Risk models to improve safety of dispensing high-alert medications in community pharmacies
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Research
Risk models to improve safety
of dispensing high-alert
medications in community
pharmacies
Michael R. Cohen, Judy L. Smetzer, John E. Westphal,
Sharon Conrow Comden, and Donna M. Horn
Received September 30, 2010, and in revised
Abstract form June 17, 2011. Accepted for publication
July 22, 2011.
Michael R. Cohen, BSPharm, MS, FASHP, is
Objectives: To determine whether sociotechnical probabilistic risk assessment President; and Judy L. Smetzer, RN, BSN,
can create accurate approximations of detailed risk models that describe error path- FISMP, is Vice President, Institute for Safe
ways, estimate the incidence of preventable adverse drug events (PADEs) with high- Medication Practices, Horsham, PA. John E.
Westphal, BS, is a consultant; and Sharon
alert medications, rank the effectiveness of interventions, and provide a more infor- Conrow Comden, BS, MPH, DrPH, is a con-
mative picture of risk in the community pharmacy setting than is available currently. sultant, Outcome Engenuity, LLC, Plano, TX.
Design: Developmental study. Donna M. Horn, BSPharm, is Director of Pa-
tient Safety for Community Pharmacy, Insti-
Setting: 22 community pharmacies representing three U.S. regions. tute for Safe Medication Practices, Horsham,
Participants: Model-building group: six pharmacists and three technicians. PA.
Model validation group: 11 pharmacists; staff at two pharmacies observed. Correspondence: Judy Smetzer, RN, BSN,
Intervention: A model-building team built 10 event trees that estimated the inci- FISMP, Institute for Safe Medication Practic-
dence of PADEs for four high-alert medications: warfarin, fentanyl transdermal sys- es, 200 Lakeside Dr., Suite 200, Horsham, PA
19044. Fax: 215-914-1492. E-mail: jsmetzer@
tems, oral methotrexate, and insulin analogs. ismp.org
Main outcome measures: Validation of event tree structure and incidence of
Disclosure: The authors declare no con-
defined PADEs with targeted medications. flicts of interest or financial interests in any
Results: PADEs with the highest incidence included dispensing the wrong dose/ product or service mentioned in this article,
strength of warfarin as a result of data entry error (1.83/1,000 prescriptions), dis- including grants, employment, gifts, stock
holdings, or honoraria.
pensing warfarin to the wrong patient (1.22/1,000 prescriptions), and dispensing an
inappropriate fentanyl system dose due to a prescribing error (7.30/10,000 prescrip- Funding: Agency for Healthcare Research
and Quality contract no. 1P20HS017107.
tions). PADEs with the lowest incidence included dispensing the wrong drug when
filling a warfarin prescription (9.43/1 billion prescriptions). The largest quantifiable Previous presentations: 10th International
Probabilistic Safety Assessment & Manage-
reductions in risk were provided by increasing patient counseling (27–68% reduc- ment Conference, Seattle, WA, June 7–11,
tion), conducting a second data entry verification process during product verification 2010, and Agency for Healthcare Research
(50–87% reduction), computer alerts that can't be bypassed easily (up to 100% re- and Quality Annual Conference, Bethesda,
MD, September 14, 2009.
duction), opening the bag at the point of sale (56% reduction), and use of barcoding
technology (almost a 100,000% increase in risk if technology not used). Combining
two or more interventions resulted in further overall reduction in risk.
Conclusion: The risk models define thousands of ways process failures and be-
havioral elements combine to lead to PADEs. This level of detail is unavailable from
any other source.
Keywords: Risk assessment, high-alert medications, preventable adverse drug
events, event trees.
J Am Pharm Assoc. 2012;52:584–602.
doi: 10.1331/JAPhA.2012.10145
584 • JAPhA • 5 2 : 5 • S e p / O c t 2012 www.j aph a. or g Journal of the American Pharmacists Associationrisk models in community pharmacies Research
A
dverse drug events (ADEs), which are defined as inju- 60 million errors during the dispensing of 4 billion prescrip-
ries from drug therapy,1 are among the most common tions annually.2,17
causes of harm during the delivery of health care.2 At Few studies have reported the frequency of harm caused
least a quarter of these events are preventable.1,3,4 On an an- by PADEs in the community pharmacy setting. Ghandi et al.12
nual basis, up to 450,000 inpatients experience a preventable found that 5% of ambulatory patients experienced a PADE with
ADE (PADE).3–5 PADEs lead to about 4% (range 1.4–15.4%) of medications dispensed from community pharmacies. Gurwitz
hospital admissions.6–12 et al.18 identified that almost one-half of serious, life-threaten-
Few prospective data detail the incidence of PADEs in am- ing, or fatal ADEs related to medications dispensed from phar-
bulatory patients.12 Four retrospective studies that examined macies were preventable. Several studies suggested that dos-
community pharmacy dispensing errors using similar defini- ing errors occur frequently and have the highest rate of clinical
tions, detection methods, and expression of incidence rates re- significance among types of medication errors.19–22 An estimate
ported a wide range of errors (from 1.7% to 24%).13–16 The low- in 2000 determined that hospital admissions caused by PADEs
est dispensing error rate (1.7%) translates to approximately accounted for $121.5 billion or 70% of total costs of drug-re-
four errors per 250 prescriptions per pharmacy per day2 or to lated problems in the United States.23
The drugs associated with the most harmful PADEs in
acute care settings were first coined “high-alert” medications
by the Institute for Safe Medication Practices (ISMP) in 1998.24
High-alert medications carry a major risk of causing serious
At a Glance injuries or death to patients if misused. Errors with these drugs
Synopsis: A model-building team built 10 event are not necessarily more common, but the consequences are
trees that estimated the incidence of preventable ad- devastating.25–27 Appendix 1 (electronic version of this article,
verse drug events (PADEs) for four high-alert medica- available online at www.japha.org) notes the characteristics,
tions and found that sociotechnical probabilistic risk medications, and types of errors involved in patient harm from
assessment (ST-PRA) was able to define thousands of PADEs in the ambulatory setting.
ways process failures and behavioral elements com- Traditionally, health care systems have relied on root
bine to lead to PADEs. PADEs with the highest inci- cause analysis (RCA) and failure mode and effects analysis
dence included dispensing the wrong dose/strength (FMEA) to understand the risks involved in prescribing, dis-
of warfarin as a result of data entry error (1.83/1,000 pensing, and administering medications.28–30 RCA and FMEA
prescriptions) and dispensing warfarin to the wrong are the most basic types of risk analysis that focus largely on
patient (1.22/1,000 prescriptions). The greatest quan- system and process errors.30–35 Both offer qualitative informa-
tifiable reductions in risk were provided by factors tion about risk and error, but neither helps quantify the level
such as increasing patient counseling (27–68% reduc- of risk or model the dependencies and effects of combinations
tion) and conducting a second data entry verification of failures.36 Sociotechnical probabilistic risk assessment (ST-
process during product verification (50–87% reduc- PRA) is a prospective technique that advances the qualitative
tion). work of FMEA and RCA into a quantitative realm by linking
Analysis: The ST-PRA models created in this process failures with estimates of human error and behavioral
study were effective at identifying dispensing system norms, yielding a more accurate picture of why and how often
vulnerabilities that were largely correctable before these failures affect patient outcomes.28,30,36,37 Online Appendix
reaching patients given environmental, technologi- 2 summarizes the advantages of ST-PRA over FMEA and RCA.
cal, system/process, and behavioral conditions that ST-PRA, which is derived from a probabilistic risk assess-
are within the reach of most community pharmacies ment (PRA) tool that originated in the mid-1970s to improve
and pharmacy staff. A sensitivity analysis identified safety in nuclear power plants, allows all possible combina-
that using automated dispensing and barcoding tech- tions of task or system failures to be considered in combina-
nology, conducting a second data entry verification tion with one another.36–40 Although PRA is predominantly used
process during final product verification, counseling to model mechanical systems, ST-PRA is especially suited for
patients more frequently and effectively, opening the modeling human systems and is the more appropriate tool
bag at the point of sale to view all filled prescriptions, for health care.28,30,36,37 Although ST-PRA use in health care
and other interventions will reduce prescribing and remains relatively new,28,30,36,37,41–44 a previous study using
dispensing errors that reach patients by as much as ST-PRA to model medication system risk in long-term care
87%, or more when combining several interventions. strongly suggests that application of this process to high-alert
The authors noted that the interventions discussed medications dispensed from community pharmacies will be
here are not meant to suggest and/or establish a successful in assessing risks and gauging the impact of system
standard of care for community pharmacies; instead, and behavioral changes on these risks.30,36
they are intended to represent future patient safety
improvements.
Journal of the American Pharmacists Association www. japh a. or g S e p /O c t 2012 • 52:5 • JAPhA • 585Research risk models in community pharmacies
Objectives Steps in the modeling process
The objectives of this study were to (1) identify a list of high- Recruit the modeling team. A voluntary modeling team was
alert medications dispensed from community pharmacies; recruited using a noncoercive protocol; all members were from
(2) determine whether ST-PRA can create accurate approxi- different pharmacies.
mations of detailed risk models that describe error pathways, Build a process and control system map. A process
estimate the incidence of PADEs involving high-alert medica- and control map of the pharmacy dispensing process was cre-
tions dispensed in community pharmacies, and rank the effec- ated. Observations in pharmacies and discussion with pharma-
tiveness of interventions to prevent PADEs; and (3) determine cy staff verified that any differences in the workflow among the
whether ST-PRA provides a more informative picture of risk sample pharmacies were minimal, allowing agreement upon
in the community pharmacy setting than currently available one standard process map. The map is a visual aid that clear-
through typical sources, such as retrospective event reporting, ly shows how work inputs, outputs, and tasks are linked and
RCA, and FMEA. shows the embedded control systems that aid in the prevention
and detection of errors.
Methods Mapping occurred at two levels. First, using an iterative
The Temple University Office for Human Subjects Protections progression, the dispensing process steps and decision points
Institutional Review Board approved the study before initia- were identified and linked according to the current workflow.
tion. During 2007–08, ISMP partnered with several community Then, control systems were identified and added to the map.
pharmacy organizations, from which a purposive sample of 22 Active control systems are deliberate steps in the process that
pharmacies from three regions was selected to ensure diversi- specifically help manage the risk of errors, such as data entry
ty in setting, prescription volume, staffing, hours of operation, verification of prescriptions entered into the computer. Pas-
and population served. sive controls are features inherent in the system that might
help control risks but are not specifically set up for that pur-
Model-building sample pose, such as differences in tablet appearance that may alert a
The modeling team consisted of two trained ST-PRA facilitators pharmacist to an incorrect medication.28
from Outcome Engenuity, LLC, two clinical research staff from Identify failure modes. An abbreviated FMEA process
ISMP, and six pharmacists and three pharmacy technicians was used as a hazard identification technique to describe pos-
from nine of the sample pharmacies in the same central south- sible failure points (e.g., errors, at-risk behaviors, equipment
west region of the United States. The participating pharmacies failures) during the dispensing process and for each targeted
served urban, suburban, and small community areas and were high-alert medication. Online Appendix 3 shows small cross
diverse regarding prescription volumes, hours of operation, sections of the FMEAs related to warfarin and fentanyl trans-
and access to drive-through services. Pharmacy staffing pat- dermal systems. The FMEAs were used to determine PADEs to
terns ranged from a single pharmacist on duty to multiple phar- be modeled for the targeted drugs. Six PADEs for warfarin and
macists and technicians on duty. The participants had diverse one PADE each for fentanyl systems, methotrexate, and insulin
ethnic backgrounds, 5 to 18 years of experience (median 10), analogs were selected (Table 1).
and included both genders. Build the risk models. During February to April 2007,
the modeling team met six times and created 10 event trees
Model validation sample for the PADEs. An event tree is a graphical quantitative risk
Pharmacists who worked in 11 community pharmacies in the model that represents the complex relationships among pro-
New England and mid-Atlantic regions participated in struc- cess steps, organizational culture, human errors, equipment
tured interviews to validate the risk models. The pharmacies failure, behavioral norms, and undesirable outcomes.28,30,36,37
and participants were diverse in regards to experience, prac- The event trees decompose the dispensing system as a whole
tice settings, daily prescription volume, and gender/ethnic into subsystems and components. The process and control map
backgrounds. Observations were also conducted at two phar- was used to guide this step. Each individual event tree defined
macies selected from a convenience sample. the event sequences that could lead to the specific PADE of in-
terest, based on what was currently known about the dispens-
Identifying high-alert medications ing process and the behavior of systems and pharmacy staff
A list of high-alert medications dispensed from community under given conditions.
pharmacies was compiled using qualitative methods, including The risk model building process starts with an initiating er-
analysis of data about PADEs from the following sources: ISMP ror that could lead to a PADE. Each initiating error then was
National Medication Errors Reporting Program,45 the Pennsyl- followed through the dispensing process steps, which were
vania Patient Safety Reporting System,46 the Food and Drug called “basic events” in the event trees. The basic events repre-
Administration MedWatch database,47 databases from partici- sent (1) exposure rates, or how often certain activities occur;
pating pharmacies, community pharmacy survey data,48 public (2) fundamental failures, such as human error, at-risk behav-
litigation data,49 and literature review.7,9–18,49,50 ior,1 or equipment failure rates; or (3) capture opportunities
when errors can be detected and corrected (online Appendix
4). These basic events flowed through the branches of the event
tree, linking them together (Figure 1)
586 • JAPhA • 5 2 : 5 • S e p / O c t 2012 www.j aph a. or g Journal of the American Pharmacists AssociationTable 1. Selected PADEs for warfarin, methotrexate, fentanyl systems, and insulin analogs
High-alert medication Selected PADE Initiating error(s) Rationale for selection
Warfarin Wrong drug dis- Dispensing errors: (1) Wrong drug selected when Drug: Warfarin is a commonly prescribed oral medication (consistently
pensed manually filling a warfarin prescription. (2) Wrong among the top 200 drugs dispensed each year)72,73 that exposes pa-
drug selected when filling an automated dispensing tients to bleeding or thrombosis (subtherapeutic doses) if used in error.
cabinet with warfarin. Initiating errors: Selected to represent a variety of prescribing and
dispensing errors associated with wrong patient, wrong drug, wrong
dose, and wrong directions; three causes of wrong dose errors select-
ed because dosing errors represent the greatest risk to patients.19–21
Wrong dose/strength Prescribing error: Wrong dose/strength tablets
of warfarin dispensed prescribed.
Wrong dose/strength Dispensing errors: (1) Wrong warfarin dose/
of warfarin dispensed strength selected when manually filling a warfarin
prescription. (2) Wrong warfarin dose/strength
selected when filling an automated dispensing
Journal of the American Pharmacists Association
cabinet with warfarin.
Wrong dose/strength Dispensing error: Wrong dose/strength selected or
of warfarin dispensed entered during data entry of a warfarin prescription.
Warfarin dispensed Prescribing error: Warfarin prescription included
with wrong directions directions to take the drug more often than daily.
for use
Warfarin dispensed Dispensing error: Warfarin prescription entered
to the wrong patient into the wrong patient’s drug profile.
Warfarin dispensed Dispensing errors: (1) Warfarin vial placed in a bag
to the wrong patient containing another patient’s medications. (2) Wrong
www. japh a. or g
patient’s medication(s) selected from the will-call
area at the point of sale.
Methotrexate Methotrexate dis- Prescribing error: Oral methotrexate for nononco- Drug: Methotrexate is an oral antineoplastic agent also commonly
pensed with direc- logic use prescribed with directions to take the drug used in less frequent dose intervals to treat other immune-modulated
tions to take daily daily. diseases (e.g., rheumatoid arthritis, psoriasis). Initiating error: Select-
ed because daily doses that exceeded 5 days have been fatal.63,64
Fentanyl patches Incorrect or inappro- Prescribing error: Incorrect dose or inappropriate Drug: Fentanyl transdermal system of delivering opioid pain medica-
priate dose of fentan- dose prescribed for a patient based on opioid toler- tion exposes patients to over sedation, respiratory depression and
yl patches dispensed ance and type/duration of pain. arrest. Initiating error: Selected because fatalities have happened
to a patient repeatedly after prescribing doses too high for opioid-naive patients or
when using the drug to treat acute, not chronic, pain.80,81
Insulin analogs Wrong insulin analog Dispensing error: Wrong insulin analog selected Drug: Insulin is a commonly prescribed injectable drug used to treat
dispensed to a patient from the screen during data entry of an insulin pre- type 1 diabetes, a prevalent chronic illness that affects 700,000 Ameri-
scription. cans.82 It is one of the most common chronic diseases in children and
S e p /O c t 2012 • 52:5 •
adolescents.83 Initiating error: Selected due to frequency of reported
mixups between insulin products with look-alike names and the seri-
ous adverse effects of those mixups.84,85
risk models in community pharmacies Research
Abbreviation used: PADE, preventable adverse drug event.
JAPhA • 587Research risk models in community pharmacies
Event trees are particularly well suited for displaying the wrong product when filling prescription) and subsystem A has
order of events and the dependencies between events, such as succeeded (e.g., pharmacist checked final prescription), sub-
when the failure of subsystem B may depend on the status of system B has failed (e.g., pharmacist did not capture error dur-
subsystem A.51 To cite a simplified example, subsystem F fails ing product verification), subsystem C has succeeded (e.g., pa-
(e.g., patient receives wrong medication) given that the initi- tient was counseled when picking up prescription), subsystem
ating event has happened (e.g., pharmacy technician selected D has failed (e.g., prescription vial not opened to view tablets
Medication dispensed to wrong
customer at the point of sale
Top level event Gate 1
Q: 0.00138 And gate
Medication given to wrong Wrong customer not detected
customer at the point of sale
Gate 2 Gate 3
Q: 0.0034 Or gate And gate Q: 0.405
Wrong customer’s medications selected by pharmacy at Medication was placed in Pharmacy staff do not detect Customer does not catch
the point of sale when dispensing medication wrong customer’s bag identification error at point of sale identification error at point of sale
Event 1 Event 2 Gate 6 Event 3
Q: 0.003
Initiating errors Q: 0.0004 Q: 0.45
Or gate Q: 0.9
Basic event
Identification error not caught when Identification error not caught when customer
following customer identification process identification process not followed
Gate 4 Gate 5
And gate And gate
Q: 0.0005 Q: 0.45
Exposure rate for following Pharmacy staff fail to detect the error when Exposure rate for not following Pharmacy staff fail to detect the error when
customer identification process following customer identifcation process customer identification process customer identifcation process does not occur
Event 4 Event 5 Event 6 Event 7
Q: 0.5 Q: 0.001 Q: 0.5 Q: 0.9
Exposure rate Basic event Exposure rate Basic event
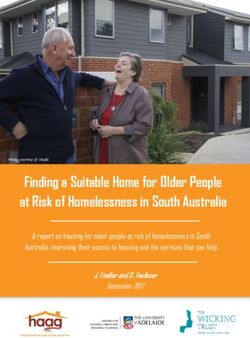
Figure 1. Illustration of fault tree for dispensing medication to wrong customer
Abbreviations used: PADE, preventable adverse drug event.
Example of a small section of a fault tree associated with dispensing a prescription to wrong customer (e.g., patient, family member, friend, caregiver). Events 1 and 2 represent the
initiating errors for one pathway leading to the PADE (top-level event in gate 1) of dispensing a medication to the wrong customer. The probability of selecting the wrong customer’s
medications (event 1) was estimated to occur with 3 of 1,000 (0.003) prescriptions. The probability of placing the medication in the wrong patient’s bag (event 2) was estimated to oc-
cur with 4 of 10,000 (0.0004) prescriptions. These initiating errors were combined with an “or” gate (gate 2), meaning that one or the other must happen for the medication to be given
to the wrong customer.
Reading from the bottom of the tree, from left to right, events 4 and 6 represent exposure rates for adherence to the patient identification process. In the example, the probabilities
were set at 0.5 for each, meaning that 50% of the time, the patient identification process is followed and 50% of the time it is not followed. Events 5 and 7 describe how often pharmacy
staff fail to notice that the wrong patient’s medications are in the bag. When following the identification process (event 5), the probability of failing to notice the error was estimated to
occur in 1 of 1,000 (0.001) prescriptions. But when the patient identification process is not followed (event 7), the probability of failing to notice the error was estimated to occur in 9 of
10 (0.9) prescriptions.
Events 4 and 5 and events 6 and 7 are connected with “and” gates (gates 4 and 5) because both of the basic events below them must occur for the gates to be true. The fault tree
software calculated the combined effects of how often the identification process is followed (events 4 and 6) and the estimated rate of failing to detect the error (events 5 and 7).
Gates 4 and 5 are connected with an “or” gate (gate 6) because the error was not detected either when following the patient identification process or not following the identification
process. Again, the fault tree calculated the combined effects of gates 4 and 5 to arrive at the probability expressed in gate 6. Event 3 to the right of gate 6 shows the probability that
the customer will fail to catch the error at the point of sale: 9 of 10 (0.9) opportunities. Pharmacy staff inability to capture the error (gate 6) was then combined with the customer’s
inability to capture the error (event 3) through an “and” gate (gate 3) because both failures need to happen for the error to continue through the dispensing process and reach the
patient. Gate 3, which expresses the combined effects of the two initiating errors, and gate 4, which expresses the combined effects of inability by pharmacy staff and customers to
capture the error, are then combined with an “and” gate to reach the top level event (gate 1). In this example, for illustrative purposes only, the medication dispensed for the wrong
patient at the point of sale is estimated to occur in 1.4 of 1,000 (0.00138) prescriptions.
588 • JAPhA • 5 2 : 5 • S e p / O c t 2012 www.j aph a. or g Journal of the American Pharmacists Associationrisk models in community pharmacies Research
to aid in error detection), and subsystem E has failed (e.g., pa- Quantify event rates. The modeling team quantified the
tient does not detect error at point of sale). probability of failure or frequency of occurrence for each basic
The event trees went through multiple iterations until the event in the event trees. The data used to support the quantifi-
modeling team was satisfied that they accurately captured cation process came from documented component-specific in-
the components of the dispensing process and dependencies formation (e.g., rates of barcode scanning overrides for a par-
among the different tasks. ticular drug), generic reference points (e.g., well-established
Table 2. Human error probabilities
Description of error probabilities Error probability
High probability of error
Unfamiliar task performed at speed with no idea of likely consequences86 0.5
Failed task involving high stress levels54 0.3
Inspection/verification of tasks with moderate stress87,86 0.2
Failed complex task requiring high level of comprehension and skill86 0.15
Failed task involving complex math computation88 0.15
Failed task conducted in the first 30 minutes of an emergency54 0.1
Failure to detect an error after it has happened89 0.1
Fairly simple task performed rapidly or given scant attention86 0.1
Moderate probability of error
Misidentify/misdiagnose given like symptoms/appearance86 0.05
Failure to select ambiguously labeled control/package89 0.05
Failure to perform a check correctly90 0.05
Wrong conclusion drawn with competing/unclear information86 0.05
Failed execution of maintenance/repair86 0.04
Failed task with cognitive or task complexity86 0.03
Failure to act correctly after the first few hours in a high-stress situation54 0.03
Symptoms noticed, but wrong interpretation86 0.03
Failed task related to values/units/scales/indicators86 0.02
Failed task related to selection of items from among groups of items88 0.02
Failed routine, highly practiced, rapid task, involving a relatively low level of skill86 0.02
General mental slip without knowledge deficit91 0.02
Failed task related to known hazards/damage86 0.02
Failed communication among workers91 0.02
Failed task involving both diagnosis and action86 0.01
Failed diagnosis task86 0.01
Error in a routine operation where care is required54 0.01
Set a switch in wrong position89 0.01
Low probability of error
Procedural omission86 0.006
Errors during read-back91 0.005
Counting/volume errors88 0.004
Selection of the wrong control/package (well labeled)89 0.003
Operate spring-loaded switch until proper position reached89 0.003
Selection of the wrong switch/package (dissimilar in shape/appearance)54 0.001
Lowest limits of human error
Completely familiar, well-designed, highly practiced, routine task occurring several times per hour, performed to high-
est possible standards by a highly motivated, highly trained, and experienced person, totally aware of implications of
failure, with time to correct potential error but without the benefit of important job aids86 0.0004
Human-performance limit: single person working alone54 0.0001
Responds correctly to system command when there is an augmented or automated supervisory system providing ac-
curate interpretation of system state86 0.00002
Human performance limit: team of people performing a well-designed task54 0.00001
Journal of the American Pharmacists Association www. japh a. or g S e p /O c t 2012 • 52:5 • JAPhA • 589Research risk models in community pharmacies
equipment failure rates that could be reasonably assumed for In very general terms, given a human performance limit
pharmacy dispensing equipment), and expert opinion. of 0.0001 (10−4 or 1/10,000) for a single worker operating in
The failure rate estimates needed as inputs in the event absolutely ideal conditions,54 the modeling team often started
trees were obtained using Bayesian statistical methods, which with an error rate of 0.001 (10−3 or 1/1,000) to account for the
work directly with estimated probabilities, rather than classi- negative influence of a single PSF such as time constraints.
cal statistical methods, which work primarily with counts of Identification of additional PSFs (e.g., illegible prescriptions,
data. Judgment and expert opinions are required with all PRAs look-alike product names, complex tasks, minimal worker
and ST-PRAs because the available data about components of training) was part of the group process. The number of PSFs
the systems are not of the precise form required for use of clas- and their degree of influence helped the team adjust its esti-
sical statistical methods.52 mates upward or downward through an iterative process be-
Most health care practitioners do not have actual rate data fore deciding on a final probability. The team quickly gained
for the underlying basic events.2 At best, data collection sys- comfort in the task of estimating error and at-risk behavior
tems only capture the end result, with the rate of intermedi- probabilities, which is typical of ST-PRA modeling teams.30,36,37
ate failures relatively unknown.31 Failures, at-risk behaviors, Experience indicates that these team estimates are more ac-
and adverse events are so underreported in health care that cepted than rates derived from event data and are often more
using any data sources relying on reporting systems is sus- accurate than rates predicted by senior management.36 More
pect. In addition, PADEs can be masked by the patient's illness information on ST-PRA and the risk modeling process are
and thereby underestimated in occurrence data.2 Thus, some available in Marx and Slonim36 and Comden et al.30
components of the event trees were developed purely through
Bayesian methods, which provided a formal and rigorous way Model validation process
of combining expert judgments with observed data to obtain Observations were conducted at two pharmacies to validate
a probability. These probabilities then were propagated in the the event trees’ representation of the dispensing process and
ST-PRA models to express the likelihood that a particular event confirm the presence or absence of visible process risks (e.g.,
would happen and the conditional uncertainty associated with infrequent patient counseling) and PSFs (e.g., look-alike prod-
that event.28,31,51,53 ucts next to each other). The observations also served to un-
The substantive accuracy of the ST-PRA depends on how derstand the relationship and dependencies among the various
well the assessors know the problem under consideration. components of the dispensing systems and to validate that the
Thus, the modeling team was led by experts in human fac- structure of the event trees accurately represented the “as is”
tors, probability theory, ST-PRA modeling, and medication dispensing process at the participating pharmacies.
safety. The pharmacists and technicians possessed deep do- A survey instrument about exposure rates, capture oppor-
main knowledge of the processes under assessment. Internal tunities, at-risk behaviors, and failures most predictive of the
pharmacy operational data verified the team's estimates of ex- PADEs was constructed and tested for interviewing pharma-
posure rates (e.g., how often technicians enter prescriptions cists who did not participate in the modeling sessions. Prob-
into the computer, how often prescriptions are received via fax, abilities estimated by the modeling group were not shared
percent of a specific drug filled via automation). Pharmacists with the validation group. Well-constructed published studies
and technicians relied on their work experiences regarding of drug mishaps were examined to provide, where possible,
frequencies of at-risk behaviors. Evidence shows that expert evidence to support the probability estimates derived for the
opinion–based probabilities are biased toward the low values PADEs and initiating errors in the event trees.
of failure rates.52 Therefore, team facilitators anchored the
group estimates of human error rates on data reported in the Quantifying the impact of risk-reduction
literature, setting lower- and upper-bound human error prob- interventions (sensitivity analysis)
ability limits as reference points for specific conditions. Table 2 Event tree software55 calculated combinations of failures and
summarizes the human error probabilities that helped inform the total combined probability of occurrence of each PADE. All
and verify team estimates. unique combinations that could lead to PADEs were identified
Numerous sophisticated techniques have been used since and ranked, producing cut sets or a “risk portfolio” for each
the early 1980s to estimate probabilities of human error.54 event tree.30 The portfolios defined which components of the
Although the formulas and tables for estimating human error dispensing system were truly important to risk in that they con-
probabilities vary from technique to technique, each factors in tributed most frequently among all of the different sequences of
error type and performance-shaping factors (PSFs) to make events that could lead to PADEs. The portfolios then were used
judgments about error rates. Examples of common PSFs can to identify the best interventions to reduce the probability of
be found in online Appendix 5. PSFs have a positive or nega- errors and at-risk behaviors or to change the tree's structure
tive effect on performance. For example, staff training can by building into the process new opportunities for capturing
influence performance either positively (e.g., when training errors. After the interventions were identified, the event trees
emphasizes the appropriate learned responses) or negatively were updated to test and quantify the impact of each strategy.
(e.g., when training is absent). The modeling team referenced
the FMEAs to uncover the most relevant PSFs before making
estimates.
590 • JAPhA • 5 2 : 5 • S e p / O c t 2012 www.j aph a. or g Journal of the American Pharmacists Associationrisk models in community pharmacies Research
Results warfarin to the wrong patient (1.22/1,000 prescriptions), and
Community pharmacy high-alert medications dispensing an inappropriate fentanyl system dose because of
Table 3 lists the drugs that were identified as high-alert medi- a prescribing error (7.30/10,000 prescriptions). PADEs with
cations dispensed from community pharmacies. Warfarin, the highest incidence were associated with single-pathway
fentanyl systems, oral methotrexate, and insulin analogs were failures, meaning that no key opportunities were available to
selected for ST-PRA modeling. Examples of risk factors with capture the error from the time it was made until it reached the
these targeted drugs can be found in online Appendix 6. patient. PADEs with the lowest incidence included dispensing
the wrong drug when filling a warfarin prescription (9.43/1 bil-
Validation of event trees lion prescriptions) and dispensing the wrong dose when filling
Based on observations and survey findings, 2 of 52 probability a warfarin prescription (9.25/10 million prescriptions). PADEs
estimates associated with at-risk behaviors were adjusted be- with the lowest incidence were associated with consistent use
cause of minor differences between modeling team and valida- of barcode scanning technology.
tion group estimates. No changes were made to 306 exposure A sensitivity analysis conducted to evaluate the impact of
rates or 211 failure rates, as modeling team and validation selected interventions (Table 5) showed that the largest quan-
group estimates were very similar. No changes occurred as a tifiable reductions in risk were provided by (1) consistently
result of comparison with error rates in published studies. No using barcoding technology (up to 100% reduction), (2) build-
changes were made to the structure of the event trees, which ing computer alerts that can't be bypassed easily (up to 100%
were determined to be accurate. reduction), (3) conducting a second data entry verification
process during product verification (50–87% reduction), (4)
Risk of PADEs reaching patients increasing patient counseling (27–68% reduction), (5) open-
This study produced 10 event trees for PADEs associated with ing the bag at the point of sale (56% reduction), and using tall
warfarin, fentanyl systems, oral methotrexate, and insulin man letters to distinguish insulin products with similar names
analogs. These 10 event trees produced more than 200,000 (50% reduction). Combining two or more interventions result-
failure pathways that could lead to PADEs. Table 4 shows the ed in further overall reduction in risk. Further description of
estimated rate of PADEs reaching patients for each event tree. the analyses of several PADEs follows.
These rates include all errors that reach patients after they
leave the pharmacy counter, even if patients discover the error Wrong warfarin dose/strength dispensed because
after leaving the pharmacy and do not take or use any of the of data entry error
erroneous medications. PADEs with the highest incidence in- Event tree analysis: High vulnerability of data entry er-
cluded dispensing the wrong dose/strength of warfarin because rors. Initially entering a wrong dose or strength of warfarin in-
of a data entry error (1.83/1,000 prescriptions), dispensing to the patient's profile during data entry was estimated to occur
Table 3. High-alert medications in community pharmacy
Drug class/category Examples
Antiretroviral agents Abacavir, atazanavir, diaveridine, lamivudine, ritonavir, zidovudine. Combination
products such as Combivir, Atripla, Epzicom, Kaletra
Chemotherapy, oral (exclusion: hormonal agents) Busulfan, chlorambucil, cyclophosphamide, lomustine, melphalan, mercaptopu-
rine methotrexate, procarbazine, temozolomide
Hypoglycemic agents, oral Chlorpropamide, glipizide, glyburide, repaglinide
Immunosuppressant agents Azathioprine, cyclosporine, daclizumab, mycophenolate, sirolimus, tacrolimus
Insulin NPH/regular, aspart, detemir, glargine, glulisine, lispro
Opioids, all formulations Butorphanol, fentanyl, hydromorphone, meperidine, methadone, morphine,
opium tincture, oxycodone
Pregnancy Category X drugs Atorvastatin, bosentan, estazolam, isotretinoin, simvastatin, temazepam
Pediatric liquid medications that require measurement
Individual drugs
Carbamazepine
Chloral hydrate liquid (for sedation of children)
Heparin (unfractionated and low molecular weight)
Metformin
Methotrexate (nononcologic use)
Midazolam liquid (for sedation of children)
Propylthiouracil
Warfarin
Journal of the American Pharmacists Association www. japh a. or g S e p /O c t 2012 • 52:5 • JAPhA • 591Research risk models in community pharmacies
Table 4. Probabilities of PADEs for warfarin, fentanyl systems, methotrexate, and insulin analogs
Capture before Rate of PADEs reach- No. PADEs reaching patients
Initiating error rate per reaching patients ing patients per 1,000 annually among all U.S. com-
Medication, PADE 1,000 prescriptions % prescriptions munity pharmacies (n = 56,000)
Warfarina
Prescribing error: wrong dose 10 94.3 0.569 (5.69/10,000) 15,022
Prescribing error: wrong direc- 2 99.9 0.0001 (1.34/10 million) 4
tions
Data entry error: wrong dose 100 98.2 1.83 (1.83/1,000) 48,312
Filling error: wrong drug Automated dispensing, 99.9 0.000009 (9.43/1 billion) 0.25 (once every 4 years)
0.1; manual dispensing,
1; combined rate, 1
Filling error: wrong dose Automated dispensing, 99.9 0.0009 (9.25/10 million) 24
0.1; manual dispensing,
100; combined rate, 100
Fentanyl transdermal patchesb
Prescribing error: wrong dose 1 27.0 0.730 (7.30/10,000) 3,431
Methotrexatec
Prescribing error: wrong direc- 1 99.9 0.0009 (9.64/10 million) 4
tions
Insulin analogsd
Data entry error: wrong drug 10 96.9 0.306 (3.06/10,000) 6,426
All prescription medicationse
Data entry error: wrong patient 5 99.0 0.052 (5.15/100,000) 197,849
Point-of-sale error: wrong Select wrong patient’s 64 1.22 (1.22/1,000) 4,641,856
patient bag, 3; place in wrong
patient’s bag, 0.4; com-
bined rate, 3.4
Abbreviation used: PADE, preventable adverse drug event.
a
Annual prescription volume for all U.S. community pharmacies: 26,400,000 (2007).72–74
b
Annual prescription volume for all U.S. community pharmacies: 4,700,000 (2007).72–74
c
Annual prescription volume for all U.S. community pharmacies: 4,400,000 (2007).72–74
d
Annual prescription volume for all U.S. community pharmacies: 21,000,000 (2007).72–74
e
Annual prescription volume for all U.S. community pharmacies: 3,804,800,000 (2007).72–74
with 1 in 10 warfarin prescriptions. Of these, 1.83 data entry prescriptions. If the prescription bottle is opened during coun-
errors per 1,000 prescriptions reached patients. The dispens- seling, a patient who knows what color tablets to expect has a
ing system is vulnerable to this type of data entry error because 99% chance of capturing the data entry error. However, the
nine different strengths of warfarin tablets exist from which to bottle is only opened about 30% of the time.
choose. These errors are rarely corrected if data entry verifica- Sensitivity analysis: Impact of data entry verification
tion and patient counseling do not occur. and patient counseling. We determined the impact of four in-
During data entry, pharmacy staff have a greater chance terventions on the incidence of dispensing the wrong warfarin
of detecting the error if the patient had previous warfarin pre- dose because of a data entry error: (1) reducing the incidence
scriptions filled at that pharmacy. But failure to detect the er- of a skipped, rushed, or inattentive data entry verification pro-
ror is high (75%) given a 90% probability that these patients cess by 50%, (2) increasing patient counseling from 30% to
will have multiple strengths of warfarin in their drug profile 80%, (3) more frequent (90%) independent verification by an-
history. other pharmacist of prescriptions entered by pharmacists, and
An independent data entry verification process by a phar- (4) the addition of a second data entry verification process dur-
macist who has not entered the prescription was estimated to ing the product verification step. The most effective interven-
capture up to 99% of errors if an out-of-range dose alert oc- tions involved the second data entry verification process and
curs and is not bypassed. However, dose alerts are not likely patient counseling.
to occur if the wrong strength tablets are selected during data Increasing patient counseling to 80% resulted in a 67% re-
entry. Duplicate therapy alerts occur during data entry with duction in dispensing the wrong warfarin dose because of data
about 80% of warfarin prescriptions but are not reliable as a entry error; errors that reached patients decreased from 1.83
means of detecting a data entry error. Patient counseling was to 0.6 per 1,000 prescriptions. Conducting a second data entry
estimated to occur with 30% of patients picking up warfarin verification process during product verification by comparing
592 • JAPhA • 5 2 : 5 • S e p / O c t 2012 www.j aph a. or g Journal of the American Pharmacists Associationrisk models in community pharmacies Research
Table 5. Sensitivity analysis of selected interventions to reduce PADEs
Errors before Decrease in risk
action, per 1,000 Errors after action, per (increase in risk)
Evaluated interventionsa prescriptions 1,000 prescriptions %
PADE: Medication dispensed to the wrong patient due to a bagging er-
ror or bag selection error at the point of sale 1.22 (1.22/1,000)
A: Open the bag at the point-of-sale to view all filled prescriptions 0.534 56
B: Increase adherence with following a patient identification process
from 50% to 80% 0.804 34
C: Increase patient counseling from 30% to 50% 0.889 27
D: Reduce at-risk behavior of working on more than one patient’s medi-
cations during product verification and bagging (which lowers the bag-
ging error rate from 0.4 to 0.1 per 1,000 prescriptions) 1.11 9
Action A and action B 0.233 81
Action A and action B and action C 0.169 86
Action A and action B and action C and action D 0.154 87
PADE: Medication dispensed to the wrong patient caused by entering 0.052
the prescription into the wrong profile (5.15/100,000)
A: Reduce at-risk behavior of conducting inattentive data entry verifica-
tion from 1 in 10 to 5 in 100 prescriptions (requires changes in the system/
environment to support a consistent, cognitive checking process) 0.034 35
B: Increase patient counseling from 30% to 50% 0.037 29
C: Increase the frequency of an independent double-check for data entry
verification when a pharmacist enters prescriptions from 50% to 90% 0.024 17
D: Conduct a second redundant data entry verification during the final
product verification step 0.007 87
E: Reduce the incidence of entering prescriptions into the wrong patient
profile from 5 to 1 per 1,000 prescriptions by requiring entry of two unique
patient identifiers (name, birth date) in the patient profile 0.010 81
Action A and action B 0.024 54
Action A and action B and action C 0.020 62
Action A and action B and action C and action D 0.002 96
Action A and action B and action C and action E 0.004 92
Action A and action B and action C and action D and action E 0.0004 99
PADE: Wrong or inappropriate dose of fentanyl patches dispensed due 0.730
to a prescribing error (7.30/10,000)
A: Conduct an intake history of opioids when receiving a prescription for
fentanyl patches; pharmacist review history before data entry (which
results in capture of 40% of prescribing errors) 0.439 40
B: Increase patient counseling from 10% to 80%, and increase the ability
to recognize inappropriate doses from 10% to 80% by reviewing the pa-
tient’s opioid history during counseling session 0.263 64
Action A and action B 0.159 78
PADE: Methotrexate dispensed with directions to take daily instead of 0.0009 (9.64/10
weekly due to a prescribing error million)
A: Include a diagnosis or indication for use on the prescription 0.0007 22
B: Set dose alert as a hard stop that does not allow the entry of metho-
trexate prescriptions with daily dosing for more than 1 consecutive week 0.00000001 (1/100 billion) 100
C: Eliminate computer warning about daily dosing of methotrexate 0.006 (522)
Action A and action B 0.00000001 (1/100 billion) 100
PADE: Wrong insulin analog dispensed due to selecting the wrong drug 0.306
during data entry (3.06/10,000)
Journal of the American Pharmacists Association www. japh a. or g S e p /O c t 2012 • 52:5 • JAPhA • 593Research risk models in community pharmacies
Table 5. Sensitivity analysis of selected interventions to reduce PADEs
Table 5 continued
A: Reduce the frequency of misreading prescriptions for insulin products
with similar names by increasing electronic prescriptions by 20% (lowers
initiating error rate from 10 to 8 per 1,000 prescriptions) 0.245 20
B: Reduce the rate of selecting the wrong insulin product during order
entry by using tall man letters to distinguish products with similar names
(lowers initiating error rate from 10 to 5 per 1,000 errors) 0.153 50
C: Increase frequency of patient counseling from 30% to 80% 0.100 67
D: Conduct a second redundant data entry verification during the final
product verification step 0.153 50
Action A and action B and action C 0.028 91
Action A and action B and action C and action D 0.014 95
PADE: Wrong drug or dose dispensed due to a selection error while (1) Wrong drug,
filling a prescription for warfarin 0.000009 (9.43/1
billion); (2) wrong
dose, 0.0009
(9.25/10 million)
A: Eliminate barcoding technology during the dispensing process (1) 0.009 (9/1 million), (2) (1) (95,340), (2)
0.900 (9/ 10,000) (97,197)
B: Use a cheat sheet to scan a barcode for warfarin 30% of time rather (1) 0.025 (2.5/100,000, (2) (1) (265,011), (2)
than scanning the bar code on the stock bottle/carton 0.200 (2/10,000) (21,521)
C: No pill image on the product verification screen (and label) (1) 0.00004 (4 /100 million),
(2) 0.004 (4/1 million) (1) (324), (2) (332)
D: Increase the automated filling of warfarin prescriptions from 20% to (1) 0.000007 (7/1 billion),
50% (2) 0.0006 (6/10 million) (1) 25, (2) 35
E: Increase the frequency of patient counseling from 30% to 80% (1) 0.000003 (3/1 billion,
(2) 0.0003 (3/10 million) (1) 68, (2) 67
Action A and action C (1) 0.042 (4.2/100 thou- (1) (445,287), (2)
sand), (2) 4.20 (4.2/1,000) (453,954)
Action D and action E (1) 0.000002 (2/1 billion)
(2) 0.0002 (2/10 million) (1) 78, (2) 78
PADE: Wrong dose/strength of warfarin tablets dispensed due to a pre- 0.569
scribing error (5.69/10,000)
Increase patient counseling from 30% to 80% 0.274 52
PADE: Wrong warfarin dose dispensed due to a data entry error 1.83 (1.83/1,000)
A: Reduce at-risk behavior of conducting inattentive data entry verifica-
tion from 1 in 10 to 5 in 100 prescriptions (requires changes in the system/
environment to support a consistent, cognitive checking process) 1.19 35
B: Increase patient counseling from 30% to 80% 0.600 67
C: Increase the frequency of an independent double-check for data entry
verification when a pharmacist enters prescriptions from 50% to 90% 0.865 53
D: Conduct a second redundant data entry verification during the final
product verification step 0.366 80
Action A and action B 0.393 79
Action A and action B and action C 0.283 85
Action A and action B and action C and action D 0.174 91
PADE: Warfarin prescription dispensed with the wrong directions due 0.0001 (1.34/10
to a prescribing error million)
Make data entry for more frequent than daily dosing of warfarin result in
an alert with a hard stop 0.000000001 (1/1 trillion) 100
Increase patient counseling when picking up prescriptions from 30% to
80% 0.00005 (5/100 million) 50
Abbreviation used: PADE, preventable adverse drug event.
a
Most evaluations measure the positive impact of increasing an existing risk-reduction strategy or implementing a new risk-reduction strategy. A few of the evaluations measure
the negative impact of reducing or eliminating an existing risk-reduction strategy.
594 • JAPhA • 5 2 : 5 • S e p / O c t 2012 www.j aph a. or g Journal of the American Pharmacists Associationrisk models in community pharmacies Research
the scanned prescription in the computer with the prescription effectiveness of using barcoding technology during dispens-
label reduced the risk of this error reaching patients by 80%. ing.16,17,59–61 With the technology, 99.9% of selection errors
More frequent independent checks and less skipped, rushed, were detected and corrected. However, without it, the prob-
or inattentive checks during data entry verification reduced the ability of dispensing the wrong drug increased from 9.43 per 1
risk of PADEs by 53% and 35%, respectively. All four interven- billion to 9 per 1 million, and the probability of dispensing the
tions together lowered the risk of dispensing the wrong warfa- wrong dose increased from 9.25 per 10 million to 9 per 10,000.
rin dose from 1.83 to 0.174 per 1,000 prescriptions. Similar increases were seen if an image of the correct tablet
was not available during product validation. When barcoding
Wrong drug or dose dispensed because of and tablet imaging are absent, the probability of dispensing the
selection error while filling prescription for wrong drug increased from 9.43 per 1 billion prescriptions to
warfarin 4.2 per 100,000 prescriptions and the probability of dispens-
Event tree analysis: Vulnerability of selecting wrong dose ing the wrong dose increased from 9.25 per 10,000,000 pre-
higher than wrong drug. Initially selecting the wrong drug scriptions to 24.2 per 1,000 prescriptions. We also evaluated
while manually filling a warfarin prescription was estimated the impact of increasing automated dispensing of warfarin
to occur in 1 of 1,000 prescriptions. Mixups between warfarin from 20% to 50% and increasing patient counseling from 30 to
and another medication have been reported rarely, although a 80%, which reduced the risk of allowing either a wrong drug or
risk exists with the branded warfarin product Jantoven (Upsh- wrong dose dispensing error to reach the patient by 78%.
er-Smith), which could be confused with Januvia or Janumet.56
However, pharmacies often stock warfarin on shelves accord- Incorrect or inappropriate dose of fentanyl
ing to generic names, thereby lessening the risk of such an er- systems dispensed because of prescribing error
ror. Event tree analysis: Dispensing system unreliable in de-
Initially selecting the wrong dose while manually filling tecting prescribing errors. Prescribing an incorrect or inap-
a prescription for warfarin was estimated to occur more fre- propriate dose of fentanyl systems was estimated to occur in 1
quently (1 of 10 prescriptions). This estimate is in line with of 1,000 prescriptions. Fentanyl systems that are prescribed to
a study that found that more than 5% of medications first se- treat acute pain (not an approved indication) and/or prescribed
lected to fill a prescription were wrong,57 as more errors are to opioid-naive patients were classified as an incorrect or inap-
expected with warfarin doses because of nine different tablet propriate dose, as were doses that exceeded safe limits based
strengths. The 1-mg and 10-mg strengths also are prone to on the patient's previous opioid use, age, general medical con-
mixups, particularly if a trailing zero is used to express the dition, conditions associated with hypoxia or hypercapnia, and/
1-mg dose (1.0 mg) on pharmacy or product labels.58 or concomitant analgesics. Including all of these wrong dose
The probability of an error reaching the patient is 9.43 per prescribing errors resulted in dispensing 0.73 wrong doses per
1 billion warfarin prescriptions for wrong drug errors and 9.25 1,000 prescriptions.
per 10 million prescriptions for wrong dose errors. These low The dispensing system in participating pharmacies was
estimates are primarily the result of using barcoding technol- largely unreliable in its ability to detect this prescribing er-
ogy while manually filling prescriptions and the availability ror; only 27% of the errors were estimated to be captured and
of a tablet image for product verification. We estimated that corrected. The low capture rate was primarily associated with
technology would fail to capture the error in 1 of 100,000 op- inadequate knowledge about the patient's prior opioid use, un-
portunities to account for an occasional problematic barcode derlying health conditions, and type of pain for which the fen-
or scanner malfunction. If the error is not picked up through tanyl system had been prescribed.
barcoding, an image of the correct drug and dose on the screen Drug use review and patient counseling are two steps dur-
during product verification facilitates capture of the error in 99 ing which fentanyl system prescribing errors can be captured,
of 100 occurrences. The final opportunity to capture these er- but with limited success. The acceptable dose range for fentan-
rors is during patient counseling, which was estimated to occur yl systems is wide, from 12.5 μg/hour to 100 μg/hour or more,
30% of the time, mostly for patients with a new prescription depending on the patient's opioid tolerance and pain level.
or dose change. If the bottle label is viewed and the bottle is Doses up to 300 μg/hour are recommended for patients with
opened during the counseling session, the chance of capturing a 24-hour intake history of oral morphine in doses from 1,035
the error during this process step was estimated to increase to 1,124 mg/day.62 An out-of-range dose alert would occur in
from 90% (bottle not opened) to 99% (bottle opened), as phar- just 1 of 100 prescriptions, as the computer cannot detect an
macists and patients often know what color tablet to expect inappropriate dose within such a wide acceptable therapeutic
for a given strength. The impact of this intervention is lessened range. If the computer issues an out-of-range dose alert, the
in the overall estimate of PADE occurrence because patient modeling team estimated that the error would be detected 98%
counseling does not always occur. of the time, but the low rate of dose alerts makes this an unreli-
Sensitivity analysis: Impact of barcode product veri- able capture opportunity.
fication, automated dispensing, tablet imaging, and pa- The frequency of patient counseling was estimated to be
tient counseling. Our event trees for warfarin drug and dose 10% because many patients on fentanyl systems do not pick
selection errors add evidence to existing knowledge about the up their prescriptions and counseling is often declined by the
Journal of the American Pharmacists Association www. japh a. or g S e p /O c t 2012 • 52:5 • JAPhA • 595You can also read