Strategies to increase the demand for childhood vaccination in low- and middle-income countries: a systematic review and meta-analysis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Systematic reviews
Strategies to increase the demand for childhood vaccination in low-
and middle-income countries: a systematic review and meta-analysis
Mira Johri,a Myriam Cielo Pérez,b Catherine Arsenault,c Jitendar K Sharma,d Nitika Pant Pai,e Smriti Pahwaf &
Marie-Pierre Sylvestrea
Objective To investigate which strategies to increase demand for vaccination are effective in increasing child vaccine coverage in low- and
middle-income countries.
Methods We searched MEDLINE, EMBASE, Cochrane library, POPLINE, ECONLIT, CINAHL, LILACS, BDSP, Web of Science and Scopus databases
for relevant studies, published in English, French, German, Hindi, Portuguese and Spanish up to 25 March 2014. We included studies of
interventions intended to increase demand for routine childhood vaccination. Studies were eligible if conducted in low- and middle-income
countries and employing a randomized controlled trial, non-randomized controlled trial, controlled before-and-after or interrupted time
series design. We estimated risk of bias using Cochrane collaboration guidelines and performed random-effects meta-analysis.
Findings We identified 11 studies comprising four randomized controlled trials, six cluster randomized controlled trials and one controlled
before-and-after study published in English between 1996 and 2013. Participants were generally parents of young children exposed to an
eligible intervention. Six studies demonstrated low risk of bias and five studies had moderate to high risk of bias. We conducted a pooled
analysis considering all 11 studies, with data from 11 512 participants. Demand-side interventions were associated with significantly higher
receipt of vaccines, relative risk (RR): 1.30, (95% confidence interval, CI: 1.17–1.44). Subgroup analyses also demonstrated significant effects
of seven education and knowledge translation studies, RR: 1.40 (95% CI: 1.20–1.63) and of four studies which used incentives, RR: 1.28
(95% CI: 1.12–1.45).
Conclusion Demand-side interventions lead to significant gains in child vaccination coverage in low- and middle-income countries.
Educational approaches and use of incentives were both effective strategies.
articles published up to 2009.9 In the interim, several new stud-
Introduction ies of potentially higher quality have been published.
Almost 40 years after the launch of the World Health Organiza- We carried out a systematic review and meta-analysis to
tion’s (WHO’s) Expanded Programme on Immunization, one evaluate whether demand-side interventions increase uptake
in five children worldwide still does not have access to basic of routine childhood vaccination in low- and middle-income
vaccines.1,2 In May 2012, the World Health Assembly approved countries. Our objectives were to ascertain the effect of de-
the Global Vaccine Action Plan to ensure that the full ben- mand-side interventions on vaccine coverage and to identify
efits of immunization are extended to people in every region, which strategies are effective. We focused on demand-side
country and community.1 Midway through the Global Vaccine interventions, since these strategies can more easily reach
Action Plan’s decade of vaccines (2011–2020)1, disparities in underserved populations and reduce inequities in immuniza-
vaccine coverage within and between countries persist,3 and tion coverage.
the search for effective strategies to reach underserved popula-
tions has gained urgency. Methods
Interventions to improve vaccination outcomes are com-
Protocol and registration
monly grouped into those targeting health services delivery
or supply (e.g. improving human resources training, logistics, The review protocol was registered in the PROSPERO database
cold chain maintenance and vaccine storage, effective financing, (CRD42013005783; available at: http://www.crd.york.ac.uk/
monitoring and evaluation and supportive supervision) and PROSPERO/display_record.asp?ID=CRD42013005783). The
those that stimulate demand for vaccines (e.g. monetary or food full report, available from the authors, includes both a narra-
incentives, knowledge transfer or communication campaigns). tive synthesis and a meta-analysis as outlined in the protocol.
Certain demand-side interventions have been associated with
Eligibility criteria
improved vaccine coverage of children in low- and middle-
income countries in previous systematic reviews.4–9 However, We defined six criteria for inclusion of studies in the review
limitations in study quality and design precluded quantitative and meta-analysis: (i) based on guidelines developed by
synthesis in these reviews. The most recent review considered the Cochrane Effective Practice and Organisation of Care
a
Centre de Recherche du Centre Hospitalier de l’Université de Montréal (CRCHUM), Tour Saint-Antoine, Porte S03-458, 850 rue St-Denis, Montréal, Québec, H2X 0A9,
Canada.
b
Département d’administration de la santé, Université de Montréal, Montréal, Canada.
c
Department of Epidemiology, Biostatistics and Occupational Health, McGill University, Montréal, Canada.
d
National Health Systems Resource Centre (NHSRC), Ministry of Health and Family Welfare, New Delhi, India.
e
Department of Medicine, McGill University, Montréal, Canada.
f
Pratham Education Foundation (ASER Centre), New Delhi, India.
Correspondence to Mira Johri (email: mira.johri@umontreal.ca).
(Submitted: 8 September 2014 – Revised version received: 5 December 2014 – Accepted: 23 January 2015 – Published online: 23 March 2015 )
Bull World Health Organ 2015;93:339–346C | doi: http://dx.doi.org/10.2471/BLT.14.146951 339Systematic reviews
Childhood vaccination in low- and middle-income countries Mira Johri et al.
(EPOC) group, randomized controlled author translated the strategy and terms
with more precise estimates. Study-
trial, non-randomized controlled trial, for the databases in other languages.
specific estimates of variance were
controlled before-after or interrupted Identified records were uploaded into
obtained by deriving standard errors
time series study designs were eligible;10 EndNote (Thomson Reuters, Philadel-
from the confidence intervals reported
(ii) the study location was a low- and phia, United States of America) and
by the studies. For cluster randomized
middle-income country as defined by duplicates eliminated. Two authors
controlled trials, we used the standard
the World Bank;11 (iii) the study was screened titles and abstracts indepen-
errors with adjustment for clustering,
published in a peer-reviewed scientific dently and eliminated studies that failed
which allowed us to use both clustered
journal, because in previous reviews to meet eligibility criteria. Full texts of
and non-clustered randomized controls
that considered the grey literature, the remaining studies were retrieved. Two
trials in the same meta-analyses. In
quality of these studies was found to authors independently screened full
addition to conducting meta-analysis
be low; 4–7 (iv) the participants were text articles against study inclusion
on all included studies, we performed
generally parents and caregivers of criteria and compared results; another
meta-analysis on five pre-specified sub-
children younger than two years, living author validated all decisions.
groups: (i) studies including the third
in communities where interventions
Data extraction dose of diphtheria-tetanus-pertussis
to increase demand for routine child-
(DTP3); (ii) studies using knowledge
hood vaccination had been carried out; From each study, two authors indepen-
transfer interventions; (iii) studies us-
(v) eligible interventions were defined dently extracted data on study design,
ing incentives, (iv) studies whose risk
broadly as any intervention that might aims, location, population, intervention,
of bias was assessed to be moderate-
increase demand for routine child- follow-up period and outcomes, using
to-high; and (v) studies whose risk of
hood vaccination, such as incentives a pre-defined template (available from
bias was assessed to be low. We also
of money or food, knowledge transfer corresponding author). We adopted the
estimated three meta-regression models
initiatives, or communication cam- original study definitions of comparator
adjusting separately for: (i) baseline
paigns (studies that included strategies or control groups. We pilot tested the
vaccination coverage (the proportion
targeting vaccine supply in addition template on a subset of studies. In ad-
of children aged 12–23 months receiv-
to demand were eligible); and (vi) the dition to vaccine outcomes, information
ing DTP3 in the study area or country);
study outcomes included quantitative on equity and economic outcomes were
(ii) intervention type; and (iii) study
estimates of routine childhood vaccina- extracted. Together, three authors cross-
quality. Heterogeneity was assessed us-
tion coverage. checked and verified these data. Study
ing Cochrane’s Q-test and I2 statistics.12
authors were contacted for clarification
Information sources Potential publication bias was assessed
if data were missing or unclear.
using funnel plots. Analyses were per-
We searched the MEDLINE (via
Risk of bias formed using the metafor package13 for
Pubmed), EMBASE, Cochrane library,
meta-analyses in R (R Foundation for
POPLINE, ECONLIT, CINAHL, LI- We used Cochrane collaboration criteria
Statistical Computing, Vienna, Austria)
LACS (Latin America and the Caribbean to assess risk of bias.12 As these criteria
and the heterogi package 14 for Stata
Center on Health Sciences Information), were developed to assess randomized
(version 13.1, StataCorp LP, College
BDSP (French public health database), controlled trials, we supplemented
Station, USA).
Web of Science and Scopus databases them to accommodate additional study
using appropriate terms and descrip- designs. To address issues specific to
tors. Searches were limited to articles cluster randomized controlled trials, we Results
concerning human data that were writ- systematically considered recruitment
Study selection
ten in English, French, German, Hindi, bias, unit of analysis bias and sample
Portuguese or Spanish. The search began size as part of the “other” category.12 To Search of the databases yielded 1705
on 1 September 2008 and was last up- accommodate non-randomized designs, citations. We also identified 59 records
dated on 25 March 2014. All published we used the Cochrane EPOC group’s through previous systematic reviews,
studies included in previous systematic additional criteria and scoring for non- article bibliographies and subject-matter
reviews4–9 were also considered. We con- randomized controlled trials, controlled experts. After removal of 643 duplicate
sulted experts and reviewed article refer- before-and-after and interrupted time- records, there were 1121 records for title
ence lists for additional articles. series studies.10 For each included study, and abstract screening. Of these, 1073
two authors independently assessed did not meet eligibility criteria and were
Search and selection
risk of bias and compared results, and excluded. The full text of the remaining
One of the authors and an academic another author validated all decisions. 48 articles was retrieved for detailed
librarian defined the MEDLINE search review (available from corresponding
Statistical analysis
strategy (available from corresponding author). It lists the 37 articles excluded af-
author). Search terms were combina- The principal measure was the rela- ter full-text evaluation and the principal
tions of “interventions”, “programs”, tive risk (RR) of vaccination among reasons for their exclusion. A total of 11
“approaches”, “subsidies”, “knowledge children in intervention versus control studies15–25 comprising four randomized
translation”, “vouchers”, “vaccination”, groups. We performed a meta-analysis controlled trials, six cluster randomized
“immunization”, “vaccines”, “child”, by estimating random effect models controlled trials and one controlled
“infant”, “newborn”, “kid”, and “low- with inverse variance weighting. This before-and-after study were included in
and middle-income countries”. The method gives greater weight to studies the review (Fig. 1 and Table 1).
340 Bull World Health Organ 2015;93:339–346C| doi: http://dx.doi.org/10.2471/BLT.14.146951Systematic reviews
Mira Johri et al. Childhood vaccination in low- and middle-income countries
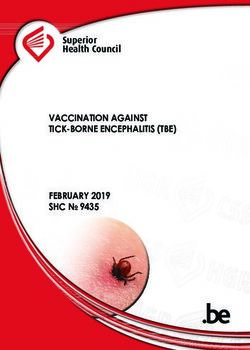
Study characteristics Fig. 1. Interventions to increase the demand for childhood vaccination: selection of
Study inclusion studies
The 11 studies were published in Eng-
lish between 1996 and 2013; eight were 1705 records identified through database searching:
from lower-middle income countries15–22 • 368 in Medline (56 with keywords)
and three were from low-income coun- • 95 in CINAHL
• 390 in PUBMED 59 additional records identified through
tries. 23–25 Study locations included • 99 in LILACS other sources:
south Asia (n = 7), 15–20,23 sub-Saharan • 202 in ECONLIT • 18 from experts
Africa (n = 3),22,24,25 and central America • 304 in POPLINE • 20 from previous reviews
(n = 1).21 • 111 EMBASE • 21 from reference lists
• 53 in BDSP
Participants • 83 in Cochrane Library
1073 excluded after screening
Data were collected from 11 512 par- titles and abstracts:
ticipants yielding outcomes for 11 512 • not an intervention study
children. As many interventions were 1764 records screened • not a primary study
directed to communities or populations • not in a low- or middle-income country
• not about routine childhood
rather than to individuals, the number of immunization
individuals reached by the interventions 1121 records after duplicates removed • not a demand-side intervention
was considerably larger. Participants • not an intervention to increase
were mothers, caregivers, households of vaccination uptake
children who were within the target age-
48 full-text articles assessed for eligibility
group for immunization (n = 9),15–18,21–25 37 full-text articles excluded:
or the general populations of target • 10 supply-side interventions
communities (n = 2).19,20 • 8 no control group
11 studies included in the systematic • 5 not about routine childhood
Interventions review and meta-analysis: immunization
• 7 education or knowledge translation • 5 immunization campaigns
Of the 11 studies, seven described educa- interventions • 3 not an intervention study
tion or knowledge translation interventi • 4 incentive interventions • 2 study design does not satisfy EPOC
criteria for admissibility
ons, 15–17,19,20,22,23 while four described
• 2 duplicate
interventions using incentives.18,21,24,25 • 1 no quantitative evidence on coverage
Of the latter, two considered monetary • 1 outcome data unavailable
incentives,21,24 and two non-monetary
incentives.18,25 One study compared two EPOC: Effective Practice and Organisation of Care.
types of monetary incentives;24 thus, the CINAHL: Cumulative Index to Nursing and Allied Health Literature
11 studies yielded data on 12 interven- PubMed: Public MEDLINE
LILACS: Latin-American and Caribbean Center on Health Sciences Information
tions. Four studies considered both ECONLIT: The American Economic Association’s electronic bibliography
demand and supply interventions to im- POPLINE: Free resource from the John Hopkins Bloomberg School of Public Health
prove vaccine coverage.16–18,21 For these EMBASE: Elsevier’s biomedical database
studies, meta-analyses were based on BDSP : Banque de Données en Santé Publique
the estimated demand-side effect.16–18,21
Outcomes
age-appropriate vaccination.25 The tim- but only two provided stratified analyses
Nine studies undertook coverage sur- ing of outcome measures was variable. related to subgroups of interest.17,20
veys to assess outcomes, 15,18–25 while While some studies addressed on-time
Risk of bias
two used administrative data.16,17 For delivery, a majority focused on the
six studies, the main aim of the inter- simpler assessment of presence or ab- We assessed risk of bias for nine cri-
vention was to increase immunization sence of vaccinations within a specified teria. Our assessments ranged from
coverage,15–19,22 while for five studies, period. This period was based on the low risk of bias on all criteria in one
improving immunization coverage was age of the child at the time outcomes study 18 to high risk of bias on five cri-
a secondary aim and data on immuni- were assessed and varied between stud- teria in one study. 25 For the purpose of
zation outcomes were included.20,21,23–25 ies: less than one year,15–17,20,25 less than subgroup analyses, we classified five
two years,19,22 less than three years,18,21 or studies with high risk of bias on one
Vaccination outcomes
less than five years.23,24 or more criteria as moderate-to-high
Four studies described full immuniza- One study recorded changes in im- risk of bias.20,21,23–25 The remaining six
tion as defined by the country’s immu- munization knowledge, attitudes and studies were categorised as low risk of
nization schedule, all of which contain beliefs19 and two estimated intervention bias. 15–19,22 Fig. 2 presents a summary
DTP3 as a subset. 18,22–24 Six studies costs and cost–effectiveness,18,19 as ad- of our assessment of the risk of bias
presented information on DTP3 vacci- ditional vaccination-related outcomes. (a detailed assessment for each study
nation.15–17,22–24 Three studies presented All studies considered equity in the and criterion, and figure summarizing
information on receipt of one or more choice of target populations by directing risk of bias assessments by criterion is
vaccine doses18,20,21 and one considered interventions to areas of greater need, available from corresponding author)
Bull World Health Organ 2015;93:339–346C| doi: http://dx.doi.org/10.2471/BLT.14.146951 341Systematic reviews
Childhood vaccination in low- and middle-income countries Mira Johri et al.
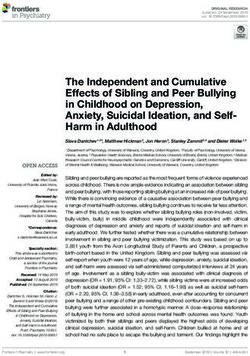
Fig. 2. Interventions to increase the demand for childhood vaccination: summary of the risk of study bias
Andersson Banerjee Briere Brugha Morris Owais Pandey Robertson Roy Usman Usman
2009 2010 2012 1996 2004 2011 2007 2013 2008 2009 2011
Random sequence generation
(selection bias)
Allocation concealment
(selection bias)
Blinding
(performance bias and detection bias)
Incomplete outcome data
(attrition bias)
Adequately protected
against contamination
Selective reporting
(reporting bias)
Baseline
charateristics similar
Baseline outcome
measurements similar
Other bias
High risk of bias Unclear risk of bias Low risk of bias
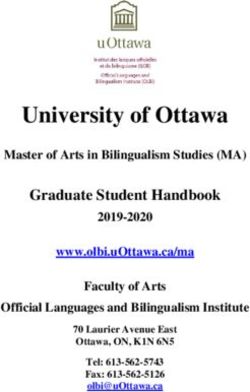
High risk of bias occurred most fre- receipt of vaccines (RR: 1.30; 95% CI:
Subgroup analyses
quently for the category “other bias” 1.17–1.44), but there was consider-
(five studies), while unclear risk of able heterogeneity (I2 = 88.96; 95% CI: The overall effect of educational or
bias was most frequent for the category 82.94– 92.16). Unweighted results were knowledge translation interventions was
“selective reporting” (nine studies). similar to weighted results (RR: 1.34; greater than for incentives RR: 1.40 (95%
Risk of bias was related to intervention 95% CI: 1.21−1.50). To reduce diversity CI: 1.20–1.63) versus RR: 1.28 (95% CI:
type: three of the four studies that used associated with outcomes measured, 1.12–1.45), respectively (available from
incentives had moderate-to-high risk we considered only the nine studies corresponding author). The pooled
of bias.21,24,25 reporting data for DTP3 or full vac- analysis considering studies with a low
cination (information available from risk of bias yielded a higher estimate
Receipt of vaccine
corresponding authors). These results of overall effect than that for studies
RR estimates, 95% confidence intervals were similar to those for all studies (RR: with moderate-to-high risk of bias,
(CI) and weights for each individual 1.32; 95% CI: 1.15–1.51; I2 = 86.31; 95% RR: 1.53 (95% CI: 1.28−1.82) and RR:
study are shown in Fig. 3. For each study, CI: 75.31–91.11). 1.15 (95% CI: 1.02–1.30), respectively
the crude proportion of participants (available from corresponding author).
Bias across studies
with and without vaccination is shown Heterogeneity was lower for educational
separately for intervention and control To explore potential sources of heteroge- or knowledge translation interven-
groups. For one study, Morris et al.,21 neity, we plotted the observed outcome tions: I2 = 80.48, (95% CI: 53.90–88.88)
data necessary for meta-analysis were against the standard error for all meta- than for incentives I2 = 89.40, (95% CI:
not available in the text or from the analyses and meta-regressions. Visual 76.83–93.73). Heterogeneity was also
study author and were taken from a inspection of funnel plots revealed no lower for studies with low risk of bias:
published article.26 evidence of asymmetry (available from I2 = 79.16, (95% CI: 42.92−88.82) versus
In the pooled analysis consider- corresponding author); however, due to studies with moderate-to-high risk of
ing all 12 interventions assessed in the the small number of studies the test has bias: I2 = 90.26, (95% CI: 81.40–93.86).
11 studies (Fig. 3), interventions were low power and we cannot exclude the Meta-regression revealed no important
associated with significantly higher possibility of publication bias. differences in results by baseline cover-
342 Bull World Health Organ 2015;93:339–346C| doi: http://dx.doi.org/10.2471/BLT.14.146951Systematic reviews
Mira Johri et al. Childhood vaccination in low- and middle-income countries
Fig. 3. Interventions to increase the demand for childhood vaccination: meta-analysis of 11 studies
Children vaccinated/total
Author(s) and year Intervention Control Weights % RR (95% CI) RR (95% CI)
Brugha and Kevany, 1996 171/200 137/219 9.21 1.40 (1.23–1.59)
Morris et al., 2004 - - 10.38 1.07 (1.01–1.13)
Pandey et al., 2007 107/149 36/79 9.57 1.57 (1.41–1.75)
Roy et al., 2008 64/126 60/104 6.78 0.88 (0.69–1.12)
Andersson et al., 2009 283/535 103/422 3.94 2.17 (1.43–3.29)
Usman et al., 2009 – received education only 242/375 205/375 9.36 1.18 (1.05–1.33)
Banerjee et al., 2010 – intervention B vs A 148/382 68/379 6.55 2.16 (1.68–2.78)
Owais et al., 2011 129/179 92/178 6.22 1.39 (1.06–1.82)
Usman et al., 2011 228/376 149/378 8.04 1.50 (1.25–1.80)
Briere et al., 2012 1062/1607 382/723 10.10 1.25 (1.16–1.35)
Robertson et al., 2013 – unconditional cash transfer 393/517 253/360 9.92 1.08 (0.99–1.18)
Robertson et al., 2013 – conditional cash transfer 317/417 253/360 9.92 1.08 (0.99–1.18)
Total 100.00 1.30 (1.17–144)
0.61 1 1.65 4.48
Favours control Favours intervention
CI: confidence interval; RR: relative risk.
Note: Weights are from random-effects analysis.
age level. Results for meta-regressions challenges confronted the studies re- by international agencies to assess im-
by intervention type and study quality viewed: (i) increases in demand cannot munization coverage and was included
were consistent with the corresponding be effective if supply-side constraints in nine of the 11 papers reviewed.3 All
meta-analyses. limit provision of vaccines;21,25 (ii) if analyses consistently showed that de-
coverage rates are already very high, mand-side interventions are beneficial
there is limited scope to demonstrate in improving coverage. However, due
Discussion improvement;24,25 and (iii) vaccination to diversity in outcomes and the small
This meta-analysis demonstrates that rates can be affected by changes in ser- number of studies, we cannot evaluate
demand-side interventions lead to an vice delivery occurring independently of the effect of interventions for specific
increase in child vaccination coverage in the study. Among the studies reviewed, vaccines.
diverse low- and middle-income settings only one study did not show a gain as- Fourth, health gains depend not
and among communities with lagging sociated with the intervention: in this only on increased vaccine coverage
health and social indicators. Immuni- study, all experimental groups experi- but also on appropriate timing of vac-
zation programmes have often focused enced substantial but similar gains in cination. With one exception,25 studies
on strengthening vaccine supply. Our vaccination coverage.23 Another study offered little information on when doses
results show that policymakers who seek noted a likely background trend with were delivered.
to increase access to vaccines through a differential impact on experimental Fifth, despite contacting the au-
the routine immunization system should groups.25 Unfortunately, neither of these thors, we were not able to retrieve data
also consider demand-side strategies. studies collected data on health system for all studies and had to use approxi-
Educational or knowledge transla- trends that might affect immunization mate values for one study 21 based on
tion interventions were more effective delivery. Studies addressing vaccine and another publication.26
on average than interventions based on non-vaccine outcomes, including three Sixth, our analysis excluded inter-
incentives; however, both strategies were of the four incentive based studies21,24,25 ventions that focused exclusively on im-
effective. The highest estimates of effect may have faced challenges related to proving vaccine supply. However, from a
and lowest heterogeneity were found broad study scope or a lack of vaccine- policy point of view, how demand-side
among studies with low risk of bias. Risk specific expertise in study planning. In interventions interact with supply side
of bias was related to intervention type, addition, two studies of financial incen- constraints is also important. With one
with three of the four incentives studies tives21,24 were large-scale interventions exception,18 immunization system per-
having moderate-to-high risk of bias. and faced substantial implementation formance was not explicitly assessed by
Our analysis has six important challenges. these studies.
limitations. First, vaccination cover- Second, the systematic review and Our results indicate that future
age is shaped by interrelated supply meta-analysis included only 11 stud- research on demand-side interven-
and demand factors. Many studies, ies. This limited our ability to explore tions to increase vaccine coverage
particularly those tackling vaccine and potential sources of heterogeneity quan- should (i) standardize measurement
non-vaccine outcomes,20,21,23–25 did not titatively and to exclude possible biases of outcomes; (ii) include vaccination
give due consideration to the role of related to publication and study size. experts during the study design phase;
the health system in delivering vaccines Third, studies measured different and (iii) collect data on health system
during the study design phase leading to vaccines over different time periods. Re- characteristics that may affect vaccine
increased risk of bias. Three supply-side ceipt of DTP3 is the measure preferred delivery.
Bull World Health Organ 2015;93:339–346C| doi: http://dx.doi.org/10.2471/BLT.14.146951 343Systematic reviews
Childhood vaccination in low- and middle-income countries Mira Johri et al.
coverage related to financial constraints, interventions can be delivered effectively
Conclusion opportunity costs, knowledge and at scale and in the long term. ■
Demand-side interventions are effective prioritization. Future research should
in improving the uptake of childhood seek to refine our understanding of Acknowledgements
vaccines delivered through routine which approaches are most effective in We thank Diego Bassani, Hospital for
immunization services in low- and specific contexts. Studies investigating Sick Kids, Toronto, Canada.
middle-income countries. Our results the value of knowledge translation and
are more definitive than those of previ- incentives-based interventions offered Funding: The Canadian Institutes for
ous systematic reviews which employed in combination are also required. Stud- Health Research (299960) and the
narrative synthesis techniques.4–9 ies that simultaneously consider sup- Bill & Melinda Gates Foundation
Demand-side strategies to improve ply- and demand-side interventions (OPP1067851) funded this study.
vaccination coverage are important – and enable us to evaluate their relative
because they are inherently equity- effectiveness – are of particular interest. Competing interests: None declared.
oriented and address specific barriers to Finally, studies should consider whether
ملخص
:اسرتاتيجيات زيادة الطلب عىل متنيع األطفال يف البلدان املنخفضة الدخل واملتوسطة الدخل
مراجعة منهجية وحتليل تلوي
منشورة باللغة اإلنجليزية،ودراسة واحدة مضبطة ملا قبل وملا بعد الغرض استقصاء لتحديد االسرتاتيجيات الفعالة يف زيادة الطلب
كان املشاركون يف األغلب آبا ًء لصغار.2013 و1996 ما بني عىل التغطية بخدمات متنيع األطفال يف البلدان املنخفضة الدخل
أظهرت ست دراسات مستوى.األطفال املعرضني لتدخل مؤهل .واملتوسطة الدخل
وكان لدى مخس دراسات مستوى،منخفض من اختطار التحيز EMBASE وMEDLINE الطريقة بحثنا يف قواعد معطيات
ً أجرينا حتلي.متوسط إىل مرتفع من اختطار التحيز
ال جتميعي ًا مع وECONLIT وPOPLINE وCochrane ومكتبة
مع بيانات من،األخذ يف االعتبار مجيع الدراسات اإلحدى عرش Scopus وويب العلوم وBDSP وLILACS وCINAHL
ارتبطت التدخالت من جانب الطلب بارتفاع. مشارك ًا11512 منشورة باللغة اإلنجليزية والفرنسية،عن دراسات ذات صلة
؛ (بنسبة1.30 : االختطار النسبي،تلقي اللقاحات بشكل ملحوظ .2014 مارس25 حتى،واألسبانية والربتغالية واألملانية واهلندية
كام أظهرت حتليالت.)1.44 إىل1.17 :95% أرجحية مقدارها ضممنا دراسات التدخل التي هتدف إىل زيادة الطلب عىل متنيع
املجموعات الفرعية آثار ًا ملحوظة لسبع دراسات ترمجة تعليمية تصبح الدراسات مؤهلة يف حالة إجرائها.األطفال الروتيني
:95% (بنسبة أرجحية مقدارها1.40 : االختطار النسبي،ومعرفية وإذا اعتمدت،يف البلدان املنخفضة الدخل واملتوسطة الدخل
االختطار،) وألربع دراسات استخدمت احلوافز1.63 إىل1.20 أو جتربة غري معشاة مضبطة،عىل جتربة معشاة مضبطة بالشواهد
.)1.45 إىل1.12 :95% (بنسبة أرجحية مقدارها1.28 :النسبي أو تصميم سالسل، أو جتربة مضبطة ملا قبل وملا بعد،بالشواهد
االستنتاج أدت التدخالت من جانب الطلب إىل مكاسب ملحوظة قمنا بتقدير اختطار التحيز باستخدام الدالئل.متقطعةِّ زمنية
يف جمال التغطية بخدمات متنيع األطفال يف البلدان املنخفضة الدخل ً وأجرينا حتلي،Cochrane اإلرشادية التعاونية ملكتبة
ال تلوي ًا
كانت كل من األساليب التعليمية واستخدام.واملتوسطة الدخل .لآلثار العشوائية
.احلوافز اسرتاتيجيات فعالة دراسة تتألف من أربع جتارب معشاة مضبطة11 النتائج توصلنا إىل
، وست جتارب عنقودية معشاة مضبطة بالشواهد،بالشواهد
摘要
在中低收入水平的国家提高儿童接种疫苗需求的策略 : 系统评价和荟萃分析
目的 旨在调查何种增加疫苗接种需求的策略能够有效 倚风险 , 并且进行了随机荟萃分析。
提高中低收入水平国家中儿童接种疫苗的覆盖率。 结果 我们在 1996 年和 2013 年期间鉴定了 11 项英文
方法 我们搜索了美国联机医学文献分析和检索系统 版研究 , 其中包括四项随机对照试验、六项整群随机
(MEDLINE)、荷兰医学文摘数据库 (EMBASE)、考克兰 对照试验和一项前后对照研究。参与者一般为接受合
(Cochrane) 图书库、人口信息数据库 (POPLINE)、经济 格干预的幼儿的父母。六项研究的偏倚风险较低 , 而
学文献资料库 (ECONLIT)、护理学数据库 (CINAHL)、 五项研究具有中高级偏倚风险。我们针对从 11 512 名
拉丁美洲和加勒比健康科学文献库 (LILACS)、公共卫 参与者处获得数据的 11 项研究全面开展汇整分析。需
生数据库 (BDSP)、科学网 (Web of Science) 以及斯高帕 求方面的干预措施会大大提高疫苗接种率 , 相对风险
斯 (Scopus) 数据库 , 旨在查找以英语、法语、西班牙语、 (RR) 为 :1.30,(95% 置信区间 ,CI:1.17–1.44)。小群组分
葡萄牙语、德语和印地语出版的相关研究资料 , 这项 析也论证了七项教育和知识翻译研究的重要作用 ,RR
工作的时间将一直持续到 2014 年 3 月 25 日。我们囊 为 :1.40 (95% CI:1.20–1.63), 以及四项采用激励措施的
括了意在提高常规儿童接种疫苗需求的干预研究。如 研究的重要作用 ,RR 为 :1.28 (95% CI: 1.12–1.45)。
果研究是在中低收入水平的国家开展 , 并且开展时采 结论 需求方面的干预措施能够大大提高中低收入水平
用的方法为随机对照试验、非随机对照试验、前后对 的国家中儿童接种疫苗覆盖率的成果。教育方法和使
照或间断时间序列设计 , 则该研究符合条件。我们通 用激励措施都是有效的策略。
过科克伦协作网 (Cochrane collaboration) 指南评估了偏
344 Bull World Health Organ 2015;93:339–346C| doi: http://dx.doi.org/10.2471/BLT.14.146951Systematic reviews Mira Johri et al. Childhood vaccination in low- and middle-income countries Résumé Stratégies pour accroître la demande de vaccination des enfants dans les pays à revenu faible et intermédiaire : examen systématique et méta-analyse Objectif Déterminer, parmi les stratégies visant à accroître la demande une étude contrôlée avant et après, qui ont été publiées en anglais de vaccination, celles qui sont efficaces pour augmenter la couverture entre 1996 et 2013. Les participants étaient généralement les parents vaccinale des enfants dans les pays à revenu faible et intermédiaire. de jeunes enfants exposés à une intervention éligible. Six études Méthodes Nous avons recherché, dans les bases de données montraient un faible risque de biais et cinq études avaient un risque MEDLINE, EMBASE, de la bibliothèque Cochrane, POPLINE, ECONLIT, de biais moyen à élevé. Nous avons réalisé une analyse combinée en CINAHL, LILACS, BDSP, Web of Science et Scopus, des études à ce tenant compte des 11 études, avec des données provenant de 11 512 sujet, publiées en allemand, en anglais, en espagnol, en français, en participants. Les interventions axées sur la demande étaient associées hindi, et en portugais, jusqu’au 25 mars 2014. Nous avons inclus les à une administration de vaccins sensiblement plus élevée, risque relatif études relatives à des interventions visant à accroître la demande de (RR) : 1,30; intervalle de confiance de 95%, IC : 1,17-1,44). L’analyse de vaccination systématique des enfants. Les études étaient recevables si sous-groupes a également montré des effets importants pour sept elles avaient été menées dans des pays à revenu faible et intermédiaire études décrivant des interventions d’éducation ou d’application des et si elles étaient de type essai contrôlé randomisé, essai contrôlé non connaissances, RR : 1,40 (IC de 95% : 1,20–1,63) et pour quatre études randomisé, contrôle avant et après ou étude de séries temporelles décrivant le recours à des incitations, RR : 1,28 (IC de 95% : 1,12-1,45). interrompues. Nous avons estimé le risque de biais suivant les directives Conclusion Les interventions axées sur la demande entraînent des de la collaboration Cochrane et avons réalisé une méta-analyse à effets avantages notables pour la vaccination des enfants dans les pays à aléatoires. revenu faible et intermédiaire. Les démarches éducatives ainsi que Résultats Nous avons relevé 11 études, comprenant quatre essais le recours à des incitations étaient tous deux des stratégies efficaces. contrôlés randomisés, six essais contrôlés randomisés en grappes et Резюме Стратегии повышения спроса на вакцинацию детей в странах с низким и средним уровнем доходов: систематический обзор и метаанализ Цель Определить, какие стратегии для увеличения спроса на контро лируемых исс ле довани я, шес ть к лас терных вакцинацию оказываются эффективными и позволяют расширить рандомизированных контролируемых исследований и одно охват вакцинацией детей в странах с низким и средним уровнем исследование, контролируемое перед началом и после доходов. окончания. Участники этих исследований — это в основном Методы Был выполнен поиск исследований, опубликованных родители маленьких детей, в отношении которых применялась на английском, французском, испанском, португальском, оправданная интервенция. Шесть исследований показали немецком языках и хинди до 25 марта 2014 г., в базах данных низкий риск системной ошибки. Другие пять — умеренный и MEDLINE, EMBASE, Кокрановской библиотеки, POPLINE, ECONLIT, высокий риск системной ошибки. Был проведен объединенный CINAHL, LILACS, BDSP, Web of Science и Scopus. Поиск охватывал анализ с учетом всех 11 исследований, включающий данные 11 исследования интервенций, направленных на повышение спроса 512 участников. Интервенции, направленные на повышение на плановую вакцинацию детей. Отбирались исследования, спроса, были связаны со значительно более активным согласием которые проводились в странах с низким и средним уровнем на вакцинацию. Относительный риск (ОР) составил 1,30 (95 % доходов и включали рандомизированные контролируемые доверительный интервал, ДИ: 1,17–1,44). Анализ в подгруппах испытания, нерандомизированные контролируемые испытания, также продемонстрировал значительный эффект в семи испытания, контролируемые перед началом и после окончания, исследованиях, связанных с информированием и передачей и испытания методом прерванного временного ряда. Оценка знаний, ОР: 1,40 (95 % ДИ: 1,20–1,63), и в четырех исследованиях, риска системной ошибки осуществлялась согласно руководящим в которых использовались льготы, ОР: 1,28 (95 % ДИ: 1,12–1,45). принципам организации «Кокрановское сотрудничество». Вывод Интервенции, направленные на повышение спроса Кроме того, был проведен метаанализ по модели со случайными на вакцинацию, приводят к значительному расширению эффектами. охвата вакцинацией детей в странах с низким и средним Результаты Были выявлены 11 исследований, опубликованных уровнем доходов. Свою эффективность показали как стратегии на английском языке в 1996–2013 гг.: четыре рандомизированных информирования, так и использование льгот. Resumen Estrategias para incrementar la demanda de vacunación infantil en países de ingresos bajos y medios: una revisión sistemática y un metanálisis Objetivo Investigar qué estrategias para incrementar la demanda marzo de 2014. Se incluyeron estudios de intervenciones con el objetivo de vacunación son efectivas en el incremento de la cobertura de de incrementar la demanda de vacunación infantil sistemática. Los vacunación infantil en países de ingresos bajos y medios. estudios fueron elegibles si se realizaron en países de ingresos bajos y Métodos Se realizaron búsquedas en las bases de datos de MEDLINE, medios y utilizaron un diseño de ensayo controlado aleatorizado, ensayo EMBASE, Cochrane Library, POPLINE, ECONLIT, CINAHL, LILACS, BDSP, controlado no aleatorizado, controlado antes y después o de series Web of Science y Scopus para encontrar estudios pertinentes, publicados temporales interrumpidas. Se estimó un riesgo de sesgo mediante las en alemán, español, francés, hindi, inglés y portugués hasta el 25 de directrices de colaboración de Cochrane y se realizaron metanálisis de Bull World Health Organ 2015;93:339–346C| doi: http://dx.doi.org/10.2471/BLT.14.146951 345
Systematic reviews
Childhood vaccination in low- and middle-income countries Mira Johri et al.
efectos aleatorios. se relacionaron con una recepción de las vacunas significativamente
Resultados Se identificaron 11 estudios que abarcan cuatro ensayos superior, riesgo relativo (RR): 1,30, (intervalo de confianza, IC, del
controlados aleatorizados, seis ensayos controlados aleatorizados por 95%: 1,17–1,44). Los análisis de los subgrupos también demostraron
conglomerados y un estudio controlado antes y después, publicados efectos importantes de siete estudios de educación y traslación de
en inglés entre 1996 y 2013. En general, los participantes fueron conocimientos, RR: 1,40 (IC del 95%: 1,20–1,63) y de cuatro estudios
padres de niños pequeños expuestos a una intervención elegible. que utilizaron incentivos, RR: 1,28 (IC del 95%: 1,12–1,45).
Seis estudios demostraron un bajo riesgo de sesgo y cinco estudios Conclusión Las intervenciones que afectan a la demanda llevan a
presentaron un riesgo de sesgo entre moderado y elevado. Se realizó mejoras significativas en la cobertura de vacunación infantil en países de
un análisis agrupado teniendo en cuenta los 11 estudios, con datos ingresos bajos y medios. Los enfoques educativos y el uso de incentivos
de 11,512 participantes. Las intervenciones que afectan a la demanda fueron estrategias efectivas.
References
1. Decade of Vaccines Collaboration 2012. Global Vaccine Action Plan 16. Usman HR, Akhtar S, Habib F, Jehan I. Redesigned immunization card and
2011-2020. Geneva: World Health Organization; 2013. Available from: center-based education to reduce childhood immunization dropouts
http://www.who.int/iris/bitstream/10665/78141/1/9789241504980_eng. in urban Pakistan: a randomized controlled trial. Vaccine. 2009 Jan
pdf?ua=1 [cited 2015 March 3]. 14;27(3):467–72. doi: http://dx.doi.org/10.1016/j.vaccine.2008.10.048 PMID:
2. Narrowing the gaps to meet the goals. New York: United Nations Children’s 18996423
Fund; 2010. Available from: http://www.unicef.org/publications/files/ 17. Usman HR, Rahbar MH, Kristensen S, Vermund SH, Kirby RS, Habib F,
Narrowing_the_Gaps_to_Meet_the_Goals_090310_2a.pdf [cited 2015 et al. Randomized controlled trial to improve childhood immunization
Mar 23]. adherence in rural Pakistan: redesigned immunization card and maternal
3. Global immunization data. Geneva: World Health Organization; 2014. education. Trop Med Int Health. 2011 Mar;16(3):334–42. doi: http://dx.doi.
Available from: http://www.who.int/immunization/monitoring_ org/10.1111/j.1365-3156.2010.02698.x PMID: 21159080
surveillance/global_immunization_data.pdf [cited 2015 Mar 23]. 18. Banerjee AV, Duflo E, Glennerster R, Kothari D. Improving immunisation
4. Batt K, Fox-Rushby JA, Castillo-Riquelme M. The costs, effects and cost- coverage in rural India: clustered randomised controlled evaluation of
effectiveness of strategies to increase coverage of routine immunizations in immunisation campaigns with and without incentives. BMJ. 2010 May
low- and middle-income countries: systematic review of the grey literature. 17;340(1):c2220. doi: http://dx.doi.org/10.1136/bmj.c2220 PMID: 20478960
Bull World Health Organ. 2004 Sep;82(9):689–96. PMID: 15628207 19. Andersson N, Cockcroft A, Ansari NM, Omer K, Baloch M, Ho Foster A, et
5. Pegurri E, Fox-Rushby JA, Damian W. The effects and costs of expanding the al. Evidence-based discussion increases childhood vaccination uptake: a
coverage of immunisation services in low- and middle-income countries: randomised cluster controlled trial of knowledge translation in Pakistan.
a systematic literature review. Vaccine. 2005 Feb 18;23(13):1624–35. doi: BMC Int Health Hum Rights. 2009;9 Suppl 1:S8. doi: http://dx.doi.
http://dx.doi.org/10.1016/j.vaccine.2004.02.029 PMID: 15694515 org/10.1186/1472-698X-9-S1-S8 PMID: 19828066
6. Haines A, Sanders D, Lehmann U, Rowe AK, Lawn JE, Jan S, et al. Achieving 20. Pandey P, Sehgal AR, Riboud M, Levine D, Goyal M. Informing resource-
child survival goals: potential contribution of community health workers. poor populations and the delivery of entitled health and social services
Lancet. 2007 Jun 23;369(9579):2121–31. doi: http://dx.doi.org/10.1016/ in rural India: a cluster randomized controlled trial. JAMA. 2007 Oct
S0140-6736(07)60325-0 PMID: 17586307 24;298(16):1867–75. doi: http://dx.doi.org/10.1001/jama.298.16.1867 PMID:
7. Ryman TK, Dietz V, Cairns KL. Too little but not too late: results of a literature 17954538
review to improve routine immunization programs in low- and middle- 21. Morris SS, Flores R, Olinto P, Medina JM. Monetary incentives in primary
income countries. BMC Health Serv Res. 2008;8(1):134. doi: http://dx.doi. health care and effects on use and coverage of preventive health care
org/10.1186/1472-6963-8-134 PMID: 18570677 interventions in rural Honduras: cluster randomised trial. Lancet. 2004
8. Shea B, Andersson N, Henry D. Increasing the demand for childhood Dec 4-10;364(9450):2030–7. doi: http://dx.doi.org/10.1016/S0140-
vaccination in low- and middle-income countries: a systematic review. 6736(04)17515-6 PMID: 15582060
BMC Int Health Hum Rights. 2009;9 Suppl 1:S5. doi: http://dx.doi. 22. Brugha RF, Kevany JP. Maximizing immunization coverage through home
org/10.1186/1472-698X-9-S1-S5 PMID: 19828063 visits: a controlled trial in an urban area of Ghana. Bull World Health Organ.
9. Oyo-Ita A, Nwachukwu CE, Oringanje C, Meremikwu MM. Interventions 1996;74(5):517–24. PMID: 9002332
for improving coverage of child immunization in low- and middle-income 23. Roy SK, Bilkes F, Islam K, Ara G, Tanner P, Wosk I, et al. Impact of pilot project
countries. Cochrane Database Syst Rev. 2011; (7):CD008145. PMID: of Rural Maintenance Programme (RMP) on destitute women: CARE,
21735423 Bangladesh. Food Nutr Bull. 2008 Mar;29(1):67–75. PMID: 18510207
10. Effective Practice and Organisation of Care (EPOC). What study designs 24. Robertson L, Mushati P, Eaton JW, Dumba L, Mavise G, Makoni J, et al.
should be included in an EPOC review and what should they be called? Effects of unconditional and conditional cash transfers on child health
EPOC Resources for review authors. Oslo: Norwegian Knowledge Centre for and development in Zimbabwe: a cluster-randomised trial. Lancet.
the Health Services; 2015. Available from: http://epoc.cochrane.org/epoc- 2013 Apr 13;381(9874):1283–92. doi: http://dx.doi.org/10.1016/S0140-
specific-resources-review-authors [cited 2015 Mar 23]. 6736(12)62168-0 PMID: 23453283
11. Country and lending groups. Data & statistics: country classification. 25. Briere EC, Ryman TK, Cartwright E, Russo ET, Wannemuehler KA, Nygren
Washington: The World Bank; 2013. BL, et al. Impact of integration of hygiene kit distribution with routine
12. Higgins JPT, Green S, editors. Cochrane handbook for systematic reviews immunizations on infant vaccine coverage and water treatment and
of interventions. Oxford: The Cochrane Collaboration; 2011. Available from: handwashing practices of Kenyan mothers. J Infect Dis. 2012 Mar;205 Suppl
http://handbook.cochrane.org/ [cited 2015 April 10]. 1:S56–64. doi: http://dx.doi.org/10.1093/infdis/jir779 PMID: 22315387
13. Viechtbauer W. Conducting meta-analyses in R with the metafor package. J 26. Bassani DG, Arora P, Wazny K, Gaffey MF, Lenters L, Bhutta ZA. Financial
Stat Softw. 2010;36:1–48. incentives and coverage of child health interventions: a systematic review
14. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat and meta-analysis. BMC Public Health. 2013;13 Suppl 3:S30. doi: http://
Med. 2002 Jun 15;21(11):1539–58. doi: http://dx.doi.org/10.1002/sim.1186 dx.doi.org/10.1186/1471-2458-13-S3-S30 PMID: 24564520
PMID: 12111919
15. Owais A, Hanif B, Siddiqui AR, Agha A, Zaidi AK. Does improving maternal
knowledge of vaccines impact infant immunization rates? A community-
based randomized-controlled trial in Karachi, Pakistan. BMC Public Health.
2011;11(1):239. doi: http://dx.doi.org/10.1186/1471-2458-11-239 PMID:
21496343
346 Bull World Health Organ 2015;93:339–346C| doi: http://dx.doi.org/10.2471/BLT.14.146951Table 1. Studies included in systematic review and meta-analysis of strategies to increase the demand for childhood vaccination in low- and middle-income countries
Study and year Site Study design Participants Intervention Control Vaccination Outcomes
Mira Johri et al.
Robertson et al., Zimbabwe, rural Cluster randomized 30 areas were matched on socioeconomic Unconditional cash transfer: every household No incentives Proportion of children
201324 areas controlled trial characteristics and randomized to three collected US$ 18 plus US$ 4 per child (up to a less than 5 years with
groups (10 UCT: 10 CCT: 10 control). maximum of three children) from designated up-to-date vaccinations
Households were eligible to participate if pay points every 2 months. (measles; BCG; polio;
they lived in a study area and met need- Conditional cash transfer: households and diphtheria–
based criteria. Vaccination outcomes consider received the same amount, but were tetanus–pertussis)
children aged 0–4 years in participating monitored for compliance with several
households (934 in the intervention arms conditions. Among others, children less than
(517 UCT; 417 CCT) and 360 controls). 5 years had to be vaccinated on time.
Briere et al., 201225 Kenya, largely Controlled before-and- Comparison between two adjacent districts. During routine immunization visits, caregivers Routine Children 2–13 months
rural after study Children aged 2–13 months were eligible; with a child aged < 12 months were offered immunization only with up-to-date
1607 children in the intervention arm and free hygiene kits (sodium hypochlorite immunization coverage
723 children in the control arm. solution for household water treatment, (3 doses of pentavalent
soap, pictorial educational materials) and vaccine at 6, 10 and
education about water treatment and hand 14 weeks and 1 dose
hygiene. of measles vaccine at
9 months)
Owais et al., 201115 Pakistan, urban Randomized controlled All mothers in five selected communities Short, home-based information sessions General health At four months after
and peri-urban trial with a child ≤ 6 weeks old were eligible to on importance of vaccines for low- promotion enrolment, children
communities participate; 179 children in the intervention literacy communities delivered by CHWs messages (including were defined as fully
near Karachi arm and 178 in the control arm. in 5 minutes. Pictorial cards conveyed information on immunized if they
Bull World Health Organ 2015;93:339–346C| doi: http://dx.doi.org/10.2471/BLT.14.146951
three messages: vaccines save children’s vaccines) delivered completed all three
lives; location of vaccination centres; and by CHWs in 10–15 doses of DTP3/Hepatitis
importance of retaining cards. minutes B; otherwise non-
immunized
Usman et al., 201117 Pakistan, rural Randomized controlled All children visiting six selected EPI centres Group 1: A redesigned immunization card in Mothers underwent DTP3 completed
area near trial for DTP1 were eligible, if mothers had lived in a plastic jacket, with a hanging string. routine EPI centre (received both DTP2 and
Karachi the area for at least 6 months. Mother–child Group 2: 2–3 minutes conversation with visits and received DTP3) versus DTP3 not
pairs were randomly allocated to 1 of 4 study mother during DPT1 visit to motivate and neither intervention completed
groups; 1 128 participants in the intervention convey the potential adverse impact of
arms (Group 1: 378; 2: 376; 3: 374) and 378 in incomplete immunization on the child’s
the control arm. health.
Group 3: Received both interventions.
Banerjee et al., India Cluster randomized Within each of 134 randomly selected Intervention A: A mobile team conducted No intervention; had Children under
201018 controlled trial villages, 30 households with a child 0–5 years monthly immunization camps in villages at access to standard 3 years who
of age were randomly selected. Children fixed dates and times to improve services. services received ≥ 1 vaccine
were included if they belonged to a selected In each village, a social worker performed dose or were fully
household and would be aged 1–3 years at outreach, linkage and educated mothers immunized;presence
the end of study (main sample) or were aged about immunization. of BCG scar, number of
0–6 months at baseline (baseline cohort). Intervention B: Intervention A plus 1 kg of immunizations, costs
761 children received interventions (A: 379; raw lentils per immunization and a set of and cost-effectiveness
B: 382); 860 children served as controls. metal plates for a child’s full immunization.
Childhood vaccination in low- and middle-income countries
Systematic reviews
346A
(continues. . .)(. . .continued)
346B
Study and year Site Study design Participants Intervention Control Vaccination Outcomes
Andersson et al., Pakistan, Lasbela Cluster randomized 32 EAs were randomly selected.18 EAs The intervention involved three structured Access to standard Proportions of children
200919 district controlled trial (3166 children < 5 years) in intervention discussions separately with male and female immunization 12–23 months receiving
group. 14 EAs (2475 children < 5 years) in groups in each village. Discussions shared services; both DTP3 and measles
control group. Vaccination outcomes reflect findings about local vaccine uptake; focused groups received vaccine;
Systematic reviews
a random sample of children aged 12–23 on the costs and benefits of childhood a district-wide knowledge, attitudes
months in each cluster (intervention: 535 vaccination; and focused on local action health promotion and norms about
children; control: 422 children). plans. Participants spread the dialogue in programme on vaccination; costs and
their communities. household hygiene cost-effectiveness
Usman et al., 200916 Pakistan, urban Randomized controlled All children visiting five selected EPI centres Group 1: A redesigned immunization card in Mothers underwent DTP3 completed
area in Karachi trial for DTP1 were eligible to participate, if a plastic jacket, with a hanging string. Group routine EPI centre (received both DTP2 and
mothers had lived in the area for at least 2: 2–3 minutes conversation with mother visits and received DTP3) versus DTP3 not
6 months. Mother–child pairs were randomly during DPT1 visit to motivate and convey neither intervention completed
allocated to 1 of 4 study groups; 1125 the potential adverse impact of incomplete
participants in the intervention arms (Group immunization on the child’s health.
1: 375; 2: 375; 3: 375) and 375 in the control Group 3: Received both interventions.
arm.
Childhood vaccination in low- and middle-income countries
Roy et al., 200823 Bangladesh, Randomized controlled 1275 poor women in 17 districts eligible The standard programme provided income Comparison group Percentages of children
rural trial for the rural maintenance programme support, employment and skill training. The received only 0–60 months receiving
were divided into three groups. Vaccination intervention group received basic nutrition standard programme; (by dose) DTP, measles,
outcomes concerned 340 children 0–60 and health education (including child control group BCG, OPV that were
months (intervention: 126, control: 104, immunization). received neither partially vaccinated or
comparison group 110). programme nor fully vaccinated
education
Pandey et al., 200720 India, Uttar Cluster randomized From 21 districts, 105 villages were randomly Campaigns to inform poor rural populations Access to standard Children less than 1 year
Pradesh controlled trial selected. 10 households per village (5 low about entitled health and education services services old receiving ≥ 1 vaccine
caste, 5 middle-to-high caste) with at least were conducted in two rounds in each dose
one child going to public primary school village. Each round comprised two to three
were invited to join the baseline survey. 1 hour meetings consisting of an audiotaped
Vaccine outcomes relate to 337 households presentation, question period and leaflet
(intervention 149; control 79) with a child distribution. Participants were re-interviewed
less than 1 year after 12 months.
Morris et al., 200421 Honduras Cluster randomized 70 municipalities with the highest rates of Group 1 received vouchers worth £2.53 per Access to standard Proportion of children
controlled trial malnutrition were selected and randomly month for each pregnant woman or child services 93 days to 3 years
assigned to one of four study groups in younger than 3 years, up to a maximum of who received DTP1;
the ratio 2:1:2:2. Approximately 470 000 two. Payments required compliance with proportion of children
people received one or both interventions. child preventive health care. 1 year old who received
Vaccination analyses for DTP1 compared 810 Group 2 improved health services via better measles vaccine
children in Group 1 to 878 controls. planning, training and small repairs and
purchases.
Group 3 received both packages.
(continues. . .)
Bull World Health Organ 2015;93:339–346C| doi: http://dx.doi.org/10.2471/BLT.14.146951
Mira Johri et al.You can also read