Rehabilitative Care Alliance - Rehab Care Alliance
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Rehabilitative Care Alliance
Assess & Restore Virtual Forum
November 1, 2018
For audio, you must call in by phone:
(416) 764-8673 or Toll Free: 1-888-780-5892
Passcode: 7677451#
Telephone lines open at 12:55 p.m. and will be muted
Webinar begins at 1:00 p.m.How to participate in the webinar
For audio, you must call in by
phone: (416) 764-8673 or Toll
Free: 1-888-780-5892
Passcode: 7677451#
Telephone lines are muted
The webinar is being recorded and
will be posted to the RCA website
within 1 week
Questions may be entered into the
chat function here for discussion
www.rehabcarealliance.ca 22018 Assess & Restore Virtual Forum
Across the Continuum of Care
www.rehabcarealliance.ca 3Agenda
1:00-1:10 Welcome Charissa Levy
A&R Backgrounder Executive Director, RCA
1:10-1:40 VON SMART Enhanced In-Home Program Mississauga Halton
1:40-2:10 The Home Independence Program (HIP) Central West
2:10-2:40 Central East Virtual Ward and Community Enhanced Central East
Recovery Program
2:40-3:10 Enhanced Service Delivery: Geriatric Care North West
Coordinator/Lead for Senior’s Clinical Pathway
Development
3:10-3:40 Enhancing Assess & Restore Capacity within the Central
Central LHIN
3:40-4:00 Shared Provincial Indicators Gabrielle Sadler
Closing Project Manager, RCA
*Presentations are 20 minutes with 10 minutes Q&A following.
4Assess & Restore Background
Program
o Target frail seniors who have experienced a recent functional loss
that puts them at high risk for long-stay LTC home placement.
o Aim to enhance timely and appropriate access to programs,
increase capacity across all elements of an A&R approach to care
and improve quality of care.
Ministry Investment
o Base Funding
www.rehabcarealliance.ca 5Assess & Restore Background
Project Requirements
o Eligible projects were required to:
• Fit within one of the five elements of an A&R approach to care, which
include: screening, assessment, navigation and placement, intervention
and transitions home; and
• Demonstrate improved A&R outcomes across the province.
o A small number of shared inter-LHIN projects with provincial
scalability have been encouraged, and LHINs are encouraged to
release portions of their funding they cannot use to other LHINs
www.rehabcarealliance.ca 62017/18 A&R Focus
More than 33,000 older adults received care across
28 A&R initiatives
Objectives Across A&R Initiatives:
1) Enhance and improve access to restorative care services for older adults.
2) Move care for older adults from facility-based to community-based,
wherever possible, by implementing proactive models of risk screening and
navigation.
3) Improve outcomes for older adults by implementing best practice care,
including comprehensive geriatric assessment and geriatric interprofessional
rehabilitative care.
4) An additional focus noted in 2017/18 was the development of a regional
strategy to address the operationalization and sustainability of the initiatives.
www.rehabcarealliance.ca 72017-18 A&R Initiatives: Key Messages A cross-sectoral integrated approach to restorative care improves outcomes for community-dwelling older adults Proactive access to comprehensive assessment and restorative interventions improves outcomes and reduces avoidable admissions Geriatric education and senior friendly care are essential components of successful A&R implementation A planned regional strategy with an aligned vision is required to support a population health approach for frail older adults www.rehabcarealliance.ca 8
RCA Annual Forum 2018
Assess & Restore
Knowledge Exchange
MH LHIN Presentation
November 1, 2018
Heather MacArthur, Victoria Order of Nursing
Amy Khan, Mississauga-Halton LHINSMART Enhanced Program
Evidence based gentle exercise program designed to restore frail,
elderly, high risk seniors who have had a recent decline in
functional abilities.
Objectives:
o Restore & improve mobility through exercise
o Improve/maintain functional independence
o Improve/maintain mental health
o Reduce hospital visits
www.rehabcarealliance.ca 10SMART Program
The Program is comprised of 2-in home visits per week for 6 weeks.
1. Referral Form
2. Phone Screening
3. Physician Clearance
4. Initial Assessment (Kinesiologist)
o Physiotherapist if needed
5. Exercise Sessions (Exercise Leaders)
6. Post Assessment (Kinesiologist)
www.rehabcarealliance.ca 11Improving Health Care
Delivery for Older Adults
Developed an upstream approach to promote healthy aging of older
adults, who otherwise might not have the opportunity to participate
in traditional exercise due to access barriers.
Improved health care delivery:
o One-on-one exercise sessions
o Consistency of care
o Exercise Leader
o Time of week/day
www.rehabcarealliance.ca 12Improving Health Care
Delivery for Older Adults
2017-2018 Results
Measurements Average Outcome Comments
Improvements
AUA 0.021 Minimal impact on AUA scores
Frailty Score -0.303 69.7% of clients had no change in their frailty
score. Of the 30.3% of clients that had a change
in their score, 88.9% saw an improvement by 1
point and 9.1% saw a decline
QoL 3.65 82% of clients had an improved QoL score
Berg Balance Scale 7.279 94.6% of clients had an improved BERG outcome
Timed Up & Go -5.353 70% of clients had an improved TUG score
www.rehabcarealliance.ca 13Developing
Integrative Models of Care
Engagement with cross-sectoral health care services including:
o Care Coordinators
oMH LHIN, Central Registry,
o Physicians
o Family Doctor, Geriatricians
o Hospitals
o Trillium Health Partners, Credit Valley Hospital
o Health Service Providers
Challenges:
o Primary Care Involvement
o Meeting eligibility of Program
o Age
o Service Area
www.rehabcarealliance.ca 14Key Learnings Issues for rehabilitative care for older adults: o Hospital admissions o Illness o Aches & Pains Identified Next Steps After Completing the Program: o Conduct Exercises Independently o Train PSW or Caregiver o Transition into group exercises classes www.rehabcarealliance.ca 15
Opportunities to spread an
A&R approach to care
o Opportunities for Home Exercise programs to partner with
community physiotherapy clinics
o Improving Community Home Exercise programs to include
pre and post standardized assessments to monitor progress
www.rehabcarealliance.ca 16Questions? www.rehabcarealliance.ca 17
RCA Annual Forum 2018
Assess & Restore
Knowledge Exchange
CW LHIN Presentation
November 1, 2018
Aruna Mitra
Director Home and Community CareHome Independence Program
2017/18
What we set out to do…
o To build on positive outcomes realized by Legacy Central
West CCAC Home Independence Programs (HIP) offered in
2015/16 and 2016/17 by:
• Streamlining program processes and resources
• Establish a sustainable approach to A & R in Central West LHIN
• Ensure program made available to patients who would most
benefit
• Include more robust outcome measures
www.rehabcarealliance.ca 19Learnings from past HIP experience Opportunity to improve centralized screening and oversight resulted in inappropriate patients admitted to program Availability of PSW as part of service package became an access issue for patients who had no other available option for PSW services which also impacted on program outcomes Education needs for providers to reinforce and support a restorative approach in home care delivery www.rehabcarealliance.ca 20
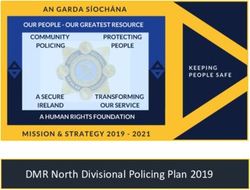
Home Independence Program
OT
oversight
PATIENT
GOAL
PSW PT
An 8-week home-based restorative care program designed using a best
practice approach to improve seniors’ independence and prevent functional
decline.
Patient program is led by an Occupational Therapist (OT) with activities
assigned to PSW
Physiotherapy services are also available and the treatment was completed
by personal support workers under the supervision of the physiotherapists.
Patients’ motivation is a significant element of the program and the OT’s
worked collaboratively with patients to establish patient centered goals.
www.rehabcarealliance.ca 21HIP: Program Improvements
1. Refined patient criteria & intake process to include OT screening and
Frailty Index
2. Standardized protocols implemented for communication between
therapist and PSW
3. Increased client centered approach with therapists – COPM
implemented & other interventions depending on the goals identified by
the patients.
4. Dedicated Rehabilitation Care Coordinator provided operational
oversight; SPO liaison; facilitated patient teleconferences
5. Orientation/ Training Session for all Rehab providers, including hands on
workshop conducted by an Rehab Care Coordinator and training
provided by a community OT for PSWs re importance of restorative
approaches
6. Refined process map to clarify processes and roles
7. Tracking & reports to support centralized program monitoring by rehab
Coordinator
www.rehabcarealliance.ca 22Developing
Integrative Models of Care
Support continuum of care through hospital discharge
support for vulnerable seniors
Community access through Home & Community Care
Coordinators & Primary Care
Integrative approach optimizing by restorative rehab
approach utilizing cost effective model (OT/ PT PSW)
www.rehabcarealliance.ca 23Program Utilization
HIP 2017/18
Total # patients 200
Average Age 77
Rockwood Frailty Score 5 & 6 (mild to moderate frailty)
Length of Stay in Program 8 weeks (56 days)
OT Average Utilization per patient 3 visits
PT Average Utilization per patient 3 visits
PSW Average Utilization per patient 12 visits
Budget $376,000
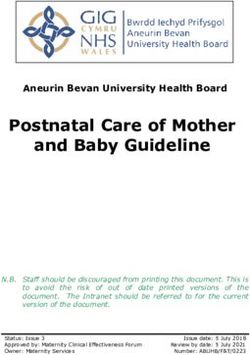
www.rehabcarealliance.ca 24HIP Referral Sources
11% 10%
3%
14%
Primary Care
Community
Hospital ED
Hospital Inpatient
6%
Hospital Outpatient
Other LHIN
56% n= 200
www.rehabcarealliance.ca 25Improving Health Care
Delivery for Older Adults
Outcome Measures
COPM Performance & Timed Up and GO
Satisfaction 42
6.1 6.1
22
3.1 2.9
INTAKE DISCHARGE
INTAKE DISCHARGE
COPM-P COPM-S
Performance Score Change: 3
TUG Score Improvement: 20
Satisfaction Score Change: 3.2
www.rehabcarealliance.ca 26Improving Health Care
Delivery for Older Adults
Reduced Falls & Prevented Hospitalization
Reduction in Falls Reduction in ER Visits
61% 61%
12% 10%
INTAKE DISCHARGE INTAKE DISCHARGE
49 % Reduction 51% Reduction
www.rehabcarealliance.ca 27Improving Health Care
Delivery for Older Adults
Self-Reported overall outcome on general
wellbeing
45%
29%
22%
3%
WORSE SAME SOMEWHAT BETTER MUCH BETTER
74 % reported wellbeing as “somewhat better” & “much better”
www.rehabcarealliance.ca 28Key Learnings The importance of consistency in scheduling of PSW’s Availability of PSW’s (shortage in Ontario and availability in all sub- regions) impacted program Training of SPOs and PSW in Restorative care approach is key to program success Oversight by Rehab Care Coordinator to monitor outcomes We are exploring role of incorporating OTA and PTA Sub-region alignment of the Service Provider Organization may provide additional efficiencies Funding limitation reduced availability of program www.rehabcarealliance.ca 29
Opportunities to spread an
A&R approach to care
Model can be incorporated across other LHINS to support
transition for frail seniors from hospital to home for
Optimizing role of OT and PT through training of PSWs to
practice skills (rather than “doing for”)
Rehab Coordinator Role
Clinical tools and resources
o HIP Protocols
o Process Map
o Education Training Materials
www.rehabcarealliance.ca 30Acknowledgements Archana Arun, Rehabilitation Care Coordinator Jackie Minezes, Manager Home and Community Care Kimberley Floyd, VP Home and Community Care Home and Community Care Coordinators in community and hospital settings CW LHIN Decision Support & Finance teams www.rehabcarealliance.ca 31
Questions? www.rehabcarealliance.ca 32
RCA Annual Forum 2018
Assess & Restore
Knowledge Exchange
CE LHIN Presentation
November 1, 2018
Liora Krinsky
Clinical Practice Leader, Scarborough Health Network
Angie Saini
Director of Care, Carefirst Seniors and Community Services AssociationA Soft Landing: The Patient Journey from
Hospital to Community Care
Scarborough Health Network (SHN) and Carefirst Seniors and
Community Services Association’s Transitional Care Centre (TCC)
established a partnership to provide patients and caregivers
seamless transitions across the health care continuum from acute
care (SHN) to a facility-based Assess and Restore intervention (TCC)
then back into the community.
www.rehabcarealliance.ca 34A Soft Landing: The Patient Journey from
Hospital to Community Care
Program Objectives:
o Extend beyond strengthening, reconditioning and returning to previous
level of functioning
o Provides participants and caregivers with access to services to improve
or maintain their abilities to enable them to continue to live
independently in the community including home care, exercise and falls
prevention classes, and chronic disease management programs.
o Collaborates with primary care to manage clients and ensure appropriate
follow-up post-discharge.
o This restorative program is an innovative model that provides wrap
around care that continues once the participants have been discharged
home from TCC
www.rehabcarealliance.ca 35A Soft Landing: The Patient Journey from
Hospital to Community Care
The partnership between SHN and Carefirst provides seniors who require
reconditioning after their acute medical illness access to physiotherapy, nursing,
personal support, social work and community support services.
This A& R Intervention has two key components:
1) Virtual Ward Program (VW): Assist the patient in meeting VW’s five
milestones:
o follow-up with primary care;
o medication reconciliation;
o tests/specialist appointments;
o health education; and
o linkage to appropriate community services
2) Enhanced Recovery Program: Individual treatment for those experiencing
significant cognitive/physical/functional impairment; health teaching i.e., falls
prevention, energy conservation; and functional training i.e. gait, transfer and
home safety equipment training
www.rehabcarealliance.ca 36A Soft Landing: The Patient Journey from
Hospital to Community Care
o SHN, Carefirst, and the Central East LHIN ensures individuals are
supported in a timely, coordinated and seamless manner as they move
from SRH to Carefirst TCC and then back into the community with the
necessary supports in place to enable them to continue to live in their
homes for as long as possible.
www.rehabcarealliance.ca 37A Soft Landing: The Patient Journey from
Hospital to Community Care
o Participant/caregiver goals are identified prior to discharge by the inter-
professional hospital team. Once the participant transitions to TCC, the
care team then leverages all available resources in order to assist
participants in achieving their goals and reintegrating them back into the
community, including:
• Meals on Wheels,
• LHIN’s Telehomecare program for participants with CHF or COPD
• Carefirst’s COPD Community Rehabilitation program,
• Geriatric Assessment and Intervention Network or GAIN team,
• Diabetes Education Program
• Community exercise and falls prevention classes
• Caregiver support groups, etc.
www.rehabcarealliance.ca 38Improving Health Care
Delivery for Older Adults
The collaboration between SHN and Carefirst was developed to ensure that
seniors who are at high risk for not being able to return home, receive the
reconditioning to enable them to continue to live in the community
independently. This restorative program is an innovative model that allows:
• A safe, comfortable environment for seniors to gain their strength,
mobility, and confidence
• Access to an interdisciplinary team that can manage their psychosocial
and physiological needs after an acute hospitalization which can be
overwhelming for both seniors and their caregivers
• For a more comprehensive look at the participants’ and caregivers’ needs
and subsequent access to all community resources including LHIN
services to prevent them from returning to hospital
• Additional benefit of much needed respite for caregivers
www.rehabcarealliance.ca 39Developing
Integrative Models of Care
The collaboration between SHN and Carefirst transcends the
boundaries between acute care and community care however it is
not without its challenges including the following:
• Access to information: difficult to gather medical and social history
particularly for those admitted from ER. Also for this reason, difficult to
assess whether they are appropriate for the program. To resolve this,
Carefirst is provided with access to appropriate hospital IT platforms and is
in the midst of trying to secure access to ConnectingOntario
• Difficult to coordinate admissions to TCC on evenings and weekends
• Initially client may have shown potential for rehabilitation but plateaued,
making discharges back into the community more difficult
• Participants who have high social needs, making discharge planning more
complex. do not have a firm discharge destination or who’s discharge
destination changes once on TCC
www.rehabcarealliance.ca 40Developing
Integrative Models of Care
The partnership does have components that work well:
• Face to face meetings with potential participants and caregivers provides
warm transfer from hospital to TCC
• Social workers from both organizations collaborate with
participants/caregivers to ensure a smooth transition and provide clear
expectations
www.rehabcarealliance.ca 41Developing
Integrative Models of Care
Lessons Learned:
• Target population was reevaluated as the program proved inappropriate
for high need participants
• Referral form was modified to reduce duplication in the collection of
information from the client/caregiver. SHN provides basic information to
provide general picture, Carefirst does thorough face to face assessment
in hospital
• Lab work services was initially a barrier but has since become
incorporated into pathway
• Participants are at a higher risk of readmissions, but readmission rate
remained the same as those discharged from hospital. Mitigation: NP
hired at Carefirst to provide more robust clinical oversight
www.rehabcarealliance.ca 42Developing
Integrative Models of Care
Opportunities for spread:
The collaboration and integration of acute care and community
care is essential in ensuring that patients are discharged from
hospitals in a safe, effective manner that optimizes their well-
being, reduces caregiver burden, reduces length of stay and
prevents readmissions.
www.rehabcarealliance.ca 43Key Learnings
Capacity planning:
o SHN’s goal has been to maintain a constant occupancy of 3 beds.
Carefirst is able to provide additional beds if it has the capacity to do
so. This has not yet been an issue. As we expand to other SHN sites, it
is something to consider
System gaps
o There is limited access/funding for this type of transitional care
setting in the Central East LHIN. Funding for these beds comes from
the operational budget of SHN.
o There are other ‘transitional care’ settings but most do not have
access to as comprehensive a basket of restorative and community
support services as that offered at Carefirst
Next steps:
o Increase hospital funding for such programs as part of total joint or
chronic disease pathway as a means to improve patient/caregiver
experience, reduce length of stay, reduce readmission rate, and
improve population health
www.rehabcarealliance.ca 44Opportunities to spread an
A&R approach to care
Key Success Factors:
• Integration of the acute care sector with community-based inpatient
rehabilitation and community support services to provide restorative
then supportive care to sustain seniors/caregivers once they return home
• Focus on prevention:
Leverage chronic disease management programs to provide patients and
caregivers the resources/education/tools they require to better manage their
health care conditions
Connect patients and caregivers with other community programs that
optimize their physical/emotional/cognitive well-being like exercise and falls
prevention classes, Adult Day Program, etc.
Ensure follow-up with primary care and provide clinical oversight in the
interim
• Collaboration across sectors: primary care, acute care, community care
including the LHIN share the same goals –enable patients/caregivers to
thrive in the community while contributing to the sustainability of the
health care system
www.rehabcarealliance.ca 45Questions? www.rehabcarealliance.ca 46
RCA Annual Forum 2018
Assess & Restore
Knowledge Exchange
NW LHIN Presentation
November 1, 2018
Susan Veltri RN., Geriatric Care Coordinator
Emergency Identified Fast Track ServiceEmergency Identified Fast
Track Service
Identification of “At Risk Seniors”
who access the Emergency Department and
implementation of a Clinical Pathway aimed at
enhanced care for Frail Seniors through referral to
the Geriatric Care Coordinator
Pathway includes:
o Rapid access to geriatric consultation and enhanced community care
and other related service with the objective of preventing avoidable
ED visits, preventing hospitalization and reducing length of stay
o Primary Care while not directly related to the care at the hospital
have been included in the Clients’ as the person progresses through
the pathway
www.rehabcarealliance.ca 48Emergency Identified Fast
Track Service
“Frail Senior” patient aged 65+ and exhibiting any
symptoms indicating risk presents to TBRHSC ED
Patient presents with :Cognitive Impairment/Delirium/Dementia,
Anxiety/Depression, Poly-pharmacy/Medication Issues, Psychosocial
Issues/Caregiver Stress, Falls/Weakness/Mobility Issues, Behavioral
Difficulties, Functional Decline/Frailty, Medical Concerns/Multiple Co
morbidities, Complex Medical Issues, Weight Loss/Nutritional
Concerns, Infection, Pain, Discharge plan follow-up, Fractured
Hips/Pelvis, Safety Concerns, Frequent Emerge Visits and/or Multiple
Hospital Admissions, Any Other Concerns
www.rehabcarealliance.ca 49Emergency Identified Fast
Track Service
Medical Stability Not safe for home
TBRHSC ED to SJCG Inpatient Geriatric Rehab Bed
Medical Stability Safe to go home
Geriatric Care Coordinator
Facilitation of appointment at SJCG Rapid Access Geri Clinic
Completion of CAM, Frailty, PPS, Depression Screen and Electronic Geriatric
Intervention and any other assessments as required
GCC completes Home Care RR RN referral to NW LHIN
GCC will make other referrals as appropriate to community agencies
Home Care Rapid Response RN
NW LHIN RR RN completes CAM, Frailty, PPS standardized home assessment
and medication reconciliation
All information gathered by the GCC and RR RN are forwarded to the Geriatric
Clinic prior to the Clients appointment
www.rehabcarealliance.ca 50Improving Health Care
Delivery for Older Adults
Improved Health Care Delivery
o Since the Clinical Pathway Process begun patients have received the benefit
of rapid access to Geriatric Consultation and resultant in-patient rehab post
the appointment or on-going follow-up with the geriatrician as well as
medical care specifically designed for the aging population
o Since the Pathway was established mid September 2017 until mid
September 2018 Fifty Six (56) patients were enrolled in the process there
by either preventing admission to hospital or promoting discharge from an
overflow bed in the ED
o Emergency Department Physicians were very pleased with the process and
engaged with Rapid Geriatric Consultation as an alternative to hospital
admission
o Many concerning issues were identified through the process and therefore
community service implemented to meet the clients ongoing needs to
assist this group of Seniors to remain at Home
o TBRHSC, SJCG and the NW LHIN Home Care Division worked as a
Collaborative Team in the enhancement of care for the identified “At Risk
Seniors”
www.rehabcarealliance.ca 51Developing
Integrative Models of Care
Collaboration between TBRHSC, SJCG and NW LHIN
o One of the biggest challenges in working together on the
Pathway was communication and education to the multiple
health care providers who were involved in the process
o Another process problem was that it was somewhat person
dependant – either Geriatric Care Coordinator, Geriatrician or
RR RN availability
o Most appointments were scheduled within a week time frame
o Patients and families were very pleased with the process
o Emergency department staff and doctors were very pleased
with the addition and assistance from the Pathway Team
www.rehabcarealliance.ca 52Key Learnings
o Capacity and ability to identify then serve the growing number of
Seniors in our community is key. TBRHSC has a very busy ED and
many of the patients who present are over 65 years
o Gaps identified : 24 X 7 coverage of Team members, availability of
geriatricians to meet the demand, availability of community
resources to meet the needs of our aging population
o Ability of the system to adapt to the varying numbers of referrals –
example: some weeks there were multiple referrals and other weeks
there were zero
o In the coming months TBRHSC and SJCG will enhance the Pathway
work through the addition of an additional GCC for extended hours
and weekends as well as in home support through a OT and/or PT
home visit
www.rehabcarealliance.ca 53Opportunities to spread an
A&R approach to care
o Clinical tools and resources
o The GCC and the RR RN both used and forwarded assessments to
the Geriatrician including the CAM, Depression Screen, Cognition
Screening, Frailty and PPS as well as Medication Reconciliation and
Comprehensive Clinical Assessments
o A consistent approach was key to the team members
o Information and collaboration occurred between TBRHSC, SJCG, NW
LHIN and Family Care Providers in a consistent approach to patient
care
o Primary Care Providers were included in the process especially
surrounding medication changes/additions that occurred either at
the hospital or the Geri Clinic
www.rehabcarealliance.ca 54Questions? www.rehabcarealliance.ca 55
RCA Annual Forum 2018
Assess & Restore
Knowledge Exchange
Central LHIN Presentation
November 1, 2018
Susan Woollard
Interim Vice President Clinical Programs, Quality and Risk, Chief Nursing Executive
North York General Hospital
Mary Burello
Director, Home and Community CareAssess and Restore Assess and Restore model developed in partnership between Central LHIN and North York General Hospital The purpose of the Assess & Restore (A&R) program is to identify frail seniors who have the potential to regain functional ability as a result of illness or decline in health. Through a system approach, the goal for the patient is to regain functional independence to a point that they can safely return home and stay in the community. www.rehabcarealliance.ca 57
Project Description
Foundational elements:
Hospital
The MOVE Project
Hourly Rounding and Bedside Reporting
Electronic Confusion Assessment Method (eCAM) Tool
Malnutrition Screening Tool
Assessment Urgency Algorithm (AUA) Tool
Weekend Mobilization & Activation Team
Enhanced client rehabilitative services in hospital and home
Dedicated Care Coordinator role in hospital and community
Community
Specialized Geriatric Services (SGS)
Single provider agency supporting community in-home services
Dedicated Care Coordinator
www.rehabcarealliance.ca 58Improved Health Care
Delivery for Older Adults
Benefits of Program
Early identification in ED using AUA Tool (assessment urgency algorithm)
Standardized level of rehab services in the inpatient services at NYGH
Enhanced rehab services at home through Central LHIN Home and
Community Care
Consistent Care Coordinator from hospital to home
Follow up post discharge with Outpatient Services at North York Seniors
Health Centre (Assess and Restore therapy – modified Day Hospital )
Measuring outcomes
Primary Care Follow up
Putting our arms around the patient from beginning to end of program
www.rehabcarealliance.ca 59Indicators & Outcomes
An increase in inpatient therapies compared to baseline:
✓✓ 40% more physiotherapy
✓✓ 52% more occupational therapy
✓✓ 127 interventions completed by registered dietitians on weekends
For patients who completed the Assess and Restore program,
significant improvement was noted in:
CHESS Scale
✓✓ Berg Balance Scale
✓✓ MAPLe Priority Levels
31% ALC rate for post-acute inpatient rehabilitative care (Medicine cases only)
7% Unplanned readmission to hospital within 30 days of discharge
1% Unplanned, less urgent emergency department visits within 30 days of
hospital discharge
www.rehabcarealliance.ca 60Indicators & Outcomes (continued) SYSTEM-LEVEL INDICATORS: ✓✓ Timed Up and Go Test ✓✓ Tinetti Gait and Balance Assessment Tool ✓✓ Activities of Daily Living Self-Performance Hierarchy Scale (RAI-HC) CONCLUSION: Improvement noted in rehab functional scales and outcome measures of the RAI-HC, including Time Up and Go Test and Activities of Daily Living Hierarchy. Patients satisfaction was very high with the comprehensive care and outcomes. www.rehabcarealliance.ca 61
Developing
Integrative Models of Care
Challenges Successes
Large numbers of staff to be Partnership with Central
trained in hospital and LHIN Home and Community
community Care
LHIN boundaries for Self-assessment with
providing Home and current services
Community Care follow up Knowledge translation and
Transportation to follow-up coaching across the LHIN
activities (road show model)
Determining appropriate Tool Kit
patients for program
www.rehabcarealliance.ca 62Key Learnings Engage stakeholders early Share outcomes with team members Key foundational elements are building blocks to growing your own Assess and Restore program System integration is the right pathway for patients Benefits of focused co-ordination and good communication for discharge planning Culture of Senior Friendly is rewarding and exciting www.rehabcarealliance.ca 63
Opportunities to spread an
A&R approach to care
www.rehabcarealliance.ca 64Questions? www.rehabcarealliance.ca 65
2017-18 Assess & Restore Shared
Provincial Indicators
66Summary of Recommended
A&R Provincial Indicators
Indicator Home &
Primary Emergency Bedded
within MOH Community
Proposed Provincial A&R Indicator Report
Care
Care
Department Care
Initiatives Initiatives Initiatives
Template Initiatives
1. Volume of patients/caregivers served
2. % admissions to rehabilitative care beds that were
directly admitted from community/ED
3. % of unplanned readmission to hospital within 30
days of discharge from hospital
4. % of unplanned, less-urgent ED visit within the first
30 days of discharge
5. ALC Rate for A&R Patients
6. Improved Function (ADLs)
7. Rate of Discharge Home vs Baseline or other
Comparator
8. Referral rate for community-dwelling frails seniors
screened at-risk for loss of independence
www.rehabcarealliance.ca 67Volume of
Patients/Caregivers Served:
Community Base Programs
TC LHIN - Independence at Home (IAH) Program - UHN & SHS
TC LHIN - Providence Health Care Assess & Restore Services
TC LHIN - West Park Assess & Restore
NSM LHIN - Enhanced SMART and Transitions of Care
CH LHIN - Central Intake for Specialized Geriatric Services
CE LHIN - CATCH (Care After The Care in Hospital) Program
CE LHIN - Virtual Ward & Community Enhanced Recovery Program
CEN LHIN - Enhancing A&R Capacity Central LHIN - Out-patient
CEN LHIN - Enhancing A&R Capacity Central LHIN - In Home
Total of 10,265
MH LHIN - Assess and Restore Clinic – HHS patients served in
MH LHIN - Community Step-Up Clinic A&R Community
MH LHIN - VON SMART Enhanced In-Home program Based Programs
CW LHIN - Home Independence Program
WW LHIN - Rapid Recovery Therapy Program (RRTP)
SW LHIN - Evaluation of Implementing Proactive Screening with…
SW LHIN - Geriatric Ambulatory Access Team
0 100 200 300 400 500 600 700 800
2016-17 2017-18
68Volume of
Patients/Caregivers Served:
Hospital-Based Programs
SE LHIN - Quinte Health Care
TC LHIN - Salvation Army Toronto Grace Health Centre Integrated… Total of 23,064
NW LHIN - St. Joseph's Care Group Geriatric Assessment and… patients served in
NW LHIN - Thunder Bay Regional Enhanced Service Delivery:…
A&R Hospital-Based
NW LHIN - Dryden Regional Weekend and Enhanced OT for A&R…
NW LHIN - Assess & Restore Expansion at Sioux Lookout Meno Ya…
Programs
CH LHIN - The Ottawa Hospital Pilot Direct Admissions to Sub-…
CH LHIN - The Ottawa Hospital 7 day/week Therapy in ABI Rehab
CE LHIN - Ross Memorial Hospital Assess & Restore Mobile team…
CE LHIN - Northumberland Hills Assess and Restore Intervention
CEN LHIN - Enhancing A&R Capacity Central LHIN
HNHB LHIN - Seniors Mobile Assess & Restore Teams (SMART)
SW LHIN - London Health Sciences Enhanced Rehabilitative Care…
ESC LHIN - Windsor Regional Oulette Campus Mobilization of…
ESC LHIN - Windsor Regional Metropolitan Campus Mobilization…
ESC LHIN - Erie Shores Mobilization of Vulnerable Elders (MOVE)…
ESC LHIN - Chatham Kent Mobilization of Vulnerable Elders…
ESC LHIN - Bluewater Health Mobilization of Vulnerable Elders…
0 500 1000 1500 2000 2500 3000 3500 4000 4500
2016-17 2017-18
69Percentage of admissions to
rehabilitative care beds that were
directly admitted from community/ED
The following sites reported number of direct
TC LHIN - Providence Health Care Assess & Restore admissions:
Services NE LHIN – Assess & Restore/Geriatric
Rehabilitative Care – 33 admits
NW LHIN – Thunder Bay Regional Enhanced
Service Delivery – 16 admits
TC LHIN – Providence Health Care Assess &
Restore Services – 167 admits
NW LHIN - St. Joseph's Care Group Geriatric Assessment
and Rehabilitative Care
CE LHIN - Northumberland Hills Assess and Restore
Intervention
0 10 20 30 40 50 60
2016-17 2017-18
70Average FIM® Total Function Score Change
NW LHIN - Assess & Restore
Expansion at Sioux Lookout Meno Ya
Additional validated
Win Health Centre tools used to report
functional changes:
• Timed Up and Go
CH LHIN - The Ottawa Hospital 7
day/week Therapy in ABI Rehab
• Berg Balance Scale
• 2 Minute Walk Test
• Grip Strength
CE LHIN - Ross Memorial Hospital • COPM
Assess & Restore Mobile team
(ARM) • ASHA NOMS FCM
• MOCA
• Chedoke-McMaster
CE LHIN - Northumberland Hills
Stroke Assessment
Assess and Restore Intervention
• Barthel ADL Index
0 5 10 15 20 25
2016-17 2017-18
71Rate of Discharge Home
TC LHIN - Assess and Restore Initiative - Providence, St. Joseph…
NW LHIN - Dryden Regional Weekend and Enhanced OT for A&R…
NW LHIN - Assess & Restore Expansion at Sioux Lookout Meno Ya…
HNHB LHIN - Seniors Mobile Assess & Restore Teams (SMART)
ESC LHIN - Windsor Regional O Mobilization of Vulnerable Elders…
ESC LHIN - Windsor Regional M Mobilization of Vulnerable Elders…
ESC LHIN - Erie Shores Mobilization of Vulnerable Elders (MOVE)…
ESC LHIN - Chatham Kent Mobilization of Vulnerable Elders…
ESC LHIN - Bluewater Health Mobilization of Vulnerable Elders…
CE LHIN - Ross Memorial Hospital Assess & Restore Mobile team…
CE LHIN - Northumberland Hills Assess and Restore Intervention
CE LHIN - Virtual Ward & Community Enhanced Recovery Program
CEN LHIN - Enhancing A&R Capacity in Central LHIN
0 10 20 30 40 50 60 70 80 90 100
2016-17 2017-18
72Questions? www.rehabcarealliance.ca 73
Thank you for joining our 2018
Assess & Restore Virtual Forum
Please complete the evaluation
74You can also read