OCA Health Conference - 2019 Bev Unger, RN OCA Health Care Committee Camp Robin Hood
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

OCA Health Conference
2019
Bev Unger, RN
OCA Health Care Committee
Camp Robin Hood:
Director Health and Wellness
April 2019 Bev Unger, RN
• Occurrence
A brief overview • Triggers
• Risk Factors
Anaphylaxis • Signs and Symptoms of an Anaphylactic
Reaction
• considerations when administering
Treatment Epinephrine
Options • Administration options
• Identification of the individual with
anaphylaxis
Camp Protocols: • Establish relationship with family
• Anaphylactic Emergency Plan
Keeping Camps • Raising Awareness
Safe for Campers • Staff Training
• How to avoid exposure to an allergen
• Camp program considerations
April 2019 Bev Unger, RN
World Allergy Organization definition:
Anaphylaxis is an acute, potentially life-threatening hypersensitivity
reaction, involving the release of mediators from mast cells,
basophils and recruited inflammatory cells.
Anaphylaxis is defined by a number of signs and symptoms, alone or
in combination, which occur within minutes, or up to a few hours,
after exposure to a provoking agent.
It can be mild, moderate to severe, or severe. Most cases are mild
but any anaphylaxis has the potential to become life-threatening.
Anaphylaxis develops rapidly, usually reaching peak severity within
5 to 30 minutes, and may, rarely, last for several days. [1]
April 2019 Bev Unger, RN
"a serious allergic reaction that is rapid
in onset and might cause death.” [2]
April 2019 Bev Unger, RN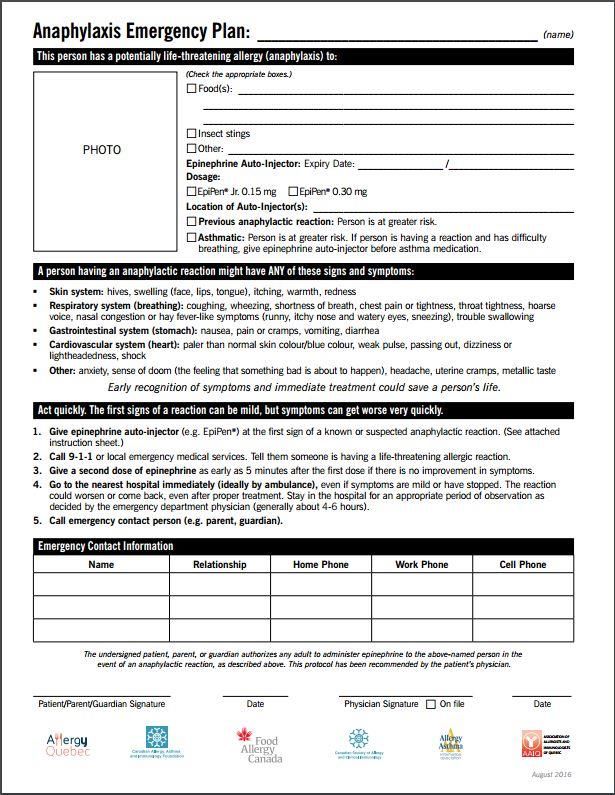
Global rate of occurrence from all triggers is unknown because of:
under-recognition by patients and caregivers…
under-diagnosis by healthcare professionals….
under-reporting….
Hospital admissions increasing…..
under 18 years more than doubled from 2000 - 2009……
more pronounced in aged 5–14 years [3]
2009-2010
estimated 8% of USA children have food allergy
2.4% have multiple food allergies
about 3% experience severe reactions [4]
April 2019 Bev Unger, RN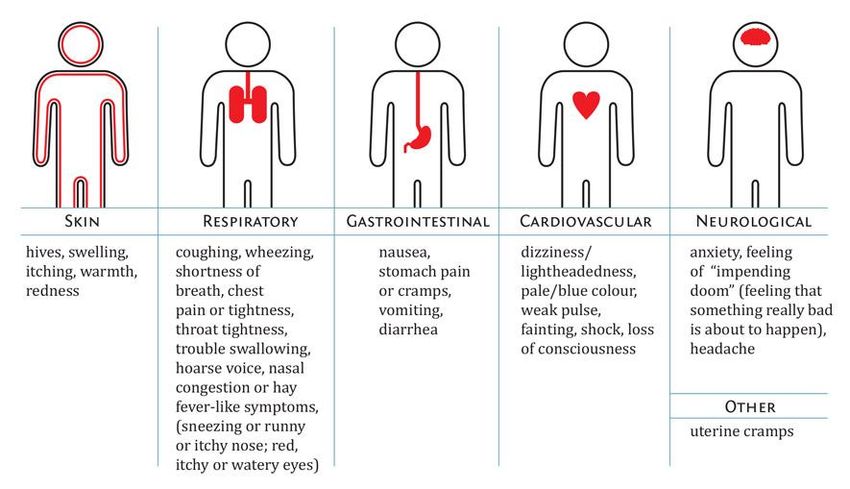
April 2019 Bev Unger, RN

Figure 1
April 2019 Bev Unger, RN
FOOD
STINGING INSECTS
NATURAL LATEX
MEDICATIONS
EXERCISE
UNKOWN CAUSES (idiopathic)
April 2019 Bev Unger, RN
Milk
Peanuts
Tree nuts Wheat
(Almonds, Brazil nuts,
cashew nuts, hazelnuts, Soy
macadamia nuts, pecans,
pine nuts, pistachios,
walnuts)
Sesame
Seafood
Fish Sulfites
Crustaceans (crab, (food additives)
crayfish, lobster, shrimp)
Shellfish
(clams,mussels,oysters,
scallops)
Mustard
not an inclusive list
Eggs More than 200 allergens
April 2019 Bev Unger, RN
Honey Bees
Bumble Bees
Yellow Jackets
Hornets
Wasps
Fire Ants
April 2019 Bev Unger, RN Surgical gloves Balloons
Dental supplies Carpet backing
Condoms Fidget toys
Erasers Sport Balls
Bandages Medical tubing / supplies
(i.e.: Band-Aid®)
April 2019 Bev Unger, RN Not Common
A combination of exercise and other
contributing factors such as food,
weather conditions, or medications can
cause exercise-induced anaphylaxis.
Itching, hives, swelling, nausea, tiredness
common – any anaphylactic S & S
April 2019 Bev Unger, RNTrigger is unknown
Hard to diagnose
Very frightening type of
anaphylaxis as unable to identify
allergy
April 2019 Bev Unger, RN• People with asthma and
anaphylaxis are more susceptible to
severe breathing problems during
Asthma an anaphylactic reaction
• Epinephrine can be used to treat
life-threatening asthma attacks.
Delay in use • Epinephrine must be given early
of • There are no contraindications to
Epinephrine using epinephrine for a life-
threatening allergic reaction
Auto injector
• Beta-blockers and ACE Inhibitors
Underlying (Angiotensin Converting Enzyme)
Cardiac may slow down the effect of
epinephrine and worsen allergic
Disease reaction
April 2019 Bev Unger, RNAsthma
a chronic inflammatory disease of the airway
Eczema
a skin condition that causes redness and itching
Eosinophilic Esophagitis (EoE)
a swallowing disorder that affects the esophagus
an allergic response that happens when eosinophils (a
type of white blood cell) collect in the esophagus
Food Protein-Induced Enterocolitis Syndrome (FPIES)
an inflammation involving both the small and large
intestine
Food Intolerance
different than food allergies, involves the digestive
system.
Oral Allergy Syndrome
an allergic reaction to certain proteins in fruit,
vegetables and nuts
April 2019 Bev Unger, RNSigns & Symptoms
of an
Anaphylactic Reaction
April 2019 Bev Unger, RNSymptoms of anaphylaxis generally include two or more of the following body systems:
Figure 2
April 2019 Bev Unger, RN Range from:
Mild – rash or hives – sometimes NO hives!
To severe - life threatening
- difficulty breathing and sudden drop in BP
The initial presentation can be delayed
S & S could develop rapidly - no way to tell how quickly a
reaction may progress
May develop some symptoms, but usually not all
There is no "typical” reaction
every reaction may be different
Effects many different body systems
April 2019 Bev Unger, RNSwelling of the airways
Difficultybreathing
a severe asthma attack for people who have asthma
A drop in blood pressure
causing dizziness, light-headedness, feeling faint
or weak, or passing out
Without immediate medical aid death can occur
April 2019 Bev Unger, RNThe first step
to control an anaphylactic
reaction is to administer
Epinephrine
ASAP!
April 2019 Bev Unger, RN Synthetic form of the hormone adrenaline
MUST be administered immediately!
Used for potentially life threatening allergies
Can be used for severe asthma attacks
Reversessymptoms of anaphylaxis by:
opening the airways
increasing blood pressure
accelerating heart rate
April 2019 Bev Unger, RNEpinephrine Auto Injector
EAI
EpiPen® The Right Dose Matters!
April 2019 Bev Unger, RN“Canadian Society of Allergy and Immunology (CSACI) has issued a new
Position Statement clarifying the need to treat all incidents of
anaphylaxis with an epinephrine auto-injector, stating that the risks of
using epinephrine for a child weighing under 15 kg are “expected to
be mild and transient” — but the consequences of not using an
epinephrine auto-injector “can include fatality.” [5]
The amount recommended by the CSACI is equivalent to an EpiPen Jr.
……0.15 mg/0.15mL (1mg/mL). [5]
April 2019 Bev Unger, RNAmpoules
• Inexpensive
• Skill set to prepare
and administer
April 2019 Bev Unger, RNIncorrect & Correct Technique
Figure 3 Figure 4
April 2019 Bev Unger, RNApril 2019 Bev Unger, RN
Who can administer the Auto Injector?
YOU !!!!!
Anindividual may NOT be able to self-
administer their epinephrine
You may need to do it for them!
BUT can you???
Ifyou have access to an EAI can you give it?
There are no contraindications!
Better safe than sorry???
April 2019 Bev Unger, RNAvoid Injuries
Holda squirmy child's leg to
avoid movement
HoldEpiPen for a few
seconds only!
Figure 5
Hold the injector firmly
April 2019 Bev Unger, RNProposed child restraint options
for the administration of an epinephrine auto-injector. [9]
Figure 6
April 2019 Bev Unger, RN Site – Intramuscular injection in the lateral thigh (vastus lateralis muscle)
Difficulty breathing: sit in an upright position
Sitting or standing may cause drop of BP
Feeling faint or dizzy: Place on back with legs raised above heart
level
If pale - lift the tail
Vomiting: Place on side
Call 911 after administration of Epi
April 2019 Bev Unger, RN Epinephrine is light sensitive
store at a temperature between 15-30° C
Ok outside in a bag / fanny pack at camp
Hang out of direct sunlight when not worn
Check solution window regularly
Ensure no brown discoloration or precipitate
Check the expiry date
Short shelf life – approx 12 months
Do not refrigerate
Tube is NOT waterproof
April 2019 Bev Unger, RN The need for a 2nd dose of epi cannot be predicted
Always have 2 or more auto injectors available
At least one must be carried by the individual
2nd (the spare) kept in an UNLOCKED location
2nd dose may be given as early as 5 minutes after the first dose
If symptoms are not improving or getting worse
Signs of a reaction getting worse may be increased breathing
difficulty, decreased level of consciousness, fainting
More than 2 doses should only be given under medical supervision
= consider this before sending campers on a trip!
April 2019 Bev Unger, RNAntihistamines
Benadryl or other antihistamines should
NOT be used as the first line of treatment
Antihistamines:
will not stop an anaphylactic reaction
can be used as secondary medication for hives and skin
reactions
April 2019 Bev Unger, RNApril 2019 Bev Unger, RN
Identification of the person who is anaphylactic
Establishing relationships with family
Anaphylactic Emergency Plan
Raising Awareness
Staff Training
How to avoid exposure to an allergen
• Food Policies / Kitchen / Meal Time
• Maintenance
Program Considerations
• Activity areas
• Swim and Waterfront
• Out Tripping and Off Site Excursions
April 2019 Bev Unger, RNIdentification of the allergic individual and the
allergy should be on the :
Camp Registration Form
The Camp Health Card / Form
Ana Poster
See Food Allergy Canada web site for sample posters
Identification of the Auto Injector:
Label the auto injector if there is no pharmacy label
Easily identifiable bag/ case/ fanny pack for camper
to carry auto injector
April 2019 Bev Unger, RNHealth Staff should speak with a guardian before
camper’s first day to discuss:
Camp Anaphylaxis Emergency Plan
Full medical history
Details of allergy and management
Documentation - is it complete?
Health form, emergency contact info, ana action plan
How the camper will carry their EAI at camp
Substitution of food if required for special events
April 2019 Bev Unger, RNA poster with clear
instructions on how to treat
symptoms and strategies to
reduce risks.
The plan should have a photo of
the individual
The action to be taken after an
EAI administration
Emergency contact information
*See Food Allergy Canada Web site for a
sample form
April 2019 Bev Unger, RNCommunicate with your camp community
(all families, all staff, bus drivers )
and inform them of anaphylactic allergies
Ask all families to:
read labels before sending food to day camp
Avoid sending food to overnight camp
Have campers wash hands and mouth before & after eating
Talk to campers about not sharing food
April 2019 Bev Unger, RN Everyone
counsellors, kitchen, bus drivers, life guards, program specialists, senior staff
Identify who has the anaphylactic allergies
What the allergy is
Precautions for avoiding exposure
S & S of an anaphylactic reaction
How to initiate the camps emergency plan
Location of EAI – easily accessible!
campers should carry their own!
camps supply
When, how and who is to administer an EAI
When to deliver a second dose of epinephrine
What to do after an EAI is given
The unknown allergic reaction – action plan
April 2019 Bev Unger, RNFood policies should include:
allergy “aware” or “safe” – NOT “free”
no food from home (overnight camps)
eat only food from own home (day)
no sharing of food policies!
read labels
know ingredients and alternate names
connect with food suppliers for lists of ingredients – share
with parents so they can substitute where necessary
April 2019 Bev Unger, RNKitchen
Avoid cross-contamination during food prep AND serving
Use allocated utensils
knowledge of food and ingredients:
Alternate names for ingredients
Is it a nut or a seed?
designated sponges and cloths
clean all surfaces well with proper cleanser
April 2019 Bev Unger, RNMeal and Snack Time
Staff should have knowledge of food ingredients / names
Know the campers and their allergies
Meal and snack time supervision = active observation
No “peanut free tables” – eliminate nuts!
peanut is extremely potent and often hidden
“schools with peanut-free tables, compared with those
without, had lower rates of reactions: 2 versus 6 per 100,000
student” [4]
Watch for insects flying into open juice boxes and onto straws
Hand washing is a must - before and after eating!
hand sanitizer is not substitute
April 2019 Bev Unger, RNMaintenance
Removal of hives or nests = immediate!
Keep lids on garbage cans to avoid insects
Weed and grass control to decrease bees
Good hand washing done by all
Clean with appropriate cleansers
April 2019 Bev Unger, RNActivity Areas
beaware of food and other products used
i.e.: eggs, pine cones, marshmallows (fish
gelatin in kosher marshmallow), bird seed
often contains nuts etc…
wash all surfaces well – dish soap is not
effective
substitiute food related prizes or rewards
April 2019 Bev Unger, RNSwim and Waterfront
Make sure the “fanny pack” is
hung or held in a secure location
central
easy access to everyone
Keep the auto-injector
Dry
If wet – discard!
Out of direct sunlight
Pickup of the “fanny pack” at the end of
the period
April 2019 Bev Unger, RNOut Tripping and Off Site Excursions
Who administers the auto injector?
Anyone who is trained
Individual themselves – IF able!
Must know where auto-injectors are stored
Must carry back ups / spare auto injectors
A second dose may be necessary
Safe Storage
Separate auto injectors into 2 different areas
if one is lost still have one
To keep from overheating:
pack in middle of packs
bottom of canoe so cooled by water
Access to doctor or health staff by phone
After administration – immediate EMS!
April 2019 Bev Unger, RNRemember……
Epinephrine is the first-line medication for anaphylaxis.
Antihistamines and asthma meds can be used after epinephrine, if needed
A second dose of epinephrine may be given as early as 5 minutes after the first
dose if symptoms do not improve or become worse.
Call 911 as soon as an allergic reaction is expected
Persons feeling faint or dizzy should lie down
Always go to to hospital is necessary (ideally by ambulance)
Phone emergency contact!
April 2019 Bev Unger, RNKeeping Camps Safe for
Campers With Anaphylaxis
Have up to date allergic protocols
Display ana posters in appropriate areas
Staff can identify the S & S
Those who are anaphylactic carry their own EAI
Makesure the right people know how to administer
the EAI
These steps May SAFE A LIFE!
April 2019 Bev Unger, RNOn line training module and certificates:
Allergyaware www.allergyaware.ca
EpiPen® www.epipen101.ca
World Allergy www.worldallergy.org/anaphylaxis/
EpiPen® www.epipen.ca and www.epipen.com
Food Allergy Canada (formerly Anaphylaxis Canada)
www.foodallergycanada.ca
www.allergysafecommunities.ca
www.safe4kids.ca
A site for teens / youth www.whyriskit.ca
Food Allergy Research and Education (FARE) foodallergy.org
Allergy Safe Communities allergysafecommunities.ca
Allergy/Asthma Information Association (AAIA) www.aaia.ca
Sabrina’s Law Regulation 137/15 (anaphylaxis) and Ryans Law (asthma)
www.edu.gov.on.ca/eng/healthyschools/anaphylaxis.html
Health Canada www.hc-sc.gc.ca/
Prescribing Information EpiPen® Mylan, January 12, 2017 www.pfizer.ca/pm/en/EPIPEN.pdf
Asthma and Allergy Foundation of America
www.aafa.org/page/anaphylaxis-in-america.aspx April 2019 Bev Unger, RNAnaphylaxis in Schools & Other Settings, 3rd Edition
available from www.foodallergycanada.ca
On line:
http://foodallergycanada.ca/wp-content/uploads/Anaphylaxis-in-Schools-
Other-Settings-3rd-Edition-Revised_a.pdf
AAIA Anaphylaxis Reference Kit Allergy/Asthma Information Association
Available on line:
http://www.aaia.ca/en/anaphylaxis_reference_final.pdf
April 2019 Bev Unger, RN1. Lockey, Richard F. “Anaphylaxis: Synopsis.” WAO, Sept. 2012,
www.worldallergy.org/professional/allergic_diseases_center/anaphylaxis/anaphylaxissynopsis.php.
2. Simons, F Estelle R, et al. “World Allergy Organization Guidelines for the Assessment and Management of Anaphylaxis.” World
Allergy Organization Journal, BioMed Central Ltd, 23 Feb. 2011, www.waojournal.org/content/4/2/13.
3. Simons, F. Estelle R., et al. “2015 Update of the Evidence Base: World Allergy Organization Anaphylaxis Guidelines.” World
Allergy Organization Journal, BioMed Central, 28 Oct. 2015, waojournal.biomedcentral.com/articles/10.1186/s40413-015-0080-
1.
4. Sampson, Hugh A. “Food Allergy: A Review and Update on Epidemiology, Pathogenesis, Diagnosis, Prevention, and
Management.” Journal of Allergy and Clinical Immunology, vol. 141, no. 1, Jan. 2018, pp. 41–58.,
doi:https://doi.org/10.1016/j.jaci.2017.11.003.
5. “Epinephrine for Infants and Toddlers: New CSACI Position Statement.” Food Allergy Canada, 19 Dec. 2015,
foodallergycanada.ca/2015/12/epinephrine-for-infants-and-toddlers-canadian-allergists-position-statement/.
6. Anaphylaxis in Schools and Other Settings. 3rd ed., Canadian Society of Allergy and Immunology, December 2005, Revised
third printing: August 2016
7. AAIA Anaphylaxis Reference Kit . Allergy/Asthma Information Association, 2004 – Revised June 2007 and October 2014
8. “Food Allergens.” Food Allergy Canada, foodallergycanada.ca/about-allergies/food-allergens/
9. Posner, Larry S, and Carlos A Camargo. “Update on the Usage and Safety of Epinephrine Auto-Injectors, 2017 Usage and Safety
of Epinephrine Auto-Injectors, 2017.” Drug, Healthcare and Patient Safety, Dove Medical Press, 21 Mar. 2017,
www.ncbi.nlm.nih.gov/pmc/articles/PMC5367766/
April 2019 Bev Unger, RN Figure 1:Allergic Reactions - https://goo.gl/images/FZDhfW
Figure 2: https://foodallergycanada.ca/food-allergy-basics/preventing-and-treating-allergic-reactions/reaction-
signs-and-symptoms/
Figure 3: shutterstock.com, Oswald, Kirsty. “All Schools Can Now Purchase Emergency Adrenaline Auto-Injectors
without Prescription.” The Pharmaceutical Journal, 2 Oct. 2017, doi:10.1211/pj.2017.20203662.
Figure 4:Medscape,
https://img.medscape.com/thumbnail_library/am_151013_epipen_epinephrine_800x600.jpg
Figure 5: American College of Emergency Physicians. "EpiPens save lives but can cut like a knife." ScienceDaily.
ScienceDaily, 8 October 2015. www.sciencedaily.com/releases/2015/10/151008142408.htm
Figure 6: Proposed child restraint options for the administration of an epinephrine auto-injector.
Note: Reprinted from The Journal of Allergy and Clinical Immunology: In Practice, Volume 4/edition 3,
Brown JC, Tuuri RE, Lacerations and embedded needles due to EpiPen use in children, Pages 549–551
April 2019 Bev Unger, RNYou can also read

















































