Prospective Evaluation of Health Outcomes in a Nationwide Sample of Aeromedical Evacuation Casualties: Methods From a Pilot Study - Oxford ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MILITARY MEDICINE, 00, 0/0:1, 2021
Prospective Evaluation of Health Outcomes in a Nationwide
Sample of Aeromedical Evacuation Casualties: Methods From a
Pilot Study
Lauren E. Walker, MSSW*; Cameron T. McCabe, PhD†,‡; Jessica R. Watrous, PhD†,‡;
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab329/6338456 by guest on 04 December 2021
Eduard Poltavskiy, PhD*; Jeffrey T. Howard, PhD§; Jud C. Janak, PhD∥;
Lt Col Laurie Migliore, PhD*; Lt Col Ian J. Stewart, MD¶; Michael R. Galarneau, MS‡
ABSTRACT
Introduction:
Although retrospective analyses have found that combat-injured service members are at high risk for mental and
physical health outcomes following injury, relatively little is known about the long-term health of injured service
members. To better understand long-term health outcomes after combat injury, a large, prospective observational
cohort collecting both subjective and objective health data is needed. Given that a study of this nature would be
costly and face many logistical challenges, we first conducted a pilot to assess the feasibility of a larger, definitive
study.
Materials and Methods:
We ran a prospective, observational pilot study of 119 combat-injured service members and veterans who completed
(1) at least one set of laboratory measurements (blood and urine sample collection and vitals measurements) at Clinical
Laboratory Improvement Amendment of 1988 compliant laboratory locations and (2) at least one online assessment for
the Wounded Warrior Recovery Project (WWRP), a 15-year examination of patient-reported outcomes among service
members injured on combat deployment. We recruited the pilot study cohort from WWRP participants who met eligibil-
ity criteria and indicated interest in additional research opportunities. We collected laboratory values and patient-reported
outcomes at baseline and again 1 year later, and obtained demographic, injury, and military service data from the Expe-
ditionary Medical Encounter Database. The David Grant USAF Medical Center Institution Review Board (IRB) and the
Naval Health Research Center IRB reviewed and approved the study protocols.
Results:
During recruitment for the pilot study, 624 study candidates were identified from WWRP. Of the 397 candidates we
contacted about the pilot study, 179 (45.1%) enrolled and 119 (66.4%) of those who enrolled completed the first year
of participation. The second study year was suspended due to the coronavirus disease-2019 pandemic. At the time of
suspension, 72 (60.5%) participants completed follow-up laboratory appointments, and 111 (93.3%) completed second-
year WWRP assessments. Participants in the pilot study were predominately male (95.0%) and non-Hispanic White
(55.5%), with a median (interquartile range) age of 38.3 (34.1-45.4) years.
Conclusions:
Collection of patient-reported outcomes and laboratory samples in a geographically dispersed cohort of combat-injured
service members is possible. While significant challenges exist, our pilot study results indicate that a larger, longitudinal,
cohort study is feasible.
* Clinical Investigation Facility, David Grant USAF Medical Center,
or employee of the U.S. Government as part of that person’s official duties.
Fairfield, CA 94535, USA This report was supported by the U.S. Navy Bureau of Medicine and Surgery
† Leidos, San Diego, CA 92106, USA
under work unit no. 60808 and the U.S. Air Force (USAF) Headquarters,
‡ Medical Modeling, Simulation, and Mission Support Department, Naval
Office of the Surgeon General. The views expressed in this article are those
Health Research Center, San Diego, CA 92106, USA of the authors and do not necessarily reflect the official policy or position
§ Department of Public Health, University of Texas San Antonio, San
of the Department of the Navy, Department of the Air Force, Department
Antonio, TX 78249, USA of Defense, or the U.S. Government. The study protocols were approved by
∥ Bexar Data, San Antonio, TX 78210, USA the Naval Health Research Center Institutional Review Board and the David
¶ Department of Medicine, Uniformed Services University of the Health Grant USAF Medical Center Institution Review Board in compliance with all
Sciences, Bethesda, MD 20814, USA applicable Federal regulations governing the protection of human subjects.
An oral presentation of part of this work was delivered at the Military Research data were derived from an approved Naval Health Research Cen-
Health System Research Symposium in Kissimmee, FL, on August 21, 2019. ter, Institutional Review Board protocol number NHRC.2009.0014 and from
Authors LM, IJS, and MRG are service members or employees of the a U.S. Air Force Surgeon General-approved Clinical Investigation Number
U.S. Government. This work was prepared part of official duties. Title 17, FDG20170020H.
U.S.C. §105 provides that copyright protection under this title is not avail- doi:https://doi.org/10.1093/milmed/usab329
able for any work of the U.S. Government. Title 17, U.S.C. §101 defines Published by Oxford University Press on behalf of the Association of
a U.S. Government work as work prepared by a military service member Military Surgeons of the United States 2021. This work is written by (a) US
Government employee(s) and is in the public domain in the US.
MILITARY MEDICINE, Vol. 00, Month/Month 2021 1Combat Casualties Longitudinal Pilot Study Methods
INTRODUCTION outcomes and blood samples from veterans of recent con-
More than 53,000 U.S. service members have been wounded flicts exist;24–26 however, currently, only one is specific to
in action, and more than 7,000 have died as a result of Over- combat-injured service members.26 Results from this study
seas Contingency Operations since October 2001.1 Although have not yet been reported and participation is limited to male
prior work has found that combat-injured service members service members from the UK injured in Afghanistan. Other
are at high risk of physical and mental health outcomes,2–13 large, prospective, cohort studies collecting patient-reported
both the mechanisms by which risk is conferred and the long- outcomes on combat-injured service members, such as the
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab329/6338456 by guest on 04 December 2021
term health of service members living with traumatic injuries WWRP, have yet to combine subjective data with prospective
remain unclear. To better understand the long-term health of objective health data. To date, no studies have reported results
combat-injured service members, a large, prospective, obser- of longitudinal, prospectively collected objective and subjec-
vational cohort with both objective (e.g., vitals and laboratory tive health measures in a geographically dispersed population
values) and subjective (e.g., patient-reported outcomes) health of combat-injured U.S. veterans from recent conflicts.
measurements is needed. Combining these prospectively col- A large, prospective study of objective and subjective
lected data with Department of Defense (DoD) administrative health measures would provide opportunities to study long-
data on military service, injury, and treatment factors will pro- term outcomes of specific subsets of injured veterans. For
vide a more comprehensive view of injured service members’ example, service members who undergo aeromedical evacu-
health years after the initial insult and could identify potential ation (AE) following traumatic brain injury (TBI) may be at
prevention and intervention targets for optimizing health out- particular risk for adverse cognitive and mental health out-
comes. Due to the heavy logistical burden and cost of such a comes. In prior models of TBI in rats, animals that were
study, a smaller pilot study is first needed. exposed to simulated AE via hypobaria had worse cognitive
Retrospective analyses suggest that combat-injured ser- function, more depressive behavior, and hippocampal neu-
vice members are at high risk of chronic diseases, including ronal loss when compared to animals with TBI who were
hypertension, chronic kidney disease, coronary artery dis- not exposed to hypobaria.27 This is particularly concerning
ease, and diabetes mellitus,4,7,12,13 and that the risk of these given that widespread exposure to blasts in current conflicts
diseases escalates with injury severity.12,13 In one large, ret- has resulted in high rates of TBI and polytrauma in service
rospective study, severely injured service members were at members. In samples of severely injured combat casualties,
more than twice the adjusted risk for subsequent hyperten- reported prevalence of moderate or severe TBI ranges between
sion and more than four times the risk for diabetes mel- 31.6 and 56%.2,28 Results from these animal models have not
litus and coronary artery disease when compared to their been validated in combat casualties and may not be gener-
non-injured, combat-deployed counterparts.13 In addition to alizable to adults with concussions.29 However, these results
chronic diseases, injured service members are at high risk suggest that additional investigation is warranted for long-
of mental health diagnoses, including posttraumatic stress term health outcomes of service members who underwent AE
disorder (PTSD), depression, and anxiety,2,7,14–18 with preva- following injury.
lence in retrospective analyses of injured cohorts ranging In this pilot study, we assess the feasibility and character-
from 38 to 64%2,3,7 , 27 to 45%,3 and 37 to 39%,2 respec- ize the challenges involved in recruitment and data collection
tively.19 Data from the Wounded Warrior Recovery Project for a larger, definitive study combining patient-reported out-
(WWRP), an ongoing longitudinal examination of patient- comes, laboratory values, and DoD administrative records
reported outcomes of deployment-injured service members, of U.S. service members who underwent AE from Iraq or
show similar rates of PTSD and depression, with approx- Afghanistan. A large-scale study of this nature, while essen-
imately 38-45% screening positive for PTSD and 43-48% tial to a more comprehensive understanding of the long-term
screening positive for depression.20,21 Given the elevated risk effects of combat injury, would be costly and face many logis-
that combat-injured service members face, as well as the tical and regulatory challenges. Here, we report the methods
often-comorbid relationships between mental and physical and success of enrollment and participation from our 2-year
health outcomes,7,22,23 an examination of both subjective and pilot study of 119 AE casualties.
objective measures from injured service members is essential
to understand the long-term effects of injury and the potential
pathways to increased risk. METHODS
Although retrospective analyses provide a description of Study protocols were reviewed and approved by the David
service members’ outcomes in the years following injury, Grant USAF Medical Center Institutional Review Board
they are also limited to using administrative data and lack (IRB) and the Naval Health Research Center IRB. The sub-
information on sub-clinical symptoms. Since diagnosis is jects’ voluntary, informed consent in this pilot study were
contingent on interaction with the healthcare system, these obtained as required by 32 CFR 219 and DODI3216.02
studies may be biased toward individuals who are more likely AFI40-402, Protection of Human Subjects and Adherence
to seek care and subsequently receive a diagnosis. A lim- to Ethical Standards in Air Force Supported Research. The
ited number of prospective studies collecting patient-reported Travis Air Force Base IRB approved a Waiver of Written
2 MILITARY MEDICINE, Vol. 00, Month/Month 2021Combat Casualties Longitudinal Pilot Study Methods
Informed Consent and all pilot study participants provided Informed Consent Document, and the contact information for
verbal consent over the phone. The pilot study protocol their preferred laboratory location.
was registered on ClinicalTrials.gov on November 9, 2018, Participants visited Clinical Laboratory Improvement
under ID NCT03736356 (https://clinicaltrials.gov/ct2/show/ Amendment of 1988 compliant laboratory locations within
NCT03736356). the USA for blood and urine samples and vitals measure-
ments (height, weight, and blood pressure). Tests performed
on patient samples included: complete blood count, compre-
Population
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab329/6338456 by guest on 04 December 2021
hensive metabolic panel, lipid panel, A1C, cystatin C, high
We identified eligible candidates for this pilot study from sensitivity C-reactive protein, B-type natriuretic peptide, and
the WWRP, an ongoing, web-based longitudinal examina- microalbumin/creatinine ratio. Participants completed labo-
tion of patient-reported outcomes of injured service members ratory work within 4 months of the date that their contact
that is being conducted by the Naval Health Research Center information was received by our study staff at DGMC. Fol-
and has enrolled more than 6,300 participants since Decem- lowing enrollment, we called or emailed participants no more
ber 2012.30,31 Individuals were eligible for our pilot study if than three times to remind them of their participation cutoff
they (1) participated in the WWRP, (2) selected “yes” to a date. If participation was not completed by the required date,
WWRP item assessing interest in additional research opportu- we removed the participant from the study and contacted new
nities, and (3) had record of AE in the Expeditionary Medical candidates for enrollment. Following completion of labora-
Encounter Database (EMED) due to combat injury in Iraq tory sample collection, participants received a $50 electronic
or Afghanistan during or after October 2001. The EMED gift card research incentive by email.
includes medical encounters of deployed service members Eligibility for the second-year laboratory visit occurred
beginning in 2001.32 To control for the possible effects of between 9 and 14 months following a participant’s first labo-
injury severity,12,13 we grouped participants into quartiles ratory collection date. Our research staff called participants to
based on the distribution of Injury Severity Scores (ISS) in the assess any change in contact information, review study pro-
overall WWRP cohort (≤3; 4-8; 9-12; >12). The ISS is a vali- cedures, and confirm participation. Following confirmation
dated measure of injury severity that ranges from 1 to 75, with of the participants’ availability, study staff sent a confirma-
higher scores indicating more severe injury.33 We enrolled no tion email with the participant’s laboratory order and preferred
more than 30 participants per ISS quartile at a time. laboratory location.
Enrollment and Participation Data Elements
Patient-reported outcomes data came from participants’ We obtained demographic (age, sex, race/ethnicity, mari-
WWRP assessment measures. Briefly, WWRP participants tal status, and education), military service (service branch,
are identified via EMED and recruited to complete assess- rank, and active duty or National guard/Reserve status), and
ments every 6 months for 15 years. Multiple contact methods injury (ISS, injury mechanism, and TBI history) data from
are used to recruit participants, who then visit the WWRP EMED and patient-reported outcomes from WWRP assess-
website, provide informed consent, and complete assessment ments. Validated measures currently used in the WWRP
measures on mental health, quality of life, and health behav- have been described previously.31 Depressive symptoms were
iors. More detailed information about WWRP methodology measured using the Patient Health Questionnaire-8,34 with a
has been previously reported.31 This pilot study used assess- positive screen of depression defined using an established cut-
ments completed between September 2018 and January 2019 off score of ≥10. Symptoms of PTSD were assessed with
as baseline measures, as well as follow-ups 1 year later. the PTSD Checklist for Diagnostic and Statistical Manual of
Beginning in September 2018, a survey item assessing Mental Disorders, 5th Edition,35 with a positive screen of
WWRP participants’ interest in additional research opportu- PTSD defined as a score of ≥33. Quality of life was mea-
nities was included in all WWRP assessments. If WWRP par- sured using the Short Form Health Survey and established
ticipants indicated interest in additional research and met all subscale scores were calculated for the Physical Component
inclusion criteria for the pilot study, their contact informa- Score and Mental Component Score. The TBI history was
tion, ISS, and date of birth were securely sent to clinical evaluated using a self-report item assessing TBI symptoms
research staff at David Grant USAF Medical Center (DGMC). and timing (while deployed vs. nondeployed). Alcohol use
We then conducted pilot study enrollment from the list of over the past 30 days was assessed using three items adapted
study candidates in the order in which they completed their from the National Institutes of Alcohol Abuse and Alcoholism
WWRP surveys, via phone call, with no more than three con- and included the number of drinking days, average number of
tact attempts per candidate. Interested candidates enrolled in drinks consumed on drinking days, and whether the partici-
the study by providing verbal consent after telephonic review pant engaged in heavy episodic drinking, defined as five or
of all study procedures. Once enrolled, we emailed pilot study more drinks within a 2-hour period for males or four or more
participants an electronic copy of their laboratory order, the drinks for females. Hazardous alcohol use was determined
MILITARY MEDICINE, Vol. 00, Month/Month 2021 3Combat Casualties Longitudinal Pilot Study Methods
TABLE I. Comparison of Study Candidates Identified through TABLE I. (Continued)
Wounded Warrior Recovery Project (WWRP) and the Pilot Study Depression .512
Cohort (screening)
Positive 211 (41.8) 46 (38.7)
Candidates Participants Negative 292 (57.8) 73 (61.3)
Characteristics (n = 505) (n = 119) P Valuea Missing 2 (0.4) 0 (0.0)
PTSD (severity) 24.0 (10.0-44.0) 25.0 (11.0-40.0) .985
Age, years 37.0 (33.4-42.5) 38.3 (34.1-45.4) .032
Sex .383 PTSD .533
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab329/6338456 by guest on 04 December 2021
Male 488 (96.6) 113 (95.0) (screening)
Female 17 (3.4) 6 (5.0) Positive 188 (37.2) 41 (34.5)
Race/ethnicity .197 Negative 313 (62.0) 78 (65.5)
Black/African 23 (4.6) 7 (5.9) Missing 4 (0.8) 0 (0.0)
American Hazardous .009
Hispanic/ 49 (9.7) 13 (10.9) alcohol useb,c
Latino Positive 81 (16.0) 9 (7.6)
Non-Hispanic 304 (60.2) 66 (55.5) Negative 249 (49.3) 72 (60.5)
White Missing 175 (34.7) 38 (31.9)
Other 12 (2.4) 7 (5.9) Cigarette use .020
Missing 117 (23.2) 26 (21.8) (current)c
Marital status .116 Yes 90 (17.8) 11 (9.2)
Married 202 (40.0) 57 (47.9) No 409 (81.0) 108 (90.8)
Unmarried 303 (60.0) 62 (52.1) Missing 6 (1.2) 0 (0.0)
Education .420 Abbreviations: PTSD, posttraumatic stress disorder; TBI, traumatic brain
Less than high 5 (1.0) 0 (0.0) injury.
school Median (interquartile range) reported for all continuous outcomes; No. (%)
High school or 434 (85.9) 100 (84.0) reported for all categorical outcomes.
equivalent a Mann–Whitney U test or chi-square difference test.
College 58 (11.5) 19 (16.0) b Items restricted to nondependent, past-month drinkers.
diploma or c Self-report items from WWRP assessment.
equivalent
Missing 8 (1.6) 0 (0.0)
Service branch .058 with a score of ≥8 on the Alcohol Use Disorders Identification
Air Force 2 (0.4) 3 (2.5) Test.36 Current cigarette use was assessed using a single item:
Army 386 (76.4) 93 (78.2) ‘do you smoke cigarettes?’ Participants who provided an affir-
Marine Corps 101 (20.0) 22 (18.5)
mative response to this item were coded as current smokers,
Navy 16 (3.2) 1 (0.8)
Rank .743 whereas those who identified as previous smokers or as having
Junior enlisted 219 (43.4) 53 (44.5) never smoked were coded as nonsmokers.
Senior enlisted 208 (41.2) 46 (38.7)
Officer 45 (8.9) 13 (10.9) Statistical Analyses
Missing 33 (6.5) 7 (5.9)
Military status .999 Descriptive statistics and nonparametric bivariate compar-
Active duty 85 (16.8) 20 (16.8) isons were obtained using IBM SPSS Statistics version 25.
National guard 13 (2.6) 3 (2.5) Mann–Whitney U tests and chi-square difference tests were
Separated/ 405 (80.2) 96 (80.7) used to examine bivariate differences between pilot study
retired
participants and candidates identified through WWRP on con-
Missing 2 (0.4) 0 (0.0)
Injury Severity 6.0 (4.0-11.5) 9.0 (4.0-13.0) .507 tinuous and binary or multicategorical variables, respectively
Score (Table I). In addition, median tests between independent
Injury .216 groups and chi-square difference tests were used to exam-
mechanism ine bivariate differences between pilot study participants and
Blast 392 (77.6) 94 (79.0)
nonparticipants on continuous and binary or multicategorical
Gunshot wound 99 (19.6) 19 (16.0)
Other 12 (2.4) 6 (5.0) variables, respectively (Table II). The significance threshold
Missing 2 (0.4) 0 (0.0) was set at 0.05.
TBI screening .418
Deployed and 143 (28.3) 26 (21.8)
nondeployed RESULTS
Deployed only 282 (55.8) 75 (63.0)
Nondeployed 37 (7.3) 7 (5.9) Enrollment and Participation
only
No TBI history 40 (7.9) 11 (9.2)
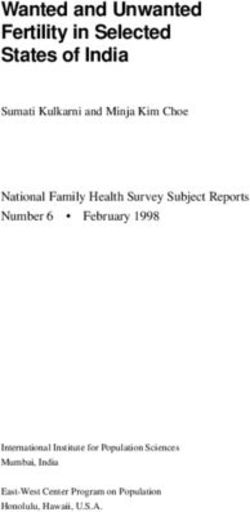
Figure 1 presents the total number of candidates, enrollees,
Missing 3 (0.6) 0 (0.0) and participants throughout each stage of the study. In total,
Depression 8.0 (3.0-13.0) 8.0 (3.0-13.0) .928 624 pilot study candidates were identified from WWRP.
(severity) Of the 397 study candidates DGMC clinical research staff
(continued) attempted to contact, 179 (45.1%) enrolled in the pilot study,
4 MILITARY MEDICINE, Vol. 00, Month/Month 2021Combat Casualties Longitudinal Pilot Study Methods
TABLE II. Comparison of Pilot Study Participants and Nonparticipants
Enrolled, did not Passive decline
Characteristics Participants (n = 119) participate (n = 60) (n = 189) Decline (n = 29) P Valuea
Age, years 38.3 (34.1-45.4) 37.1 (33.8-43.8) 37.0 (32.9-41.5) 36.8 (29.4-41.9) .625
Sex .185
Male 113 (95.0) 60 (100.0) 184 (97.4) 29 (100.0)
Female 6 (5.0) 0 (0.0) 5 (2.7) 0 (0.0)
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab329/6338456 by guest on 04 December 2021
Race/ethnicity .640
Black/African 7 (5.9) 3 (5.0) 8 (4.2) 0 (0.0)
American
Hispanic/Latino 13 (10.9) 6 (10.0) 18 (9.5) 2 (6.9)
Non-Hispanic White 66 (55.5) 38 (63.3) 114 (60.3) 21 (72.4)
Other 7 (5.9) 1 (1.7) 6 (3.2) 0 (0.0)
Missing 26 (21.8) 12 (20.0) 43 (22.8) 6 (20.7)
Quality of Life, PCS 42.8 (36.2-50.5) 44.4 (37.5-50.6) 42.0 (32.8-49.7) 41.8 (31.6-50.4) .454
Quality of Life, MCS 43.2 (28.7-53.1) 39.2 (31.3-53.6) 39.9 (28.3-52.1) 45.3 (35.1-52.2) .486
Depression (screening) .600
Positive 46 (38.7) 23 (38.3) 81 (42.9) 9 (31.0)
Negative 73 (61.3) 37 (61.7) 107 (56.6) 20 (69.0)
Missing 0 (0.0) 0 (0.0) 1 (0.5) 0 (0.0)
Depression (severity) 8.0 (3.0-13.0) 8.0 (3.0-12.0) 8.0 (4.0-13.0) 7.0 (3.5-11.5) .811
PTSD (screening) .330
Positive 41 (34.5) 23 (38.3) 77 (40.7) 7 (24.1)
Negative 78 (65.7) 37 (61.7) 110 (58.2) 21 (72.4)
Missing 0 (0.0) (0.0) 2 (1.1) 1 (3.5)
PTSD (severity) 25.0 (11.0-40.0) 25.0 (8.3-43.8) 27.0 (11.0-44.0) 20.5 (10.0-35.0) .661
Heavy episodic .759
drinkingb
Yes 18 (15.1) 10 (16.7) 34 (18.0) 5 (17.2)
No 55 (46.2) 33 (55.0) 78 (41.3) 12 (41.4)
Missing 46 (38.7) 17 (28.3) 77 (40.7) 12 (41.4)
Hazardous alcohol Useb .006
Yes 9 (7.6) 15 (25.0) 32 (16.9) 1 (3.5)
No 72 (60.5) 32 (53.3) 90 (47.6) 16 (55.2)
Missing 38 (31.9) 13 (21.7) 67 (35.5) 12 (41.4)
Cigarette use (current) .057
Yes 11 (9.2) 11 (18.3) 39 (20.6) 6 (20.7)
No 108 (90.8) 49 (81.7) 148 (78.3) 22 (75.9)
Missing 0 (0.0) 0 (0.0) 2 (1.1) 1 (3.4)
Abbreviations: MCS, Mental Component Score; PCS, Physical Component Score; PTSD, posttraumatic stress disorder.
Median (interquartile range) reported for all continuous outcomes; No. (%) reported for all categorical outcomes.
a Median test for independent groups or chi-square difference test; missing cases excluded pairwise.
b Items restricted to nondependent, past-month drinkers.
29 (7.3%) declined to participate, and 189 (47.6%) passively participants completed the first year’s WWRP assessments
declined (were unreachable or unable to set up a time to between September 2018 and January 2019.
discuss the study). We met our target enrollment before con- The second year of laboratory collection began in Septem-
tacting the remaining 227 study candidates. Reasons given for ber 2019 and was suspended in March 2020 due to the coron-
declining participation varied among pilot study candidates, avirus disease-2019 pandemic. Before study suspension, 72
and the most frequent reasons given included (1) too much (60.5%) participants completed follow-up laboratory sam-
time or effort to participate (e.g., travel time to nearest labo- ples, 11 (9.2%) were lost to follow-up, and 11 (9.2%) declined
ratory location or other scheduling conflicts; n = 12), and (2) to participate again. At the time of the study’s suspension, 8
lack of interest in the topic or procedures of the study (n = 6). (6.7%) participants had confirmed plans to go to their near-
Among the 179 pilot study enrollees, 54 (30.2%) did not com- est laboratory for specimen collection while the remaining 17
plete participation by the required date (no reason given) and (14.3%) participants had not been reached. Of the 119 par-
6 (3.4%) contacted a coordinator to withdraw from the study ticipants, 93.3% (n = 111) completed their 1-year follow-up
before participating, leaving a cohort of 119 participants who WWRP assessments between September 2019 and January
completed laboratory tests in the first year. All pilot study 2020.
MILITARY MEDICINE, Vol. 00, Month/Month 2021 5Combat Casualties Longitudinal Pilot Study Methods
a median (IQR) ISS score of 9.0 (4.0-13.0). Most partici-
pants reported experiencing TBI symptoms while deployed
(84.9%), with just 9.2% of the cohort reporting no TBI
history. When compared to all study candidates, pilot study
participants were slightly older at the date of their most
recent WWRP assessment (38.3 [34.1-45.4] years vs. 37.0
[33.4-42.5] years; P = 0.032). Hazardous alcohol use and
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab329/6338456 by guest on 04 December 2021
cigarette use were less prevalent among pilot study partici-
pants compared to candidates (7.6% vs. 16.0%, respectively;
P = 0.009 and 9.2% vs. 17.8%, respectively; P = 0.020).
There were no other significant differences between the
two groups on patient characteristics or patient-reported out-
comes.
Table II presents a comparison of select demographics
and patient-reported outcomes for participants in the pilot
study, those who enrolled and did not participate, those who
passively declined (were unable to be reached or discuss
the study), and those who declined to participate. Partici-
pants were slightly older (38.3 [34.1-45.4] years) than those
who enrolled and did not participate (37.1 [33.8-43.8] years),
those who passively declined (37.0 [32.9-41.5]), or those who
declined to participate (36.8 [29.4-41.9] years) although this
difference was not statistically significant (P = 0.625). A pos-
itive screen for hazardous alcohol use was most prevalent in
the group that enrolled and did not participate (25.0%), com-
pared to participants (7.6%), those who passively declined
(16.9%), or those who declined (3.5%; P = 0.006). Current
cigarette use was least common in the participant group
(9.2%) compared to those who enrolled and did not participate
(18.3%), those who passively declined (20.6%), and those
who declined (20.7%), although this difference was not sig-
FIGURE 1. Flowchart of eligible study candidates, enrollees, and partici-
pants.
nificant (P = 0.057). There were no other significant differ-
ences between the two groups on patient-reported outcomes
or participant characteristics.
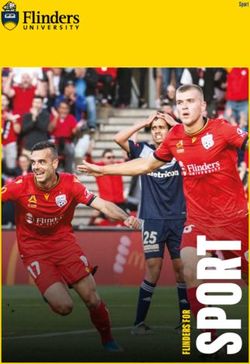
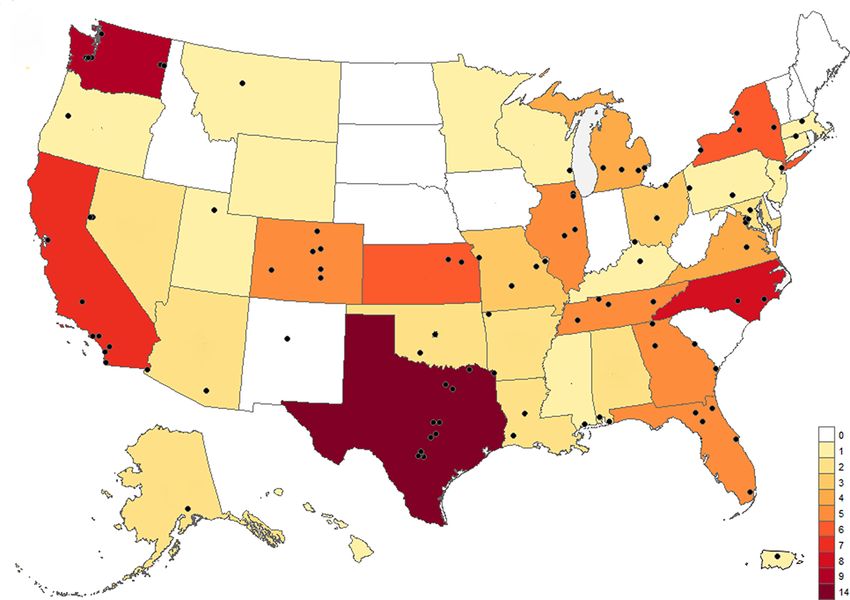
We enrolled participants from 37 states and Puerto Rico,
with the largest numbers of participants residing in Texas
(n = 14), Washington (n = 9), North Carolina (n = 8), and
DISCUSSION
California (n = 7) at enrollment time. Figure 2 displays the
Results from our pilot study indicate that collecting patient-
number of participants residing in each state at their enroll-
reported outcomes and biological samples in a geographically
ment, as well as the estimated location of laboratories selected
dispersed cohort of combat-injured service members is fea-
by participants (based on the first three zip code digits).
sible and could reasonably be scaled to a larger study. Pilot
study participants were generally similar to the pilot study
Study Cohort candidates identified from WWRP, although pilot study par-
Table I presents a comparison of participants in our pilot study ticipants were slightly older than both study candidates and
(N = 119) with all other study candidates identified through all groups of nonparticipants. Hazardous alcohol use was
WWRP (n = 505) on demographic, military service, and also less common in pilot study participants when compared
injury characteristics, and select patient-reported outcomes. to both study candidates and most nonparticipant categories.
Pilot study participants were predominately male (95.0%) Although sample sizes were small in the current study, these
and non-Hispanic White (55.5%), with a median (interquar- findings are similar to prior work identifying younger age and
tile range [IQR]) age of 38.3 (34.1-45.4) years. Most were chronic alcohol use as predictors of attrition or nonresponse
enlisted (vs. officers) at the time of injury (83.2%), served in in longitudinal follow-up.37 Consistent with previous find-
the army (78.2%), and were retired or separated from mili- ings from all WWRP participants,20,21 pilot study participants
tary service (80.7%) at the time of participation. Injuries in reported high rates of positive screens for PTSD (34.5%) and
the study cohort were primarily blast-related (79.0%), with depression (38.7%).
6 MILITARY MEDICINE, Vol. 00, Month/Month 2021Combat Casualties Longitudinal Pilot Study Methods
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab329/6338456 by guest on 04 December 2021
FIGURE 2. Geographic representation of the cohort. The map key displays the total number of participants residing in each state or territory at the time
enrollment. Dots represent unique laboratory locations selected by study participants for the first year of sample collection.
Although a larger study could face unique logistical chal- suspension. Between September 2019 and January 2020,
lenges, enrollment and participation rates from the current 111 (93.3%) participants completed 1-year follow-up WWRP
study may provide insight into the potential timeline of a assessments. Additional retention strategies, such as text mes-
large, longitudinal study of combat-injured service members. sage reminders and using a study website, could improve
Enrollment and participation primarily occurred during the laboratory data collection rates in a larger study.38 Many of
first 3 months of the pilot study’s start date, with 120 individu- these retention strategies, including a study website and a
als enrolled within the first 7 weeks and 60 laboratory samples combination of postal, email, and text reminders, are currently
collected within 11 weeks. After meeting the initial goal of being successfully used by WWRP.
120 enrollees, we conducted enrollment on an as-needed basis
following attrition. Applying the pilot study’s 33.5% with-
drawal rate, a study of 1,000 combat-injured participants is Challenges and Next Steps
possible by enrolling 1,505 individuals; an enrollment rate While this pilot study demonstrated that collecting biological
of 120 participants per 7 weeks would enable the enroll- samples and patient-reported outcomes in a geographically
ment goal to be met within 88 weeks, or roughly 1 year and disperse population of combat casualties is feasible, it also
10 months. Using additional study staff and other recruitment revealed challenges that may exist in a larger study. Our study
strategies, such as multiple contact methods, would likely was strengthened by the wide availability of laboratory facili-
increase the enrollment rate, allowing a larger study to reach ties and the option for participants to choose their preferred
its participation goals more quickly. location, which made it possible for participants to enroll
We retained a high percentage of our sample during the from 37 states and Puerto Rico. However, laboratory loca-
second year of data collection, indicating that maintaining a tions were generally less available in rural areas and none
larger cohort through multiple years is achievable. Our sec- were available in Hawai’i. Participants from these areas either
ond year of laboratory data collection was suspended early traveled a greater distance from their homes or provided sam-
due to the coronavirus disease-2019 pandemic, resulting in 25 ples while traveling for other reasons to areas that had eligible
participant withdrawals; however, initial results were promis- laboratory locations, although for some candidates, inade-
ing, with 72 (76.6%) of 94 eligible participants completing quate laboratory availability deterred participation. Partnering
follow-up laboratory appointments before the pilot study’s with multiple Clinical Laboratory Improvement Amendment
MILITARY MEDICINE, Vol. 00, Month/Month 2021 7Combat Casualties Longitudinal Pilot Study Methods
laboratories for a future study, while a greater administrative 6. Hoge CW, Auchterlonie JL, Milliken CS: Mental health problems,
burden, may allow for more widespread enrollment for service use of mental health services, and attrition from military service
after returning from deployment to Iraq or Afghanistan. JAMA 2006;
members and veterans throughout the USA. It is also possible
295(9): 1023–32.
that discrepancies in collection and measurement techniques 7. Howard JT, Sosnov JA, Janak JC, et al: Associations of initial injury
at individual laboratory locations could result in variations severity and posttraumatic stress disorder diagnoses with long-term
in reported measurements. Future work could involve a sub- hypertension risk after combat injury. Hypertension 2018; 71(5):
sample of participants with more controlled screening at 824–32.
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab329/6338456 by guest on 04 December 2021
8. Koren D, Norman D, Cohen A, Berman J, Klein EM: Increased PTSD
a centralized location. Additionally, future work could be
risk with combat-related injury: a matched comparison study of injured
strengthened by recruiting a non-injured control group and by and uninjured soldiers experiencing the same combat events. Am J
over-enrolling specific, under-represented subgroups, such as Psychiatry 2005; 162(2): 276–82.
female veterans and severely injured casualties. The labora- 9. Phillips CJ, LeardMann CA, Gumbs GR, Smith B: Risk factors for
tory data collected from this pilot study, although a limited posttraumatic stress disorder among deployed US male marines. BMC
Psychiatry 2010; 10: 52.
sample, could also be utilized in the future to analyze sub-
10. Grieger TA, Cozza SJ, Ursano RJ, et al: Posttraumatic stress disor-
groups of subjects and compare our cohort to prior studies of der and depression in battle-injured soldiers. Am J Psychiatry 2006;
injured veterans or to large, nationwide studies with subsam- 163(10): 1777–83.
ples of veterans, such as the National Health and Nutrition 11. Seal KH, Metzler TJ, Gima KS, Bertenthal D, Maguen S, Marmar CR:
Examination Survey.39 Trends and risk factors for mental health diagnoses among Iraq and
Afghanistan veterans using Department of Veterans Affairs Health
Care, 2002–2008. Public Health 2009; 99(9): 1651–8.
CONCLUSIONS
12. Stewart IJ, Sosnov JA, Howard JT, et al: Retrospective analysis of
Although significant logistical challenges exist, collecting long-term outcomes after combat injury. Circulation 2015; 132(22):
both objective health measures and patient-reported outcomes 2126–33.
in a geographically dispersed cohort of combat-injured ser- 13. Stewart IJ, Poltavskiy E, Howard JT, et al: The enduring health con-
vice members is feasible. A larger study would support future sequences of combat trauma: a legacy of chronic disease. J Gen Intern
Med 2020; 36(3): 713–21.
research that is needed to investigate relationships between
14. Cameron KL, Sturdivant RX, Baker SP: Trends in the incidence of
injury and treatment factors and subsequent health outcomes. physician-diagnosed posttraumatic stress disorder among active-duty
U.S. military personnel between 1999 and 2008. Mil Med Res 2019;
ACKNOWLEDGMENTS 6(1).
The authors would like to acknowledge the contributions of the David Grant 15. Cohen BE, Gima K, Bertenthal D, Kim S, Marmar CR, Seal KH: Men-
USAF Medical Center clinical research team. We also thank Kristen Bra- tal health diagnoses and utilization of VA non-mental health medical
ganza, Gretchen Jones, Alexandra Spruth, current and past WWRP team services among returning Iraq and Afghanistan veterans. J Gen Intern
members and students, and the Medical Modeling, Simulation, and Mission Med 2010; 25(1): 18–24.
Support research support divisions for their work on the project. 16. Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI,
Koffman RL: Combat duty in Iraq and Afghanistan, mental health
problems, and barriers to care. N Engl J Med 2004; 351(1): 13–22.
FUNDING 17. Milliken CS, Auchterlonie JL, Hoge CW: Longitudinal assessment of
This research was funded by the U.S. Air Force Headquarters, Office of the mental health problems among active and reserve component soldiers
Surgeon General, and U.S. Navy Bureau of Medicine and Surgery under work returning from the Iraq war. J Am Med Assoc 2007; 298(18): 2141–8.
unit no. 60808. 18. Seal KH, Bertenthal D, Miner CR, Sen S, Marmar C: Bringing the
war back home: mental health disorders among 103,788 US veterans
CONFLICT OF INTEREST STATEMENT returning from Iraq and Afghanistan seen at Department of Veterans
The authors declare that they do not have any conflicts of interest. Affairs facilities. Arch Intern Med 2007; 167(5): 476–82.
19. Walker LE, Watrous JR, Poltavskiy E, et al: Longitudinal mental health
outcomes of combat-injured service members. Brain Behav 2019;
REFERENCES 31(1): 34–48.
1. U.S. Military Casualties: OCO casualty summary by casualty 20. McCabe CT, Watrous JR, Galarneau MR: Health behaviors among
type. Defense casualty analysis system. Available at https:// service members injured on deployment: a study from the Wounded
www.dmdc.osd.mil/dcas/pages/report_sum_reason.xhtml; accessed Warrior Recovery Project. Mil Med 2021; 186(1–2): 67–74.
December 1, 2020. 21. Woodruff SI, Galarneau MR, McCabe CT, Sack DI, Clouser MC:
2. Chin DL, Zeber JE: Mental health outcomes among military ser- Health-related quality of life among US military personnel injured in
vice members after severe injury in combat and TBI. Mil Med 2019; combat: findings from the Wounded Warrior Recovery Project. Qual
185(5–6): e711–8. Life Res 2018; 27(5): 1393–402.
3. Copeland LA, Zeber JE, Bingham MO, et al: Transition from military 22. Cohen BE, Marmar C, Ren L, Bertenthal D, Seal KH: Association of
to VHA care: psychiatric health services for Iraq/Afghanistan combat- cardiovascular risk factors with mental health diagnoses in Iraq and
wounded. J Affect Disord 2011; 130(1–2): 226–30. Afghanistan war veterans using VA health care. JAMA 2009; 302(5):
4. Howard JT, Stewart IJ, Kolaja CA, et al: Hypertension in military 489–92.
veterans is associated with combat exposure and combat injury. J 23. Dyball D, Evans S, Boos CJ, Stevelink SAM, Fear NT: The association
Hypertens 2020; 38(7): 1293–301. between PTSD and cardiovascular disease and its risk factors in male
5. Swan AA, Amuan ME, Morissette SB, et al: Long-term physical and veterans of the Iraq/Afghanistan conflicts: a systematic review. Int Rev
mental health outcomes associated with traumatic brain injury sever- Psychiatry May 2019; 1–15.
ity in post-9/11 veterans: a retrospective cohort study. Brain Inj 2018; 24. van der Wal SJ, Gorter R, Reijnen A, Geuze E, Vermetten E:
32(13–14): 1637–50. Cohort profile: the Prospective Research in Stress-Related Military
8 MILITARY MEDICINE, Vol. 00, Month/Month 2021Combat Casualties Longitudinal Pilot Study Methods
Operations (PRISMO) study in the Dutch Armed Forces. BMJ Open 32. Galarneau MR, Hancock WC, Konoske P, et al: The navy-marine corps
2019; 9(3): e026670. combat trauma registry. Mil Med 2006; 171(8): 691–7.
25. Kessler RC, Colpe LJ, Fullerton CS, et al: Design of the Army Study 33. Baker SP, O’Neill B, Haddon W, Long WB: The injury severity score:
to Assess Risk and Resilience in Servicemembers (Army STARRS). a method for describing patients with multiple injuries and evaluating
Int J Methods Psychiatr Res 2013; 22(4): 267–75. emergency care. J Trauma 1974; 14(3): 187–96.
26. Bennett AN, Dyball DM, Boos CJ, et al: Study protocol for 34. Kroenke K, Strine TW, Spitzer RL, Williams JBW, Berry JT,
a prospective, longitudinal cohort study investigating the medi- Mokdad AH: The PHQ-8 as a measure of current depression in the
cal and psychosocial outcomes of UK combat casualties from the general population. J Affect Disord 2009; 114(1–3): 163–73.
Downloaded from https://academic.oup.com/milmed/advance-article/doi/10.1093/milmed/usab329/6338456 by guest on 04 December 2021
Afghanistan war: the ADVANCE study. BMJ Open 2020; 10(10): 35. Weathers FW, Litz BT, Keane TM, Palmieri PA, Marx BP, Schnurr PP:
e037850. The PTSD checklist for DSM-5 (PCL-5). Available at http://
27. Skovira JW, Kabadi SV, Wu J, et al: Simulated aeromedical evacuation www.ptsd.va.gov; accessed November 2, 2020.
exacerbates experimental brain injury. J Neurotrauma 2016; 33(14): 36. Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA: The
1292–302. AUDIT alcohol consumption questions (AUDIT-C): an effective
28. Okie S: Traumatic brain injury in the war zone. N Engl J Med 2005; brief screening test for problem drinking. Ambulatory Care Quality
352(20): 2043–7. Improvement Project (ACQUIP). Alcohol use disorders identification
29. Sharma TL, Kerrigan JM, McArthur DL, et al: Flying after concussion test. Arch Intern Med 1998; 158(16): 1789–95.
and symptom recovery in college athletes and military cadets. JAMA 37. Littman AJ, Boyko EJ, Jacobson IG, et al: Assessing nonresponse
Netw Open 2020; 3(11): e2025082. bias at follow-up in a large prospective cohort of relatively young and
30. Woodruff SI, Galarneau MR, Luu BN, Sack D, Han P: A study proto- mobile military service members. BMC Med Res Methodol 2010; 10:
col for tracking quality of life among U.S. service members wounded 99.
in Iraq and Afghanistan: the Wounded Warrior Recovery Project. Mil 38. Teague S, Youssef GJ, Macdonald JA, et al: Retention strategies in lon-
Med 2014; 179(3): 265–72. gitudinal cohort studies: a systematic review and meta-analysis. BMC
31. Watrous JR, Dougherty AL, McCabe CT, Sack DI, Galarneau MR: Med Res Methodol 2018; 18(1): 151.
The Wounded Warrior Recovery Project: a longitudinal examina- 39. NHANES: National Health and Nutrition examination survey
tion of patient-reported outcomes among deployment-injured military homepage. Available at https://www.cdc.gov/nchs/nhanes/index.htm;
personnel. Mil Med 2019; 184(3–4): 84–9. accessed July 12, 2021.
MILITARY MEDICINE, Vol. 00, Month/Month 2021 9You can also read