Original Article The effect of selective pterygoid canal neurotomy under nasal endoscopy on postoperative pain in patients with chronic sinusitis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Int J Clin Exp Med 2020;13(4):2807-2814 www.ijcem.com /ISSN:1940-5901/IJCEM0106803 Original Article The effect of selective pterygoid canal neurotomy under nasal endoscopy on postoperative pain in patients with chronic sinusitis Dijiang Ma, Jianing Sun, Qi Zhu Department of Otorhinolaryngology, Head and Neck Surgery, Yuyao People’s Hospital, Yuyao, Zhejiang, China Received December 23, 2019; Accepted January 15, 2020; Epub April 15, 2020; Published April 30, 2020 Abstract: Objective: To investigate the effect of selective pterygoid canal neurotomy under nasal endoscopy on patients with chronic sinusitis and nasal polyps. Methods: Eight-six patients with chronic sinusitis and nasal polyps were randomly and evenly divided into control and research groups. The control group patients underwent conven- tional minimally invasive endoscopic nasal surgery, and the research group patients underwent selective pterygoid canal neurotomy under nasal endoscopy. The pain degree, stress-response indicators, Bruggemann comfort scale (BCS) scores, quality of life, duration of the hospitalization, surgical wound recovery time, incidence of adverse reac- tions, and curative effects in the two groups were compared. Results: The patients in the research group exhibited higher levels of pain than those in the control group (P
The effect of selective pterygoid canal neurotomy
gy used in otolaryngology has reduced trauma This study was approved by the Medical Ethics
and shortened recovery times [7, 8]. The treat- Committee of our hospital, and written inform-
ment of chronic sinusitis usually involves mini- ed consent was obtained from all study partici-
mally invasive endoscopic nasal surgery. The pants or their legal guardians.
lesion tissue can be visually observed using a
nasal endoscope, and the polyps can be cle- Reagents and materials
ared, achieving the radical treatment of sinus-
itis, thereby alleviating inflammation, restoring Nasal endoscopy equipment was purchased
sinus ventilation and induction/drainage func- from Jiangsu Ouman Electronic Equipment Co.
Ltd., and a dynamic electrocardiograph was
tion, and ensuring normal physiological sinus
purchased from Beijing Avantgarde Medical
function [9, 10]. However, facial pain can be
Equipment Co., Ltd.
more intense than pain in the limbs and trunk,
and as endoscopic sinus surgery is performed
Experimental methods
in the nasal cavity, postoperative pain and
safety are receiving increased attention. This Surgical approaches: Minimally invasive en-
study set out to assess the effects of selec- doscopic nasal surgery, which primarily in-
tive pterygoid canal neurotomy on postopera- cludes endoscopic sinus surgery and nasal
tive pain and safety in patients with chronic polypectomy, was performed on the con-
sinusitis and nasal polyps. trol group patients according to the condi-
tion of each patient. The research group pa-
Materials and methods tients also received selective pterygoid ca-
General information nal neurotomy under nasal endoscopy. The sur-
gical procedures were as follows: A wide-angle
A total of 86 patients with chronic sinusitis nasal endoscopy was dissected from the pos-
and nasal polyps treated at our hospital from terior fontanel of the open maxillary sinus to
February 2016 to March 2018 were randomly find the sphenopalatine foramen at the verti-
assigned to a control or research group, with cal plate of the jaw, and the periosteum of the
43 assigned to each group. The patients in sphenopalatine foramen was torn within 2 cm.
the control group received conventional mini- The nerve fascicles from various sources, in-
mally invasive endoscopic nasal surgery. The cluding the vascular nerve fascicles perforat-
research group patients were treated with se- ing from the sphenopalatine foramen and the
lective pterygoid canal neurotomy under nasal nerve fascicles passing through the bone sur-
endoscopy, the primary procedure of which face, were identified. The nerve fascicles were
involves severing the posterior nasal nerve then separated by a slim bulbous probe and
cut off by a needle-like electrode to protect the
and the pharyngeal branch of the pterygoid
peripheral nerve arteries during the operation.
canal nerve. Of the patients, 47 were men and
Next, small nerves that may cause nerve-to-
39 women, with an average age of 43.45 ±
nerve connections were cut off using micro-
11.72 years.
scopic scissors. Finally, the pterygopharyngeal
Inclusion and exclusion criteria branch of the pterygoid nerve on the inferior
bone surface of the anterior wall of the sphe-
The inclusion criteria were as follows, patients noid sinus was found and separated from the
meeting: (1) the diagnostic criteria for chronic palatal sheath canal. The free neurovascular
sinusitis with nasal polyps [11]; (2) the evalua- fascicles were found through the bone of the
tion criteria for endoscopic sinus surgery [12]; anterior wall of the palatal sheath canal and
and (3) patients presenting with nasal conges- were cut off using a plasma knife head or nee-
tion, runny nose, facial distention and tight- dle electrode.
ness, a decline in olfactory function, and other
symptoms. Index detection method
The exclusion criteria were as follows, pati- All patients were monitored by electrocardio-
ents with: (1) fungal sinusitis; (2) cystic fibrosis; gram at 15 min, 3 min, and 1 h after surgery.
(3) immunodeficiency diseases; (4) immune or The primary monitoring indicators included dia-
blood system diseases; (5) cognitive or com- stolic and systolic blood pressure, heart rate,
munication disorders; or (6) poor compliance. and pulse oxygen saturation.
2808 Int J Clin Exp Med 2020;13(4):2807-2814The effect of selective pterygoid canal neurotomy
Table 1. General information about the patients in the two groups
Categories Control group (n = 43) Research group (n = 43) X2/t P
Sex (cases) 0.047 0.829
Male 24 (55.81) 23 (53.49)
Female 19 (44.19) 20 (46.51)
Age (years) 43.28 ± 11.79 43.83 ± 11.58 0.218 0.828
History of illness (years) 2.43 ± 0.98 2.48 ± 0.94 0.241 0.810
Smoking (cases) 0.054 0.816
Yes 30 (69.77) 29 (67.44)
No 13 (30.23) 14 (32.56)
Drinking (cases) 0.191 0.662
Yes 24 (55.81) 26 (60.47)
No 19 (44.19) 17 (39.53)
Respiratory tract infection (cases) 0.341 0.559
Yes 6 (13.95) 8 (8.60)
No 37 (86.05) 35 (81.40)
Polyp size (cm) 1.83 ± 0.42 1.89 ± 0.45 0.639 0.524
Polyp site (cases) 0.232 0.972
Maxillary sinus 7 (16.28) 6 (13.95)
Ethmoid sinus 4 (9.30) 4 (9.30)
Middle nasal meatus 17 (39.53) 16 (37.21)
Middle nasal meatus 15 (34.88) 17 (39.53)
Observational indicators (4) Quality of life was assessed using a chronic
sinusitis-related quality of life questionnaire
(1) Each patient’s degree of pain was assessed after treatment, including items related to daily
using the visual analog scale on the first day activities, nasal symptoms, ophthalmic symp-
after surgery. The patients scored themselves toms, inflammatory reactions, related behav-
according to their nasal condition on a scale iors, sleep, emotional reactions, etc. With a
ranging from 0 to 10, with mild pain given 1-3 total score of 6 points for each observation
points, moderate pain 4-6 points, and severe indicator, the scores and corresponding diag-
pain more than 7 points. The diagnoses were noses were as follows: 0 points: patients were
made based on whether there were symptoms not affected by nasal or ophthalmic symptoms;
such as nasal obstruction and runny nose in 1 point: basically unaffected; 2 points: slightly
the left and right nasal passages, sneezing, affected; 3 points: mildly affected; 4 points:
nasal itching, eye itching, facial bloating, olfac- moderately affected; 5 points: severely affect-
tory symptoms, etc. The final self-evaluation ed; 6 points: extremely severely affected. The
scores assigned by the patients were similar to lower the score, the better the quality of life
those given by the specialist medical staff [13]. [15].
(2) Patient stress-response indicators, includ- (5) The duration of hospitalization and the sur-
ing diastolic blood pressure, systolic blood gical wound recovery time in the two groups
pressure, and the heart rate and pulse oxygen were observed and recorded.
saturation of the two groups were observed
and recorded before and after surgery. (6) The incidence of adverse reactions was
compared between the two groups.
(3) The comfort levels were assessed using the
Bruggemann comfort scale (BCS) at 1, 2, and 3 (7) The curative effects of the patients in the
h after surgery. The comfort levels of all the two groups were compared using specific
patients were monitored within 1 week, and the terms-markedly effective: the symptoms and
lower the score, the worse the comfort level of signs basically disappeared compared with
the patients [14]. those before the treatment; effective: the
2809 Int J Clin Exp Med 2020;13(4):2807-2814The effect of selective pterygoid canal neurotomy
Table 2. Postoperative pain in the two groups [n (%)] phPad Prism 8. The measur-
Control group Research group able values were analyzed
Categories X2 P using chi-squared tests, and
(n = 43) (n = 43)
Mild pain 13 (30.23) 29 (67.44) 11.911 0.05) (Table 1).
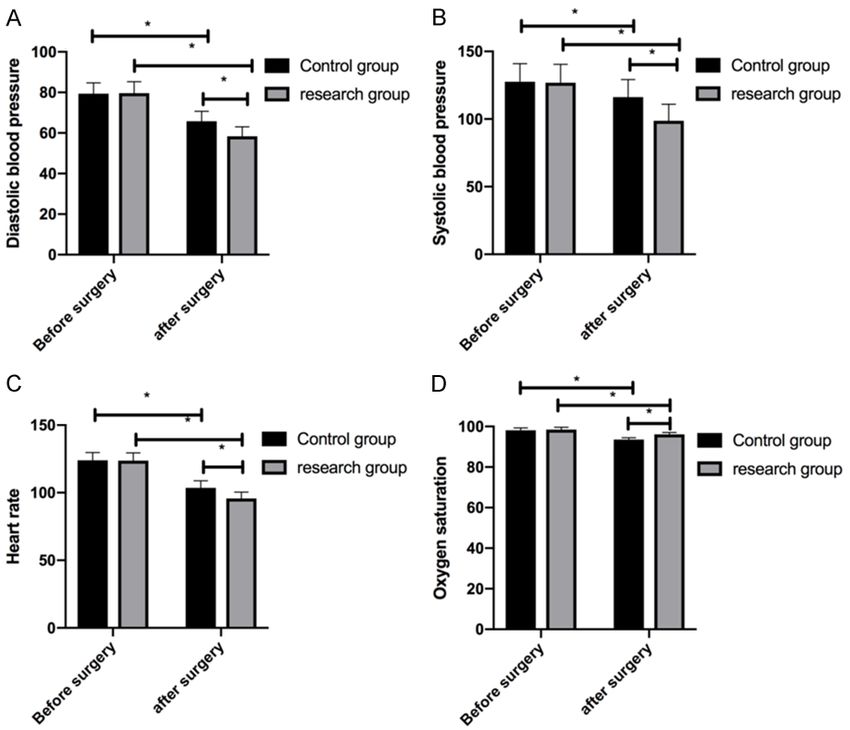
before and after surgery. A. The postoperative diastolic blood pressure in
both groups decreased significantly compared with the levels before treat-
ment, and the diastolic blood pressure in the control group was significantly No significant difference in
higher than the level in the research group. B. The systolic blood pressure the number of patients with
in both groups decreased significantly compared with the level before treat- severe pain in the two groups
ment, and the level in the control group was significantly higher than it was
in the research group. C. After treatment, the heart rates of the patients in
the two groups decreased significantly compared with the rates before treat-
The number of patients with
ment, and the rate in the control group was significantly higher than it was mild pain in the control group
in the research group. D. The postoperative oxygen pulse saturation in the was significantly lower than
two groups decreased significantly compared with before treatment, and the the number in the research
level in the control group was significantly lower than it was in the research group, and the number of pa-
group. Note: * represents P0.05). After treatment, the
Ltd.), and the data were plotted using Gra- stress-response indicators in the two groups
2810 Int J Clin Exp Med 2020;13(4):2807-2814The effect of selective pterygoid canal neurotomy
Table 3. BCS scores at various postoperative time points in the two The research group showed
groups higher BCS scores
Control group Research group
Categories t P The BCS scores of the pa-
(n = 43) (n = 43)
tients in the control group at
1 h after surgery 2.46 ± 0.47 2.79 ± 0.52 3.087 0.003
1, 2, and 3 h after surgery
2 h after surgery 2.71 ± 0.53 3.07 ± 0.56 3.062 0.003
were significantly lower than
3 h after surgery 3.09 ± 0.54 3.36 ± 0.58 2.234 0.028 the scores in the research
group, with statistically sig-
nificant differences (PThe effect of selective pterygoid canal neurotomy
Table 5. Adverse reactions in the two groups [n (%)]
Categories Control group (n = 43) Research group (n = 43) X2 P
Active hemorrhage 4 (9.30) 3 (6.98) - -
Postoperative cavity adhesion 3 (6.98) 2 (4.65) - -
Respiratory complications 2 (4.65) 2 (4.65) - -
Sinus obstruction 2 (4.65) 1 (2.33) - -
Total incidence of adverse reactions 11 (25.58) 8 (18.60) 0.608 0.436
Table 6. The curative effects in the two groups [n (%)] some degree of pain sympto-
Control group Research group ms after surgery, mostly mod-
Categories X2 P erate pain, which is the key
(n = 43) (n = 43)
reason for delayed recovery
Markedly effective 14 (32.56) 26 (60.47) - -
and reduced quality of life.
Effective 21 (48.84) 15 (34.88) - -
Based on our study results,
Ineffective 8 (18.60) 2 (4.65) - - selective pterygoid canal neu-
Total effective rate 35 (81.40) 41 (95.35) 4.074 0.044 rotomy can effectively relieve
postoperative pain in patien-
ts with chronic sinusitis and
caused by nasal hypersecretions, and the main nasal polyps. With further evaluation, it was
factor leading to active nasal secretions is the found that the stress-response indicators of
parasympathetic nerve, which regulates nasal se- the two groups decreased significantly after
cretions by innervating the nasal glands [19]. treatment. Diastolic and systolic blood pres-
The parasympathetic nerve innervating the sure and heart rates in the control group were
nasal cavity originates at the superficial petro- significantly higher than those in the research
sal nerve and is collectively referred to as the group, and the pulse oxygen saturation mea-
pterygoid canal nerve [20]. Pterygoid canal surements in the control group were signifi-
neurotomy can therefore reduce the number cantly lower than those in the research group.
of parasympathetic nerves distributed in the Previous studies [24, 25] demonstrated that
blood vessels, eliminate incentives leading to treating chronic sinusitis patients with surgi-
the increase of nasal secretions, reduce the cal treatment stimulates a strong response by
sensitivity of nasal mucosa and other associ- the sympathetic nervous system, resulting in a
ated parts, adjust the nasal environment, and significant increase in catecholamine content
reduce the production of polyps [21]. in the body and affecting the expression of the
stress-response indicators. Selective pterygoid
In this study, the number of patients with mild
canal neurotomy is a procedure that cuts off
pain in the control group was significantly lower
the mixed nerve innervating the nasal mucosa,
than it was in the research group, the number
preventing the regulation of the parasympa-
of patients with moderate pain in the control
thetic nerve’s dominant function, thereby regu-
group was significantly higher than it was in the
research group, and the number of patients lating vasoconstriction and gland secretion in
with severe pain in the control group was not the nasal cavity and sinuses and making the
significantly different from the number in the excitability of the cholinergic nerve endings
research group. This suggests that pain will disappear in the nasal cavity [26]. The above
generally decrease after recovery, and there observations are consistent with our findings,
were almost no patients with abnormal pain. which indicate that pterygoid canal neurotomy
Minimally invasive endoscopic nasal surgery can reduce the postoperative stress-response
and pterygoid canal neurotomy appear to be and alleviate pain and other adverse reactions.
equally effective treatments for sinusitis, and In terms of comfort and quality of life, the BCS
the pain degree of patients undergoing selec- scores of the control group patients were sig-
tive pterygoid canal neurotomy is significantly nificantly lower than those of the research
lower than the pain degree of patients under- group patients at 1, 2, and 3 h after surgery.
going minimally invasive endoscopy nasal sur- The quality of life indicators in the control gro-
gery alone. Studies [22, 23] have shown that up were significantly higher than those in the
patients with chronic sinusitis are prone to research group. This suggests that the pati-
2812 Int J Clin Exp Med 2020;13(4):2807-2814The effect of selective pterygoid canal neurotomy
ents’ quality of life improved after the ptery- and Ningbo Science and Nature Fund Project
goid canal neurotomy, and the discomfort cau- (No. 2019A610324).
sed by the sinusitis and nasal polyps was sig-
nificantly reduced. Furthermore, the recovery Disclosure of conflict of interest
times, adverse reactions, and curative efficacy
None.
were observed and compared between the two
groups. It was found that the duration of hospi- Address correspondence to: Qi Zhu, Department of
talization and recovery times of the surgical Otorhinolaryngology, Head and Neck Surgery, Yuyao
wounds in the research group were longer than People’s Hospital, No. 800 Chengdong Road, Yuyao
they were in the control group. The research 315400, Zhejiang, China. Tel: +86-13566085198;
group exhibited a higher effective rate than the E-mail: zhuiziq@163.com
control group. The recovery times of the pati-
ents undergoing selective pterygoid canal neu- References
rotomy under nasal endoscopy were slightly
longer than those of the patients who recei- [1] Sobol SE, Samadi DS, Ken K and Tom LW.
ved only conventional treatments. This may Trends in the management of pediatric chro-
nic sinusitis: survey of the American Society of
be because the selection of surgical sites for
Pediatric Otolaryngology. Laryngoscope 2010;
the former treatment is relatively large, which 115: 78-80.
leads to prolonged recovery times. Neverthe- [2] Ziegler A, Patadia M and Stankiewicz J. Neuro-
less, the curative effect of selective pterygoid logical complications of acute and chronic si-
canal neurotomy is superior and is associated nusitis. Curr Neurol Neurosci Rep 2018; 18: 5.
with no increase in postoperative adverse reac- [3] Majima Y, Sakakura Y and Matsubara T. Possi-
tions. According to a literature review [27], sur- ble mechanisms of reduction of nasal muco-
gical treatment for refractory chronic sinusitis ciliary clearance in chronic sinusitis. Clin Oto-
accompanied by relatively stable postoperative laryngol Allied Sci 2010; 11: 55-60.
recovery and overall curative effect may result [4] Min-man W, Hong S, Zhi-qiang X, Xue-ping F,
in dry-eye symptoms, facial or palatal numb- Chang-qi L and Dan L. Differential proteomic
ness, and other surgical risks, which are con- analysis of nasal polyps, chronic sinusitis, and
normal nasal mucosa tissues. Otolaryngol
sistent with our findings. We found no signifi-
Head Neck Surg 2009; 141: 364-368.
cant increase in adverse reactions in our study, [5] Platt MP, Soler ZM, Kao SY, Metson R and
indicating that pterygoid canal neurotomy does Stankovic KM. Topographic gene expression in
not affect overall safety under reasonable and the sinonasal cavity of patients with chronic
scientific conditions. sinusitis with polyps. Otolaryngol Head Neck
Surg 2011; 145: 171-175.
In conclusion, selective pterygoid canal neu- [6] Ren J and Huangfu H. Analysis of olfactory re-
rotomy for chronic sinusitis with nasal polyps habilitation after endoscopic sinus surgery in
can significantly alleviate pain in patients, par- patients with chronic sinusitis and nasal pol-
ticularly in the nasal cavity, with higher safety yps. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke
and a superior curative effect. A major limita- Za Zhi 2016; 30: 106-110.
tion of this study, however, is the study of [7] Atlas SJ, Metson RB, Singer DE, Wu YA and
adverse reactions. The grouping and timing of Gliklich RE. Validity of a new health-related
the postoperative adverse reactions were spo- quality of life instrument for patients with
radic, and the statistical analysis of the ad- chronic sinusitis. Laryngoscope 2010; 115:
846-854.
verse reactions was complicated. We recorded
[8] Bajaj Y, Sethi N, Carr S and Knight LC. Endo-
only those adverse reactions observed at a
scopic sinus surgery as day-case procedure. J
uniform time after surgery and only followed Laryngol Otol 2009; 123: 619-622.
the patients’ conditions for a short period of [9] Zhang W, Xiao H and Huang H. Significance of
time. Further studies are necessary to evalu- treatment chronic sinusitis in children with ad-
ate the safety and effectiveness of selective enoidectomy with nasal endoscope. Modern
pterygoid canal neurotomy for the treatment Hospital 2008.
of patients with chronic sinusitis with nasal [10] You X, Liu Z, Hu J, Gao Q and Cui Y. Rehabilita-
polyps. tion therapy after nasal endoscopic surgery for
nasal polyp and chronic sinusitis patients. Lin
Acknowledgements Chuang Er Bi Yan Hou Ke Za Zhi 2005; 19: 31-
33.
This work was supported by Yuyao People’s [11] Fokkens WJ, Lund VJ, Mullol J, Bachert C, Alo-
Hospital Youth Fund Project (No. 2018QA04) bid I, Baroody F, Cohen N, Cervin A, Douglas R,
2813 Int J Clin Exp Med 2020;13(4):2807-2814The effect of selective pterygoid canal neurotomy
Gevaert P, Georgalas C, Goossens H, Harvey R, [20] Inoue K and Kitada Y. Parasympathetic post-
Hellings P, Hopkins C, Jones N, Joos G, Kalo- ganglionic nerve fibers in the fungiform papil-
gjera L, Kern B, Kowalski M, Price D, Riechel- lae of the frog. Anat Rec 2010; 230: 131-135.
mann H, Schlosser R, Senior B, Thomas M, [21] Nishijima H, Kondo K, Toma-Hirano M, Iwasaki
Toskala E, Voegels R, Wang de Y and Wormald S, Kikuta S, Fujimoto C, Ueha R, Kagoya R and
PJ. European position paper on rhinosinusitis Yamasoba T. Denervation of nasal mucosa in-
and nasal polyps 2012. Rhinol Suppl 2012; duced by posterior nasal neurectomy sup-
23: 3 p preceding table of contents, 1-298. presses nasal secretion, not hypersensitivity,
[12] Fischer M, Grobner C, Dietz A, Lueth TC in an allergic rhinitis rat model. Lab Invest
and Strauss G. First clinical experiences with 2016; 96: 981-993.
an endoscope manipulator system in endo- [22] Finkensieper M, Poller K, Wittekindt C, Meiss-
and transnasal surgery. Laryngorhinootologie ner W and Guntinas-Lichius O. Postoperative
2012; 91: 487-493. pain assessment after functional endoscopic
[13] Kahveci OK, Miman MC, Yucel A, Yucedag F, sinus surgery (FESS) for chronic pansinusitis.
Okur E and Altuntas A. The efficiency of nose Eur Arch Otorhinolaryngol 2013; 270: 157-
obstruction symptom evaluation (NOSE) scale 166.
on patients with nasal septal deviation. Auris [23] Wu CL, Naqibuddin M, Rowlingson AJ, Lietman
Nasus Larynx 2012; 39: 275-279. SA, Jermyn RM and Fleisher LA. The effect of
[14] Yang ZL, Sun SQ and Zhang KJ. Subjective pain on health-related quality of life in the im-
evaluation model and system for sitting com- mediate postoperative period. Anesth Analg
fort based on gene expression programming. 2003; 97: 1078-1085.
CIMS 2012; 18: 2138-2144. [24] El Mograbi A and Soudry E. Ocular cranial
[15] Linder JA and Atlas SJ. Health-related quality of nerve palsies secondary to sphenoid sinusitis.
life in patients with sinusitis. Curr Allergy Asth- World J Otorhinolaryngol Head Neck Surg
ma Rep 2004; 4: 490-495. 2017; 3: 49-53.
[16] Kuhn FA, Melroy CT, Levine HL and Diamond [25] Madden KS, Sanders VM and Felten DL. Cate-
AJ. Drug-eluting spacer for chronic ethmoid si- cholamine influences and sympathetic neural
nusitis treatment. Otolaryngology Head and modulation of immune responsiveness. Annu
Neck Surgery 2008; 139: P75. Rev Pharmacol Toxicol 1995; 35: 417-448.
[17] Ma M and Liu Y. Exploring of surgery solution [26] Hwang PH, Lin B, Weiss R, Atkins J and John-
for chronic sinusitis treatment and application son J. Cryosurgical posterior nasal tissue abla-
of partial middle turbinectomy. Lin Chuang Er tion for the treatment of rhinitis. Int Forum Al-
Bi Yan Hou Ke Za Zhi 2003; 17: 454-455. lergy Rhinol 2017; 7: 952-956.
[18] Conley DB, Tripathi A, Ditto AM, Reid K, Gram- [27] Low WK. Complications of the Caldwell-Luc op-
mer LC and Kern RC. Chronic sinusitis with na- eration and how to avoid them. Aust N Z J Surg
sal polyps: staphylococcal exotoxin immuno- 1995; 65: 582-584.
globulin E and cellular inflammation. Am J
Rhinol 2004; 18: 273-278.
[19] Sapci T, Yazici S, Evcimik MF, Bozkurt Z, Kara-
vus A, Ugurlu B and Ozkurt E. Investigation of
the effects of intranasal botulinum toxin type A
and ipratropium bromide nasal spray on nasal
hypersecretion in idiopathic rhinitis without eo-
sinophilia. Rhinology 2008; 46: 45-51.
2814 Int J Clin Exp Med 2020;13(4):2807-2814You can also read