PARANEOPLASTIC IGA NEPHROPATHY AND IGA VASCULITIS IN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Int J Case Rep Images 2019;10:101063Z01KB2019. Bartolomeo et al. 1
www.ijcasereportsandimages.com
CASE REPORT PEER REVIEWED | OPEN ACCESS
Paraneoplastic IgA nephropathy and IgA vasculitis in
mesothelioma
Korey Bartolomeo, Said Al Zein, Joan Cullen,
Catherine Abendroth, Gurwant Kaur
ABSTRACT How to cite this article
Immunoglobulin A (IgA) vasculitis and IgA Bartolomeo K, Al Zein S, Cullen J, Abendroth C,
nephropathy have been associated with Kaur G. Paraneoplastic IgA nephropathy and IgA
underlying malignancies when present in adult vasculitis in mesothelioma. Int J Case Rep Images
populations. To date, we have found only two 2019;10:101063Z01KB2019.
previously reported cases of IgA vasculitis
and one IgA nephropathy case associated with
mesothelioma, with our patient being the Article ID: 101063Z01KB2019
fourth. Our case describes a patient with biopsy
proven IgA nephropathy and IgA vasculitis with
known malignant mesothelioma who presented *********
with features of lower extremity purpura, doi: 10.5348/101063Z01KB2019CR
leukocytoclastic rash, and dialysis-dependent
acute kidney injury (AKI).
Keywords: Acute kidney injury, Crescentic IgA INTRODUCTION
nephropathy, Henoch–Schönlein purpura, IgA
nephropathy, IgA vasculitis, Mesothelioma Immunoglobulin A nephropathy (IgAN) is the most
common primary glomerular pathology worldwide,
regardless of age [1, 2]. It is diagnosed by the presence of
IgA deposition in the mesangium of the glomerulus, often
accompanied by other immunoglobulins or complement
Korey Bartolomeo1, Said Al Zein2, Joan Cullen1, Catherine
Abendroth3, Gurwant Kaur4 on histological examination [3]. Prognosis is dependent
on multiple clinical and pathologic markers, but 10-year
Affiliations: 1Internal Medicine Resident, Department of Medi-
survival can be as high as 90% [4, 5].
cine, Penn State Milton S. Hershey Medical Centre, 500 Uni-
versity Drive, Hershey, Pennsylvania, USA; 2Nephrology Fel-
Immunoglobulin A vasculitis (IgAV), formerly called
low, Department of Medicine (Nephrology), Penn State Milton Henoch–Schönlein purpura, is the most common
S. Hershey Medical Centre, 500 University Drive, Hershey, vasculitis in pediatric populations [1]. It is characterized
Pennsylvania, USA; 3Department of Pathology, Penn State by nonthrombocytopenic palpable purpura with the
Milton S. Hershey Medical Centre, 500 University Drive, Her- presence of abdominal pain, arthritis, leukocytoclastic
shey, Pennsylvania, USA; 4Assistant Professor of Medicine, vasculitis on biopsy, and renal disease [6–8]. The renal
Department of Medicine (Nephrology), Penn State Milton manifestations in both IgAN and IgAV share multiple
S. Hershey Medical Centre, 500 University Drive, Hershey, pathophysiologic mechanisms, including abnormal
Pennsylvania, USA.
IgA1 O-glycosylation. The overall mechanism of injury,
Corresponding Author: Gurwant Kaur, MD, FASN, Assistant however, remains poorly defined, and despite this overlap
Professor of Medicine, Department of Medicine (Nephrol- there is considerable heterogeneity in outcomes among
ogy), Penn State Milton S. Hershey Medical Centre, 500 IgAN and IgAV [9, 10].
University Drive, Hershey, Pennsylvania 17033, USA; Email:
Immunoglobulin A vasculitis in adults is much less
gkaur1@pennstatehealth.psu.edu
common than in pediatrics, with an incidence of 0.1–1.8
per 100,000 individuals compared to 3–26 per 100,000 in
Received: 02 August 2019 children [6, 11, 12]. It also tends to have a worse prognosis
Accepted: 18 September 2019 in adults compared to children, including higher rates of
Published: 29 October 2019 progression to end stage renal disease, more frequent
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101063Z01KB2019. Bartolomeo et al. 2
www.ijcasereportsandimages.com
relapses, and higher incidence of life-threatening extra- On physical examination, he appeared to be in no
renal complications [13, 14]. acute distress although his oxygen saturation was 92% on
Immunoglobulin A nephropathy and IgAV are both 2 L of oxygen via nasal cannula. His blood pressure was
associated with many systemic illnesses, including liver 150/75 mmHg, heart rate 78 beats/minute, respiratory
disease, ankylosing spondylitis, and inflammatory bowel rate 20 breaths/minute, and his temperature was 36.2°C.
disease [15–18]. An increasing body of literature has He appeared slightly pale and had coarse crackles at
described IgAN and IgAV as a finding in malignancy, the bilateral lung bases. He had bilateral small purpuric
particularly with lung involvement [19–22]. Here we lesions on his lower extremities extending up to the thighs.
describe a case of biopsy proven IgAN and IgAV in the His abdominal and joint examination was unremarkable.
setting of recent mesothelioma diagnosis with a literature His blood work was relevant for blood urea nitrogen
review of mesothelioma associations with both disorders. of 39 mg/dL (6–23 mg/dL), creatinine of 2.07 mg/dL,
potassium 3.3 mg/dL (3.5–5.1 mg/dL), white blood cell
count 20.25 K/uL (4–10.4 K/uL), hemoglobin 10.6 g/dL
CASE REPORT (13–17 g/dL), and a platelet count of 364 K/uL (150–350
K/uL). Urine analysis showed glucose 100 mg/dL, large
A 74-year-old Caucasian man presented with amount of hemoglobin (via pseudoperoxidase activity;
recently diagnosed stage IIIb malignant desmoplastic normal: none), protein >300 mg/dL, positive nitrites,
mesothelioma by histology (immunohistochemistry and trace leukocyte esterase. Urine white blood cells were
positive for CK-AE 1/3, CK 5/6, calretinin, D240, EMA, 5–9 cells/HPF and RBCs were 50+ cells/HPF. The urine
and CK7) requiring right thoracotomy and decortication protein to creatinine ratio was 8.91 and a 24-hour urine
due to a trapped lung. At the time of mesothelioma collection revealed nephrotic range proteinuria of 8.45 g.
diagnosis, he had a creatinine of 0.8 mg/dL and no red Renal ultrasound demonstrated increased
blood cells (RBCs) on urine analysis. His other past echogenicity of the left kidney and simple cysts in the
medical history was relevant for grade II clear cell renal upper pole. The right kidney was unremarkable in size,
carcinoma treated with partial nephrectomy 11 years echogenicity, or other pathology.
prior, with no evidence of recurrence, and coronary artery During his hospital course, the patient underwent a
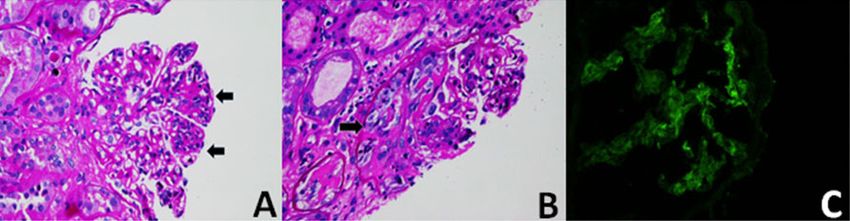
disease with coronary artery bypass grafting five years renal biopsy (Figure 1) due to rising creatinine in the setting
prior to presentation. His chronic medications included of gross hematuria and nephrotic range proteinuria.
atorvastatin, felodipine, and metoprolol. Biopsy showed asynchronous mesangial and segmental
Three weeks after diagnosis, he presented to the endocapillary proliferation with focal subcircumferential
emergency department for a purpuric rash and was found epithelial crescents. One-third of the glomerular tufts
to have an AKI, with a creatinine of 1.7 mg/dL and 50+ RBC were globally sclerotic. Mesangial deposition of IgA and
on urine analysis. A skin biopsy showed leukocytoclastic codominant C3 was noted by immunofluorescence as
vasculitis with IgA deposition on immunofluorescence. well as mesangial electron densities by ultrastructural
He was discharged on prednisone 40 mg daily. Upon examination, which supported a diagnosis of IgA
outpatient follow-up with his oncologist the patient was nephropathy with an Oxford criteria (MEST-C of M1, S0,
found to have a worsening AKI (creatinine 2.1 mg/dL). E1, T0, C1).
A planned course of carboplatin and pemetrexed was The initiation of pulse steroids was delayed until the
postponed due to concern for further nephrotoxicity. fifth day of his hospitalization due to concern for acute
He presented to the emergency department shortly after pneumonia. His creatinine continued to rise to 4.52 mg/
with persistent painless gross hematuria. dL and he received pulse methylprednisolone 1000 mg
Figure 1: Renal histology in IgAV, (A) mild global mesangial cellular proliferation and segmental endocapillary proliferation (arrows)
resulting in closure of capillary loops [Periodic acid–Schiff (PAS) × 500]. (B) Mesangial cellular proliferation and segmental tuft
necrosis with associated fibroepithelial crescent (arrow). Crescents were present in a minority of tufts (PAS × 500). (C) Granular IgA
deposition in mesangial stalks; there was codominant staining for C3 (immunofluorescence, IgA, ×500).
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101063Z01KB2019. Bartolomeo et al. 3
www.ijcasereportsandimages.com
intravenously for three days, followed by prednisone addition to the absence of evidence of renal cell carcinoma
80 mg orally daily. Initially, he remained nonoliguric recurrence, makes paraneoplastic development
without significant electrolyte abnormalities; however, secondary to malignant pleural mesothelioma much
he eventually was started on hemodialysis with a peak more likely. Immunoglobulin A nephropathy association
creatinine of 7.59 mg/dL. He was discharged 17 days after with mesothelioma, in particular, has previously been
admission and continued on prednisone therapy with scarcely described in only one other case, with our patient
hemodialysis three times a week. adding to the literature [31].
His posthospitalization course was complicated by Adult-onset IgAV has a well-described association,
atrial fibrillation with rapid ventricular rate, treated with lung malignancy and it is considered the most
medically. His purpuric rash resolved and he remained common solid tumor associated with IgAV [19, 32–
dialysis dependent even after two months of AKI and his 50]. Squamous cell carcinoma subtype represents the
prednisone was tapered to 20 mg daily. His oncologist majority of these cases, followed by adenocarcinoma
held further chemotherapy given the stability of his and small cell carcinoma, and this may represent a slight
mesothelioma on follow-up thoracic imaging. overrepresentation compared to the general incidence of
lung cancer in the United States [32, 47, 49, 51]. To date,
we are aware of only two prior cases of IgAV associated
DISCUSSION with mesothelioma, with our patient being the third
reported case [48, 50].
Immunoglobulin A nephropathy and IgAV are Comparing our patient with previously described
classically described as primary pathologies, but an IgAN and IgAV cases associated with malignant
increasing body of literature has recognized them pleural mesothelioma demonstrates a number of
as secondary to other systemic processes, including trends. All cases demonstrated initial responsiveness
malignancy [18, 19, 23]. Our patient had biopsy confirmed to immunosuppression, usually with prednisone, but
IgAN and IgAV in the setting of a recent diagnosis of without any consistent trend in dosing [31, 48, 50].
mesothelioma and distant history of clear cell renal Unfortunately, progression of renal disease occurred in
carcinoma. our patient and two of the three total IgAN and IgAV
Our patient presented with gross hematuria, cases previously described [31, 50]. The deterioration of
nephrotic range proteinuria without nephrotic syndrome, renal function observed in our patient is similar to IgAV
and an AKI which rapidly progressed toward dialysis cases reported in the elderly, who tend to have higher
dependency. This severe presentation is considerably rates of progressive renal insufficiency compared to those
uncommon for primary IgAN and IgAV [2, 24], which diagnosed at a younger age [52]. Renal prognosis, even
raised suspicion for secondary nephropathy etiologies in the elderly, remains favorable, though in aggressive
or other glomerulonephropathies, including minimal malignancy-associated IgAV, this trend would be difficult
change disease and membranous nephropathy. to detect, as most patients succumb to their malignancy
Tissue diagnosis confirmed IgAN and IgAV, with prior to resolution of the nephritis [53]. Unfortunately,
the kidney biopsy showing mesangial hypercellularity there are no large prospective or randomized clinical
>50% (M1) and endocapillary hypercellularity (E1) trials that have confirmed these observations in IgAV and
without evidence of segmental glomerulosclerosis (S0), malignancy [24].
tubular atrophy (T0), or crescent formation (C1) [25]. Mesothelioma outcomes were more difficult to
This categorization would generally correspond with a compare as the timing of diagnosis varied greatly and none
favorable overall IgAN prognosis via classic Oxford criteria of the cases opted for treatment of the mesothelioma. The
with probable immunosuppression responsiveness. Our average life expectancy of malignant pleural mesothelioma
patient had poor improvement with immunosuppression without treatment is around 12 months [54]. At eight
therapy and instead developed rapid progression toward months follow-up after mesothelioma diagnosis, two of
dialysis dependency. This may be due to lack of validation the three case reports culminated in death [31, 50]. Our
of the Oxford classification in adults with concomitant patient remains dialysis dependent at approximately five
IgAV or those with secondary IgAN, or the presence of months postmesothelioma diagnosis.
crescents, which tends to predict worse outcomes [26, 27]. Our case report adds to the growing evidence detailing
Alternatively, IgAN progression is variable overall and our the association between two rare disorders in adults.
patient may have fallen in the minority cohort who does This analysis is limited given the extremely few case
develop progressive end stage renal disease [28]. reports in the English literature and lack of large-scale
Immunoglobulin A nephropathy is uncommonly trials that have involved IgAV or IgAN in association
recognized as a paraneoplastic disorder in solid tumors, with malignancy. Our findings support the need for
with the strongest associations in renal cell carcinoma heightened awareness when making a diagnosis of IgAV
and lung cancers [23, 29, 30]. While our patient had a and maintaining a high clinical suspicion for underlying
distant history of clear cell renal carcinoma, the timing of malignancy meriting appropriate cancer screening
IgAN development with his diagnosis of mesothelioma, in in these patients. Further studies are needed to more
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101063Z01KB2019. Bartolomeo et al. 4
www.ijcasereportsandimages.com
clearly delineate the association between IgAV, IgAN, 13. Pillebout E, Thervet E, Hill G, Alberti C, Vanhille
and underlying malignancy, in particular mesothelioma. P, Nochy D. Henoch-Schönlein purpura in adults:
Future investigations that focus on the pathophysiologic Outcome and prognostic factors. J Am Soc Nephrol
links between cancer development and IgA-related 2002;13(5):1271–8.
14. Batu ED, San A, Erden A, et al. Comparing
renal disease can help elucidate potential risk factors
immunoglobulin A vasculitis (Henoch-Schönlein
for development, diagnostic modalities, and, ultimately, purpura) in children and adults: A single-centre study
evidence-based treatments. from Turkey. Scand J Rheumatol 2018;47(6):481–6.
15. Hemminger J, Arole V, Ayoub I, Brodsky SV, Nadasdy
T, Satoskar AA. Acute glomerulonephritis with large
CONCLUSION confluent IgA-dominant deposits associated with
liver cirrhosis. PLoS One 2018;13(4):e0193274.
Adult onset IgAV and IgAN are increasingly recognized 16. Peeters AJ, van den Wall Bake AW, Daha MR, Breeveld
as potential paraneoplastic syndromes. Detection of FC. Inflammatory bowel disease and ankylosing
spondylitis associated with cutaneous vasculitis,
these disorders should prompt aggressive malignancy
glomerulonephritis, and circulating IgA immune
screening in this patient population as outcomes are complexes. Ann Rheum Dis 1990;49(8):638–40.
likely to be poor and treatment of secondary IgAV and 17. Pouria S, Feehally J. Glomerular IgA deposition in liver
IgAN differs from primary variants. disease. Nephrol Dial Transplant 1999;14(10):2279–
82.
18. Pouria S, Barratt J. Secondary IgA nephropathy.
REFERENCES Semin Nephrol 2008;28(1):27–37.
19. Zurada JM, Ward KM, Grossman ME. Henoch-
1. McGrogan A, Franssen CF, de Vries CS. The Schönlein purpura associated with malignancy
incidence of primary glomerulonephritis worldwide: in adults. J Am Acad Dermatol 2006;55(5
A systematic review of the literature. Nephrol Dial Suppl):S65–70.
Transplant 2011;26(2):414–30. 20. Audemard-Verger A, Terrier B, Dechartres A, et al.
2. Rodrigues JC, Haas M, Reich HN. IgA nephropathy. Characteristics and management of IgA vasculitis
Clin J Am Soc Nephrol 2017;12(4):677–86. (Henoch-Schönlein) in adults: Data from 260 patients
3. Wyatt RJ, Julian BA. IgA nephropathy. N Engl J Med included in a French multicenter retrospective survey.
2013;368(25):2402–14. Arthritis Rheumatol 2017;69(9):1862–70.
4. Radford MG Jr, Donadio JV Jr, Bergstralh EJ, Grande 21. Pertuiset E, Lioté F, Launay-Russ E, Kemiche F, Cerf-
JP. Predicting renal outcome in IgA nephropathy. J Payrastre I, Chesneau AM. Adult Henoch-Schönlein
Am Soc Nephrol 1997;8(2):199–207. purpura associated with malignancy. Semin Arthritis
5. Cattran DC, Coppo R, Cook HT. The Oxford Rheum 2000;29(6):360–7.
classification of IgA nephropathy: Rationale, 22. Heaf JG, Hansen A, Laier GH. Quantification of
clinicopathological correlations, and classification. cancer risk in glomerulonephritis. BMC Nephrol
Kidney Int 2009;76(5):534–45. 2018;19(1):27.
6. Moran SM, Reich HN. IgA vasculitis in adults. Curr 23. Bacchetta J, Juillard L, Cochat P, Droz JP.
Treat Options Rheumatol 2018;4(1):119–32. Paraneoplastic glomerular diseases and malignancies.
7. Hočevar A, Rotar Z, Jurčić V, et al. IgA vasculitis in Crit Rev Oncol Hematol 2009;70(1):39–58.
adults: The performance of the EULAR/PRINTO/ 24. Selewski DT, Ambruzs JM, Appel GB, et al. Clinical
PRES classification criteria in adults. Arthritis Res characteristics and treatment patterns of children
Ther 2016;18:58. and adults with IgA nephropathy or IgA vasculitis:
8. Yang YH, Yu HH, Chiang BL. The diagnosis and Findings from the CureGN study. Kidney Int Rep
classification of Henoch-Schönlein purpura: An 2018;3(6):1373–84.
updated review. Autoimmun Rev 2014;13(4–5):355– 25. Trimarchi H, Barratt J, Cattran DC, et al. Oxford
8. classification of IgA nephropathy 2016: An update
9. Davin JC, Ten Berge IJ, Weening JJ. What is from the IgA nephropathy classification working
the difference between IgA nephropathy and group. Kidney Int 2017;91(5):1014–21.
Henoch-Schönlein purpura nephritis? Kidney Int 26. Xu K, Zhang L, Ding J, et al. Value of the Oxford
2001;59(3):823–34. classification of IgA nephropathy in children with
10. Nicoara O, Twombley K. Immunoglobulin A Henoch-Schönlein purpura nephritis. J Nephrol
nephropathy and immunoglobulin A vasculitis. 2018;31(2):279–86.
Pediatr Clin North Am 2019;66(1):101–10. 27. Lee H, Yi SH, Seo MS, et al. Validation of the
11. Gardner-Medwin JM, Dolezalova P, Cummins C, Oxford classification of IgA nephropathy: A single-
Southwood TR. Incidence of Henoch-Schönlein center study in Korean adults. Korean J Intern Med
purpura, Kawasaki disease, and rare vasculitides 2012;27(3):293–300.
in children of different ethnic origins. Lancet 28. Knoop T, Vikse BE, Svarstad E, Leh S, Reisæter
2002;360(9341):1197–202. AV, Bjørneklett R. Mortality in patients with IgA
12. Piram M, Mahr A. Epidemiology of immunoglobulin nephropathy. Am J Kidney Dis 2013;62(5):883–90.
A vasculitis (Henoch-Schönlein): Current state of 29. Lien YH, Lai LW. Pathogenesis, diagnosis and
knowledge. Curr Opin Rheumatol 2013;25(2):171–8. management of paraneoplastic glomerulonephritis.
Nat Rev Nephrol 2011;7(2):85–95.
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101063Z01KB2019. Bartolomeo et al. 5
www.ijcasereportsandimages.com
30. Mimura I, Tojo A, Kinugasa S, Uozaki H, Fujita T. Renal purpura associated with malignancy. J Eur Acad
cell carcinoma in association with IgA nephropathy in Dermatol Venereol 2009;23(4):394–401.
the elderly. Am J Med Sci 2009;338(5):431–2. 48. Wong SF, Newland L, John T, White SC. Paraneoplastic
31. Fawole A, Daw H, Taylor H, Rashidi A. leukocytoclastic vasculitis as an initial presentation
Immunoglobulin A nephropathy associated with of malignant pleural mesothelioma: A case report. J
mesothelioma. WMJ 2012;111(1):29–32. Med Case Rep 2012;6:261.
32. Zhang XD, Yang SY, Li W, et al. Adult Henoch- 49. Ota S, Haruyama T, Ishihara M, et al. Paraneoplastic
Schönlein purpura associated with small cell lung IgA vasculitis in an adult with lung adenocarcinoma.
cancer: A case report and review of the literature. Intern Med 2018;57(9):1273–6.
Oncol Lett 2013;5(6):1927–30. 50. Joshi S, Pillai S, Chakera A, Lee YC. Henoch–
33. Cairns SA, Mallick NP, Lawler W, Williams G. Schonlein purpura in mesothelioma. Respirol Case
Squamous cell carcinoma of bronchus presenting Rep 2014;2(4):138–40.
with Henoch-Schönlein purpura. Br Med J 51. Houston KA, Henley SJ, Li J, White MC, Richards TB.
1978;2(6135):474–5. Patterns in lung cancer incidence rates and trends
34. Carcinoma of bronchus presenting with Henoch- by histologic type in the United States, 2004–2009.
Schönlein purpura. Br Med J 1978;2(6140):831. Lung Cancer 2014;86(1):22–8.
35. Mitchell DM, Hoffbrand BI. Relapse of Henoch- 52. Hong S, Ahn SM, Lim DH, et al. Late-onset IgA
Schönlein disease associated with lung carcinoma. J vasculitis in adult patients exhibits distinct clinical
R Soc Med 1979;72(8):614–5. characteristics and outcomes. Clin Exp Rheumatol
36. Ponge T, Boutoille D, Moreau A, et al. Systemic 2016;34(3 Suppl 97):S77–83.
vasculitis in a patient with small-cell neuroendocrine 53. Komatsu H, Fujimoto S, Maruyama S, et al. Distinct
bronchial cancer. Eur Respir J 1998;12(5):1228–9. characteristics and outcomes in elderly-onset
37. Weiler-Bisig D, Ettlin G, Brink T, Arnold W, IgA vasculitis (Henoch-Schönlein purpura) with
Glatz-Krieger K, Fischer A. Henoch-Schönlein nephritis: Nationwide cohort study of data from the
purpura associated with esophagus carcinoma Japan Renal Biopsy Registry (J-RBR). PLoS One
and adenocarcinoma of the lung. Clin Nephrol 2018;13(5):e0196955.
2005;63(4):302–4. 54. Opitz I, Friess M, Kestenholz P, et al. A new
38. Solans-Laqué R, Bosch-Gil JA, Pérez-Bocanegra C, prognostic score Supporting treatment allocation
Selva-O’Callaghan A, Simeón-Aznar CP, Vilardell- for multimodality therapy for malignant pleural
Tarres M. Paraneoplastic vasculitis in patients mesothelioma: A review of 12 years’ experience. J
with solid tumors: Report of 15 cases. J Rheumatol Thorac Oncol 2015;10(11):1634–41.
2008;35(2):294–304.
39. Mifune D, Watanabe S, Kondo R, et al. Henoch *********
Schönlein purpura associated with pulmonary
adenocarcinoma. J Med Case Rep 2011;5:226.
Author Contributions
40. Podjasek JO, Wetter DA, Pittelkow MR, Wada DA.
Henoch-Schönlein purpura associated with solid- Korey Bartolomeo – Design of the work, Drafting the
organ malignancies: Three case reports and a literature work, Final approval of the version to be published, Agree
review. Acta Derm Venereol 2012;92(4):388–92. to be accountable for all aspects of the work in ensuring
41. Blanco R, González-Gay MA, Ibáñez D, Alba C, Pérez that questions related to the accuracy or integrity of
de Llano LA. Henoch-Schönlein purpura as a clinical any part of the work are appropriately investigated and
presentation of small cell lung cancer. Clin Exp resolved
Rheumatol 1997;15(5):545–7.
Said Al Zein – Conception of the work, Drafting the work,
42. Angelier AS, Petit L, Wynckel A, et al. Schoenlein-
Henoch purpura as a presentation of squamous cell Final approval of the version to be published, Agree to be
bronchial carcinoma. [Article in French]. Rev Mal accountable for all aspects of the work in ensuring that
Respir 2011;28(3):372–6. questions related to the accuracy or integrity of any part
43. Fain O, Hamidou M, Cacoub P, et al. Vasculitides of the work are appropriately investigated and resolved
associated with malignancies: Analysis of sixty Joan Cullen – Acquisition of data, Drafting the work,
patients. Arthritis Rheum 2007;57(8):1473–80.
Final approval of the version to be published, Agree to be
44. Pfitzenmeyer P, Besancenot JF, Brichon P, González
G, André F. The association of bronchial carcinoma accountable for all aspects of the work in ensuring that
and rheumatoid purpura. [Article in French]. Ann questions related to the accuracy or integrity of any part
Med Interne (Paris) 1989;140(5):423–4. of the work are appropriately investigated and resolved
45. Gutiérrez Maciás A, Alonso Alonso J, Sanz C, Catherine Abendroth – Interpretation of data, Revising
Aguirre Errasti C. Schoenlein-Henoch purpura the work critically for important intellectual content,
and epidermoid carcinoma of the lung. [Article in
Final approval of the version to be published, Agree to be
Spanish]. Rev Clin Esp 1992;191(5):282–3.
accountable for all aspects of the work in ensuring that
46. Frigui M, Kechaou M, Ben Hmida M, et al. Adult
Schönlein-Henoch purpura associated with questions related to the accuracy or integrity of any part
epidermoid carcinoma of the lung. [Article in French]. of the work are appropriately investigated and resolved
Nephrol Ther 2009;5(3):201–4. Gurwant Kaur – Conception of the work, Design of
47. Mitsui H, Shibagaki N, Kawamura T, Matsue H, the work, Revising the work critically for important
Shimada S. A clinical study of Henoch-Schönlein
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Int J Case Rep Images 2019;10:101063Z01KB2019. Bartolomeo et al. 6
www.ijcasereportsandimages.com
intellectual content, Final approval of the version to be Conflict of Interest
published, Agree to be accountable for all aspects of the Authors declare no conflict of interest.
work in ensuring that questions related to the accuracy
or integrity of any part of the work are appropriately Data Availability
investigated and resolved All relevant data are within the paper and its Supporting
Information files.
Guarantor of Submission
The corresponding author is the guarantor of submission. Copyright
© 2019 Korey Bartolomeo et al. This article is distributed
Source of Support under the terms of Creative Commons Attribution
None. License which permits unrestricted use, distribution
and reproduction in any medium provided the original
Consent Statement author(s) and original publisher are properly credited.
Written informed consent was obtained from the patient Please see the copyright policy on the journal website for
for publication of this article. more information.
Access full text article on Access PDF of article on
other devices other devices
International Journal of Case Reports and Images, Vol. 10, 2019. ISSN: 0976-3198
Submit your manuscripts at www.edoriumjournals.com


You can also read

















































