POLYCYSTIC OVARIAN SYNDROME (PCOS) - Understanding and Managing - Elizabeth Howe Submitted for Completion of Ohlone Therapeutics Certificate ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Understanding and Managing
POLYCYSTIC OVARIAN SYNDROME (PCOS)
Elizabeth Howe
Submitted for Completion of Ohlone Therapeutics Certificate
2014-2015
June 17, 2015
1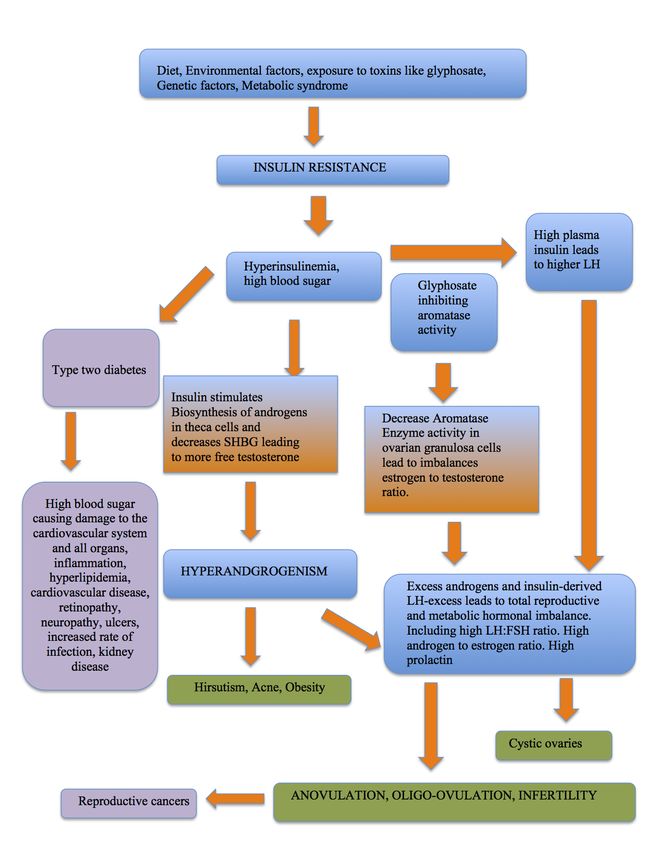
TABLE OF CONTENTS…………………………………………………………………2
INTRODUCTION:………………………………………………………………………..3
PART 1: UNDERSTANDING PCOS………………………………………………....…3
1.1 PATHOPHYSIOLOGY OF PCOS…………………………………………….…4
1.1.1 Insulin Resistance and Hyperandrogenism…………………………………….…8
1.1.2 Aromatase Enzyme…………………………………………………………….…9
1.1.3 Glyphosate and PCOS…………………………………………………………...10
1.2 SIGNS AND SYMPTOMS OF PCOS…………………………………………..12
1.2.1 Abnormal Menstrual Cycles and Infertility……………………………………...12
1.2.2 Hyperandrogenism and Hirsutism……………………………………………….15
1.2.3 Acne……………………………………………………………………………...15
1.2.4 Weight Gain and Central Obesity……………………………………………….16
1.2.5 Cystic Ovaries……………………………………………………………………16
1.2.6 Acanthosis Nigricans…………………………………………………………….17
PART 2: DIAGNOSING PCOS………………………………………………………...17
PART 3: CONDITIONS AND COMPLICATIONS ASSOCIATED WITH PCOS…..20
3.1 METABOLIC SYNDROME……………………………………………………20
3.1.1 Type 2 Diabetes…………………………………………………………………20
3.1.2 Cardiovascular Disease…………………………………………………………22
3.2 REPRODUCTIVE CANCERS………………………………………………....23
3.3 DEPRESSION AND ANXIETY……………………………………….………24
PART 4: MANAGING PCOS…………………………………………………………..24
4.1 DIETARY THERAPY…………………………………………………………..24
4.2 SUPPLAMENTS……………………………………………………………......30
4.3 EXERCISE………………………………………………………………………31
4.4 ALLOPATHIC MEDICINE…………………………………………………….32
4.4.1 Insulin-sensitizing Agents……………………………………………………….32
4.4.2 Fertility Treatments………………………………………………………….......33
4.4.3 Birth Control Pills……………………………………………………………….34
4.4.4 Acne Treatments…………………………………………………………………35
4.4.5 Ovarian Drilling………………………………………………………………….35
4.5 HERBAL PROTOCOL………………………………………………………….35
4.5.1 Goal Setting………………………………………………………………….......36
4.5.2 Sample Treatment Plan………………………………………………………….36
4.5.3 Other Herbs Useful in PCOS Management……………………………………..39
CONCLUSION…………………………………………………………………………40
REFERENCES:………………………………………………………………………..41
2INTRODUCTION
Polycystic Ovary Syndrome, more commonly referred to as PCOS, is an
endocrine, reproductive and metabolic disorder that is characterized by diverse clinical
symptoms including irregular menstrual cycles, infertility, hyperandrogenism with
subsequent hirsutism, insulin resistance (IR), acne, weight gain and cystic ovaries. PCOS
is the leading cause of infertility in women in the United States. In fact, between 2-18%
percent of women in North America have PCOS (Stansbury 2012, 11), and because so
many women with PCOS go undiagnosed, it’s hard to pin down a more precise
percentage. Not only can PCOS lead to infertility but, if left untreated, it can result in a
host of other serious health problems including type two diabetes, high blood pressure,
high cholesterol, thyroid disease, cardiovascular disease and an increased risk for
reproductive cancers. While there is not full consensus in the scientific community about
the exact cause or cure for PCOS, there are ways that women can manage the syndrome
so as to improve their health, reduce symptoms, boost fertility and increase the overall
quality of their life. The aim of this paper is to clearly explain the pathology and
physiological consequences of PCOS and discuss ways that women can use allopathic
medicine, herbal medicine, diet and lifestyle strategies to keep symptomology to a
minimum and improve health and vitality.
PART 1: UNDERSTANDING PCOS
PCOS has been described in medical literature for over two centuries. In 1845, a
French manuscript described sclerocystic ovaries. It was later coined “Bearded Ladies
Diabetes” as the correlation between excess androgens and diabetes was becoming
evident. In 1935, two doctors, Stein and Leventhal, described a syndrome associating
excessive male-patterned hair growth, obesity and menstrual cycle disturbance leading to
infertility (Thatcher 2000). This became known as Stein-Leventhal Syndrome. In the
years since, extensive research has looked into the causes of Stein-Leventhal Syndrome
and searched for ways to manage it. This syndrome is now referred to as PCOS. As you
will see in this section, PCOS is very complex in its origin, with a host of different signs
3and symptoms. However, understanding how PCOS manifests itself in a woman’s body
allows for accurate diagnosis and treatment.
1.1 PATHOPHYSIOLOGY OF PCOS
PCOS has a complicated, and not fully understood or scientifically agreed upon
pathophysiology. The disorder has very diverse and significant clinical implications for
women who suffer from it ranging from reproductive health, to endocrine and metabolic
abnormalities. Below is a flow chart that outlines some of the factors that contribute to
the pathophysiology of PCOS. Following the chart is an outline of how these processes
take place in the body. Keep in mind that no two people are the same and the reason one
woman has PCOS may be very different from the next.
4Figure 1: PCOS PATHOPHYSIOLOGY FLOW CHART
51.1.1 Insulin Resistance and Hyperandrogenism
Insulin is a hormone in the body that is secreted by the pancreas and is
responsible for getting glucose from the blood into the body’s cells. Insulin does this by
attaching to insulin receptors in the various cells throughout the body. Typically, when a
person eats and blood glucose rises, the pancreas excretes insulin to help this glucose
move from the blood stream into the body’s cells to be metabolized. The blood glucose
level then drops and the pancreas stops putting out more than the body’s basal insulin
requirement. When this feedback loop is functioning, blood glucose levels and insulin
levels should remain healthily normal. When the cells in the body are not utilizing the
insulin properly or resisting the insulin, glucose cannot get into the cells and we end up
with high blood sugar and high insulin to compensate, also called hyperinsulinemia
(Stansbury 2012). This leads to type 2 diabetes, which has it’s own cascade of health
problems that will be addressed later on.
As you can see in the chart above, Insulin resistance sets off a cascade of
imbalances in a woman as a reproductive and metabolic hormone that contributes to the
disordered state of PCOS. Between 40-80% of women with PCOS present Insulin
resistance (Thatcher 2000, 16). There are many reasons a woman may develop insulin
resistance. Most commonly, across all populations, diet is the biggest contributing factor
to the development of insulin resistance and type 2 diabetes. In these cases, people who
eat more sugars and simple carbohydrates than the body can handle develop insulin
resistance because the body is producing so much insulin in response to high sugar that
the body begins to view insulin as something that should not be received – thus making
their cells insulin resistant. However, in women with PCOS, there are much more
complicated metabolic and reproductive processes happening. Many women who have
PCOS show signs of a metabolic disorder pre-puberty and independent of diet. There are
also genetic abnormalities that play a role in the development of PCOS; we can see this in
the higher rates of PCOS among women in the same immediate family. In more recent
years, it is coming to light that environmental toxins and pollutants in our food system,
like glyphosate, play a role in the development of insulin resistance and PCOS (Samsel
and Seneff 2013). So, while it is important to know why a woman develops insulin
6resistance in the first place, it is equally important to understand how insulin resistance
contributes to imbalances that further exacerbate PCOS symptoms.
In women with PCOS, insulin resistance and compensatory
hyperinsulinemia may actually be the major underlying cause of the disease.
Hyperinsulinemia leads to an exaggerated effect of insulin in traditionally less responsive
tissues, including stimulating androgen secretion by the ovarian theca cells (Barbieri et.
Al 1986). Theca are endocrine cells that play many important roles in folliculogenesis,
which is the maturation of an ovarian follicle prior to ovulation. Theca are responsible for
producing androgen in the follicle as a precursor to estrogen, they help build structure for
growing ovarian follicles before ovulation and they provide a signaling pathway between
granulosa cells and oocytes (Young and McNeally 2010). If theca cells are overactive,
women experiences infertility due to excess androgens, if they are underactive women
experiences infertility due to lack of estrogen as a result of decreased provision of thecal
androgen for estrogen synthesis (Magoffin 2005). Typically, Theca cells are stimulated to
produce androgens by Luteinizing Hormone (LH). In women with PCOS, LH levels are
usually higher than normal and insulin is also producing stimulatory effect to produce
androgens – creating an abnormally high amount of androgens. In normal women, these
androgens are converted to estrogens in the granulosa cells in the follicle under the
influence of follicle stimulating hormone (FSH). In a study by Chen et al, it was found
that women with PCOS had higher levels of LH and lower levels of FSH than their non-
PCOS counterparts (2015). This high LH/FSH ratio creates a state of hyperandrogenism
leading to much of the PCOS symptomology. This will be discussed in the following
section on Aromatase activity.
The actual pathway in which insulin acts on the theca that stimulates androgen
production is not quite clear. Baillargeon et al., believe that, “that defective insulin-
mediated release of the d-chiro-inositol-containing inositolphosphoglycan (DCI-IPG)
mediator may contribute to the insulin resistance that characterizes obese PCOS women”
(2010). IPG’s are mediators in the insulin-signaling cascade for glucose uptake. DCI-IPG
has been shown to help activate the synthesis of glycogen in muscles and adipose tissue.
Women with PCOS have shown decreased insulin stimulated release of DCI-IPG. It is
unknown whether this is due to a lack of DCI or if something else is happening. It has
7been shown that using DCI supplements have greatly helped women with PCOS lower
insulin resistance and high blood glucose (Stansbury 2012).
Beyond this study, the relationship between insulin-resistance in women with
PCOS and hyperandrogenism is very clear as we can see based on the graph below. It has
also been shown that insulin resistance underlies the development of hyperandrogenism
in women with PCOS whereas insulin resistance does not create such androgen excess in
non-PCOS women with insulin resistance (DeUgarte 2004. Nestler et al. 1998). This
leads many researchers to believe that there is a genetic mutation in women with PCOS
where insulin can stimulate the ovaries to make androgens. Studies also show that
insulin-sensitizing agents, like Metformin, decrease circulating androgens – further
proving the correlation between insulin and hyperandrogenism (Diamanti-Kandarakis and
Dunaif 2012).
Figure 2: Influence of Insulin on Androgen production by Nester et al 1998.
8Beyond increasing circulating androgens, insulin decreases Serum hormone-
binding globulin (SHBG) in women with PCOS (Nestler 1997). SHBG is a protein that
responsible for binding free testosterone making it unavailable for use. Lower levels of
SHBG leads to higher levels of bioavailable testosterone in the blood and we see
hyperandrogenism. SHBG levels are also decreased by excess androgens and so, this
cycle plays out on itself over and over where androgens rise and SHBG decreases, only to
further perpetuate hyperandrogenism (Thatcher 2000).
There are also insulin receptors on the pituitary and here insulin modulates the
release of gonadotropins in the anterior pituitary, increasing the pulse frequency of
Luteinizing hormone, which stimulates androgen release. This further disrupts the
androgen to estrogen to progesterone and the LH:FSH feedback cycle, which contributes
to the irregular ovulatory cycles in women with PCOS and subsequent infertility.
1.1.2 Aromatase Enzyme
It has been reported that there is dysfunction of the aromatase enzyme in many
women with PCOS. The aromatase-P450 enzyme is responsible for converting androgens
(androstenedione and testosterone) into estrogens (estrone and estradiole) during
steroidogenesis (Nestler and Jakubowicz 1997). Aromatase can be found in many
estrogen producing tissues in the body including placenta, ovaries, testes, skin, bone,
adipose tissue, brain and vascular smooth muscle cells. However, for women of
reproductive age, the aromatase in ovarian granulosa cells and in luteinized granulosa
cells are of great importance. Androgens derived for steroidogenesis are produced in
theca cells and are transported to granulosa cells of growing follicles. Here, the
aromatase-P450 enzyme converts them to estradiol (E2) in the ovary. Typically this
conversion of androgens to estrogens functions in a hormone feedback loop creating a
balanced estrogen to testosterone ratio, where estrogen levels boost FSH and LH levels
and a normal menstrual cycle occurs. In women with PCOS, it appears that aromatase
activity is deficient and that excess androgens are not being converted into estrogens. In
fact, androgens inhibit aromatase activity. In PCOS, we see excess androgens, sometimes
excess estrogens, higher than normal luteinizing hormone levels and lower than normal
FSH levels. This aromatase dysfunction creates an imbalance in the estrogen to
9testosterone ratio, which further exacerbates menstrual cycle irregularities (Chen et al
2015). It was shown that a hyperestrogen state could increase aromatase activity.
Unfortunately, in many women with PCOS, the estrogen excess is overshadowed by
hyperandrogenism and aromatase activity is still inhibited.
The role of aromatase in PCOS goes beyond regulating menstrual cycles, it is also
responsible, in part, for regulating BMI. Estrogen has been proven to help lower BMI and
glucose levels as estrogen is negatively correlated with BMI (Barrera et al, 2014). Since
aromatase is responsible for converting androgens to estrogens and having a more
estrogens can help decrease BMI, aromatase activity is very important for women with
PCOS, who are, more often than not, obese.
It becomes clear that aromatase activity plays a vital role in the health of women
with PCOS in terms of their menstrual cycle, hyperandrogenism and BMI. So, while
there still needs to be more research into the role of the aromatase enzyme in PCOS, there
may be room to enhance aromatase activity as a strategy for treating PCOS women,
particularly those who are obese.
1.1.3 Glyphosate and PCOS
Glyphosate is the main active ingredient in the broad-spectrum herbicide
Roundup. Roundup is the most commonly used herbicide in the world with the United
States making up 25% of that usage (Duke and Powles 2008). Its use has only increased
in the last two decades with the introduction of its genetically modified counterparts,
“RoundUp Ready” crops. “RoundUp Ready” crops, manufactured by Monsanto, can
survive the application of RoundUp, while other weeds in the fields cannot. This allows
farmers to apply RoundUp across their entire fields, thus, introducing more Glyphosate
into our food and water supply and the environment. Glyphosate has also been used more
recently on wheat and sugar cane to ripen the crop before harvest – this introduces so
much more glyphosate onto the crops than was traditionally intended.
Glyphosate is considered by some to be non-toxic to humans because it works by
disrupting a metabolic pathway in plants not present in mammals (Herrmann and Weaver
1999). However, this pathway is present in mammalian gut bacteria and now we are
seeing correlation between glyphosate increase and increase in diseases that are
10influenced by disrupted gut bacteria. Recently, there have been many scientific studies
focusing on the connection between Glyphosate and chronic diseases that are on the rise
in the United States like Celiac Sprue, Autism, Cancer, Parkinson’s and reproductive
disorders like PCOS (Samsel and Seneff 2013b).
In the Case of PCOS, the connection to glyphosate may lie in the aromatase
enzyme. Glyphosate has been shown to affect many enzymes of the Cytochrome P450
family, including aromatase (Gasnier et al 2009). The enzymes in this family perform
many functions, which explains the assortment of diseases that glyphosate influences. In
one study, Glyphosate was shown to inhibit aromatase activity at levels 100 times lower
than the recommended use for agriculture – and these effects were seen in less than 18
hours (Moslemi et al 2005). Because we know that Aromatase is used in converting
androgens to estrogens and deficient aromatase activity inhibits this process, it becomes
clear that glyphosate’s disruption of aromatase plays a vital role in hyperandrogenism in
women with PCOS. While glyphosate may not be the only contributing factor to low
aromatase activity in PCOS women, it surely proves to be an endocrine disruptor that
should be avoided.
Glyphosate also has connection to insulin resistance. In short, long-term exposure
to glyphosate causes system wide depletion of sulfate. Sulfate is used in a chemical
process in the body, where part of the glucose that goes into the blood after a meal is
stored as heparin sulfate in the extracellular matrix in the body (Seneff et al., 2012).
Heparin sulfate breaks down after a few hours, providing a temporary buffer for our body
to more effectively pull glucose out of our blood serum. Depletion of sulfate inhibits this
process, impairs cellular glucose uptake and insulin resistance (Samsel and Seneff
2013a). This pulls us right back to insulin resistance being the underlying cause of PCOS
or at least aggravating the majority of symptoms associated with it.
Beyond insulin resistance, glyphosate depletes the plants treated with RoundUp
and the people who eat RoundUp exposed food of vital minerals and vitamins. These
include vitamin D3, Zinc, Iron, Manganese, Magnesium and so many more. All of these
vitamins and minerals are part of the treatment plan that is outlined later.
111.2 SIGNS AND SYMPTOMS OF PCOS
Beyond the pathology of PCOS, there are signs and symptoms that are very
common place in women with the disorder. While the pathology of PCOS is important,
and some of the factors outlined in the previous section can be apparent in blood test,
there are very clear clinical signs and symptoms that prove a woman has PCOS.
Symptoms like hirsutism, central obesity, abnormal menstrual cycles and infertility that
are most apparent and bothersome to women with PCOS. Below, these signs and
symptoms are outlined. Some of these symptoms contribute to the cyclic nature of the
disease state.
1.2.1 Abnormal Menstrual Cycle and Infertility
Many women first discover they have PCOS because they are having irregular or
absent menstrual cycles. In fact, 50-90% of women with PCOS show some abnormality
in their ovulation (Thatcher 2000, 16). Sometimes, PCOS will first become apparent
because a young woman will have her first period later than normal and then not have a
normal cycle again (Stansbury 2012). The absent or abnormal menstrual cycles are
caused by disrupted hormone feedback loop between the pituitary gland and the ovaries.
This disruption typically stems from the elevated presence of insulin and androgens in the
body. It should also be noted here that some women present many symptoms of PCOS
while still maintaining a somewhat normal menstrual cycle – this may be that a healthy
diet has kept them from slipping into a more progressed state of insulin resistance.
A normal menstrual cycle is under the control of many hormones. First GnRh, a
hormone messenger in our hypothalamus, is released. GnRh tells the pituitary gland to
release Luteinizing hormone (LH) and Follicle stimulating hormone (FSH). FSH and LH
enter the blood stream and are received by the ovaries. FSH and LH are used for the
development of the follicle and the production of estrogen, progesterone and inhibin –
which is meant to send a negative feedback to tell the pituitary gland to stop sending
FSH. As the follicles grow, they produces estrogen and as the estrogen rises in your body,
your womb is getting ready for a fertilized egg by building blood and nutrients. At about
day seven of the cycle there is a dominant follicle and all other follicles recede. The
dominant follicle is nourishing the egg inside it and also sends out a surge of estrogen to
12the pituitary gland. This estrogen triggers the pituitary to release more luteinizing
hormone, which triggers the follicle to finish growing and causing the egg to pop out of
the follicle and into the abdominal cavity. This is ovulation. Once the egg or oocyte is in
the cavity, the fallopian tube comes and sucks in the egg, using cilia and water muscle
contractions to move the egg into the uterus. Once in the uterus, if the egg isn’t fertilized
within 12-24 hours, it will dissolve and be shed along with the uterine lining. The follicle
that burst the egg out turns into a progesterone factory (this is called the corpus luteum)
and makes progesterone to support a pregnancy. If the egg isn’t fertilized, the
progesterone stops being produced and without the high levels of estrogen and
progesterone to support the lining of the uterus, it starts to break down and will
eventually shed from the body and the menstrual cycle starts all over. If the egg is
fertilized both progesterone and estrogen will rise back up to support the fetus and carry
it through to delivery.
In women with PCOS, this feedback loop that causes a woman to ovulate is
completely disrupted. It is very commonly seen in PCOS that LH hormone is higher
than average and FSH is lower than average. This alone does not allow for proper
hormone feedback between the ovaries and pituitary. High LH causes the ovarian
follicles to attempt to develop but without the FSH balance, the never fully mature. If a
follicle isn’t able to fully develop and ripen an egg, ovulation will not happen (Boss et al
2009). This presents itself as absent or very irregular menstrual cycles and subsequent
infertility.
Below are a couple of charts that compare the feedback loops between normally
ovulating women and women with PCOS. These charts are from:
(http://courses.washington.edu/conj/bess/reproductive/pcos.htm)
13Figure 3: Normal Hormone Feedback Loop
Figure 4: Hormone Feedback Loop in Women with PCOS
141.2.2 Hyperandrogenism and Hirsutism
Androgens are normally present in all people but normal levels vary between men
and women. Androgens are anabolic and promote the storing of nutrients and the build up
of tissue. In women, androgens are produced in the ovaries, adrenal glands and in fat
cells. Androgens play an important role in women’s health but, when they aren’t in
balance, they can cause central obesity, acne and hirsutism.
Hirsutism is male pattered hair growth. (Thatcher 2000). In women with PCOS
this most commonly causes thick, course hair growth on the face, chest and back and
sometimes hair loss and male-patterned badness. Hirsutism is the most common clinical
sign that a woman has hyperandrogenism. Hirsutism is influenced by excess circulating
androgens, by the increased number of androgen receptors in the body and by an altered
conversion of hormones by the hair follicle.
It is important to note that hyperandrogenism does not cause virilization.
Virilization causes deepening of the voice, enlarge clitoris, increased muscle mass and
rapidly developing male pattered baldness – if these symptoms are present, there could be
significantly more androgens than seen in PCOS and the patient should be tested for
ovarian and adrenal tumors (Roush 2010. p.8).
1.2.3 Acne
Acne forms when androgens increase sebum, which is the oily/waxy material that
keeps skin waterproof and moist. Sebum comes from the sebaceous glands that lie just
under the skin (Boss et al 2009). Excessive sebum can build up in the pores of the skin
and get clogged with dirt and bacteria, causing acne. Sometimes this acne is cystic and
deep under the skin, other times it will present as a white or blackheads (Roush 2009).
Women with PCOS often have very terrible acne that is painful and embarrassing,
especially during the sensitive teenage years. Very commonly, acne will remain with
these women into adulthood.
151.2.4 Weight Gain and Central Obesity
As I mentioned before, well over 50% of women with PCOS struggle with their
weight (Stansbury 2012). Often times, these women may exercise and eat just as well as
their friends without the disease and will weigh significantly more. The degree of obesity
in women with PCOS is directly correlated with androgen levels, insulin resistance and
faulty fat metabolism.
Insulin resistance may cause weight gain because the uptake of glucose into the
cells is inhibited. Because the body can only store so much glucose in the liver and
muscles (in the form of glycogen), the excess glucose is stored as body fat. This is the
process of putting on weight. In a study in 2004, it was found that in a group of women
with PCOS, the women who had insulin resistant has a much higher BMI than those with
PCOS who didn’t have insulin resistance (DeUgarte et al 2004). Also, it was found that
the degree of insulin resistance correlates with the degree of obesity – more obese
patients presented higher levels of insulin resistance.
Androgens cause central obesity – which is weight gained around the stomach
(Boss et al 2009). Elevated levels of androgens in the body promote the storage of sugar
and nutrients in the body tissue. This type of obesity carries a much higher risk for
cardiovascular disease. Often times weight gain caused by these hormone cycle
imbalances can further exacerbate the imbalance and weight loss can help bring
hormones into a more balanced place.
It appears also that women with PCOS do not metabolize fat as well. There are
hormones like Leptin and cytokines like adipokines that are responsible for directing the
metabolism of fat. These levels have found to be abnormal in women with PCOS
(Stansbury 2012). It is also believed that cortisol is released in response to inflammation
in the body and that this can cause weight gain. Because women with PCOS often have a
lot of inflammation –partially due to high blood glucose- inflammation induced cortisol is
an important factor to look at.
1.2.5 Cystic Ovaries
Cystic ovaries are found in 23% of women of childbearing age and so, while this
disease is named after this symptom, not all women with cystic ovaries have PCOS and
16not all women with PCOS have cystic ovaries (Roush 2010. 7). Cysts on the ovaries are
formed when an ovarian follicle begins to develop but due to improper hormone balance,
cannot develop fully; this leads to numerous immature follicles on the ovaries. These are
not technically cysts but have the same appearance. Having numerous immature follicles
on the ovaries often causes the ovaries to become enlarged. Typically these cysts are
benign and are not a cause for concern or the focus of treatment, unless one wants to get
pregnant – and then some western doctors may try to remove them.
1.2.6 Acanthosis Nigricans:
This is a skin disorder that causes patches of the skin to become dark, discolored,
thickened and even velvety (Boss et al 2009). These dark patches of skin are typically
seen around the neck but are also found in the groin and thighs. Acanthosis Nigricans is
associated with insulin resistance. This symptom will typically fade over time as PCOS is
managed properly (Roush 2009).
PART 2: DIAGNOSING PCOS
PCOS is so often undiagnosed in women because many of the symptoms associated with
PCOS are also symptoms of other diseases and disorders. Over the past two decades, as
research has increased on PCOS, different organizations and conventions have come up
with criteria for diagnosing PCOS. Below is a table made by the National Institute of
Health in 2012, which outlines the different criteria used for determining if a woman has
PCOS. (Table extracted from NIH 2012)
NIH 1990 Rotterdam 2003 AE-PCOS Society 2006
• Chronic anovulation • Oligo- and/or anovulation • Clinical and/or
biochemical signs of
• Clinical and/or • Clinical and/or hyperandrogenism
biochemical signs of biochemical signs of
hyperandrogenism hyperandrogenism • Ovarian dysfunction
(Oligo-anovulation and/or
(with exclusion of other • Polycystic ovaries polycystic ovarian
etiologies, e.g., congenital morphology)
adrenal hyperplasia) (Two of three criteria
needed) (Both criteria needed)
(Both criteria needed)
17As you can see, if a woman has ovarian dysfunction where they don't ovulate or
ovulate very irregularly (Oligo-ovulation – cycles longer than 36 days and less than 8
times a year) and they exhibit hyperandrogenism, they will most likely fall into the
criteria of having PCOS. Notice that having polycystic ovaries is not a main diagnostic
criterion despite the name of the disease. Using these criteria and common clinical
observations, it’s possible to diagnose by doing a physical exam of a woman and asking:
Does she show signs of hyperandrogenism like facial hair, central obesity and acne? Is
this happening in combination with an irregular menstrual cycle? This is where the power
of clinical diagnostics lies – by taking the time to observe and get to know the client
accurate diagnosis can be made, even in the absence of blood testing (Thatcher 2000).
Beyond these commonly used criteria for diagnosing PCOS, women can get a
series of blood tests that can provide more insight into hormone levels in the body and
also examine the progression of the disease – particularly in regard to Insulin resistance,
diabetes and heart disease. None of these tests will determine 100% that a person has
PCOS, they may be used just for further investigation.
Test What the test shows
Testosterone – These tests can check for elevated androgen levels and rule out the
total and free possibility of androgen producing tumor.
Luteinizing Higher ratio of LH/FSH can be indicative of PCOS, though some
Hormone/Follicle women have normal LH levels.
stimulating
hormone
SHBG Tests ability to bind testosterone. Low SHBG may indicate PCOS
and insulin resistance.
Prolactin Prolactin is a hormone secreted by the pituitary that stimulates
lactation. High prolactin can suppress periods. Women with PCOS
often have high prolactin. Persistently high prolactin can also be
caused by pituitary tumor, so it’s good to check this out.
18Thyroid Many women with PCOS have low thyroid function and TSH is a
Stimulating common way to measure thyroid function. High TSH may be
Hormone indicative of hypothyroid, which can be responsible for weight gain
and abnormal menstrual cycles. If tests results for TSH are abnormal,
further thyroid testing can be performed to rule out thyroid disease.
Fasting Insulin This will test insulin in the blood after fasting and can indicate
hyperinsulinemia.
Fasting Blood This test measures glucose in the blood after 8 hours of not eating. It
Sugar is taken first thing in the morning and can be used to evaluate insulin
resistance or glucose intolerance
Glucose If you have abnormal fasting blood sugar, the glucose tolerance test
Tolerance Test can determine how your body utilizes sugar over time. If sugar is
found in the urine during this test, there is evidence of insulin
resistance, diabetes, kidney failure or Cushing’s syndrome.
Lipid Profile This tests looks at cholesterol in the blood. Elevated androgens in
PCOS may cause abnormal lipid levels and put a person at risk for
cardiovascular disease.
Pelvic This will check to see if there are cysts on the ovaries or if the ovaries
Ultrasound are enlarged – which is a sign of PCOS. This can also show the status
of the endometrial lining, which may be thickened if a woman isn’t
having regular periods.
Chart references: (Roush 2010; Thatcher 2010)
As you can see, there are many lab tests that may be performed and while they are
not necessary to diagnose PCOS, they may provide peace of mind to the client in their
diagnosis and rule out other diseases. These tests are useful in examining the state of the
body and help as a way target diet and treatment plans accordingly, particularly if a
person is experiencing pre- or full blown diabetes and cardiovascular disease. These
secondary conditions associated with PCOS will be examined in the following section.
19PART 3: CONDITIONS AND COMPLICATIONS ASSOCIATED WITH PCOS
Beyond the troubling causes and symptoms present in PCOS, there are conditions
and complications that can be aggravated by the disorder. The two most important and
frequent are Type Two diabetes and Cardiovascular disease – both of which are linked to
metabolic syndrome and can be seen in women without PCOS who have a poor diet and
unhealthy lifestyle. There is also an increased risk of reproductive cancers, which are
linked to hormone imbalance, and an increased incidence of depression and anxiety.
3.1 METABOLIC SYNDROME
Metabolic syndrome is seen in about 40% of women with PCOS (Roush 2010)
and may present itself in early childhood, prior to the discovery of PCOS. Metabolic
syndrome is a group of metabolic disturbances that cause high blood pressure, high blood
sugar, high bad cholesterol and obesity. These four consequences of metabolic syndrome
are called the Deadly Quartet (Stansbury 2012). Metabolic syndrome really centers
around insulin resistance and the effect of insulin resistance and high blood sugar and
lipids on the blood vessels, tissues and organs of the body (Grundy et al. 2005).
3.1.1 Type 2 Diabetes
Insulin resistance and hyperinsulinemia play a profound role in the onset and
progression of PCOS. The consequence of high insulin resistance and subsequent
hyperinsulinemia is the development of Type 2 diabetes mellitus more commonly
referred to as adult onset diabetes. Diabetes is diagnosed by testing positive for elevated
blood glucose levels. Roughly 15-20% of women with PCOS will develop diabetes
(Stansbury 2012). Diabetes occurs when severe insulin resistance in the body develops
overtime, causing blood glucose to remain in the blood rather than being absorbed into
the cells to be used for energy. There are many health complications associated with
diabetes as high sugar and fats in the blood can damage cells, nerves, tissues and organs
as the disease progresses (Thatcher 2000).
Having the excess blood fats and sugars that come with diabetes can lead to
inflammation and oxidizing processes throughout the circulatory system. Inflammation
20and oxidation can damage the blood vessels causing them to become less elastic, which
can cause blood pressure to increase and lead to increased risk of heart attack, stroke and
other vascular diseases (NIDDK 2013). This is addressed in the following section.
Diabetes can cause increased risk of infections because the high sugar in the body
creates an environment that is hospitable to bacteria, viruses and fungi. We see that these
infections may be frequent colds or flus or they can be bladder and skin infections. There
may also be chronic candida issues in diabetic people or the fungus may be on the skin
(Stansbury 2012).
Diabetes can also lead to retinopathy, where the retina is damaged due to fats and
sugars in the blood that get into the tiny vessels that service the retina. If diabetes is left
untreated, this can lead to blindness. Typically, treatment for this retinopathy is based on
protecting the tiny blood vessels that service the eyes using things like ginkgo, garlic and
blueberries (NEI 2012).
10-40% of people with type two diabetes will acquire kidney disease due to the
damage sugar causes to the tiny blood vessels and nephrons in the organ (National
Kidney Foundation 2015). Many diabetics who have kidney disease will develop kidney
failure and have to go on dialysis to have their blood cleaned since the kidneys are no
longer functional. Kidney failure is a disorder that eventually is fatal.
Diabetics often lose parts of their extremities due to non-healing ulcers, this
process is called cutaneous ulceration. This happens when the tiny blood vessels that
support microcirculation are damaged and oxygen isn’t getting to the extremities. Often
times, where blood vessels are damaged, a wound will develop and it will not heal. These
can eventually get infected and gangrene and amputation may be necessary (American
Diabetes Association 2014).
About 50% of people with diabetes will also develop neuropathy or peripheral
tingling and numbness. This is a sign of nerve damage and can be aggravating to painful
but can also cause people with diabetes to not feel nerve sensations that they need to in
order to remain healthy (Stansbury 2012). For example, if you can’t feel your foot, you
might injure it and not know and develop and ulcer that won’t heal. In a more extreme
case, you might not feel heart pain that is indicating a heart attack. There are medications
to treat neuropathy but some have significant side effects.
21The extent to which diabetes affects the entire body and all of its organs is mind-
boggling. It is very important to take control of diabetes development as early as possible
to avoid as much damage as possible.
3.1.2 Cardiovascular disease
As you can see from above, diabetes greatly increases the risk of cardiovascular
diseases. If fact, people with type two diabetes are at a 100 to 200 percent greater risk of
dying from cardiovascular disease than those with out diabetes (Feinberg 2004). People
with diabetes are at risk for two major types of cardiovascular disease; first, coronary
artery disease and secondly, cerebral vascular disease. People with diabetes are also at
risk for heart failure and peripheral arterial diseases (NIDDK 2013).
Coronary artery disease is causes by thickening and hardening of the walls of the
blood vessels that run to and from your heart. When these vessels get narrowed and
blocked by fatty plaque deposits, blood flow to the heart is reduced or eliminated and will
result in a heart attack.
Cerebral vascular disease is when blood to the brain is cut off. This usually
happens when a blood vessel in the neck is narrowed or blocked due to hardening of the
blood vessels to the brain. This can result in a stroke.
Both coronary artery disease and cerebral vascular disease are seen in
people with metabolic syndrome and type-two diabetes due to the damaged caused by
high sugar and bad fats in the blood, which damage the blood vessels, causing them to
harden. Narrowed, inelastic blood vessels cause blood pressure to rise and further damage
the vessels and increase risk of a devastating heart attack or stroke.
Diabetes can cause heart failure because high blood glucose can damage the heart
muscle itself (cardiomyopathy), causing the heart muscle to be less effective. Heart
failure is not as immediate of a disease as it sounds, rather it is the progressive worsening
of the hearts ability to pump blood properly. Heart failure develops slowly and gets worse
over time. Typically, a person with heart failure will have fluid build up in the extremities
and sometimes the lungs because the heart is having trouble pumping fluids back up from
the extremities resulting in edema. Heart failure is typically treated with diuretics as a
way to get fluid out of the system – it by no way treats the heart disease itself. Besides
22edema, other symptoms of heart failure include shortness of breath, extreme fatigue, and
weakness. Edema caused by heart failure can create and exacerbate cutaneous ulceration
because the skin becomes thin and damp and infection is more prone to happen (NIDDK
2013).
Peripheral arterial disease was discussed in the previous section in regards to poor
circulation in the legs and feet, which lead to amputations.
3.2 REPRODUCTIVE CANCERS
The long-term hormonal imbalances and excessive stimulation of hormonal
tissues seen in women with PCOS greatly increases the risk of developing reproductive
cancers. Women with PCOS are two to three times more likely to develop ovarian and
endometrial cancers than those without (Stansbury 2012). As an example, women with
PCOS who never or rarely have a menstrual flow are in a constant exposure to estrogen
and have a thickening of the endometrial lining because isn’t shed regularly. This
thickening is called endometrial hyperplasia and over time, cells in the lining can change
and become abnormal and even cancerous. The fewer periods a woman has, the higher
risk she is for endometrial hyperplasia (Roush 2010). This really emphasizes the
importance of balancing hormones to bring on a more normal menstrual flow as a means
of reducing cancer risk.
3.3 DEPRESSION AND ANXIETY
As you can imagine, having PCOS and all that goes along with it can be very
stressful, upsetting and possibly depressing to those who suffer from it. Having to face
the often judgmental world as a person who, often at no fault of their own, is obese with
acne and facial hair may be very difficult. Beyond one’s outward appearance, infertility
for women who desire to have children is upsetting to say the least. In this sense, it
becomes important to educate and empower women to take charge of their own health.
To some, this may involve taking anti-depressants or anti-anxiety medication, while for
others in may mean working with herbs to boost one’s mood or working with a therapist
23or other healer (Roush 2010). This is really case-by-case and may not hold true for all
women with PCOS but it is a very important factor to consider.
PART 4: MANAGING PCOS
As you can see, PCOS is a very complex disorder involving many processes and
imbalances. The good news is that regardless of how PCOS manifests itself in a woman,
treatment options are available and can be somewhat universal across PCOS phenotypes.
Diet and exercise as a means to lose weight and decrease blood sugar and fasting insulin
is the most straightforward way to bring hormones into balance and hopefully restore a
more normal menstrual cycle. There are however supplements, allopathic and herbal
medicines that are used to treat symptoms of PCOS. Listed below are management
strategies for PCOS with the hope that symptoms/complications such as infertility,
diabetes, obesity, cardiovascular disease and other hindrances can be mitigated.
4.1 DIETARY THERAPY
For women with PCOS, it is very important to restore balance across all metabolic
and reproductive functions. Dietary changes are the most effective strategy in restoring
this balance because it can greatly reduce fasting insulin – which is the most significant
contributor to the severity of the disease (Douglas et al 2006). It has been shown that a
woman with PCOS can lose just 5-10% of body mass and increase fertility, reestablish
menstrual cycles, and begin to bring hormonal and metabolic processes into a more
normal rhythm (Thatcher 2000). Dietary therapy for women with PCOS focuses on
eliminating foods that increase blood glucose and bringing in foods that help stabilize
blood sugar, help with insulin resistance and provide therapeutic effects. In the following
dietary plan, in addition to changing food choices, women should eat more small meals
throughout the day as opposed to few larger meals. This helps balance blood sugar,
letting your body metabolize sugar and carbohydrates more efficiently.
24Below are a couple of charts outlining dietary changes for managing PCOS. This is
based off of Jillian Stansbury, ND protocol (2012).
A Healthy diet for Why? How?
women with PCOS
should include:
Complex carbohydrates are carbohydrates that take longer to
break down into sugar and occur naturally in whole fruits,
vegetables, legumes and grains. Of these complex carbs, whole
High Complex grains provide fiber and B-vitamins, Vitamin E and trace
carbohydrate Foods minerals. Fruits provide fiber, antioxidants, and nutrients,
simple and complex sugars. Legumes are high in protein, fiber,
macronutrients and pinitol. Pinitol helps with insulin
resistance. Eating complex carbohydrates provides the body an
array of vitamins, minerals and other nutrients to help meet
dietary needs.
Foods low on the The glycemic index is a measure of how fast the body will
glycemic index break foods down into sugars. Foods higher on the glycemic
index will cause blood sugar spikes. However, foods should
not be chosen based on glycemic index alone, as sometimes it
could be deceiving.
Whole foods are unprocessed foods and eating them keeps
people from filling up on junk, processed foods. Whole foods
contain all of the fiber, fats, vitamins and minerals together in
Whole Foods one balance package. Whole foods include whole grains (not
whole grain bread), fruits, vegetables, meats, fish, seaweeds
and spices. 75% of the diet should be whole foods. Good
whole grains to eat include quinoa, barley, amaranth, brown
rice, corn, whole wheat, rye, wild rice and buckwheat. When
these grains are used, its important to get grains fresh and if
they are milled to keep them refrigerated.
25Eating fiber helps slow the release of sugar into the blood
stream, which helps balance blood sugar. For example, if you
have apple juice, the fiber is extracted and blood sugar may
High-fiber foods spike, but if you eat a whole apple, the sugar spike will be
slower and lower. In addition to fiber occurring naturally in
foods, you can get fiber from freshly ground flax seed,
psyllium husk and chia seeds.
Proteins are very important in the PCOS diet. They do not
cause a spike in blood sugar and help keep one satiated for
longer, reducing snacking. It’s good to eat protein with every
High-protein foods meal on this plan. When selecting protein, its good to eat lean
meats and to prepare meat in a way that doesn’t make the fat
become rancid – as can happen when frying meats. Poached
fish and eggs contain a lot of great nutrients and fats in
addition to protein. Legumes, as mentioned above are a great
source of protein and can easily be added to many meals.
Fatty acids have been shown to prevent some diseases and are
important for a variety of metabolic functions throughout the
body. There are two types of unsaturated fatty acids that are
good to add into the diet. First, monounsaturated fatty acid,
which can raise HLD – good cholesterol. These fats have
Foods high in essential shown to increase insulin sensitivity. Monounsaturated fatty
fatty acids acids are found in olive and canola oil, avocados, cashew,
peanuts and sesame seeds. Polyunsaturated fatty acids include
omega 3 and omega 6 essential fatty acids. These are
considered essential because our body cannot synthesize these
on our own but they are important for metabolic functions.
Omega-3’s are broken down into three categories: alpha-
linoleic acid (ALA), eicosapentanoic acid (EPA) and
26docosahexaenoic acid (DHA). ALA is found in plants like flax
seeds, canola, walnuts, and chia seeds. EPA is found to reduce
risk of heart disease and is found most commonly in fatty,
cold-water fish like salmon, trout, tuna, sardines, mackerel and
can often be taken in fish oil capsules. DHA is the most
commonly found fatty acid used in the brain and can be found
in fatty fish like the ones listed above.
Omega 3’s have been shown to prevent neurological
degeneration like Alzheimer’s, Parkinson’s and has even been
sued to treat mental disorder like ADHD and bipolar disorder.
Making sure you get good quality omega 3’s into the diet it
very important.
Omega 6 fatty acids are precursors to inflammation and need
to be balanced by omega-3’s. This balance is often disrupted
because omega 6’s are very commonly used in processed foods
in the form of corn, canola and soy oils. One omega-6, linoleic
acid is important in the prevention of heart disease and can be
found in olive, sesame, sunflower and walnut oil and in many
nuts. It can also be found in borage oil, evening primrose oil,
and currant oil.
It is good to incorporate GOOD QUALITY oils into the diet in
order to get the benefits. Oils should be cold-pressed, raw, and
not heat-treated to avoid rancidity.
There are certain foods that work really well on bringing a
person with PCOS back into metabolic and hormonal balance.
These foods include flaxseed (which should be ground just
prior to using to avoid rancidity). Flax seeds can replace some
27amount of flour and eggs in baking. Legumes are a super food
Therapeutic/super for PCOS because they contain high amounts of pinitol and D-
foods chiro-inositol, which help with insulin resistance and hormone
balance. Sprouted grains are great for this dietary protocol as
they make amino acids more bioavailable to the body. They
also contain higher levels of vitamins and minerals include the
b-complex.
Maca powder can be used to lower blood sugar and balance
hormones. It can be added to many foods and smoothies. Nuts
are also a super food for PCOS, they are good sources of
protein and nutrients for snacking, baking or for making nut
milks with.
Foods that should be Why? How?
avoided in PCOS:
Refined carbohydrates Refined carbohydrates, unlike complex carbohydrates
provide high amounts of sugar without the fiber and
vitamins and minerals. Typically these will cause blood
sugar spikes and exacerbates insulin sensitivity.
Processed foods contain poor quality fats, sugars and
Highly Processed Foods many artificial colors and flavors that are not good for
anyone.
Include hydrogenated vegetable oils, commonly found
in processed foods and in margarine. These fats are
Trans fats manufactured and raise LDL and lower HDL. This
increases inflammation and risk of cardiovascular
disease.
Avoiding produce that is not grown organically, if
28possible, is really the best choice. Conventional produce
may have pesticide residues, including the terrible
Non-organic produce and glyphosate. Organic fruits have shown to have more
meats that might have nutrients in them as well. Meats that are not raised
glyphosate on them. organically may also have high levels of glyphosate
residues in them due to their commonly used round up
ready feed. Non-organic meats are also treated with
antibiotics and lots of growth hormones, which for many
reasons is not wise to ingest.
While the guidelines listed above are fairly simple, it is much harder to actually
commit to a dietary plan in practice. However, because changing diet in PCOS can have
such effective results in easing symptoms, helping with weight loss, and decreasing risk
of severe complications like diabetes and cancer, there is great incentive to stick with the
plan.
One way to help follow these guidelines is to do some meal planning – there are
still so many ingredients that you can cook with. It’s helpful to plan out meals and make
sure all of the ingredients are at home and ready to be used. This will eliminate the need
to go out and grab a quick, unhealthy snack elsewhere. Overtime, the sugar cravings will
subside, as will the symptoms of PCOS.
4.2 SUPPLAMENTS
Vitamin D: Vitamin D is a vitamin our body makes from sunshine. People are becoming
more deficient in Vitamin D they use sunblock and spend less time outside and therefore
it is important for most people to supplement vitamin D using food sources or capsules.
Vitamin D deficiency is linked to insulin resistance and diabetes. Vitamin D helps
Support the absorption of calcium and phosphorus and is an immunomodulator (Thatcher
2000). Vitamin D helps increase insulin sensitivity and blood sugar metabolism – making
29You can also read