Promoting Health and Cost Control in States: How States Can Improve Community Health & Well-being Through Policy Change - Maryland ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Promoting Health and
ISSUE REPORT
Cost Control in States:
How States Can Improve Community
Health & Well-being Through Policy Change
OPEN
Organic
FEBRUARY 2019
Acknowledgements
Trust for America’s Health (TFAH) is a nonprofit, nonpartisan Trust for America’s Health gratefully acknowledges generous
public health policy, research, and advocacy organization that financial support from the Robert Wood Johnson Foundation
promotes optimal health for every person and community and and Kaiser Permanente. Any opinions, findings, conclusions, or
makes the prevention of illness and injury a national priority. recommendations expressed in this material are those of the
authors and do not necessarily reflect the views of the funders.
TFAH BOARD OF DIRECTORS ADVISORY GROUP
Gail Christopher, DN Octavio Martinez, Jr. MD, DrPH, This report benefited from the insights and expertise of the following
Chair of the TFAH Board MBA, FAPA Advisory Group members. Although they have reviewed the report, neither
President and Founder, Ntianu Executive Director they nor their organizations necessarily endorse its findings or conclusions.
Center for Healing and Nature Hogg Foundation for Mental Health
Chris Aldridge, MSW Anand Parekh, MD, MPH
Former Senior Advisor and Vice The University of Texas at Austin
Senior Advisor Chief Medical Advisor
President, W.K. Kellogg Foundation
Karen Remley, MD, MBA, National Association of County & Bipartisan Policy Center
David Fleming, MD MPH, FAAP City Health Officials
Catherine D. Patterson, MPP
Vice Chair of the TFAH Board Former CEO and Executive Vice
Jeremie Greer, MPP Managing Director, Urban Health
Vice President of Global Health President
Vice President, Policy & Research and Policy
Programs American Academy of Pediatrics
Prosperity Now de Beaumont Foundation
PATH
John Rich, MD, MPH
Robin Hacke, MBA Marcus Plescia, MD, MPH
Robert T. Harris, MD Co-Director
Executive Director Chief Medical Officer
Treasurer of the TFAH Board Center for Nonviolence and Social
Center for Community Investment Association of State and
Senior Medical Director Justice
Territorial Health Officials
General Dynamics Information Drexel University Shelley Hearne, DrPH
Technology President Elizabeth Skillen, PhD, MS
Eduardo Sanchez, MD, MPH
CityHealth Senior Advisor
Theodore Spencer Chief Medical Officer for
Policy Research, Analysis and
Secretary of the TFAH Board Prevention and Chief of the Center Sandra Henriquez
Development Office
New York, NY for Health Metrics and Evaluation Former Chief Operating Officer
Office of the Associate Director
American Heart Association Rebuilding Together
Stephanie Mayfield Gibson, MD for Policy and Strategy
Senior Physician Advisor and Umair A. Shah, MD, MPH Chrissie Juliano, MPP Centers for Disease Control and
Population Health Consultant Executive Director Director Prevention
Harris County, Texas Public Health Big Cities Health Coalition
Cynthia M. Harris, PhD, DABT Brian Smedley, PhD
Director and Professor Vince Ventimiglia, JD John B. King, JD, EdD Co-founder and Executive Director
Institute of Public Health Chairman, Board of Managers President and Chief Executive National Collaborative for
Florida A&M University Leavitt Partners Officer Health Equity
The Education Trust
David Lakey, MD Kendall Stagg, JD, MPP
Chief Medical Officer and Vice Howard Koh, MD, MPH Director of Community Health
Chancellor for Health Affairs Harvey V. Fineberg Professor Kaiser Permanente
The University of Texas System of the Practice of Public Health
Jennifer Sullivan, MHS
Leadership, Department of Health
Senior Policy Analyst
Policy and Management
Center on Budget and Policy
REPORT AUTHORS CONTRIBUTORS Harvard T. H. Chan School of
Priorities
Public Health
Adam Lustig, MS John Auerbach, MBA
Fred Zimmerman, PhD
Manager, Promoting Health & Cost President and Chief Executive Officer Donna Levin, JD
Professor, Department of Health
Control in States (PHACCS) National Director
J. Nadine Gracia, MD, MSCE Policy and Management & Center
The Network for Public Health Law
Marilyn Cabrera, MPH Executive Vice President and Chief for Health Advancement
Policy Associate, Promoting Health Operating Officer Giridhar Mallya, MD, MSHP UCLA Fielding School of Public
& Cost Control in States (PHACCS) Senior Policy Advisor Health
Julia Sabrick
Robert Wood Johnson Foundation
TFAH Intern
Shauneequa Owusu, MS
Senior Vice President of Innovation
TFAH wishes to recognize and thank Lindsay Cloud and Scott Burris and Impact
of Temple University’s Center for Public Health Law Research for ChangeLab Solutions
their collaboration and contributions to this report.
2 TFAH • tfah.org
Table of Contents
contents
TABLE OF CONTENTS
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Report Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
GOAL 1: Support the Connections Between Health and Learning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Policy Recommendation 1a: Universal Pre-Kindergarten Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Policy Recommendation 1b: Enhancing School Nutrition Programs and Standards . . . . . . . . . . . . . . . . . 19
GOAL 2: Employ Harm-Reduction Strategies to Prevent Substance Misuse Deaths and Related Diseases . . 22
Policy Recommendation 2a: Syringe Access Programs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
GOAL 3: Promote Healthy Behavior . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Policy Recommendation 3a: Smoke-Free Policies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
Policy Recommendation 3b: Tobacco Pricing Strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
Policy Recommendation 3c: Alcohol Pricing Strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
GOAL 4: Promote Active Living and Connectedness . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Policy Recommendation 4a: Complete Streets . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
GOAL 5: Ensure Safe, Healthy, and Affordable Housing for All . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Policy Recommendation 5a: Housing Rehabilitation Loan and Grant Programs . . . . . . . . . . . . . . . . . . . . 43
Policy Recommendation 5b: Rapid Re-Housing Programs/Housing First . . . . . . . . . . . . . . . . . . . . . . . . 45
GOAL 6: Create Opportunities for Economic Well-Being . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49
Policy Recommendation 6a: Earned Income Tax Credit . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
Policy Recommendation 6b: Earned Sick Leave . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
Policy Recommendation 6c: Paid Family Leave . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
Policy Recommendation 6d: Fair Hiring Protections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
Related Policies and Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62
Current State Policies Table . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
FEBRUARY 2019
3
Executive Summary
EXECUTIVE
GOAL 1: Support
Despite advances in healthcare, too many Americans will continue to needlessly fall ill unless we
change the conditions that contribute to poor health. Adopting policies that improve access to
quality education, safe housing, jobs, and more can have lasting effects on individual health.
SUMMARY
the Connections Between Health and Learning
The circumstances we all encounter in our everyday lives
shape our health. Whether it’s where we live, how we eat,
GOAL 1: Support the Connections
where we go to school, our workplaces, who we care for, or
Between Health and Learning
what opportunities we have (or don’t have) to succeed, it all
1a. Universal Pre-Kindergarten Programs
has a profound effect on long-term health—regardless of
what type of medical care we receive. 1b. Enhancing School Nutrition Programs and
Standards
The United States spends trillions of dollars a year on health,
but currently more of that money goes toward treating
disease than it does to preventing it. Prevention starts with GOAL 2: Employ Harm-Reduction
people leading a healthy lifestyle, yet for too many Americans, Strategies to Prevent Substance Misuse
poverty, discrimination, access to education, the immediate Deaths and Related Diseases
environment, and other systemic barriers make it difficult to 2a. Syringe Access Programs
prioritize a healthy lifestyle and even more difficult to lead one.
Fortunately, state-level decision makers are in a strong position
GOAL 3: Promote Healthy Behavior
to change the conditions in which people live, work, learn, and
play. They can prevent the onset of disease, help residents lead 3a. Smoke-Free Policies
healthier lives, lower healthcare costs, and increase productivity 3b. Tobacco Pricing Strategies
by removing obstacles and expanding opportunities. 3c. Alcohol Pricing Strategies
But in an age of endless information, identifying the most
effective and efficient strategies for improved health and GOAL 4: Promote Active Living and
reduced healthcare costs can seem like an impossible and Connectedness
overwhelming task. Trust for America’s Health (TFAH)
4a. Complete Streets
created Promoting Health and Cost Control in States: How States
Can Improve Community Health & Well-being Through Policy
Change, to pinpoint evidence-based policies and provide state GOAL 5: Ensure Safe, Healthy, and
leaders with information on how to best promote healthy Affordable Housing for All
lifestyles and control costs. 5a. Housing Rehabilitation Loan and Grant
This report is the first product of the PHACCS initiative, it Programs
identifies policies for good health that look beyond healthcare, 5b. Rapid Re-Housing Programs/Housing First
part of a larger effort to foster cross-sector collaboration;
because, changes to any given policy area can impact the
GOAL 6: Create Opportunities for
population’s well-being and states’ ability to control costs.
Economic Well-Being
Additionally, PHACCS recognizes the value of state- and local-
level collaboration and includes considerations for those 6a. Earned Income Tax Credit
FEBRUARY
relationships so that policy can be implemented successfully. 6b. Earned Sick Leave
FEBRUARY
PHACCS acknowledges that the needs of every state are unique 6c. Paid Family Leave
and therefore provides a range of options for each state to 6d. Fair Hiring Protections
consider. Specifically, this report supports the following goals
2019
2019
and policies for states:
4 TFAH • tfah.org
Introduction
several evidence-based policies that
MARY JOHNSON’S STORY can be implemented to address these
hurdles and reduce health disparities.1
Mary Johnson sat in her doctor’s doctor recommended. What’s more,
office at the end of her physical exam. she didn’t feel safe exercising in her The United States is spending more and
She listened patiently as her doctor neighborhood. The YWCA was a few more on healthcare services to treat
carefully reviewed her current health miles away, but there wasn’t an easy disease. Yet spending on the drivers of
status, which included the fact that she way to get there by mass transit. And good health—quality housing, healthy
was 20 pounds overweight, prediabetic, she already knew the main trigger for foods, and education—is stagnant.
and asthmatic. The doctor reviewed her asthma: her apartment building had Residents of other countries that have
the importance of a healthful diet and a leaky roof, which resulted in mold and higher ratios of spending on social
physical activity as well as avoiding mildew. The landlord, however, wasn’t services to spending on healthcare
the environmental triggers for her inclined to fix the problem, and Mary services have better health and live longer
asthma. Mary liked her doctor and couldn’t afford to move. despite the U.S. spending more money
appreciated the doctor’s concerns. per capita on medical services than any
She ended the appointment with her other country.2,3 Healthcare spending
But she knew it would be difficult to
doctor by smiling and saying she’d is the second largest component of
make the necessary changes to her
try to adopt all the recommended states’ general fund spending, tends to
behavior. There were few local stores
behaviors. She did want to be grow at rates greater than inflation, and
that sold fresh fruits or vegetables
healthier. But she also knew those focuses on treating illness rather than
in her community. And besides, she
changes were not realistic. There were prevention. In 2018, Medicaid made up
was on a tight budget and the most
just too many obstacles in her way. an estimated 20.2 percent of all states’
affordable foods weren’t the ones her
general fund spending and grew at a rate
of 7.3 percent.4 Increasing investments in
This story will sound familiar to many policies that improve education, housing, prevention to complement the significant
Americans. No matter how good their transportation, and more. investments already being made in
medical care or how motivated they are disease treatment can promote health,
As illustrated by Mary Johnson’s case, the
to get healthier, the conditions present lower healthcare costs, and increase
social and economic factors related to
in many Americans’ lives prevent them productivity. Changing conditions to
where people live, learn, play, and work
from reaching optimal health. ensure that everyone has the opportunity
are interconnected and significantly
to make healthy choices requires
The ability to promote the health and impact health. Unfortunately, for
collaboration across fields and specialties.
well-being of the Mary Johnsons of the too many Americans, a lack of basic
That’s how the nation will weave together
world rests more and more with local resources like nutritious foods or
a culture of health.
and state policymakers than it does quality housing have resulted in poor
with the medical community. While the health. Certain populations, including Though state policymakers are in the
healthcare sector plays an important role racial and ethnic minorities, sexual best position to drive meaningful policy
in providing necessary health services to and gender minorities, people living in change, it is difficult to sift through
individuals, most of the factors that keep poverty and in rural communities, and reams of studies and ascertain which
people healthy are outside of healthcare formerly incarcerated individuals often policies work and which don’t. To
providers’ areas of expertise and control. have worse health outcomes than other provide state leaders with timely and
But state policymakers are in a position groups. These inequities in health can relevant information, TFAH identified
to ensure that everyone living in their often be attributed to differences in the strongest evidence-based policies
state has the opportunity to remain living conditions, exposure to traumatic from around the country. We scoured
healthy, to prosper, and to reach their full events, and access to needed resources several nationally recognized databases
potential. To make these opportunities in their community, which in many cases and reviewed hundreds of initiatives to
a reality, state leaders must change how are a result of discriminatory policies develop an easy-to-use single report and
they think about health and advocate for and practices. Fortunately, there are resource hub for state policymakers.
TFAH • tfah.org 5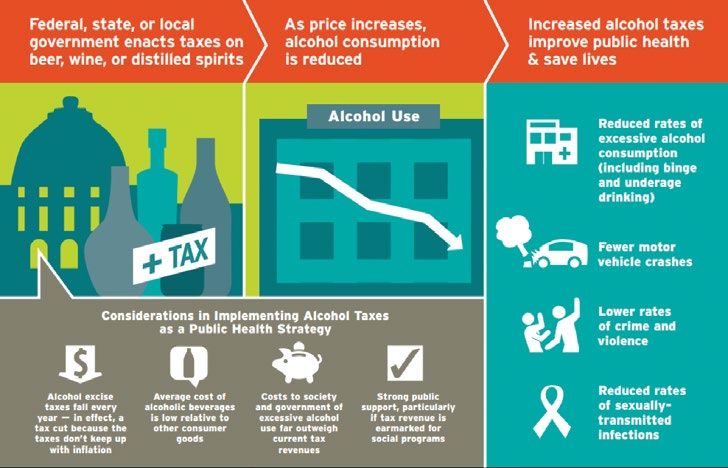
What’s in This Report? How to Use This Report
Promoting Health and Cost Control in The policies highlighted in this report important national trends related to
States: How States Can Improve Community provide a menu of options for state demographic shifts, health challenges,
Health & Well-being Through Policy leaders to explore as they consider and the wide range of factors that
Change strengthens officials’ capabilities how to best use their state’s resources influence an individual’s health.
by highlighting evidence-based and to improve the health and well-being This can help decision makers better
-informed policies that can improve of their population. The PHACCS understand why the recommended
health and well-being in their states. initiative recognizes that each state has policies in this report are so valuable.
PHACCS also focuses on state-level its own priorities and political dynamics
policies that can control healthcare to consider. This report was crafted National Trends
costs. We look beyond the healthcare specifically to cater to the needs of all
Life Expectancy
system, since policies in other sectors state policymakers and it is our hope
can also improve health and states’ that all states can consider at least one of Overall, Americans are growing older
budgets over time. This report looks the policies included in this report. This and becoming more diverse. In the
beyond medical procedures and report is intended to guide state officials last decade, the life expectancy at birth
clinical services and focuses instead on toward the best evidence-based policies in the United States rose from 77.8
opportunities to improve how people that promote health and well-being. to 78.6 years.5 However, disparities in
live, learn, work, and play. The report life expectancy by race and ethnicity
Case examples in this report highlight still exist. In 2016, the life expectancy
identifies policies that:
how some states have adopted a of Black Americans was 74.8 years,
l leverage the connection between recommended policy; this provides significantly lower than the expectancy
health and learning, decision makers with added insight for Latinos (81.8 years) and Whites
into how a policy was designed and (78.5 years). While this gap closed
l romote healthy living and
p
implemented. Each recommended over the past few decades, Black life
connectedness through the built
policy is also accompanied by a list of expectancy continues to significantly lag
environment,
considerations for effective design and behind all other races and ethnicities.6
l foster healthy behaviors, implementation to provide additional
guidance and suggestions for officials. Disparities in life expectancy are also
l s upport healthy and affordable widening between high- and low-income
Together, the policy recommendations,
housing, and earners. Men in the top 1 percent of
case examples, and considerations in
l create economic opportunities. this report can be used to inform policy household income live 14.6 years longer
proposals that can be enacted and than men in the bottom 1 percent.
This report provides detailed information While the gap for these two income
implemented by individual states to
on its recommended policies, including groups is smaller for women (10.1
promote health.
descriptions of the policies, summaries years), this persistent disparity shows
of the health and economic evidence, This report is just the start. TFAH that significant barriers remain for low-
case examples of policy implementation, looks forward to identifying more income individuals to live healthier,
and considerations for implementation. opportunities to support states interested longer, and more productive lives.7
Additionally, This report highlights a in making these policy changes. We will
set of complementary policies for state continue to provide states with additional Emerging and Continuing
officials to consider in recognition that resources to guide implementation, Health Issues
the recommended policies alone may not support recommendations, and find new
In recent years, life expectancy
be able to achieve state and national goals strategies for better health.
has decreased, which can be
for health promotion. These evidence-
Assessing what issues are affecting partly attributed to an increase in
based initiatives have the potential to
the state’s population is an important unintentional injuries, including
improve population health and can
first step for policymakers seeking drug overdoses, alcohol poisoning,
be used as either a complementary
to implement policy changes. In and suicide among young people.8
approach or as an alternative option to
the following section, we highlight Current trends show obesity rates have
the recommended policies.
6 TFAH • tfah.org
not decreased in many parts of the Focusing on Determinants of Health in 5 Years initiative, which recommends
country, and tobacco use remains the State policymakers often focus on nonclinical, community-wide
leading cause of preventable death.9 improving health outcomes by approaches that make a positive health
Despite spending $3 trillion on health expanding and ensuring access to quality impact, show results within five years,
annually, too many Americans are health services. However, to address and are cost effective or cost saving.18
still dying of preventable diseases,and the shifting socioeconomic needs of With an overlap in recommended
for some marginalized populations, an increasingly diverse population, to policies, each of these organizations is
poor health outcomes and health improve health, and to uncover the root closely communicating and supporting
disparities persist.10 causes of poor health, we must place a each other’s work—just as local and
greater emphasis on the importance of state leaders should—to promote policy
An Aging Population multisector solutions beyond healthcare. changes that result in improved health
The number of Americans aged 65 This means looking past traditional outcomes for cities and states alike.
and older is expected to grow from public health strategies and instead While state and local collaboration
15 percent to 17 percent by 2020. supporting healthy learning, promoting around policy has resulted in health
By 2030, this population is likely healthy living through the built improvements across the country,
to comprimise 20 percent of the environment, advocating for healthy there are instances when those with a
total population.11 With age comes behavior, and endorsing fair economic vested interest have advocated for state
increased risks of dementia, injuries opportunities for all. preemption laws that limit local authority
from falls, and chronic diseases such on matters related to public health.
as diabetes and heart disease, which Importance of State and Recent examples have involved the rights
account for 95 percent of healthcare Local Collaboration of local communities to enact paid sick
costs in the United States.12,13,14 The leave policies as a strategy to encourage
States and municipalities are uniquely
racial and ethnic disparities noted the appropriate use of healthcare
positioned to enact policies that
above are also reflected in this services and to reduce spreading illness
address their residents’ most pressing
population, with an elevated risk of in the workplace. A March 2016 study, for
issues. Along with states, local
death from chronic diseases and a example, showed that 68 percent of all
municipalities are important innovators
shortened life span among Black and workers have access to earned sick leave.
of public health approaches in areas
Native American older adults. However, only 41 percent of workers in
like tobacco use, obesity, and access
to clean needles for intravenous drug the bottom quartile of wages have access
A More Diverse Nation to this benefit.19 As of July 2017, 20 states
users. In numerous instances, states
The United States is becoming more adopted laws and regulations only after have preempted local municipalities
culturally, racially, and ethnically the approaches had proved successful from enacting earned or paid sick leave
diverse than ever before. By 2020 the in local communities. State and local laws. Even for states that have enacted
U.S. Census projects there will not be collaboration is thus a critical element paid sick leave laws, such as Maryland
a single racial or ethnic group that to ensuring that local, state, and federal or Oregon, the legislation contains
makes up the majority of children, and policy is effectively implemented. preemption clauses that prohibit local
by 2045, this will be the case for the governments from requiring employers
general U.S. population.15,16 Recognizing the importance of to provide more generous earned or
synergy between local and state efforts, paid sick leave benefits.20 In this and
States will need to address the needs PHACCS is collaborating with the de other instances, preemption laws have
associated with these demographic Beaumont Foundation and Kaiser inhibited potential public health progress
shifts. State decision makers will Permanente on their CityHealth in cities and other local municipalities.
need to consider new and adapted initiative, which provides local leaders This report provides more details on the
policies in order to improve the health with a package of evidence-based policy impacts of and potential strategies for
and well-being of all populations, solutions.17 PHACCS is also aligning preemption in the “Related Policies and
regardless of race, ethnicity, cultural with the Centers for Disease Control Other Issues” section (see page 62).
background or age. and Prevention on the Health Impact
TFAH • tfah.org 7
Health Is More Than Healthcare
As was the case in the example of Mary Johnson that begin this chapter, the social determinants of
health are the conditions in the environments in which people are born, live, learn, work, play, worship,
and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.21 The
social determinants of health can be organized into the following domains: Economic Stability, Education,
Health and Healthcare, Neighborhood and Built Environment, and Social and Community Context.
Economic Stability: Economic stability is related to issues of
employment, income, food security, and housing stability—all of
which affect health outcomes. Economic stability is often tied
to employment, which determines a person’s financial access to
resources like food, housing, and healthcare. Lack of economic
stability or job insecurity can lead to poverty, to an inability to
secure necessities, and to increases in chronic stress—all of
which can elevate a person’s risk for poor health. Alternatively, Source: Centers for Disease Control and Prevention
economic stability from steady employment with a livable wage
network as well as access to different types of support, such as
can provide a person with the income and benefits necessary
information sharing, emotional support, or instrumental support,
to access quality resources, like nutritious foods, safe housing,
like a ride to work.25 Social isolation, on the other hand, is
and medical care.
harmful to health, even more so than obesity or smoking 15
Education: Educational opportunities can have lasting effects cigarettes a day.26 Incarceration, can negatively impact the
on a person’s health throughout one’s life and is one of health of individuals and communities. While incarcerated,
the strongest predictors of health. Quality education from
22
individuals may not receive the healthcare they need, and once
the earliest years through adulthood can shape cognitive they are released, they often face barriers while reintegrating
development, problem-solving skills, and literacy—skills that into society. Additionally, more than half of fathers in state
influence healthy behaviors. Educational attainment is also prison report being the primary income generator in their
tied to future earnings and access to social networks. People families, which can lead to economic hardship.27
with higher educational attainment are less likely to experience
Historical and Ongoing Structural Racism and Other
unemployment or financial hardship.23
Discrimination: Discrimination can also significantly impact
Neighborhood and Built Environment: A person’s neighborhood individuals’ and communities’ health.28 Individual and
encompasses the natural and man-made physical environments structural discrimination, which are mutually reinforcing, can
in which people live, including the air they breathe and the cause intentional and unintentional harm, whether or not
water they consume. Neighborhoods overall, and physical it is perceived by the individual.29 Discrimination can be
environments specifically, affect the options an individual or understood as a social stressor that has a physiological effect
family has for housing, employment, food, transportation, on individuals, and it can be compounded over time and lead
health and social services and being physically active. All these to long-term negative health outcomes, including higher blood
factors, as well as trauma, crime and other environmental pressure, lower-birthweight infants, cognitive impairment,
conditions like climate, contribute to health outcomes. For and mortality.30,31 Inequities resulting from discrimination are
example, children and adolescents who are exposed to violence, a result of policies, often established without conscious or
either as a victim, direct witness, or just hearing about a crime, malicious intent, that disadvantage communities of color.32
are at risk for poor long-term behavioral health outcomes.24
There are other determinants of health, such as access
Social and Community Context: The nature of our social to health insurance and healthcare services. These social
interactions and relationships with other people and our determinants of health are all connected, which is why
community affect our health and well-being. A sense of improving health requires working across different sectors to
community and social cohesion helps form a person’s social prevent the onset of disease.
8 TFAH • tfah.org
Improving Health for All: State Opportunities to Advance Health Equity
It is critical that states explore how
to advance health equity by first
identifying where differences in health
outcomes exist and then developing
policies to address these inequities.
What Is “Health Equity”?
We define “health equity” as “the state
in which everyone has the chance to
attain their full health potential and no
one is disadvantaged from achieving
this potential because of social position
or any other defined circumstance.”33
Achieving health equity requires
removing obstacles to health such Source: Robert Wood Johnson Foundation37
as poverty, discrimination, and their
consequences, including powerlessness
to opportunities, there will continue
and a lack of access to good jobs with fair
to be differences in health. Groups
pay, quality education and housing, safe
of people who are marginalized or
environments, and healthcare.34 Health
disadvantaged often have worse health.
disparities are differences in health or
And though individual behaviors
the factors that influence health that
play a role in health, many of the
are closely linked with social, economic
choices people make depend on the
or environmental disadvantage.
opportunities available to them.
Policymakers can measure disparities in
health and its determinants and use the With a strong understanding of the
data to assess progress toward achieving needs of their residents, state leaders
health equity.35 are in a good position to ensure that all
individuals, of all backgrounds, have the
The graphic above depicts the
opportunity to be as healthy as possible.
difference between equality and
Every level of government has a set of
equity. Equality provides the same
responsibilities dedicated to protecting,
opportunities for all, while equity
preserving, and promoting the health
recognizes that individuals require
and safety of their residents. State
more—not equal—effort and resources
policymakers can work to improve the
to level the field of opportunities due to
health and safety of their population by
historical and ongoing discrimination
enacting laws, policies, and regulations,
and marginalization.36
and they can distribute resources.
A person’s health, including their Moreover, protecting the public’s health
ability to make healthy choices, is and preventing the onset of disease
impacted by where they live, how much can translate into cost savings and
income they earn, their educational increased productivity statewide. To
attainment, and differential access to address issues of health equity, states can
and quality of care based on their racial develop policy solutions that increase
and ethnic status. Unfortunately, as opportunities and remove obstacles to
long as there are differences in access health like poverty and discrimination.38
TFAH • tfah.org 9
How Can Policy Advance benefits when each person can thrive.
Health Equity? The Joint Center for Economic and
Addressing health inequities means Political Studies estimates that between
implementing policies and institutional 2003 and 2006, 30.6 percent of direct
practices that increase opportunities medical care expenditures for racial
for people to be healthy and make and ethnic minorities were excess costs
healthy choices. It also means stemming from health inequalities.
implementing strategies that remove The Center estimated that eliminating
barriers to achieving better health. health disparities for minorities would
have reduced direct medical care
Discrimination is not always expenditures by nearly $230 billion
intentional, but it is often built into over the four-year period examined.
institutional policies and practices. Additionally, closing existing disparities
This is referred to as “structural” or and creating additional opportunities
“institutional” discrimination.39 Policies to advance racial equity can increase
can give rise to unfair differences in economic output and consumer
the social conditions that affect health spending.41 Raising the average earnings
and result in health inequities. For of people of color to the level of
example, deliberate discriminatory Whites by closing disparities in health,
policies that were enacted decades education, and opportunity would
ago resulted in residential segregation generate an additional $1 trillion in
by race. Despite the fact that housing earnings and an additional $800 billion
discrimination is no longer legal, many in spending.42,43 This research is just the
racial and ethnic minorities continue tip of the iceberg, as reducing disparities
to live in neighborhoods with poor- can not only focus on improving equity
quality schools, housing, and services, among racial and ethnic groups; it can
all of which affect their opportunity to also address other populations who may
be healthy.40 Another example is how be marginalized or who may not receive
diversion policies are administered for essential services, such as rural residents
nonviolent, first-time criminal offenses. who lack access to many of the services
If an offender qualifies for diversion, individuals in urban areas receive.44
they will not go to jail and will have the A separate analysis estimates that the
offense expunged from their record, United States could realize an $8 trillion
but only if they are able to pay certain gain in gross domestic product by 2050 as
fees. As a result, people with lower a result of closing the racial equity gap.45
incomes are more likely to serve time
in jail and have a criminal record How Will This Report Address
compared with people with higher Health Equity?
incomes who have committed the same
Throughout this report, we identify
or worse offenses, putting them at risk
opportunities for state-level policymakers
for unemployment in the future.
to advance health equity and reduce
disparities in their states through the
The Business Case for development and implementation of
Improving Equity and evidence-based policies. While some
Reducing Disparities of these policies may be more directly
The high economic cost of health targeted to vulnerable populations, all of
inequities places a large burden on the policies in this report can facilitate
states. Equity enables everyone to live health improvement for all individuals
to their full potential, and all of society and communities.
10 TFAH • tfah.orgMethodology
methodology
METHODOLOGY
APPROACH
To inform this initiative, TFAH identified and reviewed 1,500 evidence-based
or evidence-informed policies, programs, and strategies by using several
national databases, including CityHealth, the Win-Win Project, the Centers
for Disease Control and Prevention’s (CDC) Health Impact in 5 Years (HI-
5), County Health Rankings and Roadmaps: Strategies that Work, the Pew-
MacArthur Results First Initiative, and the Community Guide Task Force
Recommendations.46,47,48,49,50,51 We removed clinical-based strategies from the
list. Throughout the review process, TFAH assessed each potential policy for
evidence of its impact on the reduction of health disparities and the promotion
of health equity. We then applied a set of criteria to the policies, programs,
and strategies to identify upstream, state-level legislative policies that improve
health and well-being and control costs. Those criteria are:
1. Strong Health Impact and Economic Evidence
We reviewed the health and economic results (that is, have a positive return on investment) or
for each policy and strategy to ensure there was produced positive economic impacts over time.
sufficient evidence to promote positive health We excluded policies that did not have supporting
outcomes and control costs. Taking a broad view of health or economic evidence available.
economic evidence, TFAH considered economic
PHACCS employed an approach that blended the
analyses such as cost avoidance, cost benefit,
rating systems and evidence criteria from different
return on investment, cost effectiveness, and cost
databases to initially filter policies that had
utility. Policies recommended in this report have
positive health and economic evidence.
demonstrated that they are either cost beneficial
TABLE 1: Databases Reviewed and Evidence Categorization Required to be Considered for
Initial Inclusion in PHACCS
Initiative Types of Policies Included in PHACCS Review Are Those Designated:
Community Guide Recommended
Under the heading “government as the decision maker”:
County Health Rankings & Roadmaps: • Scientifically supported
Strategies that Work • Expert opinion
• Some evidence
HI-5 Interventions N/A: All 14 policies considered for inclusion
Win-Win Project N/A: All 17 policies considered for inclusion
• Highest rated
Results First Clearinghouse
• Second-highest rated
FEBRUARY 2019
CityHealth N/A: All nine policies considered for inclusion
112. Population-Based Prevention Efforts regulatory rulemaking—rather than legislative
PHACCS used the “Three Buckets of Prevention” action—as well as program-level interventions
framework,52 which categorizes disease prevention and time-limited pilots. However, the importance
and health promotion interventions and policies of well-crafted regulations to guide effective
into three domains, or “buckets”. Buckets one and implementation of the policies recommended in
two focus on traditional and innovative clinical this report should not be understated.
prevention efforts, whereas bucket three focuses Legal Analysis
on population-oriented interventions. PHACCS
The Policy Surveillance Program of the Center
defines a “population-based intervention” as
for Public Health Law Research at Temple
an intervention or policy that reaches whole
University conducted a review of secondary
populations. It includes interventions that
legal resources for the policies that met the
are not intended for a single individual or
four inclusion criteria. The analysis assessed the
all the individuals within a practice or even
existence and complexity of each state law, the
all beneficiaries covered by a certain insurer.
extent to which the policy of interest was found
Rather, the target is an entire population or
in legal form, and the availability of existing
subpopulation, usually identified by a geographic
data or expertise on the law. Each policy was
area. Interventions are based not in a healthcare
analyzed to determine how widespread the policy
settings but in neighborhoods, cities, counties,
implementation was in the state, the degree of
or states. Using this framework, we excluded
variation, and the feasibility of tracking the policy
policies and strategies that were not population-
over time. In 2019, TFAH and the Center for
based prevention efforts, (such as those related
Public Health Law will release comprehensive
to clinical practice or to Medicaid care delivery or
datasets, based on publicly available data, for the
reimbursement).
recommended policies to assist state officials and
other in better understanding the key aspects of
3. Primary and Secondary Prevention the laws and the extent to which they have been
PHACCS is focused on upstream prevention adopted, and differ, in all 50 states.
efforts that effectively address communities’ and
populations’ underlying health needs. PHACCS Role of the Advisory Group
uses the CDC’s definitions of primary and We consulted an esteemed group of subject-
secondary disease prevention.53 Policies were matter experts from education, public health,
excluded that we did not consider a form of health economics, healthcare, philanthropy,
primary or secondary prevention. fiscal policy, health equity, housing, and public
health law to provide guidance on the selection
Primary Prevention: intervening before health
of the recommended policies in this report. The
effects occur, through measures such as
Advisory Group considered the following criteria
vaccinations, reducing risky behaviors (poor
for each potential policy as decisions were made
eating habits, tobacco use), and banning
about those policies included in this report:
substances known to be associated with a disease
current policy landscape, strength and availability
or health condition.
of health and economic evidence, feasibility
Secondary Prevention: screening to identify diseases for enactment, and potential implementation
in the earliest stages, before the onset of signs and barriers. A key area of consideration proposed by
symptoms. the Advisory Group addressed how each of the
recommended policies advance health equity.
4. Role for State Legislative Action Through the application of the four criteria
We reviewed evidence to ensure that the state and with input from the advisory group, TFAH
legislature was responsible for enacting and selected a set of recommended policies and
implementing each policy. We excluded policies several secondary or complementary policies for
that were implemented by administrative or inclusion in this report.
12 TFAH • tfah.org1
Support the Connections Between
GOAL 1: Support the Connections Between Health and Learning
Health and Learning Goal
There is increasing evidence that the presence of healthy environments for
learning lead to positive health and economic outcomes throughout a child’s
entire life. Despite significant progress, many families and children continue
to face enormous challenges in accessing developmentally appropriate quality
early care and education in safe and healthy settings. A range of options are
available for families, from center-based to home-based care, pre-K programs in
public schools and Head Start programs.
Education and Child Development
While brain science demonstrates the importance environmental hazards, suicidal thoughts and
of early childhood education, significant attempts, teen pregnancy, alcohol and drug
investments and supports for pre-kindergarten misuse, sexually transmitted diseases, aggression
(pre-K) learning environments have lagged.54 and violence, domestic violence and rape, not
Investments in high-quality early childhood acquiring key parenting skills or child-care
education, including pre-K programs, can support, and difficulty securing and maintaining
reduce the risk for: chronic illnesses, shorter and a job.55,56,57 Despite the evidence, families lack
less healthy lives, obesity and eating disorders, access to quality, affordable early care and
difficulty in maintaining healthy relationships, education programs. While federal resources
lower academic performance, behavioral for some early care and education programs
problems in school, high school drop out, the have increased in recent years and federal, state,
need for special education and child-welfare and local support for state-funded preschool
services, mental and behavioral health problems programs, specifically, has not grown significantly
like depression and anxiety, exposure to harmful in recent years nationwide.
LEARNING CURVE
Key Statistics on state funded pre-K Access and l State funding per child was $5,008, a slight decline
Resources from 2015–2016 when adjusted for inflation.
l Nationally, only 33 percent of 4-year-olds and l Most states’ programs have not kept pace with
5 percent of 3-year-olds were enrolled in state- inflation. Five states decreased their spending
funded preschool.58 per child when considering unadjusted dollars.
l Only 29 states served 3-year-olds in some form l Spending per child is directly related to program
of state-funded pre-K programming in 2017. quality, as it determines what resources are
available, including the likelihood of retaining
State funding for preschool rose 2 percent to
FEBRUARY 2019
l
qualified teachers.59
about $7.6 billion since 2015–2016.
Source: The State of Preschool 201760
13and school performance that are
difficult to ameliorate.61 Children who
received high-quality care in the first few
years of life scored higher in measures
of academic and cognitive achievement
when they were 15 years old, and they
were less likely to exhibit challenging
behavior than those who were enrolled
in lower-quality child care.62
The quality of preschool programs
depends on a variety of inputs,
including the workforce, the
environment, and the programming.
Research shows that better education
and training for teachers can improve
Source: The State of Preschool 201760
the interaction between children
Even for children who have access to special needs. High-quality, intensive and teachers, which in turn affects
early education programs, it is also pre-K programs for low-income children’s learning. Class size and staff-
important to ensure programs are high children have led to lasting positive child ratios are also a factor, because
quality. Research shows the positive effects, such as greater school success, smaller classes and fewer students
benefits for all children in high- higher graduation rates, lower rates of per teacher gives children more
quality, intensive pre-K programs and crime among youth, decreased need opportunities for interaction with adults
the harmful effects of inferior-quality for special education later, and lower and more individualized attention.
care. These effects—both positive and adolescent pregnancy rates. Inferior- In addition, quality programs include
negative—are magnified for children quality care, however, can have harmful evidence-based early learning standards
from disadvantaged situations or with effects on language, social development, and comprehensive services.63
POLICY Universal pre-K is publicly funded to all children, it has a larger impact
preschool offered to all 4-year-old on low-income families of color and
RECOMMENDATION 1a: children regardless of family income, English-learner students.67 Universal
High Quality Universal the child’s abilities, or any other pre-K can also alleviate the financial
Pre-Kindergarten eligibility factor, although definitions burden on families with young
of what is truly universal may vary.64 children.68 These findings show how
Research indicates that high-quality important it is for policymakers to
pre-K programs not only better understand and consider the difference
prepare students for the transition to between equity and equality when
kindergarten but can also have positive making determinations on how to
impacts later in life, such as academic allocate resources to support universal
success and lower poverty rates.65 It pre-K programs.
is critical that states ensure effective
State legislatures can provide state-
transitions from pre-K to primary
funded, high-quality pre-K programs
school, including through curricula
to children throughout the state.
alignment. An inadequate transition
Furthermore, state law governs many
from pre-K to primary school can impact
of the requirements related to the
a student’s academic performance and
provision of pre-K, such as funding,
their emotional and social adjustment.66
eligibility, hours, and health and
While universal pre-K can be a benefit
learning standards.
14 TFAH • tfah.orgHealth and Educational Evidence of pre-K participants, the children’s that access to universal pre-K
There is strong evidence that universal future earnings could exceed the cost programs can benefit children across
pre-K programs improve cognitive of the pre-K program. A benefit-cost socioeconomic backgrounds.77,78,79,80
outcomes/academic knowledge for analysis conducted by the Washington
Policy Landscape
disadvantaged children.69 But such State Institute for Public Policy
found that state and district funded The levels of funding and sources of
programs aren’t only beneficial for
pre-K education programs have a revenue streams for pre-K programs vary
low-income children. Universal high-
social benefit-to-cost ratio of $4.63:1. greatly from state to state.81 Nine states
quality pre-K programs benefit children
That includes benefits for program include pre-K funding in their K–12
across all income levels. Children who
participants, taxpayers, and others in funding formulas, thus tying it to the
attend state-sponsored pre-K, universal
society.75 The analysis took into account budgetary process for K–12 education.82
or not, show improved language, math,
the cost of the program compared Other states fund pre-K through general
and reading skills.70 The longer-term
with the benefits of reducing crime block grants or local programs, which
benefits of universal pre-K include
and increasing high school graduation are less secure revenue streams.83 Nine
reductions in teen birth and interactions
rates, academic test scores, special- states and the District of Columbia
with the criminal justice system
education placement, and grade provided state-funded pre-K to nearly
throughout a participant’s lifetime.71,72 In
retention. A more detailed analysis of 50 percent or more of their state’s
Oklahoma, state-funded universal pre-K
the monetary benefits of preschool 4-year-olds; four of those states and the
demonstrated stronger effects for Latino,
programs in Los Angeles conducted District of Columbia served more than
Black, and poor children.73 Georgia’s
by the Win-Win Project found that 70 percent.84 Federal funding can also
universal pre-K program expanded access
approximately half of the cost of such play a role in funding pre-K, such as
to care and benefited disadvantaged rural
a program would be directly recouped through the Head Start program, Pre-
children the most, including through
through reduced public spending on School Development Grants, and other
improved test scores in math and reading
Medicaid and other social programs competitive grants. Across all state and
which helped close achievement gaps in
as a result of health improvements federally funded programs, about 44
children’s education later in life.74
associated with preschool expansion.76 percent of 4-year-olds are enrolled in
some form of preschool education.85 Six
Economic Evidence While the strongest effects are states, as of 2017, provide no funding for
In Oklahoma, research showed that projected for children of lower-income pre-K programs.86
based on the academic performances backgrounds, research also demonstrates
CASE EXAMPLE
West Virginia’s Universal Pre-Kindergarten Program87,88,89
West Virginia passed legislation in 2002 requiring the state Key outcomes:
to make prekindergarten available to all 4-year-olds in the l During the 2016- 2017 school year, approximately 65% of
state by the 2012-2013 school year. West Virginia Code §18- the state’s 4-year-olds and approximately 11% of 3-year-olds
5-44 mandates that the West Virginia Board of Education, in were enrolled in West Virginia’s Universal Pre-K program.
collaboration with the Secretary of the West Virginia Department
of Health and Human Resources, ensure that every eligible
l In 2013, West Virginia aimed to improve program quality by
child has access to high quality pre-K. West Virginia requires requiring all new lead teachers in nonpublic settings to have
that a minimum of half of the programs operate in collaborative at least a BA degree in Early Childhood or a related field.
settings with private prekindergarten, child care centers, or l Beginning in the 2016-2017 school year, each pre-K
Head Start programs in order to facilitate expansion of the classroom must provide at least 1,500 minutes of
program. To date, the West Virginia Universal Pre-K program is instruction per week and 48,000 minutes of instruction
available in all 55 counties of the state. West Virginia is home annually, and programs must operate no fewer than four
to one of three state-funded pre-K programs that met all of the days per week to meet annual and weekly operational
National Institute for Early Education Research’s new quality requirements.
benchmarks in 2017 (see insert on page 16).
TFAH • tfah.org 15Considerations for Effective Design and Implementation90,91
l romote universal access to state-
P l stablish an adequate, stable funding
E Education Research’s standards in
funded pre-K for all 3- and 4-year- stream, and ensure sufficient funding the box below).
olds. For states unable to fund to provide high-quality services.
l ermit and support bilingual
P
pre-K for all 3- and 4-year-olds,
l nsure instructional alignment
E instruction and other related policies
emphasize serving those with
with kindergarten curricula and to support dual-language learners,
higher needs, particularly students
instructional practices and curricula including conducting outreach and
from low-income families, when
that are developmentally appropriate, communicating to families in the
resources are limited.
address social and emotional language spoken at home.
l upport full-day programs. Full-day
S learning, and are culturally and
l nsure that local zoning and land-use
E
programs maximize children’s time linguistically appropriate.
regulations are consistent with the
to learn and play and minimize
l ncourage the implementation
E expansion of preschool capacity near
disruptions to parents’/caregivers’
of high-quality standards (see where parents live and work.
work schedules.
the National Institute for Early
BEST IN CLASS
NIEER Preschool Policy Standards learning, language development, and have annual written, individualized
and Program Quality cognition and general knowledge. professional-development plans.
The National Institute for Early Finally, states should provide
2. Curriculum Supports. States should
Education Research (NIEER) developed some professional development
provide (a) guidance or an approval
a rating system for 10 preschool policy through coaching or similar ongoing
process for selecting curricula, and
standards related to program quality classroom-embedded support.
(b) training or ongoing technical
to help state leaders enhance and assistance to facilitate adequate 7. Maximum Class Size. State policy
support high-quality early education. implementation of the curriculum. should require class sizes to be
To do this, they benchmark state limited to 20 children at most.
programs against acknowledged 3. Teacher Degrees. Lead teachers in
leading programs. The benchmarks every classroom should be required 8. Staff-Child Ratio. State policy
provide a coherent set of minimum to have at least a bachelor’s degree. should require that classes be
policies to support meaningful, permitted to have no more than 10
4. Teacher Specialized Training. State
persistent gains in learning and children per teaching staff member.
policy should require specialized
development that can enhance later training in early childhood education 9. Screenings and Referrals. State
educational and adult achievement. and/or child development. preschool programs should ensure
Using these policies will make it more children receive vision, hearing, and
likely that pre-K programs will achieve 5. Assistant Teacher Degrees. Assistant
other health screenings and referrals.
their goals. teachers should be required to hold
a Child Development Associate 10. C
ontinuous Quality Improvement
1. Early Learning and Development certification or have equivalent System. State policy should—at a
Standards. States should have preparation. minimum—require that (1) data on
comprehensive Early Learning and classroom quality are systematically
Development Standards that cover 6. Staff Professional Development.
collected at least annually, and (2)
all areas identified as fundamental Both teachers and assistant
local programs and the state both
by the National Education Goals teachers should be required to
use information from the Continuous
Panel: physical well-being and motor have at least 15 hours of annual in-
Quality Improvement System to help
development, social-emotional service training. Lead and assistant
improve policy or practice.
development approaches to teachers should also be required to
16 TFAH • tfah.orgYou can also read