ORIGINAL ARTICLE DEEP BRAIN STIMULATION IN THE BED NUCLEUS OF STRIA TERMINALIS IN OBSESSIVE-COMPULSIVE DISORDER-1-YEAR FOLLOW-UP - DIVA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Original Article
Deep Brain Stimulation in the Bed Nucleus of Stria Terminalis in Obsessive-Compulsive
Disorder—1-Year Follow-up
Matilda Naesström1, Marwan Hariz2,3, Lotta Strömsten1, Owe Bodlund1, Patric Blomstedt2
- BACKGROUND: Deep brain stimulation (DBS) is under Surgical adverse events included 1 case of skin infection
investigation as a treatment for therapy-refractory obses- leading to reimplantation. The most common transient
sive-compulsive disorder (OCD). As a crucial part of the stimulation-related side effects were anxiety and
anxiety circuit, the bed nucleus of stria terminalis (BNST) insomnia.
has been proposed as a target for DBS in OCD. Here, we - CONCLUSIONS: BNST DBS is a promising therapy in
investigate clinical outcomes and safety of DBS in the
severe therapy-refractory OCD. Our results are in line with
BNST in a series of 11 participants with severe therapy-
previous publications regarding effect and safety profile.
refractory OCD.
Nevertheless, DBS for OCD remains an investigational
- METHODS: Eleven consecutive participants diagnosed therapy and should therefore be performed in multidisci-
with refractory OCD were treated with BNST DBS and plinary clinical studies.
completed follow-up. The primary outcome was a change
in scores of the Yale Brown Obsessive Compulsive Scale
(YBOCS) at 1 year after surgery. Secondary outcomes
included changes in scores of the Montgomery-Åsberg
INTRODUCTION
Depression Rating Scale (MADRS) and the Global
Assessment of Functioning.
- RESULTS: At baseline, the mean SD YBOCS score
was 33 3.0, MADRS score was 29 4.5, and GAF score
O bsessive-compulsive disorder (OCD), characterized by
anxiety-driven intrusive thoughts (obsessions) that lead
to repetitive behaviors or rituals (compulsions), is an
often chronic condition with a prevalence of around 2%.1 It has
was 49 5.4. One year after DBS, mean SD YBOCS been suggested that up to 25% of OCD patients will present
score was 20 4.8 (38% improvement (range 10%L60%) with severe symptoms that do not respond to established
P < 0.01), MADRS score was 21 5.8 (27% improvement, pharmacologic or psychotherapeutic therapies.2 Hence other
treatment methods such as deep brain stimulation (DBS) are
range 4%L74%, P < 0.01), and Global Assessment of
being investigated for therapy-refractory OCD.3
Functioning score was 55 6.5 (12% improvement, range DBS is an established treatment for Parkinson disease and other
4%L29%, P < 0.05). Of the 11 participants, 6 were movement disorders and was first introduced for OCD in 1999 by
considered responders (decrease in YBOCS ‡35%) and 4 Nuttin et al.4 In the literature, so far there are data from around
partial responders (decrease in YBOCS 25%L34%). 300 OCD DBS cases implanted in 10 different brain targets.4-12
Key words
- Bed nucleus of stria terminalis SD: Standard deviation
- Deep brain stimulation YBOCS: Yale Brown Obsessive-Compulsive Scale
- Obsessive-compulsive disorder
From the 1Department of Clinical Sciences/Psychiatry and 2Unit of Deep Brain Stimulation,
Abbreviations and Acronyms
Department Clinical Sciences/Neuroscience, Umeå University, Sweden; and 3Unit of
BNST: Bed nucleus of stria terminalis Functional Neurosurgery, UCL Institute of Neurology, Queen Square, London, United Kingdom
CBT: Cognitive behavioral therapy
DBS: Deep brain stimulation To whom correspondence should be addressed: Matilda Naesström, M.D.
[E-mail: matilda.naesstrom@umu.se]
GAF: Global assessment of functioning
IC: Internal capsule Citation: World Neurosurg. (2021).
MADRS: Montgomery-Åsberg Depression Rating Scale https://doi.org/10.1016/j.wneu.2021.01.097
MRI: Magnetic resonance imaging Journal homepage: www.journals.elsevier.com/world-neurosurgery
NA: Nucleus accumbens Available online: www.sciencedirect.com
OCD: Obsessive-compulsive disorder
1878-8750/ª 2021 The Authors. Published by Elsevier Inc. This is an open access article under
the CC BY license (http://creativecommons.org/licenses/by/4.0/).
WORLD NEUROSURGERY -: e1-e9, - 2021 www.journals.elsevier.com/world-neurosurgery e1ORIGINAL ARTICLE
MATILDA NAESSTRÖM ET AL. DBS IN THE BNST FOR OCD
Hence the number of patients implanted in each of these brain signs of depression with a mean SD Montgomery-Asberg-
areas is by necessity limited. From an anatomic point of view, Depression Rating Scale (MADRS) score of 29 4.5 (range 22e
there are no clear borders between some of the targets and overlap 37), indicating moderate depression. Other comorbidities included
is common, especially when taking into consideration the field of Asperger syndrome, atypical autism, attention-deficit-
stimulation. Indeed, several brain targets, such as the nucleus hyperactivity-disorder, and bipolar disorder type II (see Table 1).
accumbens, the most ventral anterior internal capsule, and the All participants had, at the time of inclusion, at least 1
inferior thalamic peduncle, cluster around the bed nucleus of stria serotonergic acting antidepressant, 73% had augmentation with a
terminalis (BNST), suggested by Nuttin et al13 as a target for OCD neuroleptic, and 55% had the addition of an anxiolytic agent (see
in 2013. To date, the number of patients with BNST DBS reported Table 1). All patients had undergone regimens of cognitive
in the literature is limited to 32 patients.7,14,15 behavioral therapy (CBT) except 1 patient who could not fulfill a
The purpose of this pilot study was to further investigate the full CBT trial due to intolerable anxiety that led to suicide
effect and safety of DBS in the BNST in patients with refractory attempts after exposure trials.
OCD.
Inclusion and Exclusion Criteria
MATERIALS AND METHODS Inclusion criteria were severe OCD according to the Diagnostic
and Statistical Manual of Mental Disorders: DSM-IV, with a
Participants YBOCS score of at least 25/40,16,17 and disease duration of 5 years
In total, 29 referrals to the study were screened between 2010 and with persistent disabling symptoms despite adequate trials with at
2017 by a multidisciplinary team including psychiatrists and neu- least 3 different serotonergic acting antidepressants,
rosurgeons. Of these 29 referrals, 12 participants met the inclusion augmentation with antipsychotics, and CBT. Only patients
criteria and agreed to participate in the study. One participant was between 18 and 65 years of age who could understand and
excluded for not being able to attend the 12-month evaluation due to comply with instructions and provide their own written consent
a gastrointestinal disorder preventing any travels. The remaining were considered for inclusion.
11 participants consisted of 7 females and 4 males, with a Participants were excluded in case of current psychotic or
mean standard deviation (SD) age of 17 14 years at onset of OCD substance abuse disorder, clinically significant medical disorder,
and 38 14 years at surgery (Table 1). The mean Yale-Brown or previous brain surgery. Before inclusion, participants under-
Obsessive-Compulsive Scale (YBOCS) score was 33 3.0 (range went magnetic resonance imaging (MRI) to rule out any structural
29e38), indicating extreme OCD, and the most common type brain pathology. The study was approved by the Ethical
of OCD was contamination/cleaning. All participants had clinical Committee of Umea University and written informed consent was
Table 1. Participants’ Demographic and Clinical Characteristics
Participant Age at Years of Illness Age at Supportive Medication at Time for
Number Sex Onset OCD Before Surgery Surgery Type of OCD Comorbidity Inclusion
1 M 35 5 40 Religious, repetition ADHD Lithium, aripiprazole, risperidone, clomipramine,
methylfenidate, alimemazine, prometazine
2 F 28 31 59 Contamination, cleaning Quetiapine, aripiprazole, clomipramine,
mianserine, hydroxizine, alimemazine, zopiclone
3 F 7 46 53 Checking, repetition Sertraline, alprazolam, zopiclone
4 M 50 9 59 Contamination, cleaning Citalopram
5 F 15 11 27 Contamination, cleaning, Atypical Quetiapine, paroxetine, Oxazepam, zopiclone
symmetry autism
6 M 15 9 27 Contamination, cleaning Asperger Quetiapine, pregabaline, tranylcypromine,
syndrome methylfenidate, zopiclone
7 F 5 16 21 Contamination, cleaning ADHD Escitalopram, methylfenidate
8 F 15 7 22 Repetitions Anorexia Aripipraziole, amitryptiline, fluoxetin,
nervosa alimemazine
9 F 10 17 27 Contamination, cleaning, Atypical Olanzapine, sertraline, mirtazapine,
aggression autism alimemazine, prometazine, zopiclone
10 M 7 31 38 Sexual, aggression Citalopram, olanzapine, zopiclone
11 F 9 36 45 Sexual, aggression Bipolar Chlorprothixene, quetiapine, lithium, zopiclone,
type II propriomazine, phenelzine
OCD, obsessive-compulsive disorder; M, male; ADHD, attention deficit hyperactivity disorder; F, female.
e2 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2021.01.097ORIGINAL ARTICLE
MATILDA NAESSTRÖM ET AL. DBS IN THE BNST FOR OCD
obtained from participants according to the Declaration of
Helsinki.
Surgical Procedure
Bilateral BNST implantations were performed in general anes-
thesia using the Leksell frame model G (Elekta Instruments,
Linköping, Sweden). The navigation software FrameLink (Med-
tronic, Minneapolis, Minnesota, USA) was used for calculations of
target coordinates and trajectories.
The BNST was visually identified on thin-slice axial stereotactic
T2-weighted 1.5 Tesla MRI scans posterior to the anterior
commissure and lateral to the fornix at the anterior
commissureposterior commissure plane. An entry point was
chosen, typically 35e50 mm lateral to the midline and about 0e15
mm anterior to the coronal suture, to provide a trajectory intu-
bating the ventral part of the anterior internal capsule (IC). The
final target point for the deepest contact of the lead was chosen 3
mm below the anterior commissureposterior commissure plane
along this trajectory.18 The electrodes (model 3387 with 1.5-mm
interspace, Medtronic, Minneapolis, USA) were connected to an
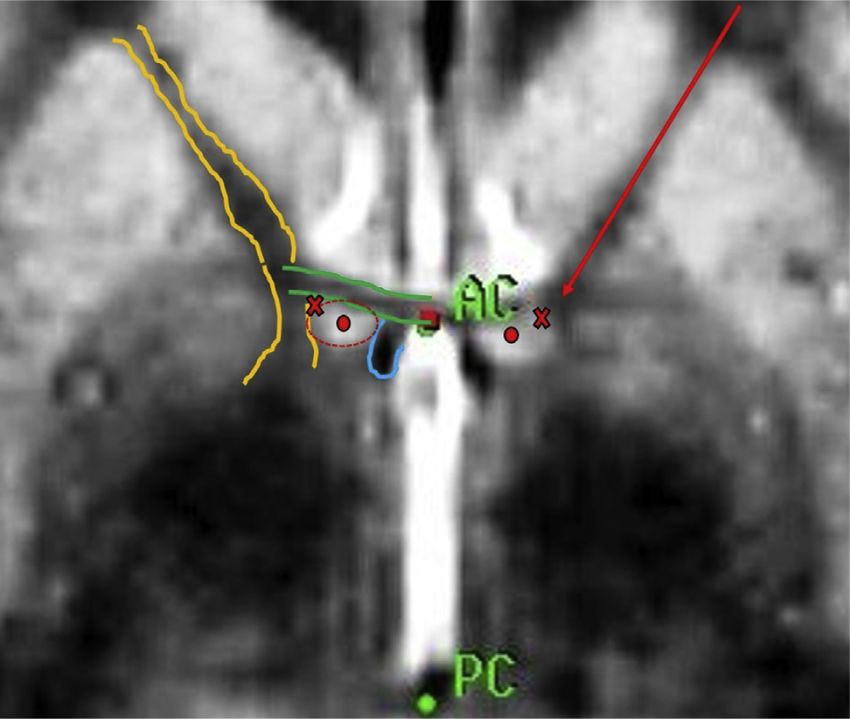
Figure 1. Magnetic resonance imaging proton density sequence of the
implantable pulse generator in the subclavicular area during the target area at the level of the anterior commissureposterior commissure.
same session. No macrostimulation or microelectrode recordings Note: The relevant structures, as seen in this axial image, are delineated:
were used during the procedure. internal capsule (anterior aspect) between the yellow lines; anterior
commissure between green lines; fornix within the blue line; bed nucleus
A postoperative computed tomography scan was performed and of stria terminalis shown by red dot. The second deepest contact will be
fused with the preoperative stereotactic MRI to verify the lead placed at this level at the red cross. The deepest contact will be placed 3
location (Figure 1). mm below this level, here represented by the red dot. The electrode is
implanted at such an angle that the higher contacts are intubating the
internal capsule (red arrow). A detailed description of the local anatomy
Programming and Follow-up and targeting process is available at the Stereotactic Academy, with
Stimulation was typically started 12 (range 3e30) days after sur- downloadable operation plans for 5 patients.18 AC, anterior commissure;
PC, posterior commissure.
gery. The initial programming session started with a screening of
each individual electrode, mainly for side effects. During the
following 3e6 months, the typically monopolar stimulation was
further titrated in voltage to obtain clinical reduction in obses- Lopez Pina et al,19 they reported a mean reliability of 0.886 for
sions, compulsions, and anxiety. During the programming Cronbach alpha, which corresponds to a satisfactory reliability.
sessions, patients were instructed to notify any adverse effects or Secondary outcome measures included the MADRS and global
any positive changes in anxiety or mood at each session. In case of assessment of functioning (GAF) scores.20,21 The MADRS is a 10-
side effects the programming was reverted to lower voltage set- item clinically rated scale of common symptoms in major
tings and the titration was done more gradually. Follow-up by a depressive disorder. The scale measures severity of depressive
psychiatrist using rating scales was performed at 6 and 12 months symptoms with a maximum score of 60 in which 0e6 indicates
after surgery. Patients were instructed not to make any changes in normal levels, 7e19 mild, 20e34 moderate, and >34 severe
medication nor participate in CBT during the first year after depression.20 A Cronbach alpha of 0.87 has been reported in
surgery. an adult outpatient clinical sample, indicating satisfactory
reliability.
Evaluation Tools In addition, participants were regularly seen by the involved
Established rating scales with adequate psychometric properties psychiatrists, neurosurgeon, and psychiatry nurse, who docu-
were used to assess obsessive-, compulsive-, depressive symptoms mented patients’ subjective reporting of perceived effects and
and daily functioning. The primary outcome measure was the adverse effects of the treatment.
psychiatrist-rated YBOCS at 1 year, with response defined as 35%
decrease in YBOCS score and partial response as a 25%34% Statistical Analyses
decrease.7,9,14,16,17 In YBOCS is a 10-item clinically rated scale For the statistical analyses, SPSS version 26 was used. Due to the
where the items are divided by obsessions and compulsions. The small sample size, normal distribution could not be established.
scale measures the severity of OCD by time spent on obsessions/ Therefore all parametric tests were cross-checked using equivalent
compulsions, level of anxiety, and decrease of functioning caused nonparametric tests yielding similar results. Statistical signifi-
by OCD symptoms and ability to control obsessions and com- cance was defined as P < 0.05.
pulsions. Maximum points on the scale are 40, where 0e7 points Descriptive statistics were given as means and standard devia-
indicate subclinical, 8e15 mild, 16e23 moderate, 24e32 severe, tion. Differences among YBOCS, MADRS, and GAF scores at
and 33e40 extreme OCD symptoms.16,17 In a meta-analysis by baseline and 12 months were investigated with the paired samples
WORLD NEUROSURGERY -: e1-e9, - 2021 www.journals.elsevier.com/world-neurosurgery e3ORIGINAL ARTICLE
MATILDA NAESSTRÖM ET AL. DBS IN THE BNST FOR OCD
t-test. This method was used in order to test the hypothesis if Secondary Outcomes
there was a difference in OCD and depressive symptoms and The mean SD MADRS score was reduced from 29 4.5 (range
function after the treatment. Effect size was calculated using 22e37) at baseline to 21 5.8 (range 9e32) 12 months after
Cohen’s d where 0.2 was interpreted as negligible, >0.2 up to surgery (t[8] ¼ 4.08, P ¼ 0.002, d ¼ 6.65) with a large effect size.
0.5 as small, >0.5 up to 0.8 as medium, and >0.8 a large effect The average reduction of depressive symptoms was 27% (range
size.22 4%74%). At the 12-month follow-up, 1 of 11 participants was in
To investigate correlations between percent of changes in remission from depressive symptoms (defined as MADRS 12).
YBOCS score with age at onset of OCD, years of illness, and age at These results are illustrated in Table 2 and as a box plot in
surgery, the Spearman rho test was used. Differences between Figure 2.
responders (defined as YBOCS change 35%) and partial/non- The mean SD GAF score increased from 49 5.4 (range 41e
responders were assessed by independent samples t-tests. 58) at baseline to 55 6.5 (range 42e65) 12 months after surgery
GAF data were missing preoperatively for participant no. 8 and (t[8] ¼ 2.75, P ¼ 0.03, d ¼ 6.18) with a large effect size.
postoperatively for participant no. 6. There were 2 outliers in the
data: postoperative MADRS scores in participants no. 1 and 6.
Stimulation Parameters
Therefore the data was cross-tested with nonparametric tests.
At 1 year follow-up, mean stimulation parameters were 4.2 0.5
Volt, 87 28 usec, and 130 0 Hertz (Table 3). The patients had
had an average of 8 programming sessions (range 3e12) during
RESULTS the previous 12 months. None of the participant required an
implantable pulse generator replacement during the first year.
Primary Outcome
The mean SD YBOCS score was reduced from 33 3.0 (range 29e
38) at baseline to 20 4.8 (range 14e27) 12 months after surgery (t Adverse Events
[8] ¼ 8, P < 0.001, d ¼ 5.24) with a large effect size. These results are Surgery-related adverse events included 1 infection after a bicycle
presented in Table 2 and illustrated in a box plot in Figure 2. At the accident necessitating explantation and later reimplantation of the
12-month follow-up, 6 of the 11 participants were defined as re- DBS system (participant no. 10).
sponders, 4 of the 11 as partial responders, and 1 of the 11 as non- The most common stimulation-induced side effect was anxiety
responders. Two of the participants were in remission (defined as and insomnia during the initial programming sessions. Minor
YBOCS score 7). The mean reduction of YBOCS was 38% (range transient hypomania, which resolved with decrease in stimulation
10%60%) for the whole group and among responders 49% (range parameters, was noted in 2 patients. There were 14 events of
36%60%). There were no correlations between percentage of impulsive medication intoxications in 1 patient that started 7
YBOCS improvement and age at onset of OCD (r[8] ¼ 0.176, P ¼ months after surgery. Table 4 shows all adverse events classified
0.60, ns.), years of illness (r[8] ¼ 0.357, P ¼ 0.28, ns.) or age at into surgically, stimulation related, probably stimulation related,
surgery (r[8] ¼ 0.169 P ¼ 0.62, ns.). and probably not stimulation related.
Table 2. Results of Evaluation Scales at Baseline and 12 Months After Surgery
YBOCS Reduction
Participant YBOCS 12 Reduction YBOCS MADRS MADRS MADRS
Number Before Months 12 Months Before 12 Months 12 Months
1* 30 14 53% 34 9 74%
2* 32 14 56% 28 19 32%
3* 35 14 60% 31 18 42%
4 29 26 10% 32 21 34%
5* 38 20 47% 30 27 10%
6y 35 23 34% 37 32 14%
7y 32 24 25% 26 23 12%
8* 29 17 41% 22 17 23%
9y 36 27 25% 29 22 24%
10* 33 21 36% 23 22 4,3%
11y 31 21 32% 31 23 26%
YBOCS, Yale Brown Obsessive Compulsive Scale; MADRS, Montgomery-Åsberg Depression Rating Scale.
*Responder with a 35% decrease in YBOCS at 12 months.
yPartial responder with a 25%34% decrease in YBOCS at 12 months.
e4 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2021.01.097ORIGINAL ARTICLE
MATILDA NAESSTRÖM ET AL. DBS IN THE BNST FOR OCD
Figure 2. Yale Brown Obsessive Compulsive Scale (YBOCS) and deep brain stimulation. Note: Changes in YBOCS (P < 0.001) and MADRS
Montgomery-Åsberg Depression Rating Scale (MADRS) before and after (P < 0.02) scores between baseline and 12 months after surgery.
DISCUSSION placed in the classical target for capsulotomies, in an anterior
location in the anterior arm of the IC. Due to modest results
Role of Bed Nucleus of Stria Terminalis Deep Brain Stimulation in and high energy consumption, Nuttin et al4,9 and other groups
Surgical Treatment of Obsessive-Compulsive Disorder started to implant DBS leads in more posterior and deeper parts
Multiple brain targets for DBS in OCD are currently being inves- of the anterior IC toward the BNST. Others targeted the ventral
tigated by various groups, and it is at this point not possible to caudate and the nucleus accumbens (NA), hence the common
decide which one, if any, might be the most optimal target with denomination of these target in several studies as ventral
respect to the safety and efficiency of the procedure (Table 5).3,26 capsule/ventral striatum (VC/VS).27,28 Some have stated that the
Several of these brain targets are anatomically closely located. best effect of DBS was achieved by stimulating more dorsal
When Nuttin et al4 introduced DBS for OCD, the leads were contacts in the ventral IC.29,30 The dorsal-most electrode
Table 3. Details of Deep Brain Stimulation Parameters at 12 Months’ Follow-up
Left Right
Contacts Contacts
Participant Frequency Pulse Width
Number IPG (Hz) (msec) 0 1 2 3 Volt 0 1 2 3 Volt
1 Activa PC 130 90 — — 3.2 — — 3.2
2 Activa PC 130 60 — 3.5 — 3.5
3 Activa PC 130 120 — — 5 — — 5
4 Activa PC 130 150 — — 4.2 — — 4.2
5 Activa PC 130 90 — — 4.1 — — 4.1
6 Activa PC 130 60 — — — 4 — — — 4
7 Activa PC 130 90 — — 4.9 — — 4.9
8 Activa PC 130 60 — — 3.8 — — 3.8
9 Activa PC 130 60 — — 4.4 — — 4.4
10 Activa PC 130 90 — — 4.3 — — 4.3
11 Activa PC 130 90 — — 3.5 — — 3.5
IPG, XXX; PC, posterior commissure.
WORLD NEUROSURGERY -: e1-e9, - 2021 www.journals.elsevier.com/world-neurosurgery e5ORIGINAL ARTICLE
MATILDA NAESSTRÖM ET AL. DBS IN THE BNST FOR OCD
activated, these will be located outside the nucleus, inside the
Table 4. Adverse Events During Study Period most ventral and posterior part of the anterior limb of the internal
Surgery-Related Adverse Events Number of Participants capsule.
It would be of value to know which areas are actually being
Surgical Lack of hair regrowth at scalp 1 stimulated in these studies, in order to have a better under-
incision site 1 standing of where to place the electrodes. Further, since the ef-
Transient postoperative fects with all probability do not stem from a single point, but from
headache circuits, similar effects can probably be achieved by stimulation at
Infection Skin infection after bicycle 1 different points within these networks.10,38
accident with reimplantation Since it is well known from DBS in movement disorders that
Transient stimulation-induced adverse different targets can be used for the same condition, and since this
events seems to be the case also in OCD, perhaps a more pressing issue
is why DBS for OCD—regardless of target—seems to have so
Psychiatric Anxiety 6
Insomnia 4 variable results among patients. The selection criteria of patients
Fatigue 2 cannot be refined until clinical factors or biological markers for
Hypomania 2 responders versus nonresponders can be discriminated. Therefore
Nightmares 1 further studies with larger patient samples are essential to gain
Adverse events, probably stimulation
much needed knowledge on possible predictive factors for
induced successful response to DBS in OCD.
Weight gain 2
Effect on Obsessive-Compulsive Disorder Symptoms
Adverse events, probably not stimulation The results from this study demonstrated positive results of BNST
induced stimulation in severe and treatment-resistant OCD in the majority
Medical intoxication (all in the same patient) 14 of our patients. After 1 year of DBS, the patients’ OCD improved
on average from extreme to moderate severity. In 4 out of 6
In total, there were 33 adverse events in 11 patients. responders, the severity of their illness receded from extreme to
mild. There was also a reduction in associated depressive symp-
toms and an improved functioning.
contacts would, however, end up in a more posterior location The mean YBOCS reduction of 38% and response rate of 55% is
within the IC, and it seems as if these contacts, rather than those consistent with prior reports on BNST DBS with 27.3%63%
in the NA itself were used for the stimulation.25,31 Posterior to the YBOCS reduction and 40%67% response rate7,9,14,15,36 and
BNST, Jimenez-Ponce et al32 had previously reported good results similar to studies of DBS in other closely related brain targets
of DBS in the inferior thalamic peduncle, and the Toronto group (see Table 5).3,26
has recently modified the inferior thalamic peduncle target, Similar to other studies, we observed a large variability of
moving it 2 mm more anterior, hence close to the BNST.33 improvement of OCD symptoms, with some patients having a
The BNST target, which was first introduced for DBS in OCD by great benefit (60% YBOCS reduction) and some less (10%). The
Nuttin et al13 in 2013, is part of an anxiety and threat monitoring reasons for this variability of response to DBS remain largely un-
network, which is believed to play an important role in anxiety- known. Finding predictive factors for DBS response to aid
related disorders, such as OCD.34,35 The nucleus is located appropriate screening of potential candidates is a crucial issue. In
posterior to the anterior commissure and lateral to the fornix a meta-analysis of treatment outcome for DBS in OCD in 116
and receives major input from the amygdala, where it serves as patients, Alonso et al39 found a positive correlation between older
an important processing center for limbic information, threat age of onset and response to the treatment. This was not verified
monitoring, and anxiety regulation.34 by the to-date largest OCD study on BNST DBS by Raymaekers
To date, the outcome of BNST DBS has been reported in 32 pa- et al.36 Similarly, in our study, correlation between improvement
tients. Islam et al14 reported a better outcome for DBS in the BNST and age of onset, age at surgery, or duration of illness could not
when comparing this with DBS in the NA in 8 patients. However, be confirmed. However, our patient population is too limited to
Farrand et al15 stated that the overall effect between these 2 allow meaningful correlation tests.
targets was similar. More recently, a larger study of 24 patients
reported a better result of DBS in the BNST compared with Adverse Effects
patients implanted in the anterior limb of IC.7 The same group Overall DBS was well tolerated in our study. The majority of
has also demonstrated that the symptom reduction was stable adverse effects related to the stimulation were transient or
over time.36 Acute positive effects on obsessions have also been resolved with adjustment of stimulation parameters. Many of the
reported with BNST stimulation in a study of 3 patients who were targets used for OCD DBS are in close proximity of each other and
stimulated with low-voltage stimulation the day after surgery.37 have similar side effects (see Table 5). One commonly described is
When discussing the results of BNST DBS, it is important to hypomania, which is by now a recognized adverse effect of
keep in mind that the effect is not necessarily achieved from stimulation of BNST and other psychiatric DBS
stimulating the nucleus itself. Typically, large fields of stimulation targets.6,8,9,15,24,36,40-43 This was also observed in our study in 2
are used and when the higher contacts of the electrode are patients. However, the episodes were mild and transient with
e6 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2021.01.097ORIGINAL ARTICLE
MATILDA NAESSTRÖM ET AL. DBS IN THE BNST FOR OCD
Table 5. Overview of Deep Brain Stimulation Obsessive-Compulsive Disorder Studies With 10 Participants in Chronologic Order
Outcome and Length of Response Mean YBOCS Stimulation-Related, Mostly Transient
Author Patients Target Follow-up Rate Reduction Adverse Events
Greenberg et al., 10 VC/VS 4 responders and 2 partial 40% 36% Transient hypomanic symptoms, anxiety, recurring
200623 responders at 3-year follow-up brief memory experiences (flashbacks)
Mallet et al., 20088 16 STN 6/8 responders* in active 75% 32% Transient hypomania, anxiety, dyskinesia with
stimulation group and 3/8 in the impulsivity, facial asymmetry, dysarthria, dysphagia
sham-stimulation group at 3 and walking difficulties
months’ follow-up
Greenberg et al., 26 VC/VS 16 responders and 3 partial 62% 39% Transient increased depression/suicidal ideation,
20109 responders at 3-year follow-up hypomania, recurring brief memory experiences
(flashbacks)
Huff et al., 201024 10 NA 1 responder and 5 partial 10% 21% Transient hypomania, anxiety, agitation,
responders at 12 months’ follow- concentration/memory difficulties, suicidal
up ideation, headaches, reduced sleep duration,
weight gainORIGINAL ARTICLE
MATILDA NAESSTRÖM ET AL. DBS IN THE BNST FOR OCD
as appropriate screening of potential candidates and clinical pre- Marwan Hariz: Data curation, Writing - review & editing. Lotta
dictors of outcome. Strömsten: Formal analysis, Data curation, Writing - review &
editing. Owe Bodlund: Methodology, Funding acquisition, Data
CRediT AUTHORSHIP CONTRIBUTION STATEMENT curation, Writing - review & editing. Patric Blomstedt: Concep-
Matilda Naesström: Funding acquisition, Formal analysis, Data tualization, Methodology, Data curation, Writing - review &
curation, Writing - original draft, Writing - review & editing. editing.
print]. Mol Psychiatry. https://doi.org/10.1038/ 24. Huff W, Lenartz D, Schormann M, et al.
REFERENCES s41380-019-0562-6, accessed October 29, 2019. Unilateral deep brain stimulation of the nucleus
accumbens in patients with treatment-resistant
1. Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The
12. van den Munckhof P, Bosch DA, Mantione MH, obsessive-compulsive disorder: outcomes after
epidemiology of obsessive-compulsive disorder in
et al. Active stimulation site of nucleus accumbens one year. Clin Neurol Neurosurg. 2010;112:137-143.
the National Comorbidity Survey Replication. Mol
deep brain stimulation in obsessive-compulsive
Psychiatry. 2010;15:53-63.
disorder is localized in the ventral internal 25. Denys D, Graat I, Mocking R, et al. Efficacy of
capsule. Acta Neurochir Suppl. 2013;117:53-59. deep brain stimulation of the ventral anterior limb
2. Bjorgvinsson T, Hart J, Heffelfinger S. Obsessive-
of the internal capsule for refractory obsessive-
compulsive disorder: update on assessment and 13. Nuttin B, Gielen F, van Kuyck K, et al. Targeting compulsive disorder: a clinical cohort of 70
treatment. J Psychiatr Pract. 2007;13:362-372. bed nucleus of the stria terminalis for severe patients. Am J Psychiatry. 2020;177:265-271.
obsessive-compulsive disorder: more unexpected
3. Naesstrom M, Blomstedt P, Bodlund O. lead placement in obsessive-compulsive disorder
A systematic review of psychiatric indications for 26. Tyagi H, Apergis-Schoute AM, Akram H, et al.
than in surgery for movement disorders. World A randomized trial directly comparing ventral
deep brain stimulation, with focus on major Neurosurg. 2013;80:S30. e11-16.
depressive and obsessive-compulsive disorder. capsule and anteromedial subthalamic nucleus
Nord J Psychiatry. 2016;70:483-491. stimulation in obsessive-compulsive disorder:
14. Islam L, Franzini A, Messina G, et al. Deep brain
clinical and imaging evidence for dissociable
stimulation of the nucleus accumbens and bed
4. Nuttin B, Cosyns P, Demeulemeester H, et al. effects. Biol Psychiatry. 2019;85:726-734.
nucleus of stria terminalis for obsessive-
Electrical stimulation in anterior limbs of internal compulsive disorder: a case series. World
capsules in patients with obsessive-compulsive 27. Fayad SM, Guzick AG, Reid AM, et al. Six-nine year
Neurosurg. 2015;83:657-663.
disorder. Lancet. 1999;354:1526. follow-up of deep brain stimulation for obsessive-
15. Farrand S, Evans AH, Mangelsdorf S, et al. Deep compulsive disorder. PLoS One. 2016;11:e0167875.
5. Martinho FP, Duarte GS, Couto FSD. Efficacy, brain stimulation for severe treatment-resistant
effect on mood symptoms, and safety of deep obsessive-compulsive disorder: an open-label 28. Sturm V, Lenartz D, Koulousakis A, et al. The
brain stimulation in refractory obsessive- case series. Aust N Z J Psychiatry. 2018;52:699-708. nucleus accumbens: a target for deep brain
compulsive disorder: a systematic review and stimulation in obsessive-compulsive- and anxiety-
meta-analysis. J Clin Psychiatry. 2020;81:19r12821. 16. Goodman WK, Price LH, Rasmussen SA, et al. disorders. J Chem Neuroanat. 2003;26:293-299.
The Yale-Brown Obsessive Compulsive Scale. I.
6. Denys D, Mantione M, Figee M, et al. Deep brain Development, use, and reliability. Arch Gen 29. Blomstedt P, Sjoberg RL, Hansson M, et al. Deep
stimulation of the nucleus accumbens for Psychiatry. 1989;46:1006-1011. brain stimulation in the treatment of obsessive-
treatment-refractory obsessive-compulsive disor- compulsive disorder. World Neurosurg. 2013;80:
der. Arch Gen Psychiatry. 2010;67:1061-1068. 17. Goodman WK, Price LH, Rasmussen SA, et al. e245-e253.
The Yale-Brown Obsessive Compulsive Scale. II.
7. Luyten L, Hendrickx S, Raymaekers S, et al. Validity. Arch Gen Psychiatry. 1989;46:1012-1016. 30. Liebrand LC, Natarajan SJ, Caan MWA, et al.
Electrical stimulation in the bed nucleus of the Distance to white matter trajectories is associated
stria terminalis alleviates severe obsessive- 18. Targeting the IC-area and the BNST. Available at: with treatment response to internal capsule deep
compulsive disorder. Mol Psychiatry. 2016;21: www.stereotactic.org; 2014. Accessed February 26, brain stimulation in treatment-refractory
1272-1280. 2020. depression. Neuroimage Clin. 2020;28:102363.
19. Lopez-Pina JA, Sanchez-Meca J, Lopez-Lopez JA, 31. Liebrand LC, Caan MWA, Schuurman PR, et al.
8. Mallet L, Polosan M, Jaafari N, et al. Subthalamic
et al. The Yale-Brown Obsessive Compulsive Individual white matter bundle trajectories are
nucleus stimulation in severe obsessive-
Scale: a reliability generalization meta-analysis. associated with deep brain stimulation response
compulsive disorder. N Engl J Med. 2008;359:
Assessment. 2015;22:619-628. in obsessive-compulsive disorder. Brain Stimul.
2121-2134.
2019;12:353-360.
20. Montgomery SA, Asberg M. A new depression
9. Greenberg BD, Gabriels LA, Malone DA Jr, et al. scale designed to be sensitive to change. Br J
Deep brain stimulation of the ventral internal 32. Jimenez-Ponce F, Velasco-Campos F, Castro-
Psychiatry. 1979;134:382-389.
capsule/ventral striatum for obsessive-compulsive Farfan G, et al. Preliminary study in patients with
disorder: worldwide experience. Mol Psychiatry. 21. Endicott J, Spitzer RL, Fleiss JL, Cohen J. The obsessive-compulsive disorder treated with
2010;15:64-79. global assessment scale. A procedure for electrical stimulation in the inferior thalamic
measuring overall severity of psychiatric distur- peduncle. Neurosurgery. 2009;65(suppl 6):203-209.
10. Huys D, Kohl S, Baldermann JC, et al. Open-label bance. Arch Gen Psychiatry. 1976;33:766-771.
trial of anterior limb of internal capsule-nucleus 33. Lee DJ, Dallapiazza RF, De Vloo P, et al. Inferior
accumbens deep brain stimulation for obsessive- 22. Cohen J. Statistical power analysis for the behavioral thalamic peduncle deep brain stimulation for
compulsive disorder: insights gained. J Neurol sciences. Mahwah, NJ: Lawrence Erlbaum Associ- treatment-refractory obsessive-compulsive disorder:
Neurosurg Psychiatry. 2019;90:805-812. ates; 1988:400. a phase 1 pilot trial. Brain Stimul. 2019;12:344-352.
11. Menchon JM, Real E, Alonso P, et al. A prospective 23. Greenberg BD, Malone DA, Friehs GM, et al. 34. Lebow MA, Chen A. Overshadowed by the
international multi-center study on safety and Three-year outcomes in deep brain stimulation for amygdala: the bed nucleus of the stria terminalis
efficacy of deep brain stimulation for resistant highly resistant obsessive-compulsive disorder. emerges as key to psychiatric disorders. Mol
obsessive-compulsive disorder [e-pub ahead of Neuropsychopharmacology. 2006;31:2384-2393. Psychiatry. 2016;21:450-463.
e8 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, https://doi.org/10.1016/j.wneu.2021.01.097ORIGINAL ARTICLE
MATILDA NAESSTRÖM ET AL. DBS IN THE BNST FOR OCD
35. Cano M, Alonso P, Martinez-Zalacain I, et al. meta-analysis of treatment outcome and predictors staggered-onset design. Biol Psychiatry. 2010;67:
Altered functional connectivity of the subthalamus of response. PLoS One. 2015;10:e0133591. 535-542.
and the bed nucleus of the stria terminalis in
obsessive-compulsive disorder. Psychol Med. 2018; 40. Bewernick BH, Hurlemann R, Matusch A, et al. Conflict of interest statement: Matilda Naesström has been
48:919-928. Nucleus accumbens deep brain stimulation sponsored for travel expenses and attendance at a DBS
decreases ratings of depression and anxiety in course by Medtronic Ltd. Patric Blomstedt is a consultant for
36. Raymaekers S, Vansteelandt K, Luyten L, et al. treatment-resistant depression. Biol Psychiatry. Abbott, Boston Scientific, and Medtronic and a shareholder
Long-term electrical stimulation of bed nucleus of 2010;67:110-116. in Mithridaticum AB. Marwan Hariz has received honoraria
stria terminalis for obsessive-compulsive disorder.
Mol Psychiatry. 2017;22:931-934. and travel expenses from Boston Scientific for speaking at
41. Tsai HC, Chang CH, Pan JI, et al. Pilot study meetings. Owe Bodlund and Lotta Strömsten have no
of deep brain stimulation in refractory disclosures or conflicts of interest.
37. Winter L, Heitland I, Saryyeva A, et al. Acute ef-
obsessive-compulsive disorder ethnic Chinese
fects of electrical stimulation of the bed nucleus of Received 7 December 2020; accepted 21 January 2021
patients. Psychiatry Clin Neurosci. 2012;66:
the stria terminalis/internal capsule in obsessive-
303-312. Citation: World Neurosurg. (2021).
compulsive disorder. World Neurosurg. 2018;111:
e471-e477. https://doi.org/10.1016/j.wneu.2021.01.097
42. Chang CH, Chen SY, Hsiao YL, et al. Hypomania
Journal homepage: www.journals.elsevier.com/world-
38. Baldermann JC, Melzer C, Zapf A, et al. Connec- with hypersexuality following bilateral anterior
limb stimulation in obsessive-compulsive disor- neurosurgery
tivity profile predictive of effective deep brain
stimulation in obsessive-compulsive disorder. Biol der. J Neurosurg. 2010;112:1299-1300. Available online: www.sciencedirect.com
Psychiatry. 2019;85:735-743. 1878-8750/ª 2021 The Authors. Published by Elsevier Inc.
43. Goodman WK, Foote KD, Greenberg BD, et al. This is an open access article under the CC BY license
39. Alonso P, Cuadras D, Gabriels L, et al. Deep brain Deep brain stimulation for intractable obsessive
(http://creativecommons.org/licenses/by/4.0/).
stimulation for obsessive-compulsive disorder: a compulsive disorder: pilot study using a blinded,
WORLD NEUROSURGERY -: e1-e9, - 2021 www.journals.elsevier.com/world-neurosurgery e9You can also read

















































