JDSM - American Academy of Dental Sleep ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
JDSM
REVIEW ARTICLE http://dx.doi.org/10.15331/jdsm.7072
Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine
Victor Lai1, Jayne C. Carberry, PhD1,2, and Danny J. Eckert, PhD1,2
1Neuroscience Research Australia (NeuRA) and the University of New South Wales, Sydney, NSW, Australia; 2Adelaide Institute for Sleep Health
(AISH), a Flinders University Centre of Research Excellence, Bedford Park, SA, Australia
New knowledge of obstructive sleep apnea (OSA) pathophysiology has highlighted the heterogeneity of this common chronic health
condition. Recent advances in OSA ‘phenotyping’ concepts have provided a novel framework in which to understand OSA
pathophysiology on an individual patient basis. This has also provided new potential precision medicine strategies to optimize efficacy
and success rates with current OSA treatments including mandibular advancement therapy.
This review summarizes how different ‘phenotypes’ contribute to OSA pathophysiology and highlights the potential mechanisms by
which mandibular advancement splints alter upper airway physiology according to an OSA phenotyping framework. In addition, it
explains how understanding these phenotypes can facilitate novel and improved approaches to therapy, with a focus on phenotyping to
improve mandibular advancement splint treatment prediction and efficacy. The potential to translate phenotyping concepts into the
clinical setting is also discussed.
Keywords: pathophysiology, precision medicine, sleep-disordered breathing, targeted therapy, upper airway
Citation: Lai V, Carberry JC, Eckert DJ. Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine. J Dent Sleep Med.
2019;6(2)
INTRODUCTION However, efficacy is more variable than with CPAP and
predicting which patients will respond to oral appliance
Obstructive sleep apnea (OSA) is a chronic and therapy remains a major clinical challenge for the field.19,20
prevalent sleep-related breathing disorder.1,2 It is Indeed, various sophisticated assessments of upper airway
characterized by recurrent, transient narrowing (hypopnea) anatomy during wakefulness and natural and drug-induced
and collapse (apnea) of the upper airway during sleep. sleep as well as clinical, demographic, anthropometric and
These breathing disturbances cause frequent oxygen polysomnographic parameters have failed to consistently
desaturations and sleep fragmentation. Up to 50% of men perform at satisfactory level to be incorporated clinically
and 23% of women aged 40 to 85 years have moderate to as prediction tools for MAS therapy outcome.19-23
severe OSA defined as 15 or more breathing disturbances Nonetheless, despite variable and unpredictable efficacy,
per hour of sleep.1 The estimated prevalence of OSA has oral appliance therapy can yield similar health benefits to
increased by 14% to 55% over the past two decades.2 Most CPAP.24 This is because lower efficacy compared to CPAP
individuals have OSA that is undiagnosed, untreated, or is typically counterbalanced by higher rates of adherence
undertreated.3 This is a major concern given the extensive to therapy.24 One barrier to improved treatment efficacy
range of symptoms and adverse health consequences with oral appliance therapy is that the precise mechanism
associated with untreated OSA. These include daytime or mechanisms of action are incompletely understood.19
sleepiness, decreased concentration, fatigue, irritability and This limits the ability to strategically alter oral appliance
memory loss,4 reduced quality of life,5 increased risk of therapy design for improved efficacy and to target patients
motor vehicle accidents,6 cardiovascular disease,7,8 with clinical and physiological characteristics who are
metabolic disorders,9 cognitive impairment,10 depression,11 most likely to respond favorably. Other interventions for
and cancer.12 Thus, there is a pressing need for effective OSA are either difficult to achieve (such as weight loss) or
treatment to reduce the significant health and safety burden also have variable efficacy (such as upper airway surgery
associated with untreated OSA. or position therapy). Existing management guidelines rely
However, there are major challenges associated with on an inefficient trial-and-error approach that often begins
the current management of OSA. Conventional therapies with CPAP as the one-size-fits-all therapy.4,25 The current
can be effective in reducing the severity and symptoms of treatment journey is often costly, time consuming, and
OSA.13-16 Yet, fewer than 50% of patients adequately imprecise (Figure 1). As a result, many patients are lost to
tolerate the first-line therapy, continuous positive airway follow-up and are left untreated or undertreated.25 Thus,
pressure (CPAP).17,18 Oral appliances such as mandibular new treatment strategies that can accurately predict and
advancement splints (MAS) are a common alternative. optimize treatment outcomes for people with OSA are
Journal of Dental Sleep Medicine Vol. 6, No.2 2019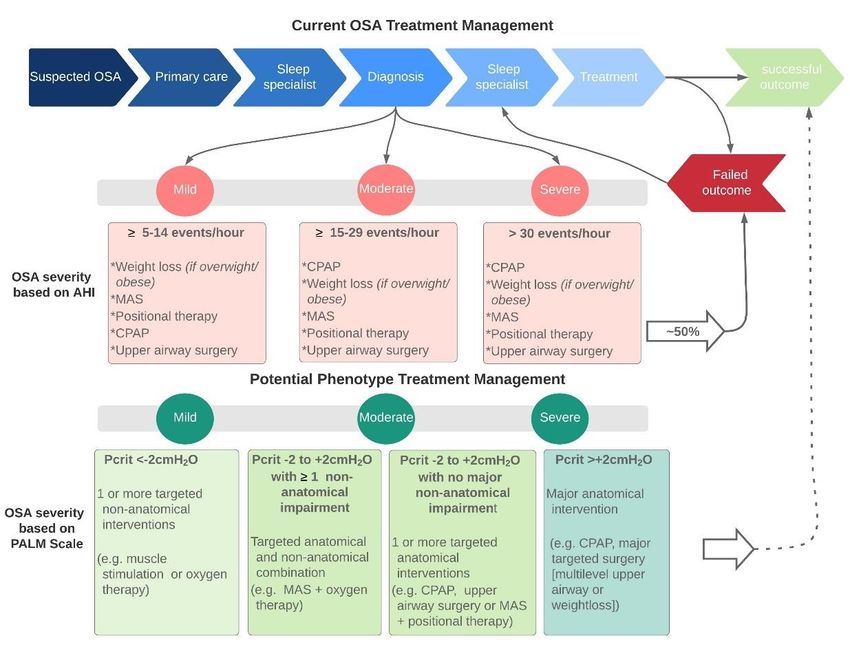
Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
Figure 1. Overview of current OSA management and severity categorization and an example of an
alternative potential phenotype-based management model.
Schematic of the current diaganosis and treament management pathway that involves multiple visits to a health care
practitioner, associated costs, with a high risk of treatment failure. This trial and error approach is often frustrating and
impractable for the patient. Diagnosis that relies on the AHI is not especially helpful in tailoring treatment decisions.
Thus, a personalized approach using targeted therapy would be desirable (potential phenotype treatment
management). The PALM scale32 (refer to the text for further details) categorizes patients according to their level of
anatomical impairment (mild, moderate, or severe) based on Pcrit (phayryngeal critical closing pressure of the upper
airway). Treatment decisions are further informed based on the contribution of nonanatomical impairment to OSA (e.g.,
arousal threshold, loop gain, and muscle responsiveness). Potential theapies that target nonanatomical phenotypes
include: supplemental oxygen, pharmacotherapies and electrical stimulation. 25 AHI = apnea/hypopnea index, MAS =
mandibular advancement splint, CPAP = continuous postive airway pressure.
required. and thus be more vulnerable to adverse cardiovascular
The current diagnostic process for OSA also has events,30,31 despite having a lower AHI. Evidently, the AHI
limitations. The apnea-hypopnea index (AHI) is the main is inadequate to capture the heterogeneous presentations
clinical measure used to define OSA severity. The AHI and consequences of OSA between individuals. Therefore,
represents the number of breathing events per hour of sleep there is a need for new diagnostic approaches that can more
lasting ≥10 s that have either a ≥90% airflow reduction comprehensively characterize OSA so that therapy can be
(apneas) from baseline or ≥30% airflow reduction tailored to the individual.
(hypopnea) with an accompanying brief awakening from To address these diagnostic and treatment challenges,
sleep (arousal) or oxygen desaturation (≥3%). Although a recent advances have been made in understanding the
widely used metric, it has several shortcomings. The characterization and management of OSA through a
severity of OSA, as measured by total AHI, correlates ‘phenotypic’ approach.25,32,33 This precision medicine
poorly with the key symptoms and consequences of approach is the focus of the current review. More
OSA.26-28 For example, a patient with longer but less specifically, this review summarizes how different
frequent events may have a lower AHI than a patient with ‘phenotypes’ contribute to the pathophysiology of OSA
shorter but more frequent events.29 However, the patient and how understanding these phenotypes can unlock new
with longer events may experience more severe hypoxemia avenues for targeted therapy. The role of phenotyping in
Journal of Dental Sleep Medicine Vol. 6, No.2 2019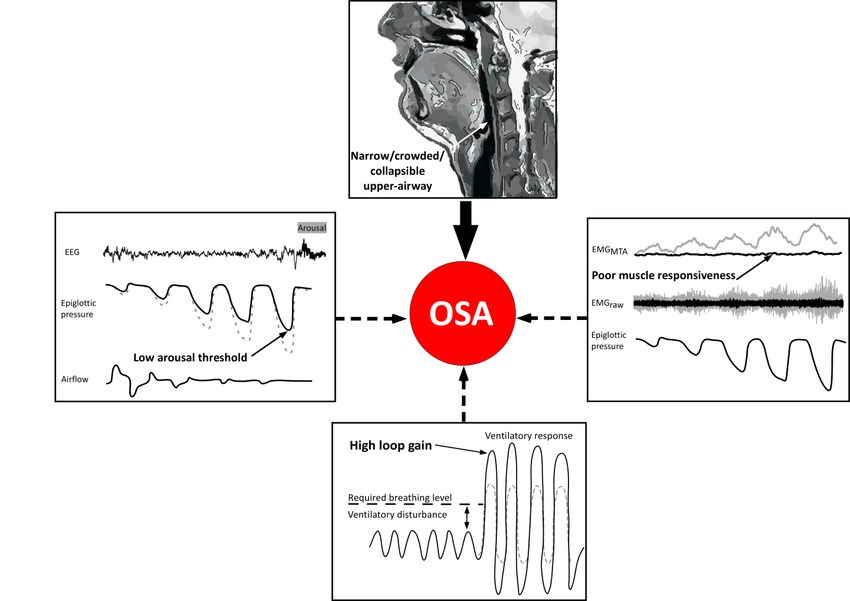
Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
MAS therapy to improve treatment and efficacy, and the tailored and comprehensive therapeutic approaches than
potential to translate phenotyping concepts into the clinical current treatment management pathways.
setting is also covered.
THE KEY PHENOTYPE FOR OSA: ANATOMICAL
A PHENOTYPIC APPROACH TO OSA IMPAIRMENT OF THE UPPER AIRWAY
PATHOGENESIS
In addition to the mandible, maxilla, and hyoid bones,
OSA is a multifactorial condition. Just as its clinical which are rigid structures, the upper airway is composed
manifestations are heterogeneous, so too is OSA of soft tissues such as the tongue, upper airway muscles,
pathogenesis. There are multiple factors or ‘phenotypes’ and parapharyngeal fat pads. This mix of bony support and
that can combine in different ways to cause OSA (Figure soft tissues allow the upper airway to quickly change its
2). The heterogeneity of OSA pathogenesis is the reason shape and size to perform its various key functions,
that simple clinical measures, such as the AHI, are including swallowing and speech. However, the malleable
inadequate to characterize the multiple manifestations of quality of the upper airway also renders it vulnerable to
OSA. This presents problems for current management closure and collapse during sleep in susceptible
approaches and the reliance on trial and error. However, individuals.
the heterogeneity of OSA also presents an opportunity. Some degree of anatomical impairment in one or more
Indeed, a more personalized approach has the potential to of the components of the upper airway is necessary for the
deliver targeted therapy or a combination of therapies to development of OSA. Imaging studies show that the cross-
the individual as each phenotype represents a unique sectional area of the upper airway is reduced in individuals
therapeutic target.25 with OSA compared with those without OSA.34 This
Although it is likely that there are other important narrowing renders the upper airway susceptible to collapse,
phenotypes or mediating mechanisms that have yet to be which can occur laterally, anteroposteriorly, or
determined, to date, four major phenotypes that contribute concentrically,37 at one or multiple levels along the
to OSA pathogenesis have been identified. A narrow, pharynx.38 Nonetheless, the site just behind the soft palate
crowded, or collapsible upper airway is the key (velopharyngeal area) is a particularly common site of
phenotype.32,34,35 Indeed, some degree of underlying collapse for most people with OSA.39 Obesity is a major
anatomical susceptibility to airway narrowing or collapse contributor to a narrow upper airway. Fat deposition in the
during sleep is essential for the development of OSA. structures surrounding the airway such as in the tongue,
However, the extent of impairment varies widely between soft tissues, lateral pharyngeal walls, and other pharyngeal
patients, even in those with similar severity of OSA as muscles can reduce the upper airway space in individuals
measured by AHI.32 Moreover, the anatomical structures with obesity and OSA.40 However, up to half of all patients
surrounding the airway remain constant between in whom OSA is diagnosed do not have obesity.41 Thus,
wakefulness and sleep and yet OSA only occurs during anatomical factors such as retrognathia and smaller
sleep. Thus, clearly there is more to OSA than just mandible area can restrict the size of the bony compartment
impairment in pharyngeal anatomy. Indeed, non- of the upper airway to cause upper airway narrowing and
anatomical phenotypes are also key contributors to OSA closure during sleep independent of obesity for many
pathogenesis. These include poor responsiveness or individuals with OSA.42 Relatively smaller increases in
contractility of the upper airway dilator muscles during weight in individuals of Chinese ethnicity compared to
sleep; unstable respiratory control (high ‘loop gain’) Caucasians also tend to favor increased propensity to
causing large breathing oscillations; and a low respiratory OSA.43 This is caused, in part, by differences in
arousal threshold to airway narrowing. Approximately craniofacial structures.43 Thus, in addition to obesity-
70% of individuals with OSA have one or more related narrowing, the shape and position of the
nonanatomical phenotypes that contribute to their OSA.32 surrounding craniofacial structures can also contribute to a
The relative contribution of anatomical and each narrow or collapsible upper airway.34,44
nonanatomical phenotype to OSA pathogenesis vary Anatomical impairment affects the collapsibility or
between individuals. This contributes to the heterogeneity functional anatomy of the upper airway during sleep,
of OSA, which can affect the clinical presentation and measured using the gold standard passive critical closing
responses to therapy. pressure (Pcrit) technique.32 On average, individuals with
Other factors such as inflammatory processes, OSA have a more collapsible or anatomically impaired
cerebral blood flow changes, hormonal changes, and upper airway than individuals without OSA (they have a
postural alterations as well as currently unknown variables higher Pcrit).32 Thus, their upper airway closes at higher
may also contribute to OSA pathophysiology and/or pressures and requires increased levels of CPAP to stay
interact with these four OSA phenotypes.36 Nonetheless, open during sleep. However, the degree of anatomical
the current phenotypic description of OSA pathogenesis, impairment varies greatly among individuals with OSA
even if incomplete, has the potential to inform more with Pcrit values ranging from -5 cmH2O to more than +5
Journal of Dental Sleep Medicine Vol. 6, No.2 2019Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
Figure 2. Schematic of the phenotypic traits that cause OSA.
Some degree of ‘impaired’ upper airway anatomy is a prerequisite for OSA (narrow/crowded/collapsible upper airway)
indicated by the thick solid arrow and MRI (top panel). Impairment in the nonanatomical traits (i.e., low respiratory arousal
threshold, poor pharyngeal muscle responsiveness, and high loop gain) also is an important contributor to OSA
pathogenesis for most patients (dashed arrows that also represent therapeutic targets). Schematic representation of each
of the nonanatomical traits (solid black lines with adjacent arrows) along with a more desirable response for each
nonanatomical trait (grey lines) is shown (left, right, and bottom panels). EEG = electroencephalogram, EMG = pharyngeal
electromyographic activity, MTA = moving time average (100 ms) of the rectified EMG signal. Adapted with permission
from Carberry JC, Amatoury J, Eckert DJ. Personalized management approach for OSA. Chest. 2018;153(3):744-755.
cmH2O.32,35 Indeed, within the subatmospheric range (Pcrit NONANATOMICAL PHENOTYPES AND THEIR
from -5 cmH2O to 0 cmH2O), there is considerable overlap ROLE IN OSA PATHOGENESIS
in Pcrit values between individuals with and without
OSA.32 For individuals with OSA with a moderate or mild Poor Upper Airway Muscle Function
anatomical impairment, there are additional nonanatomical
phenotypes that contribute to OSA pathogenesis and Because the pharynx lacks a rigid skeletal framework,
mediate OSA severity. Nevertheless, anatomical upper airway patency is instead primarily maintained by
impairment is still a key contributor to OSA and thus the surrounding dilator muscles. These muscles receive
remains an important target for therapy. Indeed, most complex neural drive from brainstem neurons that mediate
existing treatments – such as CPAP, MAS, weight loss, different patterns of activation during quiet breathing.45 For
surgery, and positional therapy – focus on rectifying the example, the genioglossus, which is the largest upper
anatomical impairment. However, as described earlier, in airway dilator muscle at the base of the tongue, has
individuals with OSA these methods have limitations and increased activation during inspiration.45 The genioglossus
provide suboptimal treatment or no treatment25 (Figure 1). also receives reflex input from pressure-sensitive
mechanoreceptors in the upper airway as well as
Journal of Dental Sleep Medicine Vol. 6, No.2 2019Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
chemoreceptor input.46,47 Sleep onset48,49 and different For example, the antidepressant desipramine prevents
sleep stages50 also alter the neural drive to dilator muscles sleep-related reductions in genioglossus muscle activity
and contribute to upper airway collapsibility during periods and reduces upper airway collapsibility in healthy
of low drive. However, there are other mediators of dilator individuals and those with OSA.61,62 The combination of
muscle activity beyond sleep-dependent neural control that reboxetine and hyoscine butylbromide also improves upper
also contribute to OSA pathogenesis. airway function during sleep, albeit via different
Even during sleep, respiratory stimuli (such as mechanisms than via increased genioglossus muscle
negative pharyngeal pressure changes or blood gas activity.63 Most recently, combination therapy with
changes) can trigger increases in neural drive to increase atomoxetine and oxybutynin, which have strong
upper airway dilator muscle activity.33,51 This response is noradrenergic and anticholinergic effects, increased
referred to as muscle responsiveness. However, more than genioglossus muscle responsiveness during sleep and
30% of individuals with OSA have negligible muscle reduced the AHI by approximately 75% (with all patients
responsiveness to airway narrowing during sleep with OSA having a ≥50% reduction in AHI).64 Although
(experimentally induced via negative pharyngeal pressures further clinical trials are needed, pharmacotherapies are
changes).32 These individuals do not have adequate dilator revealing novel and exciting potential approaches for
muscle recruitment until very high levels of respiratory management of OSA. This approach may prove to be
stimuli are reached. On the contrary, enhanced muscle especially fruitful in those with a poor upper airway muscle
responsiveness is protective against OSA, even in responsiveness phenotype.
individuals with obesity who have anatomical impairment
of the upper airway.52 Poor muscle effectiveness can also Low Respiratory Arousal Threshold
contribute to upper airway collapsibility in some
individuals with OSA.33 This is the inability of dilator It was previously thought that arousal from sleep was
muscles to adequately dilate the upper airway in response necessary to reopen the upper airway during a respiratory
to airway narrowing despite adequate neural drive and event.65 On the contrary, it is now understood that up to
muscle activation. Causes include poor coordination of 75% of respiratory events in OSA are resolved without an
neural drive to dilator muscles (which can result in arousal, or the arousal occurs after the respiratory event is
counterproductive movements),53,54 mechanically resolved.66 In other words, arousals are not necessarily
54
inefficient orientation of muscle fibers, or snoring- crucial for airway reopening and may be detrimental.
induced changes in the distribution of muscle fiber types Thirty percent to 50% of individuals with OSA wake from
(which can leave the upper airway more susceptible to sleep to very small increases in breathing effort (as
fatigue).55,56 Thus, poor muscle responsiveness or measured via negative esophageal or epiglottic pressure
effectiveness in individuals with pharyngeal anatomical swings).32 These individuals are repetitively aroused from
impairment are important contributors to OSA sleep to minimal stimuli and exhibit the phenotype of a low
pathogenesis (at least 30% of those with OSA).32 However, respiratory arousal threshold. This can contribute to their
each component of the poor muscle function phenotype is OSA pathogenesis for several reasons. One reason is that
potentially a novel target for therapy. frequent arousals prevent deeper, more stable stages of
For example, upper airway muscle training can help slow wave sleep and destabilize breathing patterns as a
reduce OSA severity. A systematic review showed that result of rapid changes in blood gases, both of which can
muscle training reduces the AHI by almost 50% and hinder adequate recruitment of upper airway dilator
improves oxygen saturation and daytime sleepiness.57 muscles.50,67 Indeed, as the stimuli for arousals are the
However, efficacy varies widely among individuals. Thus, same as those for upper airway muscle recruitment
increased knowledge into the mechanisms of how (negative pharyngeal pressure changes or blood gas
pharyngeal training improves upper airway function is changes), premature arousals limit the buildup of stimuli
required to move beyond the current trial-and-error that is required to activate these muscles and reopen the
approach and to design targeted training regimes to airway.68 Accordingly, a low respiratory arousal threshold
optimize efficacy. Stimulation of the hypoglossal nerve, is another nonanatomical phenotype that can play a crucial
which provides drive to the muscles of the tongue, reduces role in OSA pathogenesis for some patients.
the AHI by up to 70% or more with accompanying Frequent arousals also lead to fragmented sleep,
improvements in OSA symptoms.58,59 However, this which can cause sleep deprivation and a common
approach is not suitable for all patients with OSA and up to consequence of OSA, excessive daytime sleepiness.
one-third of those selected are nonresponders.58 As with Common hypnotic drugs such as eszoplicone, zoplicone,
any surgical procedure, potential safety and cost limitations zolpidem, and trazodone all raise the respiratory arousal
should be considered. Pharmacotherapies to increase upper threshold69-72 and can reduce the AHI by up to 50%69,70,73
airway muscle activity have long been a therapeutic target in certain patients. Although genioglossus activity is not
for OSA. Recent studies have highlighted the potential impaired,71,72 some hypnotic drugs at high doses may
importance of noradrenergic and anticholinergic targets.60 lengthen apneas and worsen oxygen saturation.71,74 In
Journal of Dental Sleep Medicine Vol. 6, No.2 2019Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
contrast, a recent 30-day randomized trial with zopiclone Upper Airway Anatomical Impairment
in patients with OSA with low and moderate respiratory
arousal thresholds did not worsen overnight oxygenation or MAS devices protrude the mandible with the aim of
next-day sleepiness or objective alterness.75 However, stiffening the surrounding upper airway structures to
there was also no therapeutic benefit on OSA severity.75 prevent pharyngeal narrowing or collapse during sleep.
Thus, questions remain as to the risk versus harm profile of Most studies to date have focused on how oral appliances
hypnotic drugs in OSA. This balance likely varies among alter upper airway anatomy and collapsibility (anatomical
patients according to their underlying phenotypes and impairment). Imaging studies show that MAS therapy
between different classes of hypnotic drugs. Of the studies increases the total volume of the upper airway in
conducted to date, eszopiclone has yielded the greatest responders to treatment.82-84 This is predominantly due to
therapeutic benefit for OSA.70,76 However, a recent detailed changes at the level of the velopharynx as reflected by
physiology study with zolpidem showed improvements in increased cross-sectional area, especially in the lateral
two of the key phenotypic traits, an increase in the dimensions.82,83,85 A direct soft-tissue connection between
respiratory arousal threshold and also an unexpected the ramus of the mandible and the lateral walls of the
threefold increase in genioglossus muscle responsiveness velopharynx may account for these changes.86 Lateral
during sleep.72 Thus, this agent has therapeutic potential displacement of the parapharyngeal fat pads may also
and additional studies are warranted. contribute to the increase in cross-sectional area.82
Contrary to traditional thinking,87 MAS devices do not
High Loop Gain appear to systematically increase the oropharyngeal
dimensions (section of upper airway at the level of the
A characteristic trait of OSA is the propensity to tongue).82 However, MAS devices can pull the entire
fluctuate between wake and sleep with periods of unstable tongue forward and prevent it from obstructing the upper
breathing. Breathing during sleep is regulated by partial airway in individuals with lower AHIs.86 MAS devices also
pressure of carbon dioxide, or PaCO2. A person’s elevate the hyoid bone.82 These anatomical changes are
sensitivity to changes in PaCO2 is mediated via negative associated with improvements in OSA severity82 and
feedback mechanisms that can be explained by the reflect some of the key mechanisms by which MAS therapy
engineering concept of loop gain. In simple terms, loop improves upper airway anatomy. MAS devices also
gain is the ratio of the magnitude of a ventilatory response improve functional upper airway collapsibility during
to a ventilatory disturbance. The key components that sleep.88-90 Indeed, depending on the level of advancement,
determine loop gain are: (1) plant gain (lungs, blood, and on average, MAS therapy improves upper airway
tissues where CO2 is stored in the body), (2) mixing gain collapsibility by 2 to 6 cmH2O.88,90 However, the precise
(circulatory delay, i.e., the time it takes for a change in CO2 mechanisms mediating these improvements and the
to mix with existing blood and be detected by the reasons why the magnitude of change differs markedly
chemoreceptors), and (3) controller gain (sensitivity of the between individuals remains unclear. Nonetheless, the
chemoreceptors, e.g. carotid body). A high loop gain (large predominant role of MAS therapy is to improve anatomical
ventilatory response to a small ventilatory disturbance) impairment of the upper airway.
reflects an overly sensitive ventilatory control system. This
phenotype perpetuates further breathing instability via MAS and Nonanatomical Phenotypes
excessive changes in CO2. Conversely, a more stable
system occurs when the ventilatory response is In addition to a direct role on anatomical impairment,
proportionate to the disturbance.33,77 High loop gain is MAS therapy may also improve upper airway muscle
thought to play a key role in OSA pathogenesis for at least function to reduce OSA severity. There are two key
30% of patients.32,78,79 Treatment strategies to lower loop possible mechanisms: (1) MAS therapy may stimulate
gain and reduce the AHI (typically by approximately 50%) local reflex afferents to increase upper airway muscle
include supplemental oxygen and acetazolamide.80,81 activity or, (2) changes in airway anatomy with MAS
therapy may result in increased mechanical efficiency of
MAS THERAPY: MECHANISMS OF ACTION the airway dilator muscles such that a given level of neural
drive results in greater improvements in airflow (improved
To determine how MAS therapy can best fit into a muscle efficiency). To date, the few studies that have been
personalized, phenotyping approach to treat OSA, the first conducted to investigate these two potential mechanisms
crucial step is to understand exactly how MAS therapy have yielded contrasting results. Consistent with the first
alters the key OSA phenotypes. In addition to improved mechanism, two earlier studies that used surface recording
understanding of the mechanisms, phenotyping approaches electrodes showed acute increases in upper airway dilator
should help to identify which patients with OSA will muscle activity (genioglossus and geniohyoid) awake
benefit most from MAS therapy. (seated and upright)91 and asleep during respiratory events
with mandibular advancement.92 Another study also
Journal of Dental Sleep Medicine Vol. 6, No.2 2019Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
showed that the baseline activity of the submandibular and A PHENOTYPIC APPROACH TO OSA THERAPY:
masseter muscles measured supine during quiet breathing THE PALM SCALE
and the activity of the submandibular and posterior
temporalis muscles with mandibular advancement were As highlighted, it is evident that OSA is a
higher in responders versus nonresponders to MAS multifactorial disorder. Nonanatomical phenotypes interact
therapy.93 However, two more recent studies using gold with an underlying anatomical impairment to cause OSA
standard intramuscular electromyography recordings of the and mediate its severity, or protect against OSA if
genioglossus muscle during sleep did not detect increases favorable. The combination of these phenotypes vary
in muscle activity with MAS therapy. Rather, one study between individuals with OSA, with some primarily
found that consistent with improved upper airway having an anatomical impairment whereas others may also
anatomy, MAS therapy reduced negative epiglottic have impairment in multiple nonanatomical phenotypes.32
pressure and consequently genioglossus muscle activity.94 These recent insights into the pathophysiology of OSA
The other study specifically investigated genioglossus have led to the development of a scale to characterize the
muscle responsiveness to negative airway pressure swings four key phenotypic causes of OSA to inform tailored
and did not detect systematic changes in muscle treatment: the Pcrit, Arousal threshold, Loop gain and
responsiveness with increasing levels of mandibular Muscle responsiveness (PALM scale).32,33 Briefly,
advancement.90 However, the sample size was relatively because impaired anatomy is the main driver of OSA,
small. patients are first categorized into one of three groups
Two studies have investigated the second potential according to their upper airway anatomy/collapsibility
mechanism, increased mechanical efficiency with MAS (Pcrit). PALM scale 1 patients (23%) have severely
therapy. Edwards and colleagues89 assessed changes in impaired anatomy (Pcrit> + 2 cmH2O) and likely require a
ventilation (upper airway airflow) as a surrogate measure major anatomical intervention to treat their OSA (e.g.
of muscle function. No difference in this parameter was CPAP). Most individuals with OSA (58%) are categorized
found with the MAS device in place versus without. as PALM scale 2. These patients have moderately impaired
Bamagoos and colleagues90 systematically investigated anatomy (Pcrit between -2 and + 2 cmH2O) and are
changes in minute ventilation and airflow in conjunction potential candidates for one or a combination of targeted
with genioglossus EMG in response to experimentally anatomical (such as MAS, upper airway surgery, or supine
induced airflow limitation using transient reductions in avoidance device) and/or nonanatomical interventions
CPAP at different levels of mandibular advancement. (e.g., a hypnotic increase the arousal threshold and reduce
Similar to the study by Edwards and colleagues,89 there was OSA severity in those with a low arousal threshold; O2 to
no evidence for improved muscle efficacy with mandibular reduce unstable ventilatory control in those with high loop
advancement.90 A limitation of both of these studies was gain; or a drug to increase pharyngeal muscle contractility
that the sample size was quite small; therefore, the potential in those with poor muscle responsiveness during sleep).
for some individuals with certain phenotypes to have Finally, the remaining 19% of patients are PALM scale 3.
improved muscle function with MAS therapy remains. These individuals have only mild anatomical impairment
Accordingly, additional appropriately designed studies to (Pcrit between -2 and -5cmH2O), similar to many
investigate the effects of MAS therapy on upper airway individuals without OSA. All patients categorized as
muscle function are required. PALM scale 3 have impairment in one or more
Thus, although there are clear theoretical reasons as to nonanatomical phenotypes. These patients are candidates
why MAS therapy could improve upper airway muscle for one or more targeted therapies with nonanatomic
function to complement the anatomical benefits, the interventions likely to be particularly beneficial (see
available evidence to date shows contrasting effects of Figures 1 and 3). Importantly, using this conceptual
MAS therapy on upper airway muscle activity and no framework and the known effect sizes for non-CPAP
evidence for systematic improvements in upper airway interventions, it is estimated that more than 50% of all
muscle function. Thus far, there have been limited studies patients with OSA could be treated with one or more non-
into how MAS therapy alters the other two nonanatomical CPAP interventions if appropriately directed at the
phenotypes – loop gain and arousal threshold. Edwards and abnormal trait(s).95
colleagues89 found that wearing a MAS device did not
affect these two phenotypes. However, the study Application of the PALM Scale Approach to MAS
participants were already on MAS therapy for varying Therapy
amounts of time, potentially influencing the expression of
these two non-anatomical phenotypes. Thus, future studies Consistent with the variable treatment responses to
in treatment-naïve individuals with OSA would be MAS therapy in OSA, the PALM scale predicts that MAS
insightful. therapy will improve the impaired anatomy phenotype to
yield therapeutic benefit in some but not all patients with
OSA. Specifically, given that on average MAS therapy
Journal of Dental Sleep Medicine Vol. 6, No.2 2019Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
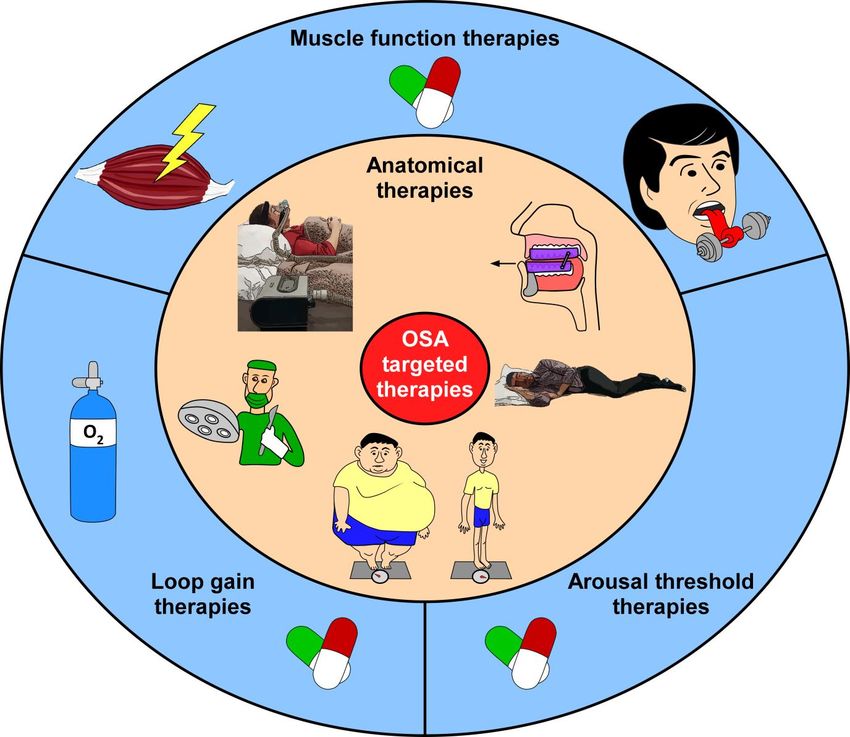
Figure 3. Schematic summary of existing and evolving targeted therapies to treat OSA.
Existing anatomical therapies (clockwise from left to right, inner peach-colored circle) include: continuous positive
airway pressure (CPAP), oral appliance therapy (e.g., mandibular advancement splint), positional therapy, weight loss,
and upper airway surgery. Nonanatomical therapies (blue outer circle) to improve pharyngeal muscle function include:
hypoglossal nerve stimulation, pharmacotherapies and pharyngeal muscle training; sleep promotion agents to increase
the respiratory arousal threshold; and O2 therapy and pharmacotherapies to decrease loop gain. Adapted with
permission from Carberry JC, Amatoury J, Eckert DJ. Personalized management approach for OSA. Chest.
2018;153(3):744-755.
improves Pcrit by 2 to 6 cmH2O,88,90 patients who have less arosual threshold). Thus, in patients who have high levels
impairment in upper airway anatomy at baseline (PALM of impairment in one or more of the nonanatomical traits
scale 2 and 3) are expected to have a larger therapeutic (e.g., low arousal threshold or high loop gain), repetitive
response with MAS therapy than those with highly awakenings and unstable respiratory control, and therefore
impaired anatomy (patients categorized as PALM scale 1) OSA, are expected to persist with MAS therapy. In support
in whom minimal or no change is expected. Indeed, in of this mechanistic rationale, a recent retrospective study
order to resolve the anatomical impediment of OSA, the in which the four phenotypic traits were estimated in 14
goal of therapy is to reduce Pcrit below -5cmH2O.33 patients with OSA with and without MAS therapy
Furthermore, the PALM scale predicts that nonanatomical demonstrated greater therapeutic efficacy in those with
traits will be important mediators of treatment response to minimal anatomical impairment (mild upper airway
MAS therapy. Specifically, with its primary role to collapsibility) and minimal respiratory instability (low loop
improve upper airway anatomy, and to a lesser extent, a gain).89 As discussed in the next paragraphs, the current
potential role on upper airway muscle function, consistent challenge is how to translate these concepts to the clinical
with the available data,89 MAS therapy is not anticipated to setting.
alter the other two nonanatomical traits (loop gain and
Journal of Dental Sleep Medicine Vol. 6, No.2 2019Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
TRANSLATION OF OSA PHENOTYPING effectiveness is likely to be superior compared to the
CONCEPTS TO THE CLINICAL SETTING current diagnostic pathway. However, formal cost-benefit
analyses will clearly be required as phenotyping
To overcome the barriers associated with current gold approaches continue to be developed, refined, and
standard phenotyping techniques (e.g., invasive overnight improved. Nonetheless, these concepts and evolving tools
in-laboratory studies limited to research investigations),33 offer promise that the goal of clinically feasible, accurate
there have been recent advances in the development of tools to tailor therapy to individual patients with OSA will
simplified phenotyping tools for clinical implementation. be a reality in the not-too-distant future. This includes new
For example, brief breathing tests acquired during approaches to optimize MAS therapy and improved
wakefulness correlate well with upper airway collapsibility prediction of treatment success.
(Pcrit) during sleep.96,97 Similarly, automated measures of
peak flow obtained via a standard overnight PSG provide SUMMARY AND CONCLUSIONS
good estimates of Pcrit.98 An individual’s therapeutic
CPAP level (≤8.0 cmH2O) also shows good sensitivity OSA phenotyping concepts offer potential to facilitate
(89%) and specificity (84%) to identify a patient with a realignment of the current treatment management approach
mildly collapsible upper airway.99 Thus, these approaches for OSA, which is too frequently time consuming, costly,
may be helpful clinically to differentiate the extent of and ineffective. In the context of dental sleep medicine,
anatomical impairment (i.e., those with highly versus detailed OSA phenotyping can help to determine the
minimally collapsible airways), the main contributor to mechanisms of MAS therapy, which may help to optimize
OSA, to facilitate targeted treatment decisions using MAS therapy design for greater efficacy. Phenotyping
PALM scale concepts. Similarly, inspiratory airflow approaches also have the potential to assist in the accurate
profiles during flow limitation from an overnight sleep identification of the characteristics of responders to MAS
study may provide information on the site of upper airway therapy. Indeed, the ideal candidate based on current
collapse.100 phenotyping concepts and the available evidence is a
Recent strategies have also been developed to patient with a mild to moderately collapsible upper airway
estimate the nonanatomical phenotypes. This includes with minimal or no impairment in the other non-anatomical
estimates of loop gain and arousal threshold from PSG phenotypes (i.e., the patient does not have high loop gain).
recordings using sophisticated analysis methods,101,102 or Clinical implementation of these concepts could improve
via simple breath hold maneuvers,103 or simply using current prediction approaches and reduce MAS therapy
standard clinical PSG variables.104 Although a simple failure rates, which has long been a major clinical
clinically useful estimate of upper airway muscle function challenge for the field. Finally, as simplified phenotyping
is yet to be determined, recent advanced signal processing approaches and novel non-CPAP therapies continue to
techniques have been used successfully to estimate all four develop and evolve, there is also scope for phenotyping
phenotypes including muscle compensation from standard approaches to be used to inform targeted combination
PSG recordings.105 therapy for those with major impairment in the
From a clinical perspective, some of these methods nonanatomical phenotypes and in those who do not
rely entirely on data (i.e. AHI, nadir oxygen saturation, respond to MAS therapy alone.107
fraction of events that are hypopneas, therapeutic CPAP
levels) that are already routinely collected during REFERENCES
diagnostic or titration sleep studies for OSA.99,104 Thus,
these strategies can be incorporated into the current 1. Heinzer R, Vat S, Marques-Vidal P, et al. Prevalence of sleep-
disordered breathing in the general population: the HypnoLaus
recommended diagnostic pathway for OSA106 with study. Lancet Resp Med. 2015;3(4):310-318.
negligible additional cost to help guide patient selection
2. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM.
decisions for MAS therapy. Conversely, others still require Increased prevalence of sleep-disordered breathing in adults. Am
advanced signal processing analysis or specialized J Epidemiol. 2013;177(9):1006-1014.
equipment before they can be implemented into the current 3. Young T, Skatrud J, Peppard PE. Risk factors for obstructive
diagnostic pathway. However, the computations for some sleep apnea in adults. JAMA. 2004;291(16):2013-2016.
of these methods can be completed within 10 minutes for 4. Adult Obstructive Sleep Apnea Task Force of the American
each patient on a standard personal computer and there is Academy of Sleep M. Clinical Guideline for the Evaluation,
Management and Long-term Care of Obstructive Sleep Apnea in
scope for automation.101,102 Other methods can be Adults. J Clin Sleep Med. 2009;5(3):263-276.
performed relatively quickly during wakefulness and do 5. Lacasse Y, Godbout C, Sériès F. Health-related quality of life in
not require entire overnight PSG.96,97 Therefore, obstructive sleep apnoea. Eur Resp J. 2002;19(3):499-503.
considering the potential health and safety benefits from 6. Ellen RL, Marshall SC, Palayew M, Molnar FJ, Wilson KG,
achieving treatment success via tailored therapy with fewer Man-Son-Hing M. Systematic review of motor vehicle crash risk
treatment failures and associated costs (Figure 1), the cost- in persons with sleep apnea. J Clin Sleep Med. 2006;2(02):193-
200.
Journal of Dental Sleep Medicine Vol. 6, No.2 2019Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
7. Hla KM, Young T, Hagen EW, et al. Coronary Heart Disease 26. Macey PM, Woo MA, Kumar R, Cross RL, Harper RM.
Incidence in Sleep Disordered Breathing: The Wisconsin Sleep Relationship between obstructive sleep apnea severity and sleep,
Cohort Study. Sleep. 2015;38(5):677-684. depression and anxiety symptoms in newly-diagnosed patients.
PLoS One. 2010;5(4):e10211.
8. Redline S, Yenokyan G, Gottlieb DJ, et al. Obstructive sleep
apnea–hypopnea and incident stroke: The Sleep Heart Health 27. Weaver EM, Woodson BT, Steward DL. Polysomnography
Study. Am J Resp Crit Care Med. 2010;182(2):269-277. indexes are discordant with quality of life, symptoms, and
reaction times in sleep apnea patients. Otolaryngol Head Neck
9. Aurora RN, Punjabi NM. Obstructive sleep apnoea and type 2 Surg. 2005;132(2):255-262.
diabetes mellitus: a bidirectional association. Lancet Resp Med.
2013;1(4):329-338. 28. Johansson P, Alehagen U, Svanborg E, Dahlstrom U, Brostrom
A. Sleep disordered breathing in an elderly community-living
10. Osorio RS, Gumb T, Pirraglia E, et al. Sleep-disordered breathing population: Relationship to cardiac function, insomnia symptoms
advances cognitive decline in the elderly. Neurology. and daytime sleepiness. Sleep Med. 2009;10(9):1005-1011.
2015;84(19):1964-1971.
29. Muraja-Murro A, Nurkkala J, Tiihonen P, et al. Total duration of
11. BaHammam AS, Kendzerska T, Gupta R, et al. Comorbid apnea and hypopnea events and average desaturation show
depression in obstructive sleep apnea: an under-recognized significant variation in patients with a similar apnea-hypopnea
association. Sleep Breath. 2016;20(2):447-456. index. J Med Eng Technol. 2012;36(8):393-398.
12. Marshall NS, Wong KK, Phillips CL, Liu PY, Knuiman MW, 30. Wu H, Zhan X, Zhao M, Wei Y. Mean apnea-hypopnea duration
Grunstein RR. Is sleep apnea an independent risk factor for (but not apnea-hypopnea index) is associated with worse
prevalent and incident diabetes in the Busselton Health Study? J hypertension in patients with obstructive sleep apnea. Medicine.
Clin Sleep Med. 2009;5(1):15-20. 2016;95(48):e5493.
13. McDaid C, Durée KH, Griffin SC, et al. A systematic review of 31. Alex R, Manchikatla S, Machiraju K, et al. Effect of apnea
continuous positive airway pressure for obstructive sleep duration on apnea induced variations in cerebral blood flow
apnoea–hypopnoea syndrome. Sleep Med Rev. 2009;13(6):427- velocity and arterial blood pressure. Conf Proc IEEE Eng Med
436. Biol Soc. 2014;2014:270-273.
14. Galic T, Bozic J, Pecotic R, Ivkovic N, Valic M, Dogas Z. 32. Eckert DJ, White DP, Jordan AS, Malhotra A, Wellman A.
Improvement of cognitive and psychomotor performance in Defining phenotypic causes of obstructive sleep apnea.
patients with mild to moderate obstructive sleep apnea treated Identification of novel therapeutic targets. Am J Resp Crit Care
with mandibular advancement device: A prospective 1-year Med. 2013;188(8):996-1004.
study. J Clin Sleep Med. 2016;12(2):177-186.
33. Eckert DJ. Phenotypic approaches to obstructive sleep apnoea –
15. Lin HC, Friedman M, Chang HW, Gurpinar B. The efficacy of new pathways for targeted therapy. Sleep Med Rev. 2018;37:45-
multilevel surgery of the upper airway in adults with obstructive 59.
sleep apnea/hypopnea syndrome. Laryngoscope.
2008;118(5):902-908. 34. Neelapu BC, Kharbanda OP, Sardana HK, et al. Craniofacial and
upper airway morphology in adult obstructive sleep apnea
16. Peppard PE, Young T, Palta M, Dempsey J, Skatrud J. patients: A systematic review and meta-analysis of cephalometric
Longitudinal study of moderate weight change and sleep- studies. Sleep Med Rev. 2017;31:79-90.
disordered breathing. JAMA. 2000;284(23):3015-3021.
35. Kirkness JP, Schwartz AR, Schneider H, et al. Contribution of
17. McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of male sex, age, and obesity to mechanical instability of the upper
cardiovascular events in obstructive sleep apnea. N Engl J Med. airway during sleep. J Appl Physiol. 2008;104(6):1618-1624.
2016;375(10):919-931.
36. Dempsey JA, Veasey SC, Morgan BJ, O'Donnell CP.
18. Weaver TE, Grunstein RR. Adherence to continuous positive Pathophysiology of sleep apnea. Physiol Rev. 2010;90(1):47-112.
airway pressure therapy: the challenge to effective treatment.
Proc Am Thor Soc. 2008;5(2):173-178. 37. Ravesloot MJL, de Vries N. One hundred consecutive patients
undergoing drug-induced sleep endoscopy: Results and
19. Sutherland K, Vanderveken OM, Tsuda H, et al. Oral appliance evaluation. Laryngoscope. 2011;121(12):2710-2716.
treatment for obstructive sleep apnea: An update. J Clin Sleep
Med. 2014;10(2):215-227. 38. Vroegop AV, Vanderveken OM, Boudewyns AN, et al. Drug‐
induced sleep endoscopy in sleep‐disordered breathing: Report
20. Sutherland K, Takaya H, Qian J, Petocz P, Ng AT, Cistulli PA. on 1,249 cases. Laryngoscope. 2014;124(3):797-802.
Oral appliance treatment response and polysomnographic
phenotypes of obstructive sleep apnea. J Clin Sleep Med. 39. Marques M, Genta PR, Azarbarzin A, et al. Retropalatal and
2015;11(8):861-868. retroglossal airway compliance in patients with obstructive sleep
apnea. Respir Physiol Neurobiol. 2018;258:98-103.
21. Lee RW, Petocz P, Prvan T, Chan AS, Grunstein RR, Cistulli PA.
Prediction of obstructive sleep apnea with craniofacial 40. Schwab RJ, Pasirstein M, Pierson R, et al. Identification of upper
photographic analysis. Sleep. 2009;32(1):46-52. airway anatomic risk factors for obstructive sleep apnea with
volumetric magnetic resonance imaging. Am J Resp Crit Care
22. Jayawardhana M, Sutherland K, Cistulli P, Chazal P. Prediction Med. 2003;168(5):522-530.
of MAS therapy response in obstructive sleep apnoea patients
using clinical data. Conf Proc IEEE Eng Med Biol Soc. 41. Gray EL, McKenzie DK, Eckert DJ. Obstructive sleep apnea
2018;2018:6040-6043. without obesity is common and difficult to treat: Evidence for a
distinct pathophysiological phenotype. J Clin Sleep Med.
23. Vroegop AV, Vanderveken OM, Dieltjens M, et al. Sleep 2017;13(1):81–88.
endoscopy with simulation bite for prediction of oral appliance
treatment outcome. J Sleep Res. 2013;22(3):348-355. 42. Okubo M, Suzuki M, Horiuchi A, et al. Morphologic analyses of
mandible and upper airway soft tissue by MRI of patients with
24. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health obstructive sleep apnea hypopnea syndrome. Sleep.
outcomes of continuous positive airway pressure versus oral 2006;29(7):909-915.
appliance treatment for obstructive sleep apnea: a randomized
controlled trial. Am J Respir Crit Care Med. 2013;187(8):879- 43. Lee RW, Vasudavan S, Hui DS, et al. Differences in craniofacial
887. structures and obesity in Caucasian and Chinese patients with
obstructive sleep apnea. Sleep. 2010;33(8):1075-1080.
25. Carberry JC, Amatoury J, Eckert DJ. Personalized management
approach for OSA. Chest. 2018;153(3):744-755.
Journal of Dental Sleep Medicine Vol. 6, No.2 2019Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
44. Chi L, Comyn F-L, Mitra N, et al. Identification of craniofacial 63. Lim R, Carberry JC, Wellman A, Grunstein R, Eckert DJ.
risk factors for obstructive sleep apnoea using three-dimensional Reboxetine and hyoscine butylbromide improve upper airway
MRI. Eur Resp J. 2011;38(2):348-358. function during non-REM and suppress REM sleep in healthy
individuals. Sleep.
45. Saboisky JP, Butler JE, Fogel RB, et al. Tonic and phasic
respiratory drives to human genioglossus motoneurons during 64. Taranto-Montemurro L, Messineo L, Sands SA, et al. The
breathing. J Neurophysiol. 2006;95(4):2213-2221. combination of atomoxetine and oxybutynin greatly reduces
obstructive sleep apnea severity: A randomized, placebo-
46. Carberry JC, Hensen H, Fisher LP, et al. Mechanisms controlled, double-blind crossover trial. Am J Resp Crit Care
contributing to the response of upper-airway muscles to changes Med. 2018; doi: 10.1164/rccm.201808-1493OC. [Epub ahead of
in airway pressure. J Appl Physiol. 2015;118(10):1221-1228. print].
47. Stanchina ML, Malhotra A, Fogel RB, et al. Genioglossus muscle 65. Phillipson EA, Sullivan CE. Arousal: The forgotten response to
responsiveness to chemical and mechanical stimuli during non- respiratory stimuli. Am Rev Resp Dis. 1978;118(5):807-809.
rapid eye movement sleep. Am J Respir Crit Care Med.
2002;165(7):945-949. 66. Younes M. Role of Arousals in the pathogenesis of obstructive
sleep apnea. Am J Resp Crit Care Med. 2004;169(5):623-633.
48. Eckert DJ, McEvoy RD, George KE, Thomson KJ, Catcheside
PG. Genioglossus reflex inhibition to upper-airway negative- 67. Eckert DJ, Younes MK. Arousal from sleep: implications for
pressure stimuli during wakefulness and sleep in healthy males. obstructive sleep apnea pathogenesis and treatment. J Appl
J Physiol. 2007;581(3):1193-1205. Physiol. 2014;116(3):302-313.
49. Wilkinson V, Malhotra A, Nicholas CL, et al. Discharge patterns 68. Younes M, Ostrowski M, Atkar R, Laprairie J, Siemens A, Hanly
of human genioglossus motor units during sleep onset. Sleep. P. Mechanisms of breathing instability in patients with
2008;31(4):525-533. obstructive sleep apnea. J Appl Physiol. 2007;103(6):1929-1941.
50. Carberry JC, Jordan AS, White DP, Wellman A, Eckert DJ. 69. Eckert DJ, Malhotra A, Wellman A, White DP. Trazodone
Upper airway collapsibility (Pcrit) and pharyngeal dilator muscle increases the respiratory arousal threshold in patients with
activity are sleep stage dependent. Sleep. 2016;39(3):511-521. obstructive sleep apnea and a low arousal threshold. Sleep.
2014;37(4):811-819.
51. Loewen AHS, Ostrowski M, Laprairie J, Maturino F, Hanly PJ,
Younes M. Response of genioglossus muscle to increasing 70. Eckert DJ, Owens RL, Kehlmann G B, et al. Eszopiclone
chemical drive in sleeping obstructive apnea patients. Sleep. increases the respiratory arousal threshold and lowers the
2011;34(8):1061-1073. apnoea/hypopnoea index in obstructive sleep apnoea patients
with a low arousal threshold. Clin Sci (Lond). 2011;120(12):505-
52. Sands SA, Eckert DJ, Jordan AS, et al. Enhanced upper-airway 514.
muscle responsiveness is a distinct feature of overweight/obese
individuals without sleep apnea. Am J Respir Crit Care Med. 71. Carter SG, Berger MS, Carberry JC, et al. Zopiclone Increases
2014;190(8):930-937. the arousal threshold without impairing genioglossus activity in
obstructive sleep apnea. Sleep. 2016;39(4):757-766.
53. Brown EC, Cheng S, McKenzie DK, Butler JE, Gandevia SC,
Bilston LE. Respiratory movement of upper airway tissue in 72. Carberry JC, Fisher LP, Grunstein RR, et al. Role of common
obstructive sleep apnea. Sleep. 2013;36(7):1069-1076. hypnotics on the phenotypic causes of obstructive sleep apnoea:
paradoxical effects of zolpidem. Eur Respir J. 2017;50(6).
54. Bilston LE, Gandevia SC. Biomechanical properties of the
human upper airway and their effect on its behavior during 73. Carberry JC, Grunstein R, Eckert DJ. The effects of zolpidem in
breathing and in obstructive sleep apnea. J Appl Physiol. obstructive sleep apnoea– an open-label pilot study. J Sleep Res.
2014;116(3):314-324. 2019:In press.
55. Saboisky JP, Butler JE, Gandevia SC, Eckert DJ. Functional role 74. Berry RB, Kouchi K, Bower J, Prosise G, Light RW. Triazolam
of neural injury in obstructive sleep apnea. Front Neurol. in patients with obstructive sleep apnea. Am J Resp Crit Care
2012;3:95-95. Med. 1995;151(2):450-454.
56. Eckert DJ, Lo YL, Saboisky JP, Jordan AS, White DP, Malhotra 75. Carter SG, Carberry JC, Cho G, et al. Effect of 1 month of
A. Sensorimotor function of the upper-airway muscles and zopiclone on obstructive sleep apnoea severity and symptoms: a
respiratory sensory processing in untreated obstructive sleep randomised controlled trial. Eur Respir J. 2018;52(1).
apnea. J Appl Physiol. 2011;111(6):1644-1653.
76. Edwards BA, Sands SA, Owens RL, et al. The combination of
57. Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy supplemental oxygen and a hypnotic markedly improves
to treat obstructive sleep apnea: A systematic review and meta- obstructive sleep apnea in patients with a mild to moderate upper
analysis. Sleep. 2015;38(5):669-675. airway collapsibility. Sleep. 2016;39(11):1973-1983.
58. Strollo PJ, Soose RJ, Maurer JT, et al. Upper-airway stimulation 77. Osman AM, Carter SG, Carberry JC, Eckert DJ. Obstructive
for obstructive sleep apnea. N Engl J Med. 2014;370(2):139-149. sleep apnea: current perspectives. Nat Sci Sleep. 2018;10:21-34.
59. Eastwood PR, Barnes M, Walsh JH, et al. Treating obstructive 78. Younes M, Ostrowski M, Thompson W, Leslie C, Shewchuk W.
sleep apnea with hypoglossal nerve stimulation. Sleep. Chemical control stability in patients with obstructive sleep
2011;34(11):1479-1486. apnea. Am J Respir Crit Care Med. 2001;163(5):1181-1190.
60. Horner RL, Grace KP, Wellman A. A resource of potential drug 79. Wellman A, Jordan AS, Malhotra A, et al. Ventilatory control and
targets and strategic decision-making for obstructive sleep airway anatomy in obstructive sleep apnea. Am J Respir Crit Care
apnoea pharmacotherapy. Respirology. 2017;22(5):861-873. Med. 2004;170(11):1225-1232.
61. Taranto-Montemurro L, Sands SA, Edwards BA, et al. 80. Wellman A, Malhotra A, Jordan AS, Stevenson KE, Gautam S,
Desipramine improves upper airway collapsibility and reduces White DP. Effect of oxygen in obstructive sleep apnea: role of
OSA severity in patients with minimal muscle compensation. Eur loop gain. Respir Physiol Neurobiol. 2008;162(2):144-151.
Resp J. 2016;48(5):1340-1350.
81. Edwards BA, Sands SA, Eckert DJ, et al. Acetazolamide
62. Taranto-Montemurro L, Edwards BA, Sands SA, et al. improves loop gain but not the other physiological traits causing
Desipramine Increases Genioglossus Activity and Reduces obstructive sleep apnoea. J Physiol. 2012;590(5):1199-1211.
Upper Airway Collapsibility during Non-REM Sleep in Healthy
Subjects. Am J Resp Crit Care Med. 2016;194(7):878-885.
Journal of Dental Sleep Medicine Vol. 6, No.2 2019Sleep Apnea Phenotyping: Implications for Dental Sleep Medicine - Lai et al.
82. Chan AS, Sutherland K, Schwab RJ, et al. The effect of 100. Genta PR, Sands SA, Butler JP, et al. Airflow shape is associated
mandibular advancement on upper airway structure in obstructive with the pharyngeal structure causing OSA. Chest.
sleep apnoea. Thorax. 2010;65(8):726-732. 2017;152(3):537-546.
83. Tsuiki S, Lowe AA, Almeida FR, Kawahata N, Fleetham JA. 101. Terrill PI, Edwards BA, Nemati S, et al. Quantifying the
Effects of mandibular advancement on airway curvature and ventilatory control contribution to sleep apnoea using
obstructive sleep apnoea severity. Eur Resp J. 2004;23(2):263- polysomnography. Eur Respir J. 2015;45(2):408-418.
268.
102. Sands SA, Terrill PI, Edwards BA, et al. Quantifying the arousal
84. Sam K, Lam B, Ooi CG, Cooke M, Ip MS. Effect of a non- threshold using polysomnography in obstructive sleep apnea.
adjustable oral appliance on upper airway morphology in Sleep. 2018;41(1).
obstructive sleep apnoea. Resp Med. 2006;100(5):897-902.
103. Messineo L, Taranto-Montemurro L, Azarbarzin A, et al. Breath-
85. Kyung SH, Park Y-C, Pae E-K. Obstructive sleep apnea patients holding as a means to estimate the loop gain contribution to
with the oral appliance experience pharyngeal size and shape obstructive sleep apnoea. J Physiol. 2018;596(17):4043-4056.
changes in three dimensions. Angle Orthod. 2005;75(1):15-22.
104. Edwards BA, Eckert DJ, McSharry DG, et al. Clinical Predictors
86. Brown EC, Cheng S, McKenzie DK, Butler JE, Gandevia SC, of the Respiratory Arousal Threshold in Patients with Obstructive
Bilston LE. Tongue and lateral upper airway movement with Sleep Apnea. Am J Resp Crit Care Med. 2014;190(11):1293-
mandibular advancement. Sleep. 2014;36(3):397-404. 1300.
87. Cistulli PA, Gotsopoulos H, Marklund M, Lowe AA. Treatment 105. Sands SA, Edwards BA, Terrill PI, et al. Phenotyping pharyngeal
of snoring and obstructive sleep apnea with mandibular pathophysiology using polysomnography in patients with
repositioning appliances. Sleep Med Rev. 2004;8(6):443-457. obstructive sleep apnea. Am J Respir Crit Care Med.
2018;197(9):1187-1197.
88. Ng AT, Gotsopoulos H, Qian J, Cistulli PA. Effect of oral
appliance therapy on upper airway collapsibility in obstructive 106. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice
sleep apnea. Am J Resp Crit Care Med. 2003;168(2):238-241. guideline for diagnostic testing for adult obstructive sleep apnea:
An American Academy of Sleep Med clinical practice guideline.
89. Edwards BA, Andara C, Landry S, et al. Upper-airway J Clin Sleep Med. 2017;13(3):479-504.
collapsibility and loop gain predict the response to oral appliance
therapy in patients with obstructive sleep apnea. Am J Resp Crit 107. Lai V, Tong B, Tran C, et al. Combination therapy with
Care Med. 2016;194(11):1413-1422. mandibular advancement and expiratory positive airway pressure
valves reduces OSA severity. J Sleep Res. 2018;27(2):P168
90. Bamagoos AA, Cistulli PA, Sutherland K, et al. Dose-dependent [abstract].
effects of mandibular advancement on upper airway collapsibility
and muscle function in obstructive sleep apnea. Sleep. 2019; Feb
22. pii: zsz049. doi: 10.1093/sleep/zsz049. [Epub ahead of print].
SUBMISSION &
91. Johal A, Gill G, Ferman A, McLaughlin K. The effect of
mandibular advancement appliances on awake upper airway and CORRESPONDENCE INFORMATION
masticatory muscle activity in patients with obstructive sleep
apnoea. Clin Physiol Funct Imaging. 2007;27(1):47-53.
Submitted for publication March 4, 2019
92. Yoshida K. Effect of a prosthetic appliance for treatment of sleep Submitted in final revised form March 28, 2019
apnea syndrome on masticatory and tongue muscle activity. J
Prosthet Dent. 1998;79(5):537-544. Accepted for publication March 29, 2019
93. Ma SY, Whittle T, Descallar J, et al. Association between resting
jaw muscle electromyographic activity and mandibular Address correspondence to: Prof. Danny J. Eckert,
advancement splint outcome in patients with obstructive sleep Adelaide Institute for Sleep Health (AISH), Flinders
apnea. Am J Orthod Dentofacial Orthop. 2013;144(3):357-367.
University, Level 2, Mark Oliphant Building, 5 Laffer
94. Burke P, Knapman F, Tong B, et al. Effects of mandibular Drive, Bedford Park SA 5042, Phone: +61 8 7421 9780,
advancement splints on upper airway physiology in obstructive
sleep apnoea. J Sleep Res. 2018;27(2):P114 [abstract]. Email: danny.eckert@flinders.edu.au
95. Owens RL, Edwards BA, Eckert DJ, et al. An integrative model
of physiological traits can be used to predict obstructive sleep DISCLOSURE STATEMENT
apnea and response to non positive airway pressure therapy.
Sleep. 2015;38(6):961-970. DJE is supported by a National Health and Medical
96. Hirata RP, Schorr F, Kayamori F, et al. Upper airway Research Council of Australia Senior Research Fellowship
collapsibility assessed by negative expiratory pressure while
awake is associated with upper airway anatomy. J Clin Sleep
(1116942), has a Cooperative Research Centre (CRC)-P
Med. 2016;12(10):1339-1346. grant: a collaborative grant between the Australian
97. Osman A, Carberry J, Burke PG, Grunstein R, Eckert D. Upper Government, Academia and Industry (Industry partner
airway collapsibility measured using a simple wakefulness test Oventus Medical), has been a collaborator on research
closely relates to the pharyngeal critical closing pressure (Pcrit) projects in which SomnoMed and Zephyr have provided
during sleep in obstructive sleep apnea. Sleep.
equipment, has research grants from Apnimed and Bayer
98. Azarbarzin A, Sands SA, Taranto-Montemurro L, et al.
Estimation of pharyngeal collapsibility during sleep by peak
and serves on the Scientific Advisory Board for Apnimed.
inspiratory airflow. Sleep. 2017;40(1). VL and JCC have no potential conflicts to declare.
99. Landry SA, Edwards BA, Hamilton GS, et al. Therapeutic CPAP
level predicts upper airway collapsibility in patients with
obstructive sleep apnea. Sleep. 2017;40(6).
Journal of Dental Sleep Medicine Vol. 6, No.2 2019You can also read

















































