PROGRAMME CORTISONE PROGRAMME BLUEPRINT DOCUMENT 20 JUNE 2014 VERSION 1.0 - MEDIS/FUTUREPLANS/PROGINIT/CORTISONE/PROGBLUE/V1.0
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MedIS/FuturePlans/ProgInit/CORTISONE/ProgBlue/v1.0 Programme CORTISONE Programme Blueprint Document 20 June 2014 Version 1.0 Programme Blueprint 20140620-cortisone-programme-blueprint-v1.doc
Programme Name CORTISONE
SRO Surgeon General within the Defence Health Change Programme
Programme Manager Col J W Cooper, SG AH J5 Med IS
Author J G Kehoe, SG KM
Date 24/07/2013 Version 0.01 Status Initial draft for internal review
06/09/2013 0.02 Revised to include future state
13/09/2013 0.03 Desk circulation
30/09/2013 0.04 Revised to incorporate
stakeholder feedback
11/12/2013 0.05 AD level circulation
30/01/2014 0.06 For DMISSG endorsement
06/03/2014 0.07 Hd MedOpCap Review
11/03/2014 0.08 1* Circulation
27/03/2014 0.09 2* Approval
05/06/2014 0.10 Revised to incorporate
stakeholder feedback
20/06/2014 1.0 Final Version
Annexes
A DMS Current State
B Gap Analysis
C Glossary of Terms
Reference Documents
A Government ICT Strategy 2011
B Defence ICT Strategy 2013
C DMS Strategy 2012-30
D DMS Information Strategy ver 1.9
E DMS Information Plan ver 1.9
F Department of Health NHS Information Strategy – ‘The Power of Information’
G Joint Medical Doctrine: Joint Doctrine Publication 4.03
Programme Blueprint i 20140620-cortisone-programme-blueprint-v1.docBlueprint
Purpose: The purpose of this Blueprint is to provide a model of the capability that must be in
place to realise the Vision of Programme CORTISONE, which is:
‘A sustainable, integrated, cohesive and enduring information capability that will fully and
effectively support the delivery of evidence-based medical and dental health and healthcare
outputs, in order to achieve the Aim 1 of the Defence Medical Services (DMS).’
It provides the focus for delivering the changes to the DMS’ health and healthcare information
capability, as required by the DMS sub-Strategy 2 and articulated in the DMS Information sub-
Strategy 3 , which will meet the continuing and emerging needs of both the organisation and wider
Defence.
This is a living document that will evolve and gain greater detail as the programme matures and
progresses but will provide an essential foundation, in the first instance, for the CORTISONE
Concept Phase.
The Blueprint is not a specification, nor does it represent any form of requirements
document for the components listed within it, and is subject to change.
SCOPE
1. The CORTISONE programme addresses the support requirement for information generated
by the DMS in producing their mandated outputs, across all contexts and capabilities of care. This
includes the clinical, administrative, business management and force generation domains.
2. The Surgeon General’s remit does not cover the provision of veterinary services medical
information. The programme specifically excludes addressing the information support service
requirements of Defence’s Military Working Animals capability. Also excluded are information
services in support of medical training administration.
ORGANISATION OF THE DMS – CURRENT STATE
3. A description of the DMS’ current structure and the primary business pillars that are likely to
be directly impacted by the CORTISONE programme is provided at Annex A.
CURRENT DMS INFORMATION SYSTEMS
4. The Surgeon General and the DMS fully recognise the importance of information in fulfilling
their remit to promote, protect and restore the health of the Defence PAR, both in the Firm Base
and on deployed operations. There is now widespread recognition that DMS must move to take its
service provision to the next level and provide coherent information services spanning all medical
capabilities, inclusive of single-Service elements, in order to maximise operational effectiveness.
Collaborative development between the DMS and service providers will be necessary in order to
achieve this goal.
1
The Aim of the Defence Medical Services is to promote, protect and restore the health of the Defence population in order to
maximise fitness for role.
2
Reference Document C, para 16, sub-para (2).
3
Reference Document D.
Programme Blueprint 1 20140620-cortisone-programme-blueprint-v1.doc5. The majority of the DMS’ information capability in the Firm Base and Permanent Joint
Operating Bases (PJOBs) is delivered via the Defence-wide Defence Information Infrastructure
(DII), although delivery over legacy infrastructures remains the only option in a very small number
of locations. The major clinical information systems currently in service are:
• DMICP – this is the core primary health and dental care information support tool, providing
an iEHR capability for Defence. The acronym is now commonly regarded as referencing the
iEHR software product/service rather than the originally-planned wider programme. DMICP is
in daily use to underpin clinical care at all medical and dental centres in the Firm Base and
PJOBs. The key enabler of the system is a centralised database for the iEHR, which replaced
the myriad standalone electronic and paper-based records systems previously in existence.
This allows DMS personnel to access accurate, up-to-date patient records at all clinical
locations where required. DMICP also provides access to a wide range of reference material
and receives nightly updates from the Joint Personnel Administration (JPA) system, which is
the definitive military personnel record repository for Defence. It also interfaces with the NHS
Spine to facilitate ‘Choose & Book’ functionality for referrals to SHC.
• DMICP Deployed – the deployable version of the application is modified in design to enable
its operation in locations where there is no guarantee of connectivity to back-end data
repositories. This includes deployments, exercises, overseas bases (OVBs), PJOBs, Afloat,
and temporary medical facilities. DMICP Deployed operates by using a local server (laptop or
tower), which synchronises with the master database when connectivity is available. Client
access is achieved via ruggedized laptops. Synchronisation can occur online (gold standard) or
via removable media.
• Whole Hospital Information System (WHIS) – the purpose of the WHIS is to implement a
SHC information management system in the Camp Bastion Role 3 Medical Treatment Facility
(MTF), utilising a Patient Administration System (PAS) as the central component. It aims to
bring coherence and interoperability between parallel projects, delivering enhanced laboratory
systems, imaging, the CT scanner equipment upgrade project and existing coalition SHC
systems – the success of this has been limited. The WHIS was procured as an Urgent
Operational Requirement (UOR). Due to software licensing restrictions, the system cannot be
used in any other location or for any other purpose than that originally specified. WHIS is not
expected to be brought into the core equipment programme as the technical solution deployed
has been assessed as being over-specified for the task. However, the need for this capability in
Deployed, Afloat (RFA Argus, in its role as a Primary Casualty Receiving Ship (PCRS)) and
Firm Base contexts is fully acknowledged.
• Radiology & Teleradiology systems – this capability facilitates the administration of patient
and examination data through the Radiology Information System (RIS), and the viewing and
subsequent archiving of Digital Images and COmmunication in Medicine (DICOM)-compliant
images to the Picture Archiving Communications System (PACS). Both of these systems
interface with other radiology equipment within the Bastion MTF and UK Medical Facilities. A
deployed PACS was procured as a UOR and interfaced with the core Centre for Defence
Radiology (CDR) PACS and RIS, which enables the transmission of image files. Again, the
capability was procured as a UOR but will is expected to be brought into the core equipment
programme (subject to a favourable ABC 14 decision), potentially allowing its wider integration
across the DMS. RFA Argus is also equipped with a standalone PACS, although it currently
has no means by which to transmit image files off-ship.
• Laboratory Information Management System (LIMS) – LIMS provides pathology support
in a number of DMS locations. It is interfaced with WHIS in the Role 3 MTF at Camp Bastion,
and also on the replica training system at the Army Medical Services Training Centre (AMSTC),
Strensall Barracks. All other instances of the system are standalone in nature, including the
Programme Blueprint 2 20140620-cortisone-programme-blueprint-v1.docRFA Argus installation. LIMS was procured as a UOR and was brought into core as part of the
Operational Deployed Medical Capability (ODMC) 2 project.
• Joint Theatre Trauma Register (JTTR) – the JTTR captures complex details of all fatalities
and trauma injuries sustained in the operational environment. Its primary role is to provide
continuous near real-time quality improvement of major trauma care and patient outcomes in
support of current operations. Its secondary roles are to support research and development,
with both Defence Statistics (Health) and Medical Director staffs analysing and exploiting the
datasets.
• Central Health Records Library (CHRL) systems – CHRL is the main repository for the
archiving of both physical and electronic medical records. CHRL receives records from many
sources and in many formats, which are then converted to image format (where possible) for
storage/retrieval electronically. The systems in use at CHRL are not readily accessible to the
wider DMS or Defence. The CHRL service is in danger of systemic failure and is the subject of
a programme of stabilisation work at present.
• EPINATO – the NATO health surveillance system mandated for use on NATO operations
(described in AMedP 4.1, currently awaiting promulgation by the NATO Standardization
Agency (NSA)). Developed from the UK paper-based J95 health surveillance system, this is
currently used on Op HERRICK. On a weekly basis, medical facilities complete a spreadsheet
(or paper-based return where ICT support is not available) which, in HERRICK, is e-mailed to
HQ Joint Force Support (Afghanistan) (JFSp(A)), where returns are consolidated before
onward transmission to the ISAF chain of command and PJHQ. NATO has recently released
EPINATO 2; the UK has decided to continue to use EPINATO on Op HERRICK and to
introduce EPINATO 2 for contingency operations.
• Defence Statistics (Health) systems – DS (Health), formerly DASA (Health), provides a
number of in-house developed software applications in support of DMS activities and statistical
requirements, for example:
o Defence Patient Tracking System (DPTS) – the DPTS contains clinical data
related to patients who are the subject of a strategic Aeromedical Evacuation
NOTification of CASualty (NOTICAS) signal, and all those who enter a secondary care
physical rehabilitation pathway. The primary role of the system is incident-based
tracking of patients through their individual care pathways to a clinically-appropriate
secondary care facility. This serves to provide assurance to the DMS that the subject
patients are being suitably progressed along their pathways. Its secondary role is to
provide a single point of truth for patient care pathways and to provide an information
source for enquiries relating to service patient numbers, types of injuries etc.
o Automated Significant Event Reporting (ASER) System – developed to enable
the capture, processing and tracking of patient safety events. Undergoing trialling at the
time of writing.
o Dashboards – DS(Health) produces a number of bespoke statistical ‘Dashboards’
in varying formats, which are designed in conjunction with the customer e.g. Defence
Primary Health Care (DPHC). The base data is extracted from DMICP and various
other datasets within Defence and amalgamated to present the required information in
an accessible format.
• Defence Science and Technology Laboratory (DSTL) systems – DSTL provides a
number of in-house developed software applications in support of DMS operational planning
and statistical requirements. These will be captured during the Concept Phase in order to gain
a full scope of services required.
Programme Blueprint 3 20140620-cortisone-programme-blueprint-v1.doc6. In addition to the systems above, there are many spreadsheet, database, MOSS-based and manual solutions being used across the DMS that have been developed by different units, in isolation, to meet specific local needs. Much of the functionality provided by these unsupported applications and administrative systems is duplicated across the organisation in different formats. CORTISONE will seek to harmonize the core requirements for inclusion within its service offering. Programme Blueprint 4 20140620-cortisone-programme-blueprint-v1.doc
FUTURE STATE
OVERVIEW
7. The primary objective of the CORTISONE programme is to introduce coherence across the
breadth of the DMS information space and to enable seamless interoperability with the information
systems of partner and other supporting organisations, principally the NHS structures of the home
nations. This in turn enables the DMS to achieve their clinical outputs in a fully-informed, efficient
and effective manner, and to maximise the return on investment in clinical research programmes
and projects.
8. Coherence and interoperability across information systems:
• Provides timely access to accurate, up-to-date patient information in support of clinical
activities and diagnoses.
• Underpins clinical best practice through provision of integrated health and reference
information at the point of delivery of care.
• Ensures that data can be captured once, at source, and used for their primary and secondary
purposes across the organisation, regardless of host system configuration or location.
• Enables integration of deployed services into the DMS’ information mainstream.
STRATEGIC COMPLIANCE
9. CORTISONE will adhere to government and Defence strategic direction in designing and
implementing its information services. Figure 1 illustrates the ‘golden thread’ that links the
programme to overarching departmental strategy, and thus supports Defence outputs:
Figure 1 – Strategic ‘Golden Thread’
Programme Blueprint 5 20140620-cortisone-programme-blueprint-v1.doc10. The Cabinet Office has published the Government ICT Strategy 4 , which provides clear and
unambiguous direction on the standards to be adopted and approach to be taken when
considering the implementation of ICT solutions going forward. The key elements are:
• The mandated reuse of proven common application solutions.
• A move towards ‘cloud’ computing.
• A move away from sourcing via large systems integrators in favour of small to medium
enterprises (SMEs).
• Adoption of open standards to promote interoperability.
• A presumption against projects with a through-life estimated cost of £100m or higher.
11. This represents a step-change in the specifying and sourcing of public-sector information and
communication technology and provides a solid foundation on which to build next-generation DMS
information support services. The approach has been contextualised for Defence with the
publication of the Defence ICT Strategy 2013 5 . CORTISONE will fully align with both the
government and MOD ICT strategies. Additionally, Defence has created the Defence Information
Reference Model (DIRM) 6 , the purpose of which is to promote information and ICT re-use,
coherence, interoperability and open standards across the department. Reference to and full use
of the DIRM will also be made in specifying and designing service offerings.
12. In line with Cabinet Office and MOD Chief Information Officer (CIO) direction, CORTISONE
will, wherever possible, adopt a service-orientated approach to acquisition. All service component
solutions will be tightly integrated with the clinical and business capabilities and processes that
they are ultimately designed to support.
4
Reference Document A.
5
Reference Document B.
6
Defence Information Reference Model.
Programme Blueprint 6 20140620-cortisone-programme-blueprint-v1.docFUTURE MODEL
13. Future information support services for the DMS must be innovative, agile, efficient and
effective. In line with strategic direction, every effort will be made to avoid acquisition of highly-
bespoked information services that are expensive to develop and maintain, and are a barrier to
rapid adoption of technological developments.
14. JDP 4.03 7 sets out the 7 Capabilities of Care applicable on deployed operations:
a. Force Health Protection (FHP);
b. Primary Health Care and Dental Care;
c. Pre-Hospital Emergency Care (PHEC);
d. Medical Evacuation (MEDEVAC);
e. Deployed Hospital Care;
f. Medical C4I;
g. Medical Logistics.
The CORTISONE model will seek to deliver information services that provide full support across all
of these capabilities, allied with a comprehensive Firm Base provision that, combined, will underpin
patient-focused DMS activities and outputs end to end (E2E).
CORE COMPONENT – THE iEHR
15. The core business of the DMS is delivering military medical operational capability, the major
component of which is PHC as part of E2E healthcare provision. It therefore follows that the future
information support service must be designed around the iEHR. The iEHR is defined as a digital
collection of patient health information compiled at one or more clinical encounters in any care
delivery setting. It will be constructed using commercial off-the-shelf (COTS) software products
specifically designed to support primary health care service delivery, including support for
occupational and mental health.
16. Any military functionality deemed essential will be incorporated into sub-components that will
interface with the chosen COTS package. This approach ensures that the core health record
remains separate from (though related to) Defence-specific information and can therefore be
readily transferred to/from NHS or other provider systems as and when required, with the military
element remaining within the DMS information domain. It also simplifies procurement and reduces
the cost of implementing upgrades to COTS products, as the manufacturers’ standard
maintenance releases can be applied without a need for additional customisation.
17. The existing iEHR database will be exported from DMICP and used to populate the new PHC
support system, with the military elements extracted to populate the relevant sub-component(s).
The concept of a centralised data warehouse for the PHC record – as developed under the DMICP
initiative – remains a valid and essential part of the overall service architecture and will endure for
the foreseeable future. A key work stream when evaluating suitable COTS products will be
analysis of the underlying database structure to ensure that open standards can be applied and
used for data interrogation and exchange, and to guard against proprietary lock-in. Where
7
Reference Document G, Annex 2A-1
Programme Blueprint 7 20140620-cortisone-programme-blueprint-v1.docpracticable and possible, established commercial frameworks – within Defence; NHS England; or
wider UK Government – will be utilised to acquire CORTISONE capability.
18. The current DMICP solution has 2 variants: Firm Base and Deployed, the latter of which is
also used Afloat. The new iEHR solution will consist of a single service provision that has full utility
across all contexts and environments that the DMS is required to provide health, healthcare,
medical and dental support. It will present a common interface through which sub-systems can
easily and securely interoperate, linked via a unique patient identifier.
SUB-COMPONENTS
19. The following sub-components will interface with the iEHR to provide an information
capability that spans the DMS. Each will be capable of modular deployment and incremental
introduction to service. Similarly, each will be designed to be upgradeable discretely from other
service components, so that advances in technology can be taken advantage of with minimal risk
to the integrity of the wider system.
20. Figure 2 below provides a graphical representation of how component information services
will, where appropriate, interact with and update the core iEHR:
Figure 2 – Suite of Services
21. A fuller listing of sub-components, loosely arranged into functional groupings to aid clarity, is
shown below:
Programme Blueprint 8 20140620-cortisone-programme-blueprint-v1.docPRIMARY HEALTHCARE SUPPORT
• Fitness for Duty – a capability for recording PULHHEEMS (or any future classification
system) to enable decisions to be made regarding suitability for postings and roles, and
generation of Joint Medical Employment Standard (JMES) codes. This functionality exists
within recruiting support software applications, the reuse of which will be explored.
• Dental Imaging – a distinction is made between medical and dental digital imaging. Dental
practitioners capture and interpret radiographs in the primary healthcare environment as an
integral part of most routine consultations. Dental records, including ante mortem radiographs,
are frequently used in forensic human identification as odontology is an internationally
accepted primary identification criteria. There is currently no requirement for immediate wide-
area communication of dental images from deployed locations; however, a means by which
they can be stored, related to/incorporated with the iEHR and retrieved to support future
treatment decisions or investigations will be designed and developed.
• Near Real-Time Disease Surveillance (NRTDS) – a warning and reporting, tracking and
intervention capability for outbreaks of disease by time/place/person. To be enabled via close
coupling with the core EHR, NATO and Allies.
SECONDARY HEALTHCARE SUPPORT
• Digital Imaging – a vital part of Deployed Medical Care (DMC) provision on operational
deployments is an ability to capture and interpret radiograph, CT and other images to aid rapid
and often life-saving diagnosis. CORTISONE will provide an asynchronous means by which
images can be transmitted to consultants in the Firm Base for interpretation and for reports to
be returned, as there is no guarantee that a radiologist will be available in-Theatre. A fully
portable solution for the capture, recording and transmission of patient monitoring data will host
the service at the DMC MTF.
• Laboratory Information Management – functionality that is required to track and control
pathology requests and analyses, which can be related to the subject’s iEHR.
• Bed Management and Record Keeping – this is an important extension of the patient
administration capability that enables control and monitoring of bed allocation. Records of bed
occupancy are necessary in the investigation of disease outbreaks and cross-infection.
Acquisition of a suitable solution will replace the current manually-intensive methods, which are
prone to transcribing errors and do not provide an audit trail of bed usage.
PAN-HEALTHCARE SUPPORT
• Telemedicine – a synchronous service that will also incorporate a video-conferencing
capability that supports the provision of remote consultations, and additionally enables tele-
consultations to be conducted with forward-deployed clinicians. This also allows assurance of
junior doctors by appropriate senior doctors.
• Health Surveillance - a capability that enables the extraction of data from the iEHR, allowing
clinicians and other authorised users in medical headquarters to access and analyse
anonymised data sets. The requirement covers both diseases and health conditions.
• Pharmacy and Medicines Management – a solution for controlling and auditing the supply
of drugs and medicines, it will also provide clinical decision support functionality at the point of
delivery. A key component in delivering increased patient safety.
Programme Blueprint 9 20140620-cortisone-programme-blueprint-v1.doc• Clinical Research Repository – much of the valuable research undertaken by DMS staffs is
currently unavailable electronically to the wider Defence medical community. CORTISONE will
provide a means by which this material can be stored, indexed and retrieved across the
organisation for contextual use.
• Medical Equipment – enabling the capture at source of data generated through the use of
specialised medical equipment, and subsequent integration with the iEHR. This capability has a
close correlation with planned telemedicine functionality and will be developed to complement
and enhance the telemedicine service.
• Blood Supply Management – close control and accounting for blood products is mandatory
and of paramount importance on deployed operations. CORTISONE will provide a deployable
solution that can integrate with DHC MTFs and exchange information with the iEHR.
• Quality Improvement – a capability to capture near real-time clinical outcome data,
matched to detailed injury/illness mechanisms and diagnoses, physiology and interventions in
order to monitor and assure clinical performance at the individual patient and institutional level.
This capability is linked to the telemedicine function to provide reach forward direction and
reach back advice to enhance performance in the deployed medical treatment facility.
ADMINISTRATIVE AND BUSINESS SUPPORT
• Patient Tracking – an ability to track, in near-real time, the location of patients both
geographically and through their respective care pathways. This functionality will ensure that
patients complete their care programmes in a timely and effective manner, and mitigates the
risk of DMS staffs losing sight of individuals. There are a number of mature, in-house produced
systems within Defence that currently provide elements of this functionality (JTTR; DPTS;
WISMIS etc.) and there exists an opportunity to identify ‘best of breed’ for further development
and integration.
• Patient Administration – for use on deployment and in the Firm Base (primarily at DMRC,
Headley Court and/or the planned DNRC, Stanford Hall). The system will make use of the PHC
Master Patient Index (MPI) to maintain accuracy and avoid duplication of data. There are many
COTS packages on the open market that provide this functionality; key to product choice will be
scalability and flexibility regarding modules that can be added to the base system.
• Health Records Management – a large and complex area that has suffered from an
element of neglect in the past. The DMS are in the process of developing a new policy for the
management of health records and the CORTISONE solution will directly support its
implementation. The CHRL medical records archive contains valuable information that cannot
be readily exploited at present, thus leaving a gap in regard to epidemiological capability. The
future solution will ensure that metadata is clearly defined and rigidly applied as an integral part
of the archiving process, and that there is tighter integration with the wider DMS information
domain. This will include a link to the individual’s iEHR.
• Revalidation of Health Professionals – since 3 Dec 12, there has been a General Medical
Council requirement 8 for doctors to undergo revalidation, currently every 5 years, in order to
maintain their licence to practise in the UK. This will be extended to other health professional
groupings in the future. A number of COTS packages have been created to support this activity
and a scalable, flexible solution will be selected to meet the needs of the DMS. An ability to
interface with Defence personnel systems will be explored.
8
The General Medical Council (Licence to Practise and Revalidation) Regulations Order of Council 2012 (www)
Programme Blueprint 10 20140620-cortisone-programme-blueprint-v1.doc• Medical Data Interrogation – an essential capability that will enable cross-platform
interrogation of all electronic data repositories. It will be designed so that suitably authorised
system users can create and produce reports and reporting formats independently of the
service provider.
• Corporate Support – in order to allow clinical staffs to discharge their responsibilities in a
manner that is compliant with all legal and statutory requirements, with minimum encroachment
on their primary duties, a suite of information services in support of corporate administration
and governance activities will be designed. This will enable the analysis by HQ staffs of data
captured during routine clinical activities, whilst reducing the administrative burden on patient-
facing personnel. Correctly-specified services will promote continuous improvement activities
and provide reliable and consistent performance evidence against Key Performance Indicators
(KPIs).
22. All sub-components/information services will be designed to be device and platform-
independent where possible. This will enable access to DMS information services across a range
of End User Devices (EUDs) and promote the spiral acquisition of value-adding emerging
technology as and when it becomes available.
DMS INFORMATION DOMAINS
23. The CORTISONE suite of services will provide support, either directly or indirectly, for the
following domains of information, which the DMS routinely augment or require access to in the
production of their clinical and business outputs:
Domain Elements
Archived information Defence Health Records.
Business Intelligence Decision Support; Continuous Improvement.
Business Support KPIs; Compliance; Governance; Infrastructure;
Asset Management.
Clinical Administrative information Appointments Scheduling; Bed Management;
Hygiene; Staff Rotas.
Clinical Information PHC; SHC; Intermediary; Dental; Occupational;
Rehabilitation.
Clinical Research Outcome Information; Performance Information;
Force Protection Information; Reports and Papers
(outputs).
Deployability information Fitness for Duty; Fitness for Deployment.
Epidemiological information Analytical datasets.
Logistical information AEROMED & MEDEVAC; Blood Stocks; Pharmacy
Supplies and Restock; Medical Equipment
Movements & Serviceability States.
Personnel information DMS Service Personnel (Reserves tba); DMS
Civilian Personnel; PAR (Reserves tba).
Programme Blueprint 11 20140620-cortisone-programme-blueprint-v1.docQuality Improvement Registries for Major Trauma and Medical Illness;
Performance data (KPIs; actions taken following
significant events; clinical case conference
minutes; post mortem analyses; public enquiry
outcomes)
Strategy & Policy outputs Strategic Planning; Medical Policy.
Table 1 – Information Domains
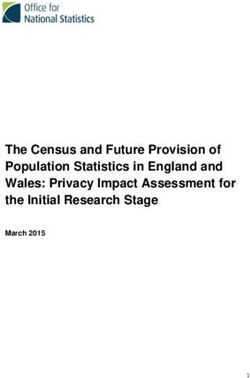
24. Figure 3 below provides a graphical representation of how these domains integrate with the
overarching CORTISONE model:
Figure 3 – Information Service Structure
INTERFACES
25. Central to the CORTISONE approach is an understanding that information should be entered
only once, at source, and then be made available for contextual use across the DMS information
domain and sphere of operations. This links in with the CTO’s and DBS Data Management
Services’ drive to identify producers and consumers of data, in order to ensure that there is ‘…only
one authoritative source for each type of master data.’ 9 Once established, authoritative data
sources (ADS) must be made available in open and common formats for exploitation i.e. data will
be shared unless there is a valid reason for not doing so. ADS custodians will also be responsible
for managing their data in such a way as to maintain quality and accuracy over time.
9
Reference Document B, page 17
Programme Blueprint 12 20140620-cortisone-programme-blueprint-v1.doc26. Defence Core Network Services (DCNS) will supply Enterprise Service Bus 10 (ESB)
functionality, which will provide the means by which CORTISONE service elements can co-
operatively interact, regardless of physical location or technical platform.
27. Much of the base information required by the DMS is created and held within other ADS
domains, both internal to and outside of Defence: robust and secure interfaces will be established
with each as necessary. Interoperability will be underpinned by a clearly-defined technical
specification for interface requirements, as mandated by the government and Defence ICT
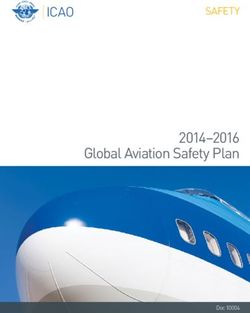
strategies, which will be strictly adhered to during service and solution design. Figure 4 below
provides a high-level schematic of a future interoperability model, with each ADS being provided
with its own Applications Hosting Environment (AHE).
Figure 4 – Authoritative Data Sources
10
Reference Document B, page 12.
Programme Blueprint 13 20140620-cortisone-programme-blueprint-v1.doc28. The CORTISONE suite of services will interface with:
• Defence civilian and military Personnel Administration systems and/or successor services –
JPA currently provides the definitive military personnel record within Defence; HRMS is its
civilian equivalent. Both provide key personal identifiable data.
• Defence logistics systems – to exchange information for AEROMED and MEDEVAC
operational requirements; tracking of medical equipment locations and maintenance states;
blood stock management; medical inventory management and stock control; pharmacy and
medicines management.
• NHS National Network (N3) spine (and/or successor services) – to commission secondary
care and to enable the exchange of the Defence iEHR with NHS service providers when
required; access to Choose & Book and other NHS services, both existing and planned. This
interface will also enable interaction with NHS trust systems where there is a military presence.
• Medical equipment supplier systems (including Medical & General Supplies (M&GS) Delivery
Team) – to enable an integrated approach to procurement, maintenance and monitoring.
• NATO, allies and other health service providers (including 3rd Sector organisations 11 ) – for
the exchange of health records (where authorised 12 ); medical planning, management and
support information; epidemiological data.
• Wider UK Government departments – for the exchange of statistical and other information as
required.
11 rd
The Oxford Dictionary defines the 3 Sector as: ‘The part of an economy or society comprising non-governmental and non-profit-
making organizations or associations, including charities, voluntary and community groups, cooperatives, etc.’
12
There is uncertainty at time of writing as to whether member-state agreement on NATO iEHR exchange can be achieved.
Programme Blueprint 14 20140620-cortisone-programme-blueprint-v1.docFigure 5 - Interfaces
29. CORTISONE services will also extend into:
• The Defence Statistics (DS(Health)) organisation – for the exploitation of health information
to support the delivery and continuous improvement of health and healthcare services.
• DSTL – for the exploitation of health information for Operational Analysis, to inform
Operational Medical Planning.
30. All CORTISONE services will present a standards-based interface that can be readily utilised
for any future, as-yet unidentified interoperability requirement. The standards mandated for
Defence and government are outlined later in this document.
NHS ALIGNMENT
31. A key strategic objective of the DMS is the strengthening of relationships with the NHS. An
important element in shaping the future CORTISONE landscape is therefore alignment with
planned information initiatives across the NHS organisations of the UK 13 . The Department of
Health has published its information strategy 14 for NHS England, and CORTISONE service design
will be fully informed by the direction provided therein, together with corresponding initiatives in
Scotland 15 , Wales and Northern Ireland.
COMMUNICATIONS INFRASTRUCTURE
13
Reference Document C, para 16, sub-para c (1).
14
Reference Document F.
15
It is recognised that the relationship with NHS Scotland may necessarily change depending upon the outcome of the Scottish
independence referendum in Sep 14.
Programme Blueprint 15 20140620-cortisone-programme-blueprint-v1.doc32. The global nature of DMS deployment demands a global reach for supporting information
services. CORTISONE services will therefore be designed and developed in close liaison with
Defence technical authorities to ensure full compatibility with Defence communications
infrastructures, both existing (principally DII Fixed, Deployed and Maritime) and planned (DCNS)),
and deployed Combat Net Communications; to include an appropriate Reach-Back capability.
33. Services designed for use on deployment will require an integrated networking component to
enable the capability to operate ‘out of the box’ in environments where this provision cannot be
guaranteed.
34. Cognisant of the need for cross-Governmental and inter-departmental communication, those
service elements that can be hosted in the government secure cloud will be designed so to be.
SERVICE ACCESS
35. The service interface presented to the end-user will allow access to all functionality, service
components and information commensurate with their role and responsibilities, in a seamless and
coherent manner, via a single login. With the introduction of common, Defence-wide Enabling
Technical Services under DCNS, this will be achieved through utilisation of the Identity and Access
Management (IdAM) service. IdAM is ’…an integrated set of policies, processes, standards and
technologies that create and manage digital identities and associated access privileges for all
people and other entities within an organisation and over the whole lifecycle of activity 16 .’
TECHNICAL STANDARDS
36. Adherence to common, agreed standards is critical to future CORTISONE service
interoperability across Defence and the wider stakeholder community. CIO has mandated 17 that all
Defence ICT programmes must apply the following standards hierarchy, in the order shown, when
designing and implementing ICT solutions and information services:
• Open standards, including International Standards and the Cabinet Office ‘Open Data
Standards Process’.
• NATO standards.
• British Standards Institute standards.
• Other Government standards.
• Proprietary standards; prior agreement to each application of proprietary standards must be
sought from the Network Authority.
37. The CORTISONE suite of services will be designed in accordance with this direction. In
particular, proprietary standards will be avoided unless there is absolutely no viable alternative.
GAP ANALYSIS
38. Annex B provides a Gap Analysis, which has been cross-referenced with the strategic
objectives of the DMS. Whilst not exhaustive, it aims to:
• Highlight the major areas where an information capability shortfall has been clearly identified;
16
Reference Document B, page 11.
17
Reference Document B, page 17.
Programme Blueprint 16 20140620-cortisone-programme-blueprint-v1.doc• Provide a focus for initial programme planning and project identification.
INTERMEDIATE STATE AT END OF TRANCHE 1 – TARGET DATE: 30 APR 2015
39. Tranche 1 will concentrate on producing the deliverables required from the Concept Phase of
the CADMIT 18 programme/product life-cycle. Key tasks will include:
• Identification, analysis and justification of resourcing requirements for Concept Phase;
• Development of ABC funding options;
• Stakeholder identification and initial engagement;
• Establishment of programme structure;
• Assessment of programme governance requirements.
END STATE – TRANCHE 1
40. Tranche 1 will not address business change issues, which will be further developed during
future stages of the programme. At the end of Tranche 1 the SG CORTISONE Team, in
conjunction with Cap C4ISR, DIST and the wider DMS stakeholder community, will have:
• Created a programme plan;
• Established a programme governance structure;
• Identified the major component elements of the CORTISONE programme;
• Identified candidate options for assessment as possible projects;
• Developed a programme Risk Management strategy;
• Clearly articulated expected programme benefits and how they are to be achieved;
• Consolidated all relevant reference material into a central ‘Lessons Learned’ repository;
• Developed and refined an acceptable ABC funding option for the Concept Phase;
• Decided upon a viable Procurement Strategy;
• Within an Enterprise Architecture framework, prioritised and initiated business process
mapping and data-flow analysis work streams;
• Initiated production of CONEMPs for priority capability requirements;
• Produced Initial Gate business cases for the following projects:
o ACTUARY;
o INTERMOLAR;
18
Concept; Assessment; Demonstration; Migration; In-service; Termination.
Programme Blueprint 17 20140620-cortisone-programme-blueprint-v1.doco REBRACE;
o Records Archiving (awaiting official name allocation).
• Written and implemented an effective programme Communications Strategy and Plan.
Successful completion of Tranche 1 will provide a robust programme organisation and governance
structure, a clear vision of high-level benefits, and a framework for taking forward work under
follow-on phases.
INTERMEDIATE STATE AT END OF TRANCHE 2 – TARGET DATE: 31 DEC 2016
41. The core deliverable for Tranche 2 is continued provision of a Defence iEHR capability
following cessation of the DMICP contract in April 2016, which is being taken forward under Project
INTERMOLAR. Procurement of a future iEHR service will go ahead under CORTISONE (Project
REBRACE) using processes mandated by the Defence Acquisition Operating Framework (AOF),
and within the timelines and constraints determined by EU Legislation. In the meantime, it will be
necessary to maintain current capability, or a facsimile thereof delivered by Project INTERMOLAR,
until such time as the future iEHR service has been designed and developed, and can be reliably
delivered to all required locations. The principal business beneficiaries of INTERMOLAR will be
DPHC.
42. Successful delivery of INTERMOLAR will:
• Maintain capability and existing service levels, in the Firm Base and deployed environment;
• Maintain patient records, in accordance with MOD and statutory body requirements;
• Maintain patient confidentiality, in accordance with DPA 1998 and Caldicott principles;
• Maintain availability and integrity of records, across clinical environments;
• Maintain prompt and efficient record retrieval;
• Maintain health and healthcare information gathering capability;
• Maintain epidemiological investigation and research capabilities;
• Maintain interoperability with Defence information systems and infrastructure;
• Maintain connection with the N3 Spine;
• Maintain electronic services with the NHS;
• Ensure compliance with MOD and NHS Policies and Standards.
43. As the INTERMOLAR project is not seeking to extend or enhance current capability it is
envisaged that DPHC business and operational processes/functions will not need to change.
Similarly, the management and organisational structures of the beneficiary business units will
remain as at present.
44. Project REBRACE – a Defence iEHR that enables health and healthcare information to be
captured, integrated, accessed and maintained across all DMS clinical environments. Start-up and
Initiation phases completed. Project Board, Project Team, Project Plan and associated Stage
Plans in place. Funding issues resolved and significant progress made towards defining the
products and services required to provide the capability, together with a clear procurement
strategy.
45. Project ACTUARY – a fully-scalable and deployable medical information capability for
deployed hospital care, which will include support for, though not necessarily be limited to:
Programme Blueprint 18 20140620-cortisone-programme-blueprint-v1.doc• Patient administration (incl. bed management);
• Radiology (incl. dental);
• Pathology;
• Clinical information;
• Medicines management;
• Internal & external communications infrastructure.
46. With HERRICK drawdown due in 2014 it is imperative that ACTUARY provides as many of
the required capabilities as possible ahead of full withdrawal, as the DMS’ focus returns to
contingent operations. Target date for completion of the project is end-Dec 2016.
47. Whilst ACTUARY will provide an encapsulated deployable capability, its constituent parts, if
correctly specified, will have utility in a number of other DMS clinical contexts. This will necessitate
careful planning, design and contracting to ensure that reuse of components is possible, thus
realising the benefits of the programme approach.
PRELIMINARY DLOD EVALUATION – TRANCHE 2 (to be examined in detail during Assessment
Phase)
48. Interoperability – The CORTISONE programme approach is designed to provide cohesion
across the breadth of the DMS’ information systems and those of the wider MOD; the NHS
organisations of the home countries; allies, and other partner organisations. A key deliverable of
Tranche 2 will be the implementation of Government and Defence ICT Strategy-mandated
standards that clearly and unambiguously set out the technical and administrative pre-requisites for
participation, and thus guarantee interoperability. This will ensure that future information services
can seamlessly interface with each other, duplication of data is avoided, and health information
exploitation can be achieved across the full portfolio of datasets.
49. Training – DMSTG (DCHET) will continue to provide iEHR training for the user community,
as is currently the case for DMICP. Dependent upon the eventual solution, there may be a ‘train
the trainer’ requirement for the interim capability provided by INTERMOLAR, with a new course
design required. The eventual training solution will require a period of assessment before being
formally introduced. Training in the use of ACTUARY-provided capability will be undertaken at the
2 Med Bde deployed hospital facility, Army Medical Services Training Centre (AMSTC), Strensall
Barracks as an integral part of the Mission Ready Assessment (MRA) contingency-readiness
confirmation process.
50. Equipment – End-user access devices currently in place on DII and, where applicable,
legacy infrastructures will continue to be used to access the INTERMOLAR service. Again, the
eventual service model will dictate whether there is a need to procure/replace back-end server
equipment/software. ACTUARY will almost certainly require the acquisition of additional equipment
and software to provide the required capability.
51. Personnel – The supplier selected to deliver INTERMOLAR must ensure that an optimum
number of sufficiently skilled personnel is in place to operate the service efficiently and effectively.
52. Infrastructure – Dependent upon the INTERMOLAR solution, there may be a need to host
back-end servers on MOD property, which would necessitate evaluation of, and possibly changes
to the preferred location. ACTUARY may involve a change requirement to the configuration of
infrastructure provided for training at Strensall Barracks.
53. Concepts & Doctrine – Documentation for ACTUARY to be developed in conjunction with
Cap C4ISR, DIST and the user community.
Programme Blueprint 19 20140620-cortisone-programme-blueprint-v1.doc54. Organisation – Potential changes to organisational structures will be identified in
conjunction with DMS management and business pillars.
55. Information – The Defence iEHR (currently DMICP) database will be reused to provide the
core information repository for INTERMOLAR services. Provision for this is made as part of the
DMICP exit strategy.
56. Logistics – The core data necessary to ensure continuity of the iEHR service may need to
be migrated to a new hardware platform/location.
END STATE – TRANCHE 2
57. Tranche 2 is not designed to deliver fundamental changes to the structure, organisation or
clinical business processes of the DMS. Rather, it will ensure that the DMS can continue to
produce their clinical outputs in a safe, effective and legally-compliant manner until such time as
the major CORTISONE components are successfully delivered under future tranches. At the end
of Tranche 2, the DMS will have:
• Retained the centralised iEHR capability that underpins patient safety in the delivery of
clinical outputs, with minimal (if any) additional personnel training requirement;
• Retained business organisational structures and clinical processes/functions (although other
non-CORTISONE restructuring activities, as yet unknown, may be initiated during this period);
• Consolidated interconnectivity and interoperability with the NHS;
• Acquired a scalable, robust, fully portable and deployable medical information capability, the
component parts of which can be reused across the CORTISONE programme;
• Established Project REBRACE, which will form the central pillar of Defence medical
information capability for the future.
58. Successful completion of Tranche 2 will provide a firm foundation on which to build the major
component elements of the programme.
INTERMEDIATE STATE AT END OF TRANCHE 3 – TARGET DATE:
59. The component elements of Tranche 3 will be further developed over the next 6-10 months.
Business and clinical priorities will dictate the structure and content of this phase of the
programme, as will funding profiles.
FINAL STATE AT END OF FINAL TRANCHE
60. Narrative to be developed, to include:
• Description of business structure and major clinical processes/functions post-implementation
of CORTISONE component project outputs;
• Description of new services and enabling technologies, including service levels and
operating costs when known;
• Description of technical/service architecture to be adopted.
Programme Blueprint 20 20140620-cortisone-programme-blueprint-v1.docANNEX A TO
CORTISONE BLUEPRINT V 1.0
DATED 20 JUN 14
DMS – CURRENT STATE
1. The DMS’ current structure, and the primary business pillars that are likely to be directly
impacted by the CORTISONE programme, is described below.
Surgeon General (SG)
2. SG is the 3-star Defence Authority for End-to-End (E2E) Healthcare and Medical Operational
Capability, and is the professional head of the DMS. He directly oversees the Joint Medical
Command (JMC) and Defence Primary Health Care (DPHC). SG has ultimate responsibility for
delivering the 3 core outputs of the DMS, as articulated in the DMS sub-Strategy and its
accompanying Strategic Plan:
• Medical Support to Operations – Developing and generating deployable medical capability;
interoperable with our multi-national partners and capable in an increasingly complex mission
space, in order to promote, protect and restore the health of deployed forces.
• Healthcare – Delivering safe, effective, seamless and resource-efficient healthcare across
Defence, either directly or through partners, in order to restore the health of Service personnel.
• Expert Medical Advice – Providing specialist advice on Health and Healthcare to the Chain of
Command, in order to promote and protect the health of the Armed Forces.
Assistant Chief of Defence Staff (Health) (ACDS(H))
A –1ANNEX A TO
CORTISONE BLUEPRINT V 1.0
DATED 20 JUN 14
3. ACDS(H) is the 2-star officer who provides the key health and healthcare interface within HQ
SG and more broadly acts as the cross-cutting health lead within Defence and its relationships with
other governmental departments. He works directly in support of SG but reports to the Chief of
Defence Personnel (CDP), the designated Defence Authority for People, on health issues relating
to Service personnel policies; and to DCDS (Mil Strat & Ops) on delivery of medical operational
capability.
4. A key output of ACDS(H)’s area is medical strategy and policy, which provides the
framework and direction for delivery of the DMS’ core clinical outputs. This, in turn, creates the
environment in which the CORTISONE suite of services must be designed to operate.
Joint Medical Command (JMC)
5. The JMC provides support to the Permanent Joint Headquarters (PJHQ), single Services,
Director Special Forces (DSF) and other Joint users in providing medical operational capability,
healthcare, education, training and research in order to maximise fighting power and medical
excellence within the armed forces. JMC supports the provision of continuously improving
healthcare on operations, including contingency, and in peacetime. It builds on past training and
research achievements and develops ways of capturing operational evidence and lessons. This is
to ensure that all such lessons are incorporated at the earliest opportunity into the training given to
personnel deploying on operations and into the treatment at every level of the Defence Population
at Risk (PAR). The JMC high-level organisational structure is shown below:
A –2ANNEX A TO
CORTISONE BLUEPRINT V 1.0
DATED 20 JUN 14
Defence Medical Group (DMG)
6. The DMG Mission statement is:
‘To provide highly capable Secondary Health Care (SHC) personnel for operations and to deliver
the operational Role 4 pathway in order to support the physical and moral components of Fighting
Power. Concurrently to coordinate all non-PHC military patient care pathways in the UK in order to
ensure Defence requirements are met’.
7. The DMG has responsibility for managing the patient care pathway within the Role 4 Medical
Group, which encompasses the Royal Centre for Defence Medicine (RCDM) Clinical Unit,
Birmingham; 5 (4 from 1 Apr 14) MOD Hospital Units (MDHUs); and the Defence Medical
Rehabilitation Centre (DMRC) at Headley Court. This also involves implementing a robust patient
tracking regime for all operational casualties. DMG has wide-ranging contact with the NHS in order
to establish high-quality placements for DMS SHC personnel to maintain their readiness for
operational deployment. The organisational structure is shown below:
A –3ANNEX A TO
CORTISONE BLUEPRINT V 1.0
DATED 20 JUN 14
8. DMG has responsibility for operating the Defence Patient Tracking Cell (DPTC) and its
current supporting software application, the Defence Patient Tracking System (DPTS). The DPTS
is further described under DMS Information Systems below.
Medical Directorate
9. The 1* Medical Directorate is currently based within the Joint Medical Command. This
position requires routine engagement and acceptance of taskings directly from across SGs HLB;
most notably with ACDS(H) and the Surgeon General. This is a unique position within SGs HLB.
Now that Defence Primary Health Care (DPHC) is established, a further Command relationship
with Commander DPHC and his HQ is developing. The forthcoming changes to the Top Level
structures of the Defence Medical Services (DMS) will see the Medical Directorate move under the
new 2* Director Medical Operational Capability & Policy.
10. The frequency and complexity of injuries inflicted on our Service personnel places demands
for skills which require intelligent investment in training and education, informed by research. The
environment in which our personnel operate requires appropriate military competencies that need
to be delivered by a suitably structured, resourced and led training organisation. The need to
prepare personnel for operations both militarily and clinically within a hostile and austere
environment requires constant refinement and development that the Medical Directorate is central
to.
11. The Medical Directorate mission is to both:
a. SUPPORT Defence with expert clinical advice in order to PROMOTE, PROTECT
and RESTORE physical and mental health; and PLAN, EXECUTE and SUSTAIN
operations with minimal risk and optimal clinical care. This will be achieved through:
(1) Defence Consultant Advisers.
(2) Defence Advisers (General Practice, Nursing, Dental).
(3) Defence Specialist Advisers.
and
A –4You can also read