable Weightsfor the Framingham Heart During the 26-year follow-up, 870 men and 688
Study Participants
women developed clinically recognizable CVD. Al-
Height Weight (lb) though some subjects had more than one manifestation
(inches) Men Women of disease, coronary heart disease accounted for a large
55 94 proportion of the events, 75% and 66% in men and
56 97 women, respectively. Congestive failure occurred in
57 100
183 men and 165 women and atherothrombotic stroke
in 106 men and 103 women. Intermittent claudication
58 103 was diagnosed more often in males than in females
59 106 (171 vs 112).
60 116 109 At entry to the study, the disease-free Framingham
61 119 112 cohort appeared to be considerably overweight. On the
62 122 116 average, men were 18.9% and women 20.5% above
desirable weight. Although the distributions of initial
63 125 120 relative weights were very similar in men younger than
64 128 124 40 years, 40-49 years and 50 years or older, women
65 131 128 appeared to be heavier in each subsequent age group
66 135 132 (fig. 1). Clearly, a larger proportion of females than
67 140 136 males were at the upper end of the weight distribution,
68 144 140
particularly among the 50-62-year-olds.
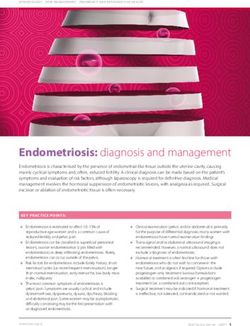
Figure 2 shows sex- and age-specific crude inci-
69 148 dence rates for total CVD over 26 years by MRW at
70 152 entry to the study. For this purpose only, relative
71 157 weight was categorized as less than 110, 110-129, and
72 161 130 or over; the middle category spanned evenly over
73 166 the mean weights for men and women. The risk of
CVD increased in both men and women with increas-
74 170 ing MRW. However, the association of weight to inci-
Downloaded from http://circ.ahajournals.org/ by guest on March 16, 2015970 CIRCULATION VOL 67, No 5, MAY 1983
MEN Similar relationships were evident between MRW
and coronary disease, the most frequent manifestation
of CVD (fig. 3). Incidence also increased with increas-
ing MRW, and the gradient of risk was steeper in the
U younger men and women. Among men younger than
z 50 years, the heaviest group experienced twice the risk
U11
of coronary disease compared with the leanest group.
LU
0- 10l The risk was increased 2.4-fold among obese women
of similar age. The relationships for risk of myocardial
infarction were similar to those for total coronary dis-
ease (fig. 4). However, there was a much stronger
gradient of risk for sudden death with increasing MRW
WOMEN
in each age group in both sexes (fig. 5). In fact, these
30 crude rates suggest that the impact of weight on risk
may be most pronounced for this outcome. Figure 6
shows that the 26-year incidence of congestive heart
failure in the younger men and women increased 2.5-
z to 3-fold from the leanest to the heaviest subjects.
LU
C) Unlike coronary disease, it appeared that the risk of
a: congestive failure in women was elevated only in the
LU
a- most obese group. MRW had a greater impact on the
incidence of atherothrombotic stroke in women than in
men (fig. 7). Women younger than 70 years who wereOBESITY AND CARDIOVASCULAR DISEASE/Hubert et al. 971
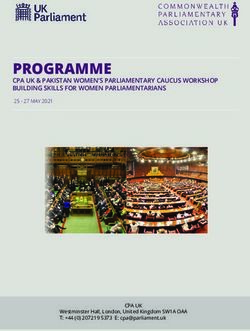
MEN WOMEN
500
400k
300F FIGURE 3. Twenty-six-year incidence of coro-
w nary heart disease by Metropolitan Relative
z
CX
w Weight at entry among Framingham men and
0
200k women younger than age 50 years and age 50
z years or older. N = the number at risk for an
event. Numbers above the bars give the actual
1001 incidence rates per 1000.
n972 CIRCULATION VOL 67, No 5, MAY 1983
MEN WOMEN
FIGURE 6. Twenty-six-year incidence of con-
gestive heart failure by Metropolitan Relative
w
C) Weight at entry among Framingham men and
z women younger than age 50 years and age 50
years or older. N = the number at risk for an
z event. Numbers above the bars give the actual
incidence rates per 1000.OBESITY AND CARDIOVASCULAR DISEASE/Hubert et al. 973
MEN WOMEN
l5Or974 CIRCULATION VOL 67, No 5, MAY 1983
MEN WOMEN infarction in Framingham men, subscapular skinfold
measurements were significantly and independently
300 r
associated with this outcome. Thus, it may be mislead-
267 ing to suggest that obesity in men did not play an
important role as a precursor to infarction.
250 Age differences in the contribution of obesity to risk
have also been noted by others. 1 4 Similarly, other risk
200
factors for disease do not predict as well at older ages
200 as at younger ages.4'28 Selection has been suggested as
an explanation for such findings. Here, the older,
LLI
heavier subjects may have been a selective group, be-
150 cause they remained resistant to the influence of obesi-
z
125 121
128 ty during earlier years. However, weights at older ages
0
may be less typical of the lifetime exposure to obesity,
105
z
100 which may be important in determining risk. If, as
suspected, age at onset and duration of obesity play a
part in explaining the observed associations with dis-
ease, then earlier measurements may more accurately
50
classify individuals into risk categories than those
made in later years. The fact that certain risk factors
L .
correlated more strongly with relative weight at youn-OBESITY AND CARDIOVASCULAR DISEASE/Hubert et al. 975
1.0 that obesity is associated with fibrinolytic activity and
plasma fibrinogen concentrations, which have been
implicated in the onset and course of ischemic heart
disease.3' Moreover, obesity appears to increase cardi-
We MRW ac work load and intravascular volume32 and to alter
t t6
- glucose and lipid metabolism.33 Increased cardiac
R 2110-129 work load in a heavier person may precipitate an acute
E .5 01030+
event or elicit symptoms if the coronary circulation is
already compromised. The burden of excess weight on
the heart also has been shown in autopsy studies in
which relative weight was independently related to
CL .9 heart size.34 35 Obesity has also been associated with
the extent of coronary atherosclerosis at autopsy.34
Despite the findings from clinical and experimental
studies, there is still much confusion over the complex
relationship between obesity and CVD risk. Most epi-
demiologic studies have been concerned with the im-
sE sWeu
Ot MoNl E D
pact of overweight on coronary heart disease in men.
These studies can be used to highlight some of the
difficulties in interpreting and comparing results. For
example, the Seven Countries Study showed no sig-
eatv e 7 i nificant association between body mass index in most
regions and coronary disease incidence over 10
years. However, many of the populations observed
thanR Thpa ralle ls t freviously frep re o f ina d i o fa
were considerably leaner than the Framingham cohort,
thar diseaenpatracfllowsup pexaiaiouslyreportedofinding Rel- whose weights compared favorably with those in the
general U.S. population.'9 The lack of sufficient het-
erogeneity in adiposity, and the different cultural and
changeribuin the presentistudy suggests ever,o genetic context in which this characteristic may have
die ausE
thWat meayge no moryeas
t be tri obu ed solelationthe
generall seansiie than womiieny
a suin operated, make comparability between these two stud-
ies difficult.
levels
toteeffects of weightah
of
eRi at beeits
beaue
entry chnutange, impactgon
to Different indexes of obesity can be differentially
cheFringhanm t The wigt
hnMRW at age 25 years,
preStudy hangwalsepsindicael
afbtpesditor oevef related to disease risk,37 which may explain some vari-
that ies was remost pnuncerae amongythe who stmena ability in study results. While body mass index (weight/
theffectsof weight class betweensthe its imepwert height2) has been suggested as the preferred measure of
tanuceiof ofeiy obesityronge incaidencehof CVD.e
adiposity, in Framingham it was very highly correlated
toetherdevlo te of theimajor risk factors
en orthough with MRW (r = 0.99) and had no greater predictive
mtah bolinc
term ofale' ws
prmedcin ph catudy
and r ests
mayebeoisl reoltedasndiaow prcror
bei e power. However, skinfold measurements of subcuta-
neous fat accumulation correlated with MRW to a less-
risk on
il Theae aditonal
ue the o pmea sobesiy
devlt
eatributiodo o wathe
to s cthya
orsrsloing- er degree (r = 0.40-0.65), and preliminary results
in the heaviest weight class between the two time peri- suggest that these measures were associated somewhat
ods. These findings lend further support to the impor- differently with disease risk in Framingham. Further-
tance of duration of obesity on incidence of CVD. more, if indexes of obesity are more powerful predic-
thyereso.EtyMWi contribution of obesity
The additional FraminghamStd reitoto thef long-
was a V tors of disease in younger than older persons, differ-
term prediction of CVD may be its role as a precursor
rindependenst prediuctor aofnhpethoension ovaerd2
nifiant
ences in the age distributions of study populations may
to the' development of the major risk factors or through also serve to explain what appear to be conflicting
metabolic and physiologic mechanlisms yet to be iden- results.
tified. It seems that the degree of obesity may, in fact, The length of follow-up for events in each popula-
influence the later development of risk factors such as tion can also affect the conclusions drawn from various
hypertension. Entry MRW in Frami'ngham was a sig- studies. Some effects of overweight may be evident
nificant independent predictor of hypertension over 26 only after follow-up over long periods of time, as sug-
years in women, but not in men. Excess weight in this gested by the importance of duration of obesity on
population ihay also have been associated with other disease. Both the Framingham and Manitoba studies'
lifestyle or behavioral characteristics which, over found obesity to be an independent predictor of disease
time, may have influenced CVD risk. While no data at on long-term observation only. Table 4 shows how
entry were available on physical activity, diet or per- observation over different periods of time may result in
sonality type, analyses that included an index of social different interpretations of the same data. In Fra-
class did not ap'pear to have any impact on the relation- mingham men, a strong and significant association
ships between weight and disease. between MRW and coronary disease incidence did not
Other direct effects of overweight may explain its emerge until the 8-year follow-up, at which point the
unique contribution to CVD risk. Recent data suggest strength of the relationship remained fairly constant for
Downloaded from http://circ.ahajournals.org/ by guest on March 16, 2015976 CIRCULATION VOL 67, No 5, MAY 1983
TABLE 4. The Association Between Metropolitan Relative Weight nese men living in Japan, Hawaii and California. Am J Cardiol 39:
at Entry and Coronary Heart Disease Incidence by Length of Fol- 244, 1977
low-up in Framingham Men and Women 3. Paul 0, Lepper MH, Phelan WH, Dupertuis GW, MacMillan A,
McKean H, Park H: A longitudinal study of coronary heart disease.
Multivariate logistic regression Circulation 28: 20, 1963
coefficients for MRW 4. Chapman JM,. Coulson AH, Clark VA, Borun ER: The differential
Length of effect of serum cholesterol, blood pressure and weight on the inci-
follow-up Men (n = 2197) Women (n = 2714) dence of myocardial infarction and angina pectoris. J Chronic Dis
6 years 0.006 (114) 0.011 (56) 23: 631, 1971
5. Petitti DB, Wingerd J, Pellegrin F, Ramcharan S: Risk of vascular
8 years 0.014* (154) 0.008 (78) disease in women. Smoking, oral contraceptives, noncontraceptive
14 years 0.012t (314) 0.008* (166) estrogens, and other factors. JAMA 242: 1150, 1979
20 years 0.012: (480) 0.007* (301) 6. Heyman A, Karp HR, Heyden S, Bartel A, Cassel JC, Tyroler HA,
Hames CG: Cerebrovascular disease in the biracial population of
26 years 0.012t (636) 0.008t (437) Evans County, Georgia. Arch Intern Med 128: 949, 1971
7. Chiang BN, Perlman LV, Epstein FH: Overweight and hyperten-
Regressions include adjustments for age, systolic blood pressure, sion. A review. Circulation 39: 403, 1969
serum cholesterol, cigarettes/day, glucose intolerance, and electro- 8. Kannel WB, Gordon T, Castelli WP: Obesity, lipids, and glucose
cardiographic left ventricular hypertrophy at exam 1. intolerance. The Framingham Study. Am J Clin Nutr 32: 1238,
The number of events at different follow-up times is given in 1979
parentheses. 9. Garrison RJ, Wilson PW, Castelli WP, Feinleib M, Kannel WB,
*Coefficient is significantly different from zero, p < 0.05. McNamara PM: Obesity and lipoprotein cholesterol in the Fra-
tCoefficient is significantly different from zero, p < 0.01. mingham Offspring Study. Metabolism 29: 1053, 1980
tCoefficient is significantly different from zero, p < 0.001. 10. Noppa H, Bengtsson C, Bjorntorp P, Smith U, Tibblin E: Over-
Abbreviations: MRW = Metropolitan Relative Weight; n - weight in women metabolic aspects. The population study of
number at risk. women in Goteborg 1968-1969. Acta Med Scand 203: 135, 1978
11. Leren P, Askevold EM, Foss OP, Froili A, Grymyr D, Helgeland
the duration of the study. Among women, the logistic A, Hjermann I, Holme 1, Lund-Larsen PG, Norum KR: The Oslo
Study. Cardiovascular disease in middle-aged and young Oslo
coefficients were fairly strong and consistent in all men. Acta Med Scand (suppl 588): 1977
observation periods. However, statistical significance 12. Noppa H: Body weight change in relation to incidence of ischemic
was not achieved until nearly 14 years of follow-up, heart disease and change in risk factors for ischemic heart disease.
for the small number of events in this group resulted Am J Epidemiol 111: 693, 1980
in insufficient power to test assumptions. Previous 13. Ashley FW, Kannel WB: Relation of weight change to changes in
atherogenic traits: the Framingham Study. J Chronic Dis 27: 103,
analyses, based on shorter periods of observation, 1974
have suggested that there is no independent relation- 14. Truett J, Cornfield J, Kannel W: A multivariate analysis of the risk
ship between MRW and coronary risk in Framing- of coronary heart disease in Framingham. J Chronic Dis 20: 51 1,
ham women.'4 These illustrations clearly show that 1967
the accumulated evidence describing the nature of 15. Kannel WB, Gordon T: Obesity and cardiovascular disease. The
Framingham Study. In Obesity Symposium. Proceedings of a Ser-
the weight-disease relationship should be interpreted vier Research Institute Symposium, edited by Burland WL, Sam-
cautiously. uel PD, Yudkin J. Edinburgh, Churchill-Livingstone, 1974, p 24
The issue of independence can be resolved only by 16. Metropolitan Life Insurance Company: New weight standards for
men and women. Stat Bull Metropol Life Insur Co 40: 1, 1959
further study, but we conclude from the existing data 17. Society of Actuaries and Association of Life Insurance Medical
that leanness and avoidance of weight gain before mid- Directors of America: Build Study 1979. Society of Actuaries,
dle age are advisable goals in the prevention of CVD 1980
for most American men and women. These data fur- 18. Garrison RJ, Feinleib M, Castelli WP, McNamara PM: Cigarette
ther-indicate that intervention on the well-established smoking as a confounder of the relationship between relative
weight and long-term mortality in the Framingham Heart Study.
risk factors for disease should be accompanied by JAMA. In press
weight loss in the overweight individual. Likewise, 19. United States DHEW: Vital and Health Statistics. Weight by
revisions to the actuarial desirable weight tables are Height and Age for Adults 18-74 Years. United States, 1971-74.
premature, because such changes suggest that mainte- National Center for Health Statistics, series 11, no. 208
nance of heavier weights will not diminish health stat- 20. United States DHEW: Advanced Data from Vital and Health Statis-
us. This assumption appears to be unsubstantiated by tics, no. 3, November 19, 1976
these as well as other data concerned with the impact of 21. Dawber TR, Meadors GF, Moore FE: Epidemiological approaches
obesity on morbidity and mortality.'2'4' 18 to heart disease: the Framingham Study. Am J Public Health 41:
279, 1951
Acknowledgments 22. Sperry WJ: A micromethod for the determination of total and free
cholesterol. Am J Clin Pathol (suppl 2): 91, 1938
The authors thank Felicia Carr and Doris Scherbak for their assistance
in preparing this manuscript. 23. Shurtleff D: Some characteristics related to the incidence of cardio-
vascular disease and death: Framingham Study, 18-year follow-up.
In The Framingham Study: An Epidemiological Investigation of
References Cardiovascular Disease, edited by Kannel WB, Gordon T. Wash-
1. Rabkin SW, Mathewson FA, Hsu PH: Relation of body weight to ington, DC, U.S. DHEW, 1974
development of ischemic heart disease in a cohort of young North 24. Walker SH, Duncan DB: Estimation of the probability of an event
American men after a 26 year observation period. The Manitoba as a function of several independent variables. Biometrika 54: 167,
Study. Am J Cardiol 39: 452, 1977 1967
2. Robertson TL, Kato H, Gordon T, Kagan A, Rhoads GG, Land 25. Fabsitz R, Feinleib M, Hrubec Z: Weight changes in adult twins.
CE, Worth RM, Belsky JL, Dock DS, Miyanishi M, Kawamoto S: Acta Genet Med Gemellol 29: 273, 1980
Epidemiologic studies of coronary heart disease and stroke in Japa- 26. Waldron I: Sex differences in longevity. In Second Conference on
Downloaded from http://circ.ahajournals.org/ by guest on March 16, 2015OBESITY AND CARDIOVASCULAR DISEASE/Hubert et al. 977
the Epidemiology of Aging, edited by Haynes SG, Feinleib M. Characteristics affecting fibrinolytic activity and plasma fibrinogen
Washington, DC, DHHS, 1980, p 163 concentrations. Br Med J 1: 152, 1979
27. Bengtsson C: Ischaemic heart disease in women: a study based on a 32. Alexander JK: Obesity and cardiac performance. Am J Cardiol 14:
randomized population sample of women and women with myocar- 860, 1964
dial infarction in Goteborg, Sweden. Acta Med Scand (suppl 549): 33. Gordon ES: Metabolic aspects of obesity. Adv Metab Disord 4:
1973 229, 1970
28. Kannel WB, Gordon T: Cardiovascular risk factors in the aged: the 34. Rhoads GG, Blackwelder WC, Stemmermann GN, Hayaski T,
Framingham Study. In Second Conference on the Epidemiology of Kagan A: Coronary risk factors and autopsy findings in Japanese-
Aging, edited by Haynes SG, Feinleib M. Washington, DC, American men. Lab Invest 38: 304, 1978
DHHS, 1980, p 65 35. Feinleib M, Kannel WB, Tedeschi CG, Landau TK, Garrison RJ:
29. Dyer AR, Stamler J, Berkson DM, Lindberg HA: Relationship of The relation of antemortem characteristics to cardiovascular find-
relative weight and body mass index to 14-year mortality in the ings at necropsy. Atherosclerosis 34: 145, 1979
Chicago Peoples Gas Company. J Chronic Dis 28: 109, 1975 36. Keys A: Seven Countries. A Multivariate Analysis of Death and
30. Garcia-Palmieri MR, Sorlie PD, Costas R, Havlik RJ: An apparent Coronary Heart Disease. Cambridge, MA, Harvard University
inverse relationship between serum cholesterol and cancer mortal- Press, 1980
ity in Puerto Rico. Am J Epidemiol 114: 29, 1981 37. Sanders K: Coronary-artery disease and obesity. Lancet 2: 432,
31. Meade TW, Chakrabarti R, Haines AP, North WRS, Stirling Y: 1959
Association Between Coronary Heart Disease
Risk Factors and Physical Fitness
in Healthy Adult Women
LARRY W. GIBBONS, M.D., M.P.H., STEVEN N. BLAIR, P.E.D.,
KENNETH H. COOPER, M. D., M.P. H., AND MIKE SMITH, M.S.
SUMMARY We examined associations between physical fitness and risk factors for coronary heart
disease in healthy women ages 18-65 years. Physical fitness was objectively determined by the duration of a
maximal treadmill exercise test. Six physical fitness categories (very poor to superior), specific within 10-
year age increments, were established. Mean risk factor levels varied across categories, but so did potential
confounders such as age and weight. Multiple linear regression modeling was used to control for the effects
of age, weight and year of exam on coronary risk factors. After adjustment, physical fitness was independ-
ently associated with triglycerides (p < 0.001), high-density lipoprotein cholesterol (HDL-C) (p 0.001), -
total cholesterol/HDL-C ratio (p S 0.001), blood pressure (p si 0.001) and cigarette smoking (p 0.001). -
IT IS WELL ESTABLISHED that men have a higher aware of any such studies in women. Although the
incidence of cardiovascular disease than women. precise role of physical activity in the prevention of
Nonetheless, coronary heart disease (CHD) is the lead- CHD is not known, a tenable hypothesis is that more
ing cause of death in women (259 deaths/100,000 per active persons have lower levels of established -risk
year), with women in the United States having high factors. We previously showed that men who were
rates compared with the rest of the world. ' These sta- more physically fit had lower levels of CHD risk than
tistics belie the relative paucity of research in CHD their less physically fit peers.6
epidemiology in women. Available data, notably from The purpose of this paper is to examine the associ-
the Framingham study, support the classic risk factor ation between physical fitness and CHD risk factors in
hypothesis for CHD in women. Women with higher women. We hypothesized that women with higher lev-
levels of blood cholesterol, high blood pressure, and els of physical fitness have a lower CHD risk.
who smoke cigarettes are more likely to develop CHD
than women without these risk factors.2 Other pre- Methods
sumed CHD risk factors have been less thoroughly More than 3900 adult women, ages 18-65 years,
studied in women. For example, several studies asso- were examined from 1971 to 1980. Some women re-
ciating sedentary living habits with the incidence of ceived only a treadmill test, but 2854 received a com-
CHD in men have been published,3-5 but we are un- plete physical examination, including CHD risk factor
measurements. Most of these women were self-re-
From the Cooper Clinic and Institute for Aerobics Research, Dallas, ferred for the purpose of physical fitness evaluation,
Texas, and the School of Public Health, University of South Carolina, periodic health examination or receiving preventive
Columbia, South Carolina. medical advice. These patients tended to be well edu-
Address for correspondence: Larry W. Gibbons, M.D., Cooper Clin- cated and from middle to upper socioeconomic strata.
ic, 12200 Preston Road, Dallas, Texas 75230.
Received July 6, 1982; revision accepted January 18, 1983. More than 99% of the women were white. Data report-
Circulation 67, No. 5, 1983. ed in this paper are from the first clinic visit for these
Downloaded from http://circ.ahajournals.org/ by guest on March 16, 2015Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of
participants in the Framingham Heart Study.
H B Hubert, M Feinleib, P M McNamara and W P Castelli
Circulation. 1983;67:968-977
doi: 10.1161/01.CIR.67.5.968
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1983 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on
the World Wide Web at:
http://circ.ahajournals.org/content/67/5/968
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally
published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the
Editorial Office. Once the online version of the published article for which permission is being requested is
located, click Request Permissions in the middle column of the Web page under Services. Further
information about this process is available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/
Downloaded from http://circ.ahajournals.org/ by guest on March 16, 2015You can also read