Spinal Emergencies and Red Flags - ANP-BC, FAAPM, FAAN Jackie Rowles, MBA, CRNA Meridian Adult Health Indianapolis, IN
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Spinal
Emergencies
and Red
Flags
Jackie Rowles, MBA, CRNA
ANP-BC, FAAPM, FAAN
Meridian Adult Health
Indianapolis, IN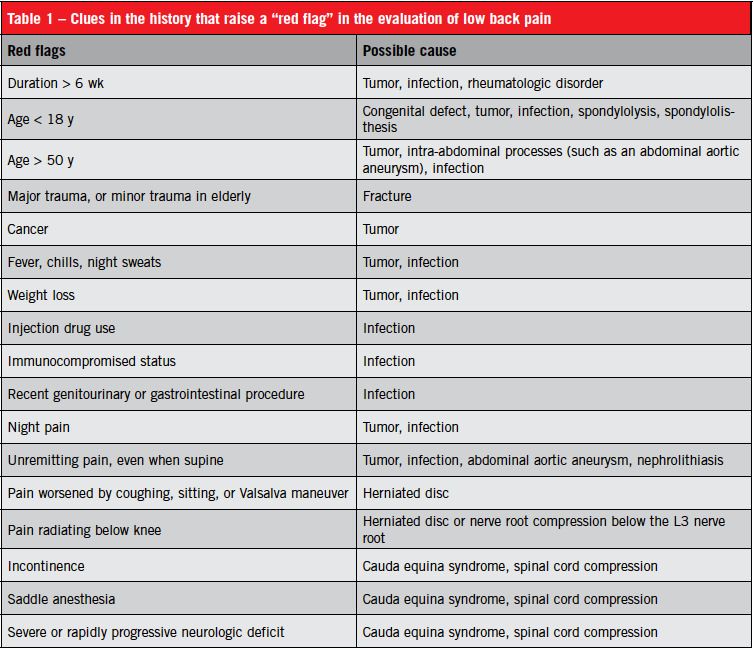
Acknowledgements: • A special thank you to Mindy Wallace and Paul Darr who have previously given this lecture at the JN workshop and who has shared materials for this lecture. And also to Mindy for the powerpoint design which fits this lecture perfectly!

Objectives: • Identify and describe common and uncommon medical disorders that may present with back or neck pain. • Identify pertinent history, physical, and diagnostic findings of serious medical conditions accompanied by pain. • Identify medical disorders that require immediate or urgent treatment.
Urgencies or Emergencies? • There are many, many urgencies but true emergencies only occur with spinal cord compression
And …………. Red Flags??? • Signs/Symptoms that are associated with severe or life threatening/altering spinal pathology
So, what exactly are spinal emergencies? • Cauda Equina syndrome • Trauma • Infection • Tumor
How do we avoid missing
something so important?
• By acquiring the necessary knowledge,
skills, and competencies needed to assess
and determine an appropriate diagnosis or
list of differential diagnoses!
• By not becoming too comfortable or
complacent with our routine
• By not accepting referrals at face value
• By keeping the focus, and the priority on the
patient and safe provision of careRequired actions • Obtain a thorough history • Perform a thorough physical exam • In depth review medical records • Ask more questions • Perform additional assessment • Order appropriate labs and imaging • Know Differential Diagnoses! • Listen to the patient/family • Listen to your inner voice
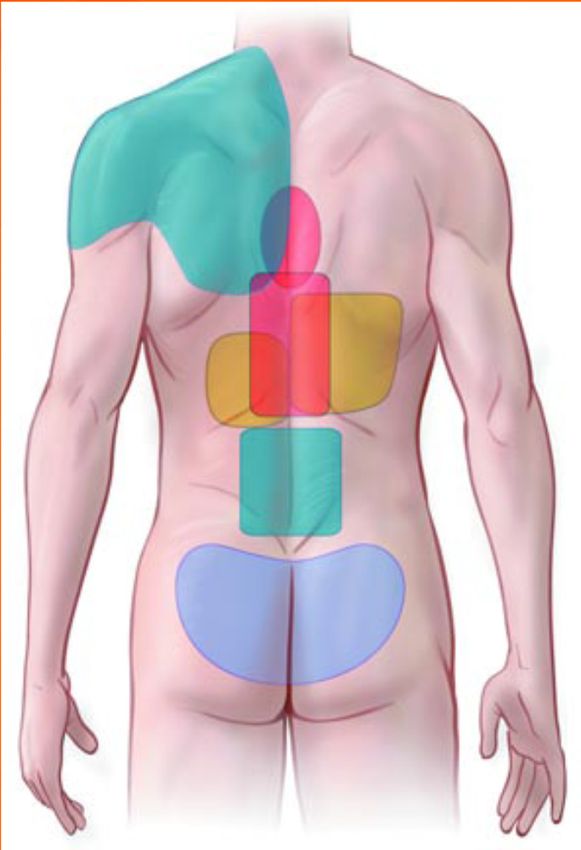
Referred Back Pain patterns:
Cardiac ischemia
(common)
Cardiac ischemia
Dissecting abdominal (atypical)
aortic aneurysm, visceral
injury Cholelithiasis,
peptic ulcer disease,
Pyelonephritis, pancreatitis
renal stones
Deep-seated pelvic pain Classic low back pain,
PID Lumbar spondylosis
Ectopic pregnancy
Fibroids Activity-related, persistent
Endometriosis Severe, tearing
Prostatitis Colicky
Tumors Cramping, spasmodic,
Masquerade: Medical causes of back pain: REVIEW ERIC KLINEBERG, MD, abdominal
DANIEL MAZANEC, MD, DOUGLAS ORR, MD, CLEVELAND CLINIC
JOURNAL OF MEDICINE . VOL. 74, 12:2007, pp 905-913.Visceral pathology pain patterns (googlesearch.com)
Most Common Causes of Neck & Back Pain: • 70% due to: muscle strain, ligament sprain, myospasm, or combination without anatomic abnormality • Only about 25% involve specific structural lesions that clearly cause the symptoms, primarily: – Disk herniation – Disc or facet degeneration – Compression fracture (trauma or osteoporosis) – Lumbar spinal stenosis – Osteoarthritis – Spondylolisthesis
Serious Spinal Disorders: • Infections – discitis, epidural abscess, osteomyelitis • Primary tumors of spinal cord or vertebrae • Metastatic vertebral tumors – most often from breasts, lungs, or prostate • Spinal cord or nerve root compression may result from: – tumors – epidural abscess – hematoma. – mechanical spine disorders
Serious Extraspinal Disorders:
Emergent Conditions Serious Conditions
• Dissecting arterial aneurysm • Cholecystolithiasis
• Ectopic pregnancy • Pancreatitis/ appendicitis
• Myocardial infarction
• Salpingitis/ pelvic inflammatory
• Cardiac tamponade disease
• Acute meningitis
• Nephrolithiasis
• Carotid or vertebral artery
dissection • Prostatitis
• Ovarian cancer
• Pleuritis/ pneumonia
Urgent Conditions
• Acute pancreatitis
• Duodenal ulcers
• Pyelonephritis
• Visceral trauma
• Acute meningitisOther Less Common Causes:
•Herpes zoster •TMJ syndrome
•Paget's disease •Thoracic outlet syndrome
•Torticollis
•Rheumatoid Disorders •Spondyloarthropathies
•Polymyalgia rheumatica •Ankylosing spondylitis
•Psoriatic arthritis •Bechet’s syndrome
•Enteropathic arthritis •Whipple’s disease
•Reactive arthritis •Diffuse idiopathic skeletal
hyperostosis
•Undifferentiated
spondyloarthropathyWhat to be aware of • Age, 50 • Cancer history (no matter when!) • Unexplained weight loss • Long term use of steroids • Recent report of serious illness • Recent report serious infection
Cancer signs: MUST know! • Bowel or bladder habits changed • Sores that won’t heal • Unusual bleeding/discharge • Breast lump or thickening • Steady nausea, indigestion, dysphagia • Change in wart/mole • Nagging cough/hoarseness
Weight loss • Without explanation • More than 5% in one month • Always considered to be cancer until proven wrong
Response to previous therapy • Good initial response followed by relapse is always a cause for concern
Misc. things to note • Long term or high dose steroids • Appearance of systemic illness • Presence of bilateral pins and needles sensation • History of trauma, TB or osteoporosis • Smoking • Severe headache • S/S of cauda equina
Increased risk for infection – IV drug use – Severe – Immunosuppres constipation sion – Recent UTI – Recent surgery – Diabetes – Penetrating – HIV/AIDS trauma
Red Flags by History (S):
Back/Neck Pain with:
• Reported Progressive
• Thoracic pain
neurologic deficit
• Pain with sneeze, cough or
– Loss of sensation
valsalva
– Saddle anesthesia • Severe pain > 4-6 weeks
– Loss of power • Acute, tearing mid-back pain
– Urinary or bowel • Constant & Increasing Pain
incontinence • Constant, non-mechanical
– Urinary retention pain
• Excruciating pain
• Abdominal pain
• Nocturnal Pain DominantRed Flags by Assessment (O)
• Spinal deformity
• Severely limited ROM (tumor, osteoma)
• Myospasm with scoliosis or deformity
• Neurological deficit: myotome or
dermatomal abnormality; + Babinski
(plantar reflex) + Hoffmans and clonus
may equal upper motor neuron lesionRed Flags by Physical Exam
(O)
Observation Palpation
– Diaphoresis – Lymphadenopathy
– Cachexia – Costovertebral angle
– Skin erythema tenderness
– Fever – Abdominal aorta that
– Structural deformity is > 5 cm (particularly
if tender)
– Pain behavior – Localized abdominal
Testing tenderness
– Persisting severe restriction – Lower-extremity pulse
of forward trunk flexion deficits
– Spine tenderness to
percussion
– Meningismus
– Lhermitte’s signRed Flags by Physical Exam
(O):
Progressive Neurologic Deficits as
compared to earlier PE:
Sensory
Strength
– Loss of pain and temperature – Severe weakness in extremities
sensation in extremities or in myotomal pattern
– Loss of position, vibration sense – Muscle atrophy
(long tract signs) – Widespread or progressive loss
of strength in the legs
– Sensory deficits in dermatomal – Gait disturbance
pattern Reflexes
– Pain or deficits in “stocking – Hyperreflexia with clonus
glove” pattern – Hoffman’s reflex/ Babinski
– Saddle anesthesia – Asymmetric reflexes
– Loss of perianal/perineal
sensation
– Loss of bulbocavernous or anal
wink reflexesEstablishment of a Diagnosis (A) • Differential Diagnosis: systematically processing results of clinical information/test results to identify the appropriate diagnosis from a list of possible diagnoses.
Establishment of Treatment (P) • Definitive diagnosis or R/O • Appropriate treatment plan • Periodic evaluation • Plan modification as needed
What does the evidence say? • An 2009 article in Physiotherapy reported the results of obtained from a focus group results of 7 palliative care providers concerning the most common objective based red flags. • 3 responses were in strongest agreement
What does the evidence say about Red Flags? • 1. Trunk pain in a band-like distribution – Often proceeded by vague symptoms – Commonly bilateral in distribution – Related to bone or nerve root pathology
What does the evidence say
about Red Flags?
• 2. Vague and nonspecific LE symptoms
– Late in disease process
– Often predating overt spinal cord
compression
– Leg sensation “odd or strange” before
progressing to heaviness
– Reports that legs “misbehave”What does the evidence say
about Red Flags?
• 3. Reduced Mobility
– May present with mild foot drop
– May drag one leg
– Lack of recognition of these symptoms as
significant or important
– Greenbaugh,S and Selfe, J. Physiotherapy, 2009.What might I see?
Acute low back pain
• “A focused history taking is the most
critical tool for identifying risk factors for
serious disease in a patient who presents
with low back pain. Directing the history
taking toward the red flags allows for an
efficient, cost-effective assessment”
Della-Giustina, D. 2013Cauda Equina Syndrome
History (S)
• Saddle anesthesia
• Bladder dysfunction (distended bladder; loss of sensation when
passing urine)
• Fecal incontinence (loss of sensation of rectal fullness)
• Erectile dysfunction
Physical Examination (O)
• Perianal / perineal sensory loss
• Unexpected laxity of the anal sphincter
• Severe or progressive neurological deficit in the lower extremities
– Major motor weakness with knee extension, ankle eversion, or foot
dorsiflexion.
– Bilateral lower extremity weakness or numbnessCauda Equina Syndrome Causes (A) • Usually disc, spondylolisthesis, rarely tumor, abscess, advanced AS Diagnosis/Treatment (P) • Urgent MRI and surgical decompression
Cervical Myelopathy History (S) • Insidious progression of symptoms usually Physical Exam (O) • Gait disturbance; clumsy or weak hands; loss of sexual/bladder/bowel function • Lhermitte's sign (flexing the neck causes electric shock-like sensations that extend down the spine and shoot into the limbs) • Upper motor neuron signs UEs: Hoffman’s reflex • Upper motor neuron signs LEs: Upgoing toes/ babinski, hyperreflexia, clonus, spasticity) • Lower motor neuron signs in the upper limbs (atrophy, hyporeflexia)
Cervical Myleopathy • (A) amyotrophic lateral sclerosis, multiple sclerosis, syringomyelia, and spinal tumors. • (P) immobilization of the neck, steroids, NSAIDS, PT, surgery
Vascular Insufficiency
History
• Dizziness and blackouts (restriction of vertebral
artery) on movement, especially upward gaze
• Fainting or drop attacks
• Headaches
Physical Exam
• May be normal
• Claudication
• Pulse deficits
• Trophic changes (changes resulting from interruption of
nerve supply: wasting away of the skin, tissues, or
muscle, thinning of the bones, thickening or thinning of
hair or brittle nails)Abdominal Aortic Aneurysm History • Age greater than 60 years • Atherosclerotic vascular disease • Pain at rest or nocturnal pain Physical Exam • Abdominal pulsating mass
Visceral Problems • Renal • GU • Refer • GI quickly!! • Hepatic • GYN • Cardiopulmonary
Spinal Fractures History • Sudden onset of severe central pain, relieved by lying down • Recent significant trauma at any age – Ejection from motor vehicle – Fall from substantial height • Minor trauma, or even strenuous lifting, in people with osteoporosis • Prolonged use of Corticosteroids • Mild trauma over age 50 years • Age greater than 70 years Physical Exam • Structural deformity of the spine
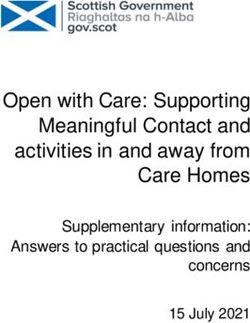
Compression Fractures
Cancer
History
• History of cancer
• Onset in a person over 50 years, or under 20 years, of age
• Constitutional symptoms, such as fever, chills, or unexplained
weight loss
• Recent bacterial infection (e.g. urinary tract infection)
• Intravenous drug abuse
• Immune suppression
• Pain that remains when supine
• Aching night-time pain disturbing sleep
• Thoracic pain (which also suggests aortic aneurysm)
• Failure to improve with therapy
• Pain persists for more than 4 to 6 weeks
Physical Exam
• Structural deformity of the spine
• Vague low back pain
• Nonmechanical back pain
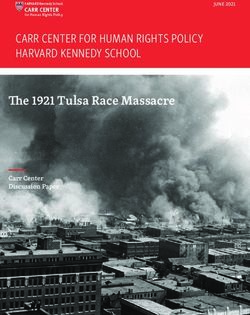
• Systemic symptomsCancer
• Metastatic / primary tumors such as multiple
myeloma more common than spinal infections /
inflammatory conditions
• 80% of patients with an underlying malignancy are
over age 50
• Predilection for vertebral body and pedicles
• Cancer associated with lumbar pain include:
– pancreas, duodenum, colon, uterus, cervix, and
ovaryCancer
Cancer
Infection
History
• History of intravenous Drug Abuse
• Recent bacterial infection
– Urinary Tract Infection or Pyelonephritis
– Cellulitis
– Pneumonia
• Immunocompromised states
– Systemic Corticosteroids
– Organ transplant
– Diabetes Mellitus
– Human Immunodeficiency Virus (HIV)
– Rest Pain
Physical Exam
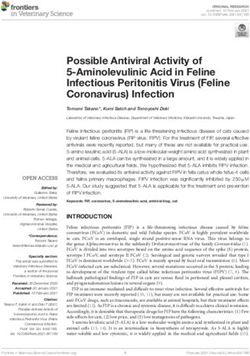
• Persistent fever (temperature over 100.4 F)Infection Facts • Discitis, osteomyelitis, and epidural abscess • Hematogenic spread • Post-op symptoms 2 to 4 weeks after surgery • One third have fever • 3% to 15% present with neurologic deficit • Infections typically involve intervertebral disc/ vertebral body endplate • Occur in about 1% of patients • More frequently in diabetics/ immunocompromised
Infection: Imaging Studies
• Radiographic changes at 2 to 4 weeks
• Bone scan positive as early as 2 days,
75% specific.
• MRI appearance is abnormal in infected
disc
• Enhancement after gadoliniumInfection
Infection
Ankylosing Spondylitis
History
•Morning stiffness and pain >30 mins -1
hr
•Better with activity
•Peripheral joint involvement
•Inflammatory bowel disease
•Recent GI or GU infection
•Family history of similar problems
•Gradual onset before the age of 40
yearsAnkylosing Spondylitis
Physical Exam
• Peripheral joint involvement
• Eye inflammation
• Psoriasis
• Colitis
• Decreased spinal range of motion in all
planesAnkylosing Spondylitis
Psychosocial Disorders History • Negative attitude that back pain is harmful or potentially severely disabling • Fear avoidance behavior and reduced activity levels • An expectation that passive, rather than active, treatment will be beneficial • A tendency to depression, low morale, and social withdrawal • Social or financial problems • Intolerance of treatments • Constant pain
Psychosocial Disorders Physical Findings • Superficial tenderness • Non-dermatomal numbness / sensory loss • Increased pain with axial loading /rotation distraction • Emotional and overt pain behaviors • SLR improves with distraction • Non-anatomical pain complaint
When do I send for Advanced Imaging? • Objective neurologic deficits • Potential surgical treatment • Signs of spinal stenosis • Pathological reflexes • Cervical myelopathy • Chest/Abdominal pain
And, what imaging type is indicated? • Plain films – fracture (AP, Lateral) • MRI – is the best visualization of lesions in the vertebral bodies, soft tissue, spinal canal, spinal cord, of disc disease • Emergent MRI for suspected spinal infection (vertebral osteomyelitis or epidural abscess) and epidural compression syndrome.
Type of imaging indicated: • MRI (routine or urgent) for evaluation of neoplastic spinal processes, disc disease or when the patient’s symptoms continue after 6 to 8 weeks • CT -- superior to MRI for evaluation of bony spine details. Best for evaluating vertebral fractures, facet joints, and the posterior spinal elements. of the spine..
Type of imaging indicated • CT myelogram -- best for spinal canal lesions, or if the patient cannot have an MRI. • If epidural compression or spinal infection is suspected, go directly to MRI as CT without myelography will not identify lesions inside the spinal canal
Labs • CBC, erythrocyte sedimentation rate (ESR), and UA for suspected infection or tumor. • WBC may be normal or elevated in patients with infection; ESR is almost always elevated in patients with osteomyelitis and epidural abscess.
Labs • C-reactive protein levels may be elevated in patients with acute infection, but they may not be elevated in those are severely immunocompromised. • ESR may be elevated in patients with neoplastic disease • UA to r/o UTI as infection source causing referred back pain. If WNL, order MRI to r/o infection or tumor
Take away thoughts Although serious extraspinal disorders (e.g., cancers, aortic aneurysms, epidural abscesses, osteomyelitis) are uncommon causes of back pain, they are not rare, particularly in high-risk groups.
Remember • Serious underlying pathology not common (around 3%) • Red flags should be explicitly sought • Cannot rely on referring practitioners to rule out these conditions
Pearls
• Most neck and back pain is caused by mechanical spinal disorders,
usually nonspecific, self-limited musculoskeletal derangements.
• Back pain is often multifactorial, making diagnosis difficult.
• Red flag findings often indicate a serious disorder and the need for
testing.
• Patients with segmental neurologic deficits suggesting spinal cord
compression require MRI or CT myelography as soon as possible.
• Normal spinal cord function during physical examination is best confirmed
by tests of sacral nerve function (eg, rectal tone, anal wink reflex,
bulbocavernosus reflex).
• Pain not worsened by movement is often extraspinal, particularly if no
vertebral or paravertebral tenderness is detected.
• Abdominal aortic aneurysm should be considered in any elderly patient
with low back pain, even if no physical findings suggest this diagnosis.
June 2008 by Sally Pullman-Mooar, MD, online Merck ManualEvidence Based Practice • http://www.cochrane.org • http://www.ahrq.gov • http://www.cebm.net • http://www.evidencebasedradiology.net • http://www.merck.com/mmpe/sec04/ch04 1/ch041a.html
References • Della-Giustina, D. Acute Low Back Pain: Recognizing the “Red Flags” in the Workup. Consultant. 2013;53(6):436- 440. • Greenbaugh, S., Selfe, J. Red Flags: A qualitative investigation of Red Flags for serious spinal pathology. Physiotherapy. 95, pp: 223-226. 2009
Thank
You!
Any Questions?You can also read