STRATEGIES AND TECHNIQUES FOR BTK INTERVENTIONS - LANFROI GRAZIANI M.D. SERVIZIO DI EMODINAMICA
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Strategies and Techniques
for BtK Interventions
Lanfroi Graziani M.D.
Servizio di Emodinamica
Istituto Clinico “Città di Brescia”
Istituto Clinico Sant’Anna, Brescia
An Overview: Specific Morphological
Differences
• Atherosclerotic lesions: asymmetric
plaque distribution and extension, with
focal-eccentric sub-intimal and medial
atheromasic degeneration (common in
Carotid and Iliac arteries, the only condition present
in the Coronary tree)
• Diabetic Macroangiopathy: symmetric
diffuse vessel wall thickening due to
connective degeneration and medial
(macrophages free !!) calcification (particularly
evident in BtK arteries)
Shanahan, Cary, Salisbury, Proudfoot, Weissberg, Edmonds. Circulation.1999;100:2168-2176
Morphological Differences in Collaterals Development
between Diabetics and Non-Diabetics
DIABETIC NON-DIABETICInterventions Strategies in CLI:
Differences between Diabetics and Non-
Diabetics
DIABETICS NON-DIABETICS
ILIAC OBSTRUCTIONS RARE COMMON
NEED OF ILIAC STENT RARE COMMON
CATHETER-BASED RARE FREQUENT
THROMBOLYSIS REQ.
BENEFIT OF TREATING NONE OR LOW HIGH
PROXIMAL LESIONS ONLY
PROFUNDA FEMORIS NEVER CRUCIAL FREQUENT BENEFIT
ANGIOPLASTY
DISTAL ALWAYS NECESSARY SELDOM NECESSARY
RECANALIZATION
RISK OF MAJOR VERY HIGH LOW
AMPUTATION
INFECTION AND COMMON INFREQUENT
NECROSIS… and for an improved strategy, a new
categorization was suggested…
Eur J Vasc Endovasc Surg 33, 453e460 (2007)
Vascular Involvement in Diabetic
Subjects with Ischemic Foot Ulcer:
A New Morphologic Categorization
of Disease Severity
L. Graziani, A. Silvestro, V. Bertone, E. Manara,
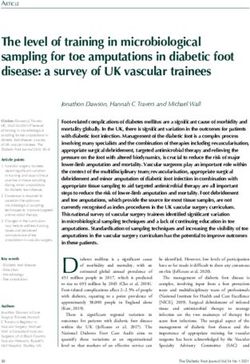
R. Andreini, A. Sigala, R. Mingardi, R. De GiglioTYPE AND DISTRIBUTION OF 2,893 LESIONS in 417
Consecutive Diabetics with CLI and Ischemic Foot Ulcer:
occlusions more common than stenoses !
Eur J Vasc Endovasc Surg 33, 453e460 (2007)
700
600
Stenoses
500
Occlusions
400
300
200
100
0
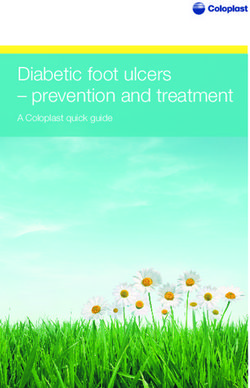
Iliac Fem oral Popliteal Peroneal Post.Tib. Ant.Tib.Arterial Involvement in 7 Classes of Progressive
Severity
63% of all cases !
1% 8% 14% 36% 11% 27% 1%
Graziani l. et al. Eur J Vasc Endovasc Surg 2007;33,453-460General Revascularization
Strategy in Diabetics with CLI
1. The best therapy for Limb Salvage in
diabetics with CLI is to give direct flow to
the foot. LoGerfo FW. et al.NEJM.1984;311:1615–19
2. Tibial Artery CTO recanalization is now
possible in more than 70% of cases Graziani L.,
unpublished data
3. Obtain a normally perfused isolated
Peroneal artery, may determine only limited
improvement of TcPo2 values (non-direct flow),
strictly depending on collaterals efficiency.
4. Alternative techniques (plantar arch crossing,
collaterals dilation) can represent a possible
option. Cardiovasc Intervent Radiol
2008;31(1),49-55Intervention Strategy, for CLI and BTK Lesions
1. Antegrade approach ! (>90% of cases)
2. Extensive use of Balloon Angioplasty
(P.O.B.A.)
3. Provisional Stenting in: Localized True Bifurcating
Lesion with Plaque Shifting, Persistent Recoil, Stenoses
Recurrence, non-Removable Thrombus, Obstructive and
localized Dissection
4. Elective Stenting in Stenosis of By-pass Graft
Anastomosis, ostial lesions, complex Stenoses &
Recurrences,
5. Self-Expandable Stents preferable in all cases
6. Avoid putting Stents in the middle Popliteal
and medium-distal Tibials.
7. No Stents in the Foot Arteries
8. Atherectomy for BTK in-Stent restenosis and
selected lesionsTips to Optimize the result of Balloon
Angioplasty
1. Prolonged balloon inflation (>180 sec)
2. Gradual high-pressure balloon
dilatation
3. Dilatation using a correct balloon size
Circulation 1989,Vol 80, 1029-1040; J Am Coll Cardiol. 1989
Apr;13(5):1094-100; Cathet Cardiovasc Diagn. 1993 Jul;29(3):199-202;
Circulation 1994,Vol 89, 1118-1125; Am J Cardiol. 1996 May 15;77(12):
1062-6; Z Kardiol. 1996 Apr;85(4): 273-80; Am Heart J. 1996
May;131(5):884-91; Am Heart J. 1998 Apr;135(4):709-13; J Vasc Interv
Radiol 2002, 13:355-359; J Vasc Interv Radiol 2002 Apr;13(4):361-9;The New Generation of Over-the-Wire and RX
Balloons for Tibial Artery Recanalization
Perfect
Transition
.014 GW
< 3Fr Small-Vessel
balloon tapered to .014Intraluminal Crossing using a .014 hydrophilic support wire
RESULT Invatec Amphirion Deep
Critical Limb Ischemia and foot lesions in a diabetic:
the effectiveness of P.O.B.A.RESULT
Ischemic ulcerated diabetic foot. Extensive occlusion of all leg and foot
arteries. Intraluminal balloon-angioplasty recanalization with direct flow in a
collateral foot branch: the importance of foot branchesRESULT
Minor branches can
represent the last
resource.
The best strategy is to
give direct flow to the
foot in any cases !Diabetic foot ulcer and gangrene. Diffuse occlusion of most femoral, popliteal
and leg arteries. The plantar artery arise from the peroneal but is stenosed
proximally: the importance of Extensive balloon Angioplasty and
femoral Stenting.… pain immediate ceased and a transmetatarsal amputation
was performed with limb salvage.
RESULThaving a foot artery normally perfused, at least, is
the best resource for wound healing
RESULTDiabetic necrotic foot lesions in a subject with extensive occlusion of leg arteries: POBA recanalization of Anterior tibial and Peroneal arteries
but the contribution of Peroneal Artery
recanalization is poor in most of cases…
RESULTCardiovasc Intervent Radiology
Volume 31, Number 1, pag 49-55, January, 2008
TRANSLUMINAL ANGIOPLASTY OF
PERONEAL ARTERY BRANCHES IN
DIABETICS: INITIAL TECHNICAL
EXPERIENCE
Lanfroi Graziani, Antonio Silvestro, Luca Monge,
Gian Mario Boffano, Francesco Kokaly, Ilaria
Casadidio, Francesco Giannini.
T IVE
R NA UE
L TE HNIQ
A C
TEThrough the Posterior Perforating Branch RESULT
Through the Posterior Perforating Branch
RESULT
balloon
wireAn emerging problem: the Ischemic Calcanear
Ulcer
• Difficult to manage
• High risk of osteomielitis
• P.T. frequently occluded
• Poor Peroneal artery
contribution
• Increased risk of major
amputationNon healing Calcanear Ulcer
T I VE
R NA UE
E
ALT CHNIQ
TE
Invatec
Amphirion DeepRESULT
RETROGRADE
R
T I
NA UE
VE CATHETERIZATION
E
ALT CHNIQ OF THE PEDAL
TE
ARTERY:
19G needle & 4Fr introducer
< 1% of our procedures !Dedicated Self- Expandable Stents: A new Device for Recurrences…
nytinol tibial Stent
RESULT…and Complex Lesions
nytinol tibial Stent
RESULTComplications in Extreme Vascular
Interventions
(SINGLE CENTER EXPERIENCE: Istituto Clinico Città di Brescia, L. Graziani, non published data)
• Minor (no surgery or transfusion req.) : 6%
• Major : 2%
• Mortality : 0.2%
• Data referred to 1,500 consecutive procedures in diabetics
performed in a single Center (1998-2000)Our Results with 5-year follow-up in 993
Consecutive Diabetics with CLI & Foot Ulcer
Eur J Vasc Endovasc Surg. 2005;29:620-7
Peripheral Angioplasty as the First-choice
Revascularization Procedure in Diabetic Patients
with Critical Limb Ischemia: Prospective Study
of 993 Consecutive Patients Hospitalized and
Followed Between 1999 and 2003
E. FAGLIA, L. DALLA PAOLA, G. CLERICI, J. CLERISSI, L. GRAZIANI, M.
FUSARO, L. GABRIELLI, S. LOSA, A. STELLA, M. GARGIULO, M. MANTERO,
M. CAMINITI, S. NINKOVIC, V. CURCI and A. MORABITOResults:
Eur J Vasc Endovasc Surg. 2005;29:620-7
The Largest Prospective Multicentric Study : 5 year follow-up in 993 pts
• Intervention Feasibility: 83%
• Cumulative Major Amputation rate after Intervention: 1.8 -
4.0%
• Cumulative Major Amputation rate after By-Pass surgery:
(157 pts, 13.2%) 8.3%
• In 47 subjects not revascularized (5 anesthesiology risk, 4 patient
refusal, 38 not considered by the Vascular Surgeon as candidates for By-Pass
Surgery), Major Amputation: 34.0%
• Clinical recurrence rate: 12.5%, (7.1% per year)
• In 85.4% of clinical recurrences, a second Intervention was
successfully performed.
• 5 year Limb Salvage: 88%You can also read