Prevalence and correlates of anxiety and depression in frontline healthcare workers treating people with COVID-19 in Bangladesh - BMC Psychiatry
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Tasnim et al. BMC Psychiatry (2021) 21:271
https://doi.org/10.1186/s12888-021-03243-w
RESEARCH Open Access
Prevalence and correlates of anxiety and
depression in frontline healthcare workers
treating people with COVID-19 in
Bangladesh
Rafia Tasnim1,2† , Md. Safaet Hossain Sujan1,2† , Md. Saiful Islam1,2*† , Asmaul Husna Ritu1 ,
Md. Abid Bin Siddique1 , Tanziha Yeasmin Toma1 , Rifat Nowshin1 , Abid Hasan3 , Sahadat Hossain1 ,
Shamsun Nahar4 , Salequl Islam4 , Muhammad Sougatul Islam5 , Marc N. Potenza6,7,8,9 and Jim van Os10,11
Abstract
Background: Healthcare workers (HCWs) who are in the frontline during the COVID-19 pandemic are often under
significant pressures that may predispose them to symptoms of poor mental health. This study aimed to investigate
the prevalence of anxiety and depression among HCWs and factors correlated with mental health concerns during
the COVID-19 pandemic in Bangladesh. And, it also aimed to evaluate the psychometric properties of the Bangla
version of the Hospital Anxiety and Depression Scale (HADS).
Methods: A cross-sectional survey was conducted between July and August, 2020. A self-reported online
questionnaire was utilized to collect data. The survey included questions concerning socio-demographic, lifestyle,
and work setting, as well as the HADS. A confirmatory factor analysis (CFA) and multiple linear regression analysis
were performed.
Results: Data from 803 HCWs (50.7% male; mean age: 27.3 [SD = 6.9]; age range: 18-58 years) were included in the
final analysis. The Bangla HADS was psychometrically sound, and demonstrated good internal consistency and
reliability (α = 0.83), and excellent construct validity. Prevalence estimates of anxiety and depression were 69.5%,
and 39.5%, respectively, for less severe symptomology (at least borderline abnormal), and 41.2% and 15.7% for more
severe (at least abnormal) symptomology. Regression analyses with the total HADS score as a dependent variable
revealed significant (p < 0.05) associations with female gender, moderate and poor health status, infrequent
physical exercising, smoking, having had regrets about one’s profession because of the pandemic and associated
experiences, not updating on the latest COVID-19-related research, experiencing discrimination in the workplace,
and facing social problems due to working in a lab or hospital during the COVID-19 pandemic.
(Continued on next page)
* Correspondence: islam.msaiful@outlook.com
†
Rafia Tasnim, Md. Safaet Hossain Sujan, and Md. Saiful Islam contributed
equally to this work.
1
Department of Public Health and Informatics, Jahangirnagar University,
Savar, Dhaka 1342, Bangladesh
2
Centre for Advanced Research Excellence in Public Health, Savar, Dhaka
1342, Bangladesh
Full list of author information is available at the end of the article
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,
which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if
changes were made. The images or other third party material in this article are included in the article's Creative Commons
licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain
permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the
data made available in this article, unless otherwise stated in a credit line to the data.Tasnim et al. BMC Psychiatry (2021) 21:271 Page 2 of 14 (Continued from previous page) Conclusions: Symptoms of anxiety and depression are prevalent among HCWs during the COVID-19 pandemic in Bangladesh. The findings suggest a need for screening for mental health concerns, and employing early intervention to help these individuals. Keywords: Anxiety, Depression, Healthcare workers, COVID-19, Bangladesh Background who had experienced quarantines or served in wards The emergence of a novel coronavirus, severe acute re- treating infected patients were two- or three-fold more spiratory syndrome coronavirus-2 (SARS CoV-2), which likely to experience PTSD [18]. causes coronavirus disease 2019 (COVID-19), has sub- Timely interventions are important for improving the stantially impacted healthcare systems globally. The mental resilience of HCWs and optimizing function of COVID-19 pandemic has generated a public health crisis healthcare systems [19]. Effective communication, re- worldwide [1]. The World Health Organization (WHO) striction of shift hours, provision of rest areas and broad declared it an international public health emergency [2]. access to them, availability and appropriate management According to the WHO, there have been over 31.1 mil- of PPE, and advanced training on COVID-19 may lion confirmed cases of COVID-19, including 962,008 minimize HCWs’ anxiety [20]. deaths as of September 22, 2020 [3]. Globally, there have Bangladesh, where the present study was conducted, is been more deaths from COVID-19 than from severe a South Asian country whose healthcare system has been acute respiratory syndrome (SARS) and Middle East re- considerably impacted by COVID-19. Bangladesh has spiratory syndrome (MERS) combined, although there experienced numerous COVID-19 patients, lack of pre- has been a relatively lower death rate for COVID-19 paredness, and shortages of hospital beds and other among people infected with SARS CoV-2 [4]. Currently, items relevant to COVID-19 patient care. In Bangladesh, no fully effective treatment has been developed for treat- the virus was first reported on March 8, 2020 [21–23]. ing patients with COVID-19 [5]. This global pandemic Since then, the virus quickly spread and there have now poses a huge challenge for local healthcare services. As been more than 352,178 cases and 5,007 deaths at the the number of patients with COVID-19 increases, health time of writing (September 22, 2020) [24]. According to resources, including inpatient or intensive care beds, recent reports of the Bangladesh Medical Association, ventilators, medications, and personal protective equip- there were 8,125 infected cases of HCWs including doc- ment (PPE), have at times been limited. With fewer re- tors, nurses, and other staff with 117 fatalities (115 phy- sources, health care workers (HCWs) may experience sicians and 2 dental surgeons) [25, 26]. Moreover, there considerable pressure and anxiety [1, 6]. is also an acute shortage of medical practitioners, includ- Frontline HCWs during the COVID-19 pandemic may ing physicians, nurses and medical personnel in this be at considerable risk of developing mental problems country. Bangladesh has 0.79 hospital bed per 10,000 [7, 8], as HCWs were during SARS or Ebola outbreaks population, while China has 4.31, and the USA has 2.87 [9]. Frontline HCWs directly involved in diagnosing and beds per 1,000 people [27]. Moreover, the government treating COVID-19 patients may experience mental dis- health department of Bangladesh has only 432 ICU beds tress and other mental health concerns [7, 10]. The large in total (total population 170 million), only 110 of which number of confirmed and suspected cases, dispropor- are placed outside the capital city, Dhaka. The private tionate workloads, shortages of PPE and medications, healthcare sector has an additional 737 ICU beds [28, extensive media attention, and feelings of insufficient as- 29]. The Bangladesh government has published an act sistance may predispose to emotional strain in HCWs describing the rules of infectious disease management [10–12]. Prior studies have reported that HCWs feared and the allocation of staff; it declared an emergency re- for contagion and contamination of their family, friends, sponse committee to monitor the spread of the infection and colleagues [13], felt insecurity and shame, reported [30]. The number of HCWs is insufficient as the number unwillingness to work or contemplate resignation [14], of positive patients has been rising rapidly, overwhelm- and frequently reported stress, anxiety, and depression ing HCWs who are in contact with these positive pa- [15, 16]. Thus, understanding shorter- and longer-term tients. To reduce the transmission, the government mental impacts on HCWs is important. published a plan, identifying six basic country-wide re- During the SARS epidemic, 29%-35% of HCWs experi- sponse measures. The government also implemented a enced considerable distress [17]. Several years after the plan to form a 500-person local response committee outbreak, 10% of healthcare staff reported symptoms of covering the country along with the national Rapid Re- post-traumatic stress disorder (PTSD) [18]. Individuals sponse Committee (RRC) and the Rapid Response Team
Tasnim et al. BMC Psychiatry (2021) 21:271 Page 3 of 14
(RRT). Additionally, 500 hospital beds were prepared for educators) are those who had direct interaction with
the treatment of COVID patients [31]. Hence, the gov- COVID-19 patients, and whose role formed part of the
ernment of Bangladesh took important steps, and ap- national plan to alleviate the spread of COVID-19. Lab
plied these at a national level for the prevention of workers were those people who are working in the lab
transmission of the virus [32], although there exist vari- to identify individuals' COVID-19 status (positive/nega-
ous macro or microsystemic reasons for why the WHO tive). Other caregivers included pharmacologists, micro-
recommendations sometimes cannot be fully followed biologists, virologists, and biotechnologists. All
[33]. participants (HCWs) had full to limited, but at least
During the pandemic, HCWs have been experiencing some, direct interaction with COVID-19 patients in their
heavy workloads and shortages of PPE, and these and workplace. Data were collected between July and August,
other factors may increase anxiety [6, 34]. Shortcomings 2020, using a self-reported online survey. After adminis-
in COVID-19 testing facilities may worsen the situation tering all survey questions in Google Forms, a shareable
[35]. There is no specific working schedule for HCWs link was generated. This link was then shared in differ-
and sometimes they are required to work up to 17 hours ent online platforms involving HCWs to collect data effi-
per day [36]. In this study, respondents (HCWs) com- ciently in the setting of lockdown and spatial distancing
pleted the questionnaire after at least several months of measures. Individuals provided informed consent prior
frontline exposure during the pandemic. to participating in the study. Approximately 8-10 mi-
The impact of COVID-19 may be influenced signifi- nutes were required to complete the entire question-
cantly by psychosocial and cultural contexts. While dif- naire. The inclusion criteria included (i) 18 years or
ferential impact of COVID in higher-income and lower- older; and (ii) completing the entire questionnaire. Ini-
income countries have been hypothesized, few studies tially, 825 respondents participated. Ultimately, 803 sur-
have investigated COVID-19-related phenomena in veys (50.7% males; mean age: 27.3 years [SD = 6.9]; age
lower-income countries. It is therefore important to range: 18-58 years) were included in final analysis after
gather COVID-19-related data in countries with limited removing incomplete surveys.
resources like Bangladesh in order to understand mental
health concerns and related factors. It is particularly im- Measures
portant to understand these concerns in HCWs in A self-reported survey questionnaire assessed variables
under-resourced countries as changes in mental health related to socio-demographics, lifestyle, work environ-
often have long-term consequences, potentially further- ment, anxiety, and depression. Variables selection was
ing the impact of COVID-19 on HCWs after the pan- guided by previous epidemiological literature on anxiety
demic subsides. In addition, mental health impacts on and depression in Bangladesh [37–40].
HCWs due to the COVID-19 have been poorly studied
in Asian jurisdictions and lower-income countries like Socio-demographic and lifestyle measures
Bangladesh. We hypothesized that many HCWs would Socio-demographic information included gender, age,
report anxiety and depression and, as in prior outbreaks, marital status, occupation, and residence location
anxiety and depression would be associated with virus- (urban/rural). Self-reported health status (good, moder-
related experiences and exposures. ate, and poor) and chronic diseases (e.g., high blood
pressure, heart problems, diabetes, respiratory problems;
Study objectives yes/no) were also assessed. Numbers of average sleep
The study objectives were to investigate mental health hours, physical exercising (yes/no), and current smoking
among Bangladeshi HCWs treating COVID-19 patients (yes/no) were assessed. Sleeping status, conforming to
by assessing severity of depression and anxiety; to assess methodology in previous works in the Bangladeshi
relationships between depression and anxiety and care- population [38, 39, 41, 42], was classified into three cat-
related measures; and, to evaluate the psychometric egories as previously: normal [7-9 hours], less than nor-
properties of the Bangla version of the Hospital Anxiety mal [< 7h], and more than normal [> 9h].
and Depression Scale (HADS).
Work-setting-related questions
Methods The following ‘yes/no’ questions concerning the working
Participants and procedure environment were asked during the survey: Have you
A cross-sectional survey was conducted among HCWs been infected with COVID-19 while at work?, Have any
(e.g., doctors, nurses, public health professionals, lab of your colleagues been infected with COVID-19?, Do you
workers, and other caregivers) during the COVID-19 feel adequately trained to conduct COVID-19-related
pandemic in Bangladesh. Here, public health profes- treatment/PCR tests/provision of patient care?, Have you
sionals (e.g., epidemiologists, biostatisticians, health experienced shortages of PPE/hand sanitizer/masksTasnim et al. BMC Psychiatry (2021) 21:271 Page 4 of 14
during the pandemic?, Have you had regrets about your statistically significant if the two-sided p-value was less
choice of profession because of the pandemic and related than or equal to 0.05. A confirmatory factor analysis
unexpected experiences?, Are you frequently updating (CFA) was performed using SPSS Amos version 23 to
yourself with the latest research papers on COVID-19?, evaluate the psychometric properties of the Bangla ver-
Do you currently have to work overtime?, Have you ever sion of the HADS.
been discriminated against in your workplace (lab or
hospital)?, Have you been counseled regarding how to Ethics
maintain your mental health in the current situation?, All procedures of the present study were performed in
and Have you encountered social problems (e.g., neighbor accordance with human involving regulations (i.e., Dec-
neglect) due to working in a lab or hospital? laration of Helsinki) and with guidelines of institutional
research ethics. The formal ethics approval was granted
Hospital Anxiety and Depression Scale (HADS) by the ethical review board of the Faculty of Biological
The HADS is a self-reported instrument for assessing Sciences, Jahangirnagar University, Savar, Dhaka-1342,
anxiety and depression symptomatology. The HADS was Bangladesh [BBEC, JU/M 2020 COVID-19/9(5)]. All par-
developed by Zigmond & Snaith (1983) which is widely ticipants provided their consent to participate in the
used globally. This scale consists of 14 questions con- study after being informed about the purpose of the
cerning problems over the past week (e.g., “I still enjoy study. Anonymity and confidentiality of participants’ in-
the things I used to enjoy”) including 2 subscales (i.e., 7- formation were strictly maintained.
item anxiety and 7-item depression) with a four-point
Likert scale ranging from 0 to 3 [43]. The raw scores for Results
each subscale are summed as total scores ranging from 0 Participant characteristics
to 21 for each subscale. The present study employed the Data from 803 healthcare professionals were included in
Bangla HADS described recently [44]. The most widely final analysis. Approximately half (50.7%) were male,
used standardized translation procedure, proposed by mean age was 27.3 years (SD = 6.9; age range: 18-58
Beaton et al. (2000), was used to perform the back trans- years), and most were doctors (68%). Likewise, nurses
lation for this scale [45]. In the present study, predefined (10%), public health professionals (7%), lab workers (9%),
thresholds for normal (0–7), borderline abnormal (8-10), and other caregivers (6%) participated. Most participants
and abnormal (11-21) levels were used to categorize were unmarried (69.9%), resided in urban areas (81.7%),
levels of anxiety and depression [43]. The cutoff (> 8) reported good health status (62.4%), and denied chronic
utilized to screen for symptoms for anxiety and depres- diseases (90.2%). Moreover, 52.4% participants reported
sion for each subscale was the same as used previously normal sleep durations, most (62.6%) reported not get-
in the Bangladesh population [44, 46]. In the present ting physical exercise, and a minority reported cigarette
study, Cronbach’s alpha of the anxiety and depression smoking (13.7%) (Table 1).
subscales were 0.80 and 0.70, respectively, and overall
Cronbach’s alpha of the HADS scale was 0.83, indicating Psychometric properties of the Bangla HADS
good reliability. Mean, standard deviation, item-total correlation, Cron-
bach’s alpha of the scale if each item were omitted,
Statistical analysis skewness, and kurtosis of each item of the Bangla HADS
Data were analyzed using four statistical software pack- are presented (Table 2). The inter-item correlation
ages including Microsoft Excel 2019, SPSS version 25, matrix contained no negative values, indicating that the
SPSS Amos version 23, and STATA version 13. First, items were assessing the same construct. All items
data were cleaned, sorted, and coded using Microsoft yielded skewness, and kurtosis values within the ± 2.2
Excel, and after the completion of data coding, the file range, indicating that they were normally distributed.
was imported to SPSS. Descriptive statistics (i.e., fre- Confirmatory factor analysis (CFA) was performed to
quencies, percentages, means, standard deviations) were evaluate the structural validity of the Bangla HADS in-
performed using SPSS. Regression analyses with the strument using a two-factor model (anxiety, and depres-
HADS score as a dependent variable, and all examined sion). For this model, the Absolute Fit (i.e., χ2, Root
variables modeled simultaneously (i.e., adjusted for each Mean Square Error of Approximation [RMSEA], Stan-
other) were executed in STATA. The normally distrib- dardized Root Mean Square Residual [SRMR], Goodness
uted HADS total score was used as the outcome in a of Fit Index [GFI]), and the Incremental Fit (i.e., Ad-
multiple linear regression model. The reason for this ap- justed Goodness of Fit Index [AGFI], Comparative Fit
proach was that the two subscales of depression and Index [CFI], Tucker-Lewis Index [TLI], Normed Fit
anxiety were strongly associated with each other (Pear- Index [NFI]) were observed for the model fit estimation
son r = 0.64, p < 0.001). Associations were considered (Table 3). Thresholds and conventional fit indices wereTasnim et al. BMC Psychiatry (2021) 21:271 Page 5 of 14 Table 1 General characteristics of participants (health care workers [HCWs] treating COVID-19 patients; N = 803 HCWs) Variables n (%) Gender Male 407 (50.7) Female 396 (49.3) Age (27.33 ± 6.88) Young (18-25 years) 422 (52.6) Adult (>25 years) 381 (47.4) Marital status Unmarried 561 (69.9) Married 242 (30.1) Occupation Doctors 549 (68.4) Nurses 77 (9.6) Public health professionals 59 (7.3) Lab workers 73 (9.1) Others caregiversa 45 (5.6) Residence Rural 147 (18.3) Urban 656 (81.7) Self-reported health status Good 501 (62.4) Moderate 291 (36.2) Poor 11 (1.4) Chronic diseases Yes 79 (9.8) No 724 (90.2) Sleep status Less than normal 356 (44.3) Normal (7-9 hours) 421 (52.4) More than normal 26 (3.2) Physical exercising Yes 300 (37.4) No 503 (62.6) Tobacco smoking Yes 110 (13.7) No 693 (86.3) Have you been infected with COVID-19 while at work? Yes 47 (5.9) No 756 (94.1) Have any of your colleagues been infected with COVID-19? Yes 362 (45.1) No 441 (54.9) Do you feel adequately trained to conduct COVID-19-related treatment/PCR tests/provision of patient care? Yes 286 (35.6) No 517 (64.4)
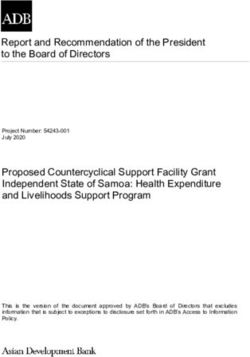
Tasnim et al. BMC Psychiatry (2021) 21:271 Page 6 of 14 Table 1 General characteristics of participants (health care workers [HCWs] treating COVID-19 patients; N = 803 HCWs) (Continued) Variables n (%) Have you experienced shortages of PPE /hand sanitizer/masks during the pandemic? Yes 454 (56.5) No 349 (43.5) Have you had regrets about your choice of profession because of the pandemic and related unexpected experiences? Yes 365 (45.5) No 438 (54.5) Are you frequently updating yourself with the latest research papers on COVID-19? Yes 639 (79.6) No 164 (20.4) Do you currently have to work overtime? Yes 415 (51.7) No 388 (48.3) Have you ever been discriminated against in your workplace (lab or hospital)? Yes 312 (38.9) No 491 (61.1) Have you been counseled regarding how to maintain your mental health in the current situation? Yes 150 (18.7) No 653 (81.3) Have you encountered social problems (e.g., neighbor neglect) due to working in a lab or hospital? Yes 195 (24.5) No 601 (75.5) Anxiety Normal 245 (30.5) Borderline abnormal 227 (28.3) Abnormal 331 (41.2) Depression Normal 486 (60.5) Borderline abnormal 191 (23.8) Abnormal 126 (15.7) Note: aPharmacologists, microbiologists, virologists, and biotechnologists applied to investigate the goodness of fit of the model Symptoms at different severity levels under statistical analysis: RMSEA (< 0.08), SRMR The HADS’ anxiety subscale revealed that anxiety symp- (< 0.08), GFI (> 0.9), AGFI (> 0.90), CFI (> 0.90), TLI toms were experienced by HCWs at different predeter- (> 0.90), and NFI (> 0.90) [47–50]. All fitness indexes mined thresholds including normal (30.5%), borderline were very satisfactory within their conventional abnormal (28.3%), and abnormal (41.2%) levels. Regard- thresholds, suggesting models provided excellent fit to ing the depression subscale, symptoms were experienced the data. by HCWs at normal (60.5%), borderline abnormal Figure 1 presents structural equation modeling (23.8%), and abnormal (15.7%) levels. The anxiety and (SEM) of the Bangla HADS, and demonstrates that depression scores were strongly associated with each the two subscales (anxiety, and depression) were posi- other (Pearson r = 0.64). tively and significantly correlated with each other. The factor loadings for each item of the Bangla HADS Regression analyses ranged between 0.38 and 0.71 (except item D5), and The HADS-score was significantly (p < 0.05) higher were acceptable. The acceptability factor is greater among participants who reported being female, having than the load value of 0.32 [51]. moderate and poor health status, not engaging in
Tasnim et al. BMC Psychiatry (2021) 21:271 Page 7 of 14
Table 2 Item-level psychometric properties of the Bangla HADS
Variables Mean SD Skewness Kurtosis Item-total correlation Cronbach's α if Item Omitted
A1 1.47 0.92 0.81 -0.73 0.51 0.82
A2 1.66 0.89 -0.19 -0.70 0.59 0.81
A3 1.45 0.87 0.29 -0.62 0.52 0.82
A4 1.14 0.74 0.29 -0.13 0.49 0.82
A5 0.88 0.72 0.31 -0.64 0.44 0.82
A6 1.67 0.87 -0.19 -0.62 0.52 0.82
A7 1.52 0.86 -0.08 -0.64 0.60 0.81
D1 0.89 0.97 0.79 -0.47 0.46 0.82
D2 0.36 0.70 1.80 2.12 0.32 0.83
D3 1.00 0.68 0.51 0.69 0.59 0.82
D4 1.33 0.87 0.20 -0.62 0.49 0.82
D5 1.77 1.09 -0.43 -1.10 0.20 0.84
D6 0.67 0.83 1.02 0.14 0.43 0.82
D7 0.83 0.89 0.83 -0.13 0.46 0.82
Note: A1: I feel tense or 'wound up'; A2: I get a sort of frightened feeling as if something awful is about to happen; A3: Worrying thoughts go through my mind;
A4: I can sit at ease and feel relaxed; A5: I get a sort of frightened feeling like 'butterflies' in the stomach; A6: I feel restless as I have to be on the move; A7: I get
sudden feelings of panic; D1: I still enjoy the things I used to enjoy; D2: I can laugh and see the funny side of things; D3: I feel cheerful; D4: I feel as if I am slowed
down; D5: I have lost interest in my appearance; D6: I look forward with enjoyment to things; D7: I can enjoy a good book or radio or TV program.
physical exercising, smoking tobacco, having had regrets and depression among HCWs in Bangladesh during the
about their profession because of the pandemic and re- COVID-19 pandemic. Our hypotheses were partially sup-
lated unexpected experiences, not updating on the latest ported in that anxiety and depression were prevalent among
COVID-19-related research, experiencing discrimination HCWs, and some but not all COVID-19-related experiences
in the workplace, and facing social problems due to were linked to anxiety and depression. The study also inves-
working in a lab or hospital (Table 4). tigated the psychometric properties of the Bangla HADS.
The Bangla HADS was psychometrically sound, and demon-
Discussion strated good internal consistency and reliability (α = 0.83),
The COVID-19 pandemic appears to have impacted the and excellent construct validity. The study included doctors,
lives of many individuals, and may influence mental nurses, public health professionals, lab workers, and other
wellbeing [37], especially among HCWs who are on the caregivers (e.g., pharmacologists, microbiologists, virologists,
frontline caring for people with COVID-19. To our best biotechnologists) who were directly or indirectly involved in
knowledge, the present study is the first to assess anxiety the care of patients with COVID-19.
Table 3 Scale-level psychometric properties of the Bangla HADS
Name of index Index Anxiety Depression HADS Level
abbreviation subscale subscale scale of acceptance
Absolute Fit
Discrepancy chi square χ2 (df) 52.19* (14) 106.69* (14) 397.18* (76) p > 0.05
Root Mean Square Error of Approximation RMSEA (90% CI) 0.06 (0.04-0.08) 0.09 (0.08-0.11) 0.07 (0.07-0.08) < 0.08
(90% Confidence interval)
Standardized Root Mean Square Residual SRMR 0.03 0.06 0.06 < 0.08
Goodness of Fit Index GFI 0.98 0.96 0.93 > 0.9
Incremental Fit
Adjusted Goodness of Fit AGFI 0.96 0.92 0.9 > 0.9
Comparative Fit Index CFI 0.97 0.9 0.9 > 0.9
Tucker-Lewis Index TLI 0.96 0.83 0.9 > 0.9
Normed Fit Index NFI 0.96 0.9 0.9 > 0.9
Note: *p < 0.001Tasnim et al. BMC Psychiatry (2021) 21:271 Page 8 of 14 Fig. 1 Structural equation modeling (SEM) of the Bangla Hospital Anxiety and Depression Scale (HADS). Note: Items of anxiety subscale (A1, A2, A3, A4, A5, A6, A7); Items of Depression subscale (D1, D2, D3, D4, D5, D6, D7); All e values represent (unobserved variables). The specific questions to which these items refer are as follows. A1: I feel tense or 'wound up'; A2: I get a sort of frightened feeling as if something awful is about to happen; A3: Worrying thoughts go through my mind; A4: I can sit at ease and feel relaxed; A5: I get a sort of frightened feeling like 'butterflies' in the stomach; A6: I feel restless as I have to be on the move; A7: I get sudden feelings of panic; D1: I still enjoy the things I used to enjoy; D2: I can laugh and see the funny side of things; D3: I feel cheerful; D4: I feel as if I am slowed down; D5: I have lost interest in my appearance; D6: I look forward with enjoyment to things; D7: I can enjoy a good book or radio or TV program Comparisons with other studies Rating Anxiety Scale) and depression (using Self-Rating The current findings indicate that anxiety and depres- Depression Scale) of 45.6%, and 11.4%, respectively [52]. sion are common among HCWs in Bangladesh during A study in India of HCWs suggested the prevalence esti- the COVID-19 pandemic, with 69.5% screening positive mates of anxiety symptoms (17.7%) requiring add- for anxiety, and 39.5% for depression. A cross-sectional itional evaluation and depressive symptoms (11.4%) study across 34 hospitals in China similarly found that needing treatment [53] are lower than those in the frontline HCWs experienced mental health concerns in- present study. Moreover, an examination of anxiety cluding depression and anxiety when directly engaged that included 12 studies (1 from Fuyang, 2 Wuhan, 1 with treating and managing patients with COVID-19 Fujian, 1 Singapore, 7 from China), and for depres- [10]. A prior study in China documented prevalence es- sion that included 10 studies (2 Wuhan, 1 Fujian, 1 timates of anxiety (46.0% versus 39.5% in the present Singapore, 6 from China) reported that the pooled study) with the Generalized Anxiety Disorder Scale prevalence estimates of anxiety and depression among (GAD-7) and depression (44.4% versus 69.5% in the HCWs during COVID-19 were 23.2% and 22.8%, re- present study) with the Patient Health Questionnaire spectively, and these values are numerically lower (PHQ-9) among HCWs during the COVID-19 pandemic than those in the present study [54]. However, one [7], which suggests that the prevalence estimate of anx- should consider comparisons across studies cautiously iety was somewhat higher and that of depression lower given other factors that may influence estimates, and compared to the present study. Another study of anxiety studies that directly compare estimates concurrently and depression among first-line medical staff in China across jurisdictions, and using similar methodologies showed prevalence estimates of anxiety (using Self- are warranted. The extent to which different findings
Tasnim et al. BMC Psychiatry (2021) 21:271 Page 9 of 14
Table 4 Regression analyses by total HADS score with all examined variables
Variables Total HADS score
Mean (SD) β SE
Gender
a
Male 16.1 (6.8)
Female 17.2 (6.6) 0.13*** 0.43
Age
a
Young (18-25 years) 17.0 (6.6)
Adult (>25 years) 16.2 (6.8) -0.02 0.52
Marital status
a
Unmarried 16.7 (6.5)
Married 16.4 (7.2) -0.06 0.56
Residence
a
Rural 16.0 (7.2)
Urban 16.8 (6.6) 0.03 0.53
Self-reported health status
a
Good 14.7 (6.0)
Moderate 19.4 (6.4) 0.23*** 0.46
Poor 29.0 (6.7) 0.18*** 1.79
Chronic diseases
a
No 16.3 (6.6)
Yes 19.3 (7.1) 0.04 0.74
Sleep status
a
Less than normal 16.6 (6.4)
Normal (7-9 hours) 16.5 (6.8) -0.05 0.45
More than normal 18.2 (9.8) -0.02 1.18
Physical exercising
a
Yes 14.6 (6.3)
No 17.8 (6.7) 0.08** 0.44
Tobacco smoking
a
No 16.4 (6.6)
Yes 18.0 (7.4) 0.07* 0.64
Have you been infected with COVID-19 while at work?
a
No 16.5 (6.7)
Yes 18.0 (7.1) -0.02 0.88
Have any of your colleagues been infected with COVID-19?
a
No 15.8 (6.4)
Yes 17.7 (7.0) 0.03 0.45
Do you feel adequately trained to conduct COVID-19-related treatment/PCR tests/provision of patient care?
a
Yes 16.0 (6.2)
No 17.0 (7.0) -0.01 0.48
Have you experienced shortages of PPE /hand sanitizer/masks during the pandemic?
a
No 15.8 (6.2)
Yes 17.2 (7.0) -0.04 0.45
Have you had regrets about your choice of profession because of the pandemic and related unexpected experiences?
a
No 14.6 (6.0)Tasnim et al. BMC Psychiatry (2021) 21:271 Page 10 of 14
Table 4 Regression analyses by total HADS score with all examined variables (Continued)
Variables Total HADS score
Mean (SD) β SE
Yes 19.0 (6.7) 0.16*** 0.46
Are you frequently updating yourself with the latest research papers on COVID-19?
a
Yes 16.0 (6.4)
No 19.2 (7.3) 0.08** 0.52
Do you currently have to work overtime?
a
No 16.5 (6.9)
Yes 16.7 (6.6) -0.03 0.46
Have you ever been discriminated against in your workplace (lab or hospital)?
a
No 14.8 (6.1)
Yes 19.5 (6.6) 0.21*** 0.47
Have you been counseled regarding how to maintain your mental health in the current situation?
a
Yes 14.7 (5.1)
No 17.1 (7.0) -0.01 0.62
Have you encountered social problems (e.g., neighbor neglect) due to working in a lab or hospital?
a
No 15.6 (6.4)
Yes 19.7 (6.8) 0.13*** 0.51
Note:
SE Standard error
β– Standardized regression coefficient
*p < 0.05, **p < 0.01, ***p < 0.001
a
Reference category
may relate to cultural differences, differences in disease, hypertension, and kidney disease [60], and find-
healthcare systems, and their responses during the ings from a literature review [61].
COVID-19 pandemic, differences in instruments used In the present study, participants who did not engage in
to assess anxiety and depression or other factors war- physical exercising compared to those who did were more
rants additional investigation. likely to endorse anxiety and depression, similar to prior
Females were more likely to experience anxiety and studies conducted in Bangladesh [39, 56, 59, 62]. HCWs
depression, similar to prior studies conducted in who smoked cigarettes were more likely to be anxious and
Bangladesh during the COVID-19 pandemic [39, 55]. depressed than non-smokers, also consistent with previ-
However, the findings contrast with those from a study ous studies [63–66]. A pre-COVID-19 study among med-
among university students that showed no gender- ical staff in Greece similarly showed significant
related differences [56]. A prior study conducted among associations with anxiety and depression [67]. These find-
Chinese medical staff during the COVID-19 pandemic ings may have clinical relevance as exercise and smoking
reported that anxiety was more frequently observed in represent modifiable risk factors. Therefore, if the associa-
females relative to males [57]. tions between low exercise and/or smoking, and poor
HCWs with moderate and poor health status were mental health are causal [68–70], risk reduction strategies
more depressed and anxious than those who self- focusing on regular exercise and smoking discontinuation
reported good health. These findings resonate with those may be helpful in reducing potentially deleterious impacts
among Bangladeshi university students in which individ- of COVID-19 on the mental health of HCWs. In such ef-
uals with moderate and poorer self-related health were forts, combination approaches may be particularly rele-
more depressed and anxious [58]. Another study con- vant [71]; however, other stress-reduction approaches
ducted in Bangladesh among individuals who had recov- (e.g., meditation, massage) may be helpful, although more
ered from COVID-19 found a positive association research is needed in this area [72]. Further, some benefits
between poor health status and depression [59]. The of engaging in physical activity may be transmitted to pa-
findings are also similar to those from a study in Syria tients, although this too warrants further study [73].
among community adults that observed an association Anxiety and depression were associated with negative
between depression and chronic diseases including heart feelings about choice of profession due to the ongoingTasnim et al. BMC Psychiatry (2021) 21:271 Page 11 of 14
crisis of the pandemic and unexpected pandemic-related depression during the COVID-19 pandemic. Multiple
experiences. Considering the limited availability of PPE, factors may contribute to anxiety and depression, includ-
disinfection materials, and medical (N95) masks, and in- ing those inside and outside of workplace settings. After
creasing numbers of positive COVID-19 cases [74], severe crises have ended, anxiety and depression may
HCWs may question their choice of profession. Other persist, and PTSD may emerge [12, 18]. The present
factors (e.g., possible trauma-related to patient care dur- findings suggest that understanding factors influencing
ing the pandemic) may also impact HCWs, and lead to the mental health of HCWs, and those that may gener-
mental health concerns. ate vulnerability or promote resilience are important to
Anxiety and depression were significantly higher understand currently and moving forward. It seems im-
among respondents who did not feel up to date on the portant to implement monitoring initiatives, and pos-
latest COVID-19-related research/information. Lack of sible interventions to help potentially vulnerable groups
information may precipitate mental health concerns, and like HCWs.
prior studies have suggested updates and knowledge
about COVID-19 may have psychosocial impacts, pos-
Limitations
sibly as they represent an active way of coping and deal-
This study has several limitations. First, it was a cross-
ing with pandemic-related issues [75].
sectional online survey involving a convenience sample.
HCWs who encountered discrimination in their work-
Hence, causal inferences cannot be defined. Further
place were more likely to be anxious, similar to findings
studies are required to examine longitudinal trajectories
among Chinese physicians in which workplace violence
of anxiety and depressive symptoms in HCWs during
was associated with poor mental health [76]. Other stud-
and following the COVID-19 pandemic. Second, there
ies have found that discrimination in the workplace was
was a small number of doctors, nurses, lab workers, and
related negatively to mental wellbeing [77–79]. Given
public health professionals who participated, which may
the current scarcity of HCWs in Bangladesh, shortages
not be representative of the general population. Finally,
of PPE and fear of being infected by the virus [74], and
findings of self-reported mental health symptomatology
transmitting it to family members could promote anxiety
may differ from those obtained from clinical interviews.
and depression. As a lower-middle income country,
Bangladesh is particularly vulnerable to the transmission
of a communicable disease due to overcrowded environ- Conclusions
ments, and having poor infection prevention and control The present study describes prevalence estimates and
mechanisms [74]. As such, HCWs may fear that they correlates of anxiety and depression in HCWs during
may infect their families, particularly in Bangladesh be- the COVID-19 pandemic in Bangladesh. HCWs’ mental
cause of multifamily households, which often do not wellbeing is an important consideration during the
permit separate personal spaces. These issues may pose COVID-19 outbreak. Interventions to promote the men-
particular challenges for Bangladeshi HCWs during the tal wellbeing of HCWs during and following the
pandemic. A previous study reported frequent reports of COVID-19 pandemic should be introduced, imple-
lack of water (50%), and handwashing soaps used to mented, and tested, with a particular focus on vulnerable
clean hands and kill germs/coronavirus (39%) in health groups.
care facilities in low-middle income countries [80].
HCWs should be provided with adequate PPE to protect Abbreviations
themselves and their patients within a health-promoting HCWs: Healthcare workers; HADS: Hospital Anxiety and Depression Scale;
atmosphere. SARS CoV-2: Severe acute respiratory syndrome coronavirus-2; COVID-
19: Coronavirus disease-2019; WHO: World Health Organization; PPE: Personal
Respondents facing social problems due to their pro- protective equipment; PTSD: Post-traumatic stress disorder;
fession were more likely to experience anxiety and de- CFA: Confirmatory factor analysis; RMSEA: Root Mean Square Error of
pression. Similarly, social difficulties and stressful Approximation; SRMR: Standardized Root Mean Square Residual;
GFI: Goodness of Fit Index; AGFI: Adjusted Goodness of Fit Index;
incidents have been linked to anxiety and depression CFI: Comparative Fit Index; TLI: Tucker-Lewis Index; NFI: Normed Fit Index
[81].
The present study revealed that anxiety and depression Acknowledgments
were strongly associated with each other (r = 0.64). Anx- The authors would like to thank all of the participants who consented
iety and depression frequently co-occur [82], including willingly and enrolled in the study voluntarily. Finally, the authors wish to
express profound gratitude to Sadman Sakib Rahman, Salman Hridoy,
in Bangladeshi groups [39, 56, 66, 83]. Nishrita Debnath, Md. Fahad Shahariar Nayon, Rubaiya Binthe Hashem,
Mohtasin Monim, Md. Naeem Islam, Shahan Ara Taskin Tanha, Nowrin Islam,
Implications Safa Akter Ruma, Md. Sifat Farhan Sany, Antara Raidah Rashid, Umma
Motahara Anamika, Shahrina Tasnim Manami, Mohosina Akther, Soniya Akter
The present findings indicate that many Bangladeshi Sony, and Nusrat Zahan for their voluntary contributions during the data
HCWs have been experiencing anxiety and/or collection periods.Tasnim et al. BMC Psychiatry (2021) 21:271 Page 12 of 14
Authors’ contributions 8. Shaukat N, Ali DM, Razzak J. Physical and mental health impacts of
Conceptualization: RT, MSHS, and Md. Saiful Islam (MSI). Data collection: AHR, COVID-19 on healthcare workers: a scoping review. Int J Emerg Med.
MABS, TYT, RN, and AH. Analysis and interpretation of data: MSI. Drafting of 2020;13:40.
the manuscript: RT, MSHS, and MSI. Editing: SH, SN, SI, Muhammad Sougatul 9. Liu X, Kakade M, Fuller CJ, Fan B, Fang Y, Kong J, et al. Depression after
Islam (MuSI), MNP, and JVO. Critical revision of the manuscript: MSI, MNP, exposure to stressful events: Lessons learned from the severe acute
and JVO. RT, MSHS, and MSI are equally contributed in the manuscript. All respiratory syndrome epidemic. Compr Psychiatry. 2012;53:15–23.
authors have read and approved the manuscript. 10. Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental
health outcomes among health care workers exposed to coronavirus
Funding disease 2019. JAMA Netw open. 2020;3:e203976.
The authors didn’t receive any grants or remunerations from either public or 11. Kang L, Li Y, Hu S, Chen M, Yang C, Yang BX, et al. The mental health of
private organizations or other funding agencies. medical workers in Wuhan, China dealing with the 2019 novel coronavirus.
Lancet Psychiatry. 2020;7:e14.
12. Chong M-Y, Wang W-C, Hsieh W-C, Lee C-Y, Chiu N-M, Yeh W-C, et al.
Availability of data and materials
Psychological impact of severe acute respiratory syndrome on health
The datasets used and/or analyzed during the current study are available
workers in a tertiary hospital. Br J Psychiatry. 2004;185:127–33.
from the corresponding author on reasonable request.
13. Maunder R, Hunter J, Vincent L, Bennett J, Peladeau N, Leszcz M, et al. The
immediate psychological and occupational impact of the 2003 SARS
Declarations outbreak in a teaching hospital. CMAJ. 2003;168:1245–51.
14. Bai Y, Lin C-C, Lin C-Y, Chen J-Y, Chue C-M, Chou P. Survey of stress
Ethics approval and consent to participate reactions among health care workers involved with the SARS outbreak.
All procedures of the present study were performed in accordance with the Psychiatr Serv. 2004;55:1055–7.
Declaration of Helsinki. Formal ethics approval was granted by the ethical 15. Lee AM, Wong JGWS, McAlonan GM, Cheung V, Cheung C, Sham PC, et al.
review board of the Faculty of Biological Sciences, Jahangirnagar University, Stress and psychological distress among SARS survivors 1 year after the
Savar, Dhaka-1342, Bangladesh [BBEC, JU/M 2020 COVID-19/9(5)]. All partici- outbreak. Can J Psychiatry. 2007;52:233–40.
pants provided their informed consent to participate in the study after being 16. Islam MS, Potenza MN, Van Os J. Posttraumatic stress disorder during the
informed about the purpose of the study. COVID-19 pandemic: upcoming challenges in Bangladesh and preventive
strategies. Int J Soc Psychiatry. 2020;20764020954469. https://doi.org/10.11
Consent for publication 77/0020764020954469.
Not applicable. 17. Maunder R. The experience of the 2003 SARS outbreak as a traumatic stress
among frontline healthcare workers in Toronto: Lessons learned. Philos
Competing interests Trans R Soc Lond B Biol Sci. 2004;359:1117–25.
The authors declare that they have no potential conflict of interest in the 18. Wu P, Fang Y, Guan Z, Fan B, Kong J, Yao Z, et al. The psychological impact of
publication of this research output. the SARS epidemic on hospital employees in China: exposure, risk perception,
and altruistic acceptance of risk. Can J Psychiatry. 2009;54:302–11.
Author details 19. Bao Y, Sun Y, Meng S, Shi J, Lu L. 2019-nCoV epidemic: Address mental
1
Department of Public Health and Informatics, Jahangirnagar University, health care to empower society. Lancet. 2020;395:e37–8.
Savar, Dhaka 1342, Bangladesh. 2Centre for Advanced Research Excellence in 20. Chen Q, Liang M, Li Y, Guo J, Fei D, Wang L, et al. Mental health care for
Public Health, Savar, Dhaka 1342, Bangladesh. 3Department of Population medical staff in China during the COVID-19 outbreak. Lancet Psychiatry.
Science and Human Resource Development, Rajshahi University, Rajshahi 2020;7:e15–6.
Sadar, Rajshahi 6205, Bangladesh. 4Department of Microbiology, 21. Rahman ME, Islam MS, Bishwas MS, Moonajilin MS, Gozal D. Physical
Jahangirnagar University, Savar, Dhaka 1342, Bangladesh. 5BioTED, Mirpur, inactivity and sedentary behaviors in the Bangladeshi population during the
Dhaka 1216, Bangladesh. 6Department of Psychiatry and Child Study Center, COVID-19 pandemic: An online cross-sectional survey. Heliyon. 2020;6:
Yale School of Medicine, New Haven, Connecticut, USA. 7Connecticut Mental e05392.
Health Center, New Haven, Connecticut, USA. 8Connecticut Council on 22. Ferdous MZ, Islam MS, Sikder MT, Mosaddek ASM, Zegarra-Valdivia JA, Gozal
Problem Gambling, Wethersfield, Connecticut, USA. 9Department of D. Knowledge, attitude, and practice regarding COVID-19 outbreak in
Neuroscience, Yale University, New Haven, Connecticut, USA. 10Department Bangladesh: an online-based cross-sectional study. PLoS One. 2020;15:
of Psychiatry, UMC Utrecht Brain Center, University Medical Center Utrecht, e0239254.
Utrecht University, Utrecht, The Netherlands. 11Department of Psychosis 23. Islam MS, Emran GI, Rahman E, Banik R, Sikder T, Smith L, et al.
Studies, Institute of Psychiatry, Psychology & Neuroscience, King’s College Knowledge, attitudes and practices associated with the COVID-19
London, London, United Kingdom. among slum dwellers resided in Dhaka City: a Bangladeshi interview-
based survey. J Public Health (Oxf). 2021;43(1):13–25. https://doi.org/10.1
Received: 23 September 2020 Accepted: 26 April 2021 093/pubmed/fdaa182.
24. Institute of Epidemiology Disease Control and Research. Covid-19 status for
Bangladesh. 2020. http://old.iedcr.gov.bd/. Accessed 22 Sep 2020.
References 25. Bangladesh Medical Association. List of Death Doctors Due to COVID-19_
1. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of Detail. 2020. https://bma.org.bd/covid-19/ListofDeathDoctorsDuetoCOVID-1
global health concern. Lancet. 2020;395:470–3. 9_Detail.pdf. Accessed 22 Sep 2020.
2. Mahase E. China coronavirus: WHO declares international emergency as 26. Bangladesh Medical Association. District wise total number of affected
death toll exceeds 200. BMJ. 2020;368:m408. doctor, nurse & staff (COVID 19+). 2020. https://bma.org.bd/covid-19/TotalA
3. World Health Organization. Coronavirus disease (COVID-19) pandemic. 2020. ffectedDoctorNurse&Staff.pdf. Accessed 22 Sep 2020.
https://www.who.int/emergencies/diseases/novel-coronavirus-2019. 27. The World Bank. Hospital beds (per 1,000 people) - Bangladesh. 2017.
Accessed 22 Sep 2020. https://data.worldbank.org/indicator/SH.MED.BEDS.ZS?locations=BD&name_
4. Mahase E. Coronavirus: covid-19 has killed more people than SARS and desc=false. Accessed 22 Sep 2021.
MERS combined, despite lower case fatality rate. BMJ. 2020;368:m641. 28. Corona Info. How long can they last? 2021. https://corona.gov.bd/banner/
5. Baden LR, Rubin EJ. Covid-19 - The Search for Effective Therapy. New Engl J 72. Accessed 22 Sep 2021.
Med. 2020;382:1851–2. 29. Dhaka Tribune. Number of ICU beds insufficient to combat Covid-19
6. Catton H. Global challenges in health and health care for nurses and pandemic. 2020. https://www.dhakatribune.com/bangladesh/2020/03/21/
midwives everywhere. Int Nurs Rev. 2020;67:4–6. number-of-icu-beds-insufficient-to-combat-covid-19-pandemic.
7. Que J, Shi L, Deng J, Liu J, Zhang L, Wu S, et al. Psychological impact of the 30. Siraj MS, Dewey RS, Hassan ASMFU. The infectious diseases act and resource
COVID-19 pandemic on healthcare workers: A cross-sectional study in allocation during the COVID-19 pandemic in Bangladesh. Asian Bioeth Rev.
China. Gen psychiatry. 2020;33:e100259. 2020;12:491–502.Tasnim et al. BMC Psychiatry (2021) 21:271 Page 13 of 14
31. Directorate General of Health Services. National preparedness and response 54. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P.
plan for COVID-19, Bangladesh. 2020. https://reliefweb.int/sites/reliefweb.int/ Prevalence of depression, anxiety, and insomnia among healthcare workers
files/resources/nprp_covid-19_v6_18032020.pdf. Accessed 22 Sep 2020. during the COVID-19 pandemic: A systematic review and meta-analysis.
32. Directorate General of Health Services. National Guidelines on Clinical Brain Behav Immun. 2020;88:901–7.
Management of Coronavirus Disease 2019 (COVID-19). 2020. https://mofa. 55. Islam MS, Tasnim R, Sujan MSH, Ferdous MZ, Sikder MT, Masud JHB, et al.
portal.gov.bd/sites/default/files/files/mofa.portal.gov.bd/page/ad1f289c_4 Depressive symptoms associated with COVID-19 preventive practice
7cf_4f6c_8dee_887957be3176/NationalGuidelines on ClinicalManagement measures, daily activities in home quarantine and suicidal behaviors:
of Covid-19-DGHS.pdf. Accessed 22 Sep 2020. Findings from a large-scale online survey in Bangladesh. Accepted in BMC
33. Islam MT, Talukder AK, Siddiqui MN, Islam T. Tackling the COVID-19 Psychiatry. 2021.
pandemic: the Bangladesh perspective. J Public health Res. 2020;9:1794. 56. Islam MS, Akter R, Sikder T, Griffiths MD. Prevalence and factors associated
https://doi.org/10.4081/jphr.2020.1794. with depression and anxiety among first-year university students in
34. The Lancet. COVID-19: protecting health-care workers. Lancet. 2020;395:922. Bangladesh: a cross-sectional study. Int J Ment Health Addict. 2020. https://
35. Anwar S, Nasrullah M, Hosen MJ. COVID-19 and Bangladesh: Challenges and doi.org/10.1007/s11469-020-00242-y.
how to address them. Front Public Heal. 2020;8:154. 57. Huang JZ, Han MF, Luo TD, Ren AK, Zhou XP. Mental health survey of
36. United Nations Development Programme (UNDP). Covid-19: A reality check medical staff in a tertiary infectious disease hospital for COVID-19.
for Bangladesh’s healthcare system. 2020. https://www.bd.undp.org/ Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 2020;38:192–5.
content/bangladesh/en/home/stories/a-reality-check-for-bangladesh-s-hea 58. Hossain S, Anjum A, Hasan MT, Uddin ME, Hossain MS, Sikder MT. Self-
lthcare-system.html. Accessed 22 Sep 2020. perception of physical health conditions and its association with depression
37. Islam MS, Ferdous MZ, Potenza MN. Panic and generalized anxiety during and anxiety among Bangladeshi university students. J Affect Disord. 2020;
the COVID-19 pandemic among Bangladeshi people: an online pilot survey 263:282–8.
early in the outbreak. J Affect Disord. 2020;276:30–7. 59. Islam MS, Ferdous MZ, Islam US, Mosaddek ASM, Potenza MN, Pardhan S.
38. Tasnim R, Islam MS, Sujan MSH, Sikder MT, Potenza MN. Suicidal ideation Treatment, persistent symptoms, and depression in people infected with
among Bangladeshi university students early during the COVID-19 pandemic: COVID-19 in Bangladesh. Int J Environ Res Public Health. 2021;18:1453.
prevalence estimates and correlates. Child Youth Serv Rev. 2020;119:105703. 60. Kilzieh N, Rastam S, Maziak W, Ward KD. Comorbidity of depression with
39. Islam MS, Sujan MSH, Tasnim R, Sikder MT, Potenza MN, van Os J. chronic diseases: a population-based study in Aleppo. Syria. Int J Psychiatry
Psychological responses during the COVID-19 outbreak among university Med. 2008;38:169–84.
students in Bangladesh. PLoS One. 2020;15:e0245083. 61. Chapman DP, Perry GS, Strine TW. The vital link between chronic disease
40. Al ZA, Rahman ME, Islam MB, SZD B, Rahman QM, MRAM B, et al. and depressive disorders. Prev Chronic Dis. 2005;2:A14.
Psychological states of Bangladeshi people four months after the COVID-19 62. Islam MS, Akter R, Sikder MT, Griffiths MD. Weight-related status and
pandemic: an online survey. Heliyon. 2020;6:e05057. associated predictors with psychological well-being among first-year
41. Islam MS, Sujan MSH, Tasnim R, Ferdous MZ, Masud JHB, Kundu S, et al. university students in Bangladesh: a pilot study. Int J Ment Health Addict.
Problematic internet use among young and adult population in 2020. https://doi.org/10.1007/s11469-020-00243-x.
Bangladesh: correlates with lifestyle and online activities during the COVID- 63. Tjora T, Hetland J, Aarø LE, Wold B, Wiium N, Øverland S. The association
19 pandemic. Addict Behav Rep. 2020;12:100311. https://doi.org/10.1016/j.a between smoking and depression from adolescence to adulthood.
brep.2020.100311. Addiction. 2014;109:1022–30.
42. Islam MS, Sujan MSH, Tasnim R, Mohona RA, Ferdous MZ, Kamruzzaman 64. Martini S, Wagner FA, Anthony JC. The association of tobacco smoking and
S, et al. Problematic smartphone and social media use among depression in adolescence: Evidence from the United States. Subst Use
Bangladeshi college and university students amid COVID-19: The role of Misuse. 2002;37:1853–67.
psychological wellbeing and pandemic related factors. Front Psychiatry. 65. Boden JM, Fergusson DM, Horwood LJ. Cigarette smoking and depression:
2021;12:647386. tests of causal linkages using a longitudinal birth cohort. Br J Psychiatry.
43. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta 2010;196:440–6.
Psychiatr Scand. 1983;67:361–70. 66. Islam MS, Rahman ME, Moonajilin MS, van Os J. Prevalence of depression,
44. Chowdhury SH, Karim MN, Selim S, Ahmed F, Azad AK, Maksud SA, et al. anxiety and associated factors among school going adolescents in
Risk of depression among Bangladeshi type 2 diabetic patients. Diabetes Bangladesh: Findings from a cross-sectional study. PLoS One. 2021;16:
Metab Syndr. 2017;11(Suppl 2):S1009–12. e0247898.
45. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process 67. Tselebis A, Papaleftheris E, Balis E, Theotoka I, Ilias I. Smoking related to
of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976). anxiety and depression in Greek medical staff. Psychol Rep. 2003;92:529–32.
2000;25:3186–91. 68. Wootton RE, Richmond RC, Stuijfzand BG, Lawn RB, Sallis HM, Taylor GMJ,
46. Bocéréan C, Dupret E. A validation study of the Hospital Anxiety and et al. Evidence for causal effects of lifetime smoking on risk for depression
Depression Scale (HADS) in a large sample of French employees. BMC and schizophrenia: a Mendelian randomisation study. Psychol Med. 2020;50:
Psychiatry. 2014;14:354. 2435–43.
47. Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure 69. De Moor MHM, Boomsma DI, Stubbe JH, Willemsen G, de Geus EJC. Testing
analysis: Conventional criteria versus new alternatives. Struct Equ Model a causality in the association between regular exercise and symptoms of
Multidiscip J. 1999;6:1–55. anxiety and depression. Arch Gen Psychiatry. 2008;65:897–905.
48. Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis 70. Scott JG, Matuschka L, Niemelä S, Miettunen J, Emmerson B, Mustonen A.
of covariance structures. Psychol Bull. 1980;88:588. Evidence of a Causal Relationship Between Smoking Tobacco and
49. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990; Schizophrenia Spectrum Disorders. Front psychiatry. 2018;9:607.
107:238. 71. La Torre G, Tiberio G, Sindoni A, Dorelli B, Cammalleri V. Smoking cessation
50. Hooper D, Coughlan J, Mullen MR. Structural equation modelling: interventions on health-care workers: a systematic review and meta-analysis.
Guidelines for determining model fit. Electron J Bus Res methods. 2008;6: PeerJ. 2020;8:e9396.
53–60. 72. Ruotsalainen JH, Verbeek JH, Mariné A, Serra C. Preventing occupational
51. Tabachnick B, Fidell LS. Using Multivariate Statistics; 2007. stress in healthcare workers. Cochrane Database Syst Rev. 2015;2015:
52. Zhu J, Sun L, Zhang L, Wang H, Fan A, Yang B, et al. Prevalence and CD002892.
influencing factors of anxiety and depression symptoms in the first-line 73. Banday AH, Want FA, Alris FFA, Alrayes MF, Alenzi MJ. A cross-sectional
medical staff fighting against COVID-19 in Gansu. Front psychiatry. 2020;11: study on the prevalence of physical activity among primary health care
386. physicians in Aljouf Region of Saudi Arabia. Mater Sociomed. 2015;27:263–6.
53. Wilson W, Raj JP, Rao S, Ghiya M, Nedungalaparambil NM, Mundra H, et al. 74. Hassan MZ, Monjur MR, Styczynski AR, Rahman M, Banu S. Protecting
Prevalence and predictors of stress, anxiety, and depression among frontline healthcare workers should be the top priority in low-resource
healthcare workers managing COVID-19 pandemic in India: a nationwide health systems: Bangladesh and COVID-19. Infect Control Hosp Epidemiol.
observational study. Indian J Psychol Med. 2020;42:353–8. 2020;42:121–2.You can also read